Embed Size (px)
Citation preview

Association of Schizophrenia With Low MaternalBody Mass Index, Small Size at Birth,and Thinness During ChildhoodKristian Wahlbeck, MD, MScD; Tom Forsen, MD, MScD; Clive Osmond, PhD;David J. P. Barker, FRS; Johan G. Eriksson, MD, MScD
Background: Nutritional factors in early life may con-tribute to the neurodevelopmental deficit in schizophre-nia. This study explores the influence of maternal bodysize, size at birth, and childhood growth on future riskfor schizophrenia.
Subjects and Methods: This population-based co-hort study comprised births at Helsinki University Cen-tral Hospital in Helsinki, Finland, from 1924 to 1933. Pro-spective data from birth and school health records of 7086individuals were collected and linked to the Finnish Hos-pital Discharge Register.
Results: Schizophrenia or schizoaffective disorder hadbeen diagnosed in 114 individuals. A lower late-pregnancy maternal body mass index (BMI) increased therisk (odds ratio [OR], 1.09 per kilogram/meter2; 95% con-
fidence interval [CI], 1.02-1.17) for schizophrenia amongthe offspring. The risk of schizophrenia increased withlow birth weight (OR, 1.48 per kilogram; 95% CI, 1.03-2.13), shortness at birth (OR, 1.12 per centimeter; 95%CI, 1.03-1.22), and low placental weight (OR, 1.22 per100 g; 95% CI, 1.04-1.43). Schizophrenia cases were thin-ner than comparison subjects from 7 to 15 years of age.In a joint model comprising late-pregnancy maternal BMI,body size at birth, and childhood BMI, childhood BMIwas an independent predictor of schizophrenia, whereasother factors exhibited attenuated effects.
Conclusion: Indicators of intrauterine and childhood un-dernutrition are associated with an increased lifetime riskof schizophrenia.
Arch Gen Psychiatry. 2001;58:48-52
S CHIZOPHRENIA IS a severe syn-dromewithaprevalenceofap-proximately1.3%intheFinn-ish adult population.1 Al-though the etiopathogenesis
of schizophrenia is inconclusive, the evi-dence supports genetic predisposition anddisturbed early neurodevelopmental pro-cessesasimportantunderlyingfactors.2Pub-lished data indicate that an array of adversepregnancy and perinatal factors are relatedtosubsequentschizophrenia,3 including in-fectionsduringthesecondtrimesterofpreg-nancy,4 starvation in utero,5 and obstetriccomplications.6 Preeclampsia, which is as-sociated with a reduced nutritional supplyto the fetus, is the obstetric complicationmost strongly associated with schizophre-nia.7 Delayedmotordevelopmentandlowerchildhood educational achievements inpeoplewholaterdevelop thesyndrome8 in-dicate that schizophrenia originates longbefore the onset of evident illness.
An association between low birthweight (,2500 g) and schizophrenia hasbeen reported in a retrospective case-control study9 and replicated in a recentpopulation-based prospective study fromnorthern Finland,10 which found that low
birth weight and the combination of lowbirth weight and short gestation (,37weeks) were more common among schizo-phrenic subjects. However, that study didnot find a connection between schizophre-nia and low weight for gestational age.10 Ina Swedish population-based cohort, smallbirth size for gestational age and a low pon-deral index (birth weight/length3) were as-sociated with increased risk of schizophre-nia, but only among men.11 However, bothcohort studies were restricted to prenataland perinatal risk factors and had a fol-low-up only until subjects were in their20s, which excluded later cases of schizo-phrenia from the analyses. In the British1946 birth cohort with 30 schizophreniacases, no evidence of differences betweencases and controls in birth weight or inheight and weight at ages 7 and 11 yearswas found.8
We assembled a cohort of 7086 menand women who were born at HelsinkiUniversity Central Hospital in Helsinki,Finland, between 1924 and 1933. The aimof the study was to clarify the effects of fe-tal and childhood nutrition, as reflectedin late-pregnancy maternal body mass in-dex (BMI), size at birth, and growth dur-
ORIGINAL ARTICLE
From the Department ofPsychiatry, University ofHelsinki (Dr Wahlbeck), andthe National Public HealthInstitute (Drs Forsen andEriksson), Helsinki, Finland;and the Medical ResearchCouncil EnvironmentalEpidemiology Unit, Universityof Southampton, Southampton,England (Drs Osmond andBarker).
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, JAN 2001 WWW.ARCHGENPSYCHIATRY.COM48
©2001 American Medical Association. All rights reserved.Downloaded From: http://archpsyc.jamanetwork.com/ on 03/17/2013

ing childhood, on lifetime risk of developing psychosesin the broad schizophrenia group.
RESULTS
In the cohort, 114 cases with a hospital diagnosis of broadschizophrenia were identified, which indicates a cumu-lative incidence of 1.6% (1.3% in men and 1.9% inwomen). A primary diagnosis of schizoaffective disor-der was found in 16 cases, and the remainder were di-agnosed with schizophrenia. None had a diagnosis ofschizophreniform disorder. The occurrence of schizo-phrenia was not related to year of birth.
The mean±SD age of mothers in the cohort was27.6±5.7 years, and the mean±SD parity was 2.3±1.8.The mothers of schizophrenic subjects were similar tothe other mothers regarding their age and parity.
In the unaffected control group (n=6972), mean±SDmaternal BMI was 26.8±3.2 kg/m2, mean birth weight
was 3383±508 g, mean birth length was 50.0±2.0 cm,and average BMI at age 7 years was 15.3±1.2 kg/m2.
MATERNAL BODY SIZE
Table 1 presents ORs for schizophrenia associatedwith a unit decrease in late-pregnancy body size. Moth-ers’ late-pregnancy BMI was significantly related to theoccurrence of schizophrenia in their offspring. Table 2indicates that this finding depended mainly on an in-creased risk with late-pregnancy BMIs of 30 or less.Mothers’ heights were not related to schizophrenia inoffspring.
BIRTH SIZE
Men and women who were born small had an increasedrisk of schizophrenia. Both low birth weight and a shortlength at birth increased the risk (Tables 1 and 2). Schizo-
SUBJECTS AND METHODS
SAMPLE
The risk set originated from 27068 men and women bornat the public Helsinki University Central Hospital be-tween 1924 and 1933. The hospital served both people liv-ing within Helsinki (population 221524 in 1933) and peopleliving outside the city in southern Finland. This study in-cluded children who went to primary schools in the cityof Helsinki. Both birth and school health records were avail-able for 8580 subjects. School health records of subjectsborn at the Helsinki hospital but who lived outside the cityand went to rural primary schools were not included.
We used birth and school health records to trace 7086subjects who still lived in Finland in 1971.12,13 At that time,a unique personal identification number was assigned toall residents by the Finnish Population Register.
RISK FACTORS
Data on mothers’ height, weight in late pregnancy, age, par-ity, and the date of the last menstrual period were extractedfrom birth records together with data on the newborns’ length,weight, head circumference, and placental weight.14 Using thefather’s occupation, the subjects were grouped according toa social classification used by the Central Statistical Office ofFinland.15 Overall, 78% of the fathers were laborers, and 10%were lower middle class. Together these constitute the lowersocial class as opposed to the upper social class, which is sub-divided into upper middle class (2%) and self-employed (2%).The social status of 8% could not be classified.
For each subject, height and weight were measuredduring school medical examinations twice a year from ages6 to 16 years.12,13 The number of household inhabitants andthe number of rooms in the home had been recorded whenthe child first began school.
IDENTIFICATION OF CASES
Using the unique personal identification number, the indi-viduals were linked with the Finnish Hospital Discharge
Register (HDR). The HDR was founded in 1967 and cov-ers all psychiatric and general hospitals. It contains data onprimary diagnosis and up to 3 subsidiary diagnoses onboth discharges and deaths of inpatients, regardless oflength of hospitalization. The HDR is a valid and reliabletool for epidemiological research.16 Accuracy of primarydiagnoses in the HDR is acceptable; a 96.3% agreementbetween HDR data and case notes has been reported in aschizophrenia sample.17 The predictive power of an HDRdiagnosis in a broad schizophrenia spectrum is 0.93 whencompared with a “gold standard” consensus diagnosismade against clinical records by 2 senior research psychia-trists using the Diagnostic and Statistical Manual of MentalDisorders, Revised Third Edition (DSM-III-R) criteria.17
Diagnoses have been entered in the HDR according tothe International Classification of Diseases, Eighth Revision(ICD-8) until 1986, according to ICD-9 using the DSM-III-Rcriteria between 1987 and 1995, and according to ICD-10 cri-teria from 1996 onward. The first 3 digits from the cause ofadmission were used to identify the occurrence of schizo-phrenia, schizophreniform disorder, or schizoaffective dis-order: 295 in ICD-8 and ICD-9 and F20 and F25 in ICD-10.
STATISTICAL ANALYSES
In this study, any individual found in the HDR with a pri-mary or subsidiary diagnosis as defined previously until De-cember 1996 was assigned to the schizophrenia group. Thisgroup of broad schizophrenia was compared with the re-mainder of the risk set. We used multiple logistic regres-sion analysis to calculate odds ratios (ORs) for schizophre-nia, adjusting for sex. Odds ratios are reported with 95%confidence intervals (CIs). The independent variables weincluded were maternal, neonatal, and childhood growthmeasurements. We assessed the joint effect of variables inthis sequence by including them simultaneously in a mul-tiple regression analysis. Childhood heights, weights, andBMIs were all converted to age- and sex-specific z scoresusing the method of Royston.18 We interpolated betweensuccessive z scores with a piecewise linear function andobtained a z score at each birthday from age 7 years to age15 years. We then converted back these z scores to obtainthe corresponding height, weight, and BMI at each age.
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, JAN 2001 WWW.ARCHGENPSYCHIATRY.COM49
©2001 American Medical Association. All rights reserved.Downloaded From: http://archpsyc.jamanetwork.com/ on 03/17/2013

phrenia was not associated with head circumference atbirth or with ponderal index (birth weight/length3).Length of gestation (days) was not associated with in-creased risk of schizophrenia (OR, 1.01; 95% CI,0.99-1.02). There was no difference in the proportion ofpreterm births ( # 37 weeks) in the schizophrenia group(11.2% of births) when compared with the rest of the co-hort (10.9% of births) (x2
1=0.008, P=.93). A low pla-cental weight was associated with an increased risk ofschizophrenia. As expected, size at birth was related tomothers’ late-pregnancy BMI (r=0.23 with birth lengthP,.001). In a simultaneous regression, both shortnessat birth (OR, 1.11; 95% CI, 1.01-1.22; P=.03) and lowlate-pregnancy maternal BMI (OR, 1.07; 95% CI, 1.00-1.15; P=.05) were related to schizophrenia.
CHILDHOOD GROWTH
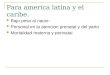
Table 1 indicates that at age 7 years, boys and girls wholater developed schizophrenia had below-average weightand BMI. These differences were statistically significantand remained so at each age up to 15 years (Figure).The height of boys and girls who developed schizophre-nia did not differ significantly from the average betweenages 7 and 15 years. Table 3 presents the simultaneouseffect of birth length and BMI at 7 years on risk ofschizophrenia. The highest risk was in people who wereshort at birth and thin in childhood. In a simultaneousregression with mothers’ late-pregnancy BMI, birthlength, and offspring’s BMI at age 7 years, only lowerBMI at age 7 years remained significantly associated withschizophrenia (OR, 1.37; 95% CI, 1.13-1.66; P=.001).Shortness at birth was of borderline significance (OR,1.10; 95% CI, 1.00-1.20; P=.06), and lower late-preg-nancy maternal BMI was not significant (OR, 1.05; 95%CI, 0.97-1.12; P= .22). Findings in men and womenwere similar.
CHILDHOOD SOCIOECONOMIC CIRCUMSTANCES
The average number of inhabitants in the homes where theboys and girls grew up was 5 (range, 1-27). The averagenumber of rooms in the house was 2 (range, 1-14), and47% lived in homes with only 1 room. As in previous stud-ies,12,13 we used the ratio of the number of inhabitants tothe number of rooms as an index of crowding. Families liv-ing in less crowded conditions were of higher social class,and the children were taller and weighed more between ages7 and 15 years.12,13 However, the level of crowding in thehousehold during childhood was not related to the risk ofbroad schizophrenia (OR, 0.93; 95% CI, 0.58-1.47), norwas risk related to social class at birth, defined by the fa-ther’s occupation (OR, 1.38; 95% CI, 0.91-2.09).
COMMENT
Schizophrenia is a disorder with a multifactorial patho-genesis. The importance of pregnancy and delivery fac-tors has been highlighted in previous studies. The presentstudy is unique in combining maternal, birth, and child-hood growth characteristics. Our results indicate that in asemiurban setting, small infants who are born to lean moth-ers and become thin in childhood are at increased risk for
Table 1. Odds Ratios for SchizophreniaAssociated With a Unit Decrease in Body Sizein 7086 Men and Women in Helsinki, Finland*
Variable OR (95% CI) P Value
Mothers’ late-pregnancy body sizeWeight, kg 1.02 (1.00-1.04) .08Height, m 0.99 (0.95-1.02) .40Mother’s BMI, kg/m2 1.09 (1.02-1.17) .01
Placental sizePlacental weight, 100 g 1.22 (1.04-1.43) .01
Neonatal body sizeBirth weight, kg 1.48 (1.03-2.13) .03Length at birth, cm 1.12 (1.03-1.22) .009Ponderal index, kg/m3 1.02 (0.94-1.10) .67Head circumference, cm 1.06 (0.93-1.21) .41
Childhood body sizeWeight at age 7 y, kg 1.14 (1.05-1.23) .001Height at age 7 y, cm 1.02 (0.99-1.06) .20BMI at age 7 y, kg/m2 1.39 (1.17-1.66) ,.001Weight at age 15 y, kg 1.03 (1.00-1.05) .04Height at age 15 y, cm 1.00 (0.97-1.02) .88BMI at age 15 y, kg/m2 1.16 (1.05-1.28) .003
*OR indicates odds ratio; CI, confidence interval; and BMI, body mass index.
Table 2. Odds Ratios for Schizophrenia Accordingto Late-Pregnancy Maternal, Neonatal, and ChildhoodBody Size in 7086 Men and Women in Helsinki, Finland*
Variable No. of Subjects OR (95% CI)
Mothers’ late-pregnancyBMI, kg/m2†
#24 1101 3.75 (1.42-9.89)#26 1825 3.04 (1.18-7.84)#28 1746 3.06 (1.19-7.91)#30 933 3.06 (1.12-8.38).30 904 1.00 (Reference)
P for trend = .01
Birth weight, g#2500 336 2.91 (0.81-10.39)#3000 1265 4.17 (1.47-11.84)#3500 2747 2.16 (0.77-6.09)#4000 2044 3.00 (1.07-8.45).4000 694 1.00 (Reference)
P for trend = .03
Birth length, cm‡#48 1225 2.35 (1.15-4.81)#49 1119 2.42 (1.18-4.98)#50 2077 1.90 (0.96-3.77)#51 1343 1.54 (0.72-3.28).51 1295 1.00 (Reference)
P for trend = .009
BMI at 7 y, kg/m2
#14.5 1656 2.60 (1.54-4.40)#15 1273 0.91 (0.45-1.83)#15.5 1285 1.25 (0.66-2.37)#16 1114 1.13 (0.57-2.24).16 1758 1.00 (Reference)
P for trend ,.001
*OR indicates odds ratio; CI, confidence interval; and BMI, body mass index.†Data on 577 mothers missing.‡Data on 27 newborns missing.
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, JAN 2001 WWW.ARCHGENPSYCHIATRY.COM50
©2001 American Medical Association. All rights reserved.Downloaded From: http://archpsyc.jamanetwork.com/ on 03/17/2013

schizophrenia. Leanness during childhood seems to be anindependent, additive risk factor to small size at birth. Thus,our results support the role of early life and childhood in-fluence in the pathogenesis of schizophrenia.
Our study was restricted to men and women born atHelsinki University Central Hospital. About 60% of Hel-sinki births occurred at this hospital. The fathers of 78%of the cohort subjects were classified as laborers. The sub-jects may be unrepresentative of all people living in Hel-sinki, although we know that in 1930, around 60% of thecity’s men were laborers. This would introduce a bias onlyif the associations between maternal, neonatal, and child-hood body size and schizophrenia differed between peopleborn in the hospital and those born in other places.
Subjects who died before 1971 and subjects who neverwent to primary school, such as severely mentally re-tarded children, are excluded from our cohort. Some sub-jects were lost because of early mortality; infant mortalitywas 6.5% during the period between 1924 and 1933.19
Therefore, the associations in our study are representa-tive of a population that has reached middle age. One canassume that adverse maternal, pregnancy, and childhoodfactors exert their maximum effect early in life,20 and thusthe possible bias arising from selective loss of people whodied before middle age is more likely to lead to an under-estimation of the associations between early risk factorsand schizophrenia than to an overestimation.
We were able to trace 92% of the people originallyidentified through birth and school records. Our find-ings gain strength from the prospectively collected growthdata and the occurrence and coverage of the HDR. Re-sults from retrospective case-control studies on schizo-phrenia may be distorted or inflated because of bias incase selection or ascertainment of risk factor informa-tion. However, in the present population- and register-based study, all data on risk factors for schizophrenia wereascertained before an outcome was known.
One limitation of our study is that it excluded bothschizophrenia subjects who were never hospitalized andthose hospitalized in young adulthood only before 1971.
In an extensive cross-sectional health survey of a repre-sentative sample of the Finnish adult population be-tween 1978 and 1980, 86% of those with psychosis werecurrently receiving treatment.21 In Finland, treatment ofschizophrenia almost always includes hospitalization. Thecumulative incidence of 1.6% in our cohort, born be-tween 1924 and 1933, is compatible with the findings ofa declining incidence of schizophrenia in Finnish birth co-horts22 and the 1-month prevalence of schizophrenia of1.3% in the population study from 1978 to 1980.1
Like another population-based cohort study,11 wefailed to replicate the finding of small head circumfer-ence at birth made in retrospective case-control studies ofclinical samples.23,24 Those studies may include more se-verely ill patients, with a stronger connection to premor-bid brain abnormalities. A similar discrepancy between co-hort and case-control studies has been described concerningobstetric complications as a risk factor for schizophre-nia.6 Together these observations may indicate a true dif-ference between clinical- and population-based samples,and they suggest the need for caution when interpretingfindings from retrospective case-control studies.
The association between small birth size and schizo-phrenia was not due to shortened gestation and must there-fore be caused by reduced rates of growth. We suggest thatthe associations with reduced fetal growth, small placen-tal size, and late-pregnancy maternal thinness indicate thatschizophrenia may originate through fetal undernutri-tion. This conclusion is strengthened by findings amongpeople who were conceived during the height of the Dutchfamine in 1945, whose risk for a schizophrenia-spectrumdisorder was increased almost threefold.25 Although therewas no acute food shortage in Finland during the years ofcohort birth, the nutritional situation of the lower classeswas not good. About half of an average blue-collar work-er’s wages was spent on food, and food shortage was com-mon in working-class families with many children. The pri-mary source of protein was cereal products, mainly bread.26
Inapreviousanalysisofthissemiurbancohort,wefoundthat high maternal BMI in late pregnancy was associatedwithahighrateof coronaryheartdisease inmen.14 Wenowfind that low late-pregnancy maternal BMI increased thechild’s risk of subsequent schizophrenia. Mothers’ late-pregnancyBMIreflectsbothweightgainduringpregnancy
75%
21
20
19
18
17
16
15
147 8 9 10
Boys and Girls WithSubsequent Schizophrenia
11Age, y
12 13 14 15
50%
25%
Body
Mas
s In
dex,
kg/
m2
Body mass index (BMI) during childhood for 114 girls and boys who laterdeveloped schizophrenia in comparison with rest of cohort.
Table 3. Odds Ratios (95% Confidence Intervals)for Schizophrenia According to Tertiles of BirthWeight and Length, and Body Mass Index (BMI)at Age 7 Years, in 7086 Subjects*
BMI at Age 7 y, kg/m2
#14.8 .14.8 and #15.7 .15.7
Birth weight, g#3180 2.5 (1.3-5.0) 0.9 (0.4-2.3) 1.5 (0.7-3.5)3190-3590 1.9 (0.9-3.9) 1.0 (0.4-2.4) 0.5 (0.1-1.4)$3600 1.5 (0.7-3.5) 1.1 (0.5-2.6) 1.0 (Reference)
Birth length, cm#49 4.0 (1.8-8.8) 1.2 (0.4-3.2) 2.2 (0.9-5.4)49.5-50.5 2.7 (1.2-6.3) 2.3 (0.9-5.6) 1.2 (0.4-3.4)$51 2.1 (0.8-5.1) 1.1 (0.4-3.0) 1.0 (Reference)
*The total number of schizophrenia cases was 114.
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, JAN 2001 WWW.ARCHGENPSYCHIATRY.COM51
©2001 American Medical Association. All rights reserved.Downloaded From: http://archpsyc.jamanetwork.com/ on 03/17/2013

and BMI before pregnancy. Body mass index in late preg-nancy is highly correlated with BMI before pregnancy(r=0.86;KeithMalcolmGodfrey,BM,PhD,MRCP,unpub-lished data, 1991-1992, 1994-1995).
In a later Finnish general-population cohort of sub-jects born in 1966, when the socioeconomic circum-stances in Finland had improved, a high prepregnancy ma-ternal BMI was associated with schizophrenia. In asecondary analysis of that cohort, the heaviest fifth per-centile (BMI $29) of mothers had a doubled risk of off-spring with schizophrenia when compared with the middle90%, but the finding was not statistically significant.10 Thediffering findings between our study and the later Finnishcohort may reflect societal changes. A low BMI in the late1920s or early 1930s, in a society without developed wel-fare structures,was linked tomalnutritionor illness,whereasin 1966, when the population’s nutritional status was good,it was more a matter of choice. In current Western popu-lations, a high rather than low maternal BMI is more likelyto be associated with adverse outcomes,27 such as late fe-tal death,28 neural tube defects,29 and other congenital mal-formations.30 However, it does protect against the deliv-ery of an infant that is small for its gestational age. Wesuggest that our cohort’s independent association be-tween thinness in childhood and schizophrenia may re-flect childhood undernutrition. Our data indicate that chil-dren with a length of 49 cm or less at birth, and who werebelow the lowest BMI tertile at age 7 years, had a fourfoldrisk of developing schizophrenia when compared with chil-dren who were above upper BMI tertile at age 7 years andwere longer at birth (Table 3). In 1932, only 29% of chil-dren were offered meals in primary schools. The cohort ex-perienced a food shortage during adolescence in 1942, butthere was no wartime famine in Finland because of orga-nized food rationing.26 In the Dutch famine study,25 peri-conceptional famine was associated with an increased riskof schizophrenia. The current study associates indicatorsof continued undernutrition with schizophrenia.
Epidemiologic studieshave foundthat schizophrenicpatients usually belong to lower socioeconomic groups.However, the classic study by Goldberg and Morrison31
found that the social class distribution of the fathers ofschizophrenic subjects did not differ from that of the gen-eral population, which indicates that the excess of personswithschizophrenia inthe lowestsocioeconomicgroupmaybe more the result of a downward drift, or a decrease insocial status, than of a socioeconomic causative factor. Inthe present study, those original findings were replicated:we found no significant difference between groups in so-cioeconomicdistributionaccording to fathers’ occupation.Schizophreniadevelopedin1.5%ofchildrenof laborersandin 2% of children of nonlaborers. A similar trend of asso-ciationbetweenschizophreniaandhighsocial classatbirthwas reported in the British 1946 cohort.8 Thus, the asso-ciation with nutritional status does not seem to be medi-ated by socioeconomic status of the family.
In conclusion, low late-pregnancy maternal BMI,small placental size, and small size at birth, possibly in-dicating fetal undernutrition, are associated with in-creased lifetime risk of schizophrenia. Subjects who sub-sequently developed schizophrenia remained lean duringchildhood, which may indicate continued malnutrition.
Accepted for publication July 20, 2000.This study was supported in part by the British Heart
Foundation, London, England (Dr Barker), and the Wilhelmand Else Stockmann Foundation, Helsinki, Finland(Dr Wahlbeck).
Corresponding author: Kristian Wahlbeck, MD, MScD,Department of Psychiatry, University of Helsinki, Lapp-viksvagen, PO Box 320, FIN-00029, Helsinki, Finland(e-mail: [email protected]).
REFERENCES
1. Lehtinen V. The epidemiology of mental disorders in Finland. Nord J Psychiatry.1996;50(suppl 36):25-30.
2. Murray RM. Neurodevelopmental schizophrenia. Br J Psychiatry. 1994;165:6-12.3. Cannon TD. Abnormalities of brain structure and function in schizophrenia. Ann
Med. 1996;28:533-539.4. Mednick SA, Machon RA, Huttunen MO, Bonett D. Adult schizophrenia following
prenatal exposure toan influenzaepidemic. ArchGenPsychiatry. 1988;45:189-192.5. Susser E, Neugebauer R, Hoek HW, Brown AS, Lin S, Labovitz D, Gorman JM.
Schizophrenia after prenatal famine. Arch Gen Psychiatry. 1996;53:25-31.6. Geddes JR, Lawrie SM. Obstetric complications and schizophrenia. Br J Psy-
chiatry. 1995;167:786-793.7. Dalman C, Allebeck P, Cullberg J, Grunewald C, Koster M. Obstetric complica-
tions and the risk of schizophrenia. Arch Gen Psychiatry. 1999;56:234-240.8. Jones P, Rodgers B, Murray R, Marmot M. Child developmental risk factors for adult
schizophrenia in the British 1946 birth cohort. Lancet. 1994;344:1398-1402.9. Rifkin L, Lewis S, Jones P, Toone B, Murray R. Low birth weight and schizo-
phrenia. Br J Psychiatry. 1994;165:357-362.10. Jones PB, Rantakallio P, Hartikainen AL, Isohanni M, Sipila P. Schizophrenia as
a long-term outcome of pregnancy, delivery and perinatal complications. Am JPsychiatry. 1998;155:355-364.
11. Hultman CM, Sparen P, Takei N, Murray RM, Cnattingius S. Prenatal and peri-natal risk factors for schizophrenia, affective psychosis, and reactive psychosisof early onset. BMJ. 1999;318:421-426.
12. Eriksson JG, Forsen T, Tuomilehto J, Winter PD, Osmond C, Barker DJP. Catch-upgrowth in childhood and death from coronary heart disease. BMJ. 1999;318:427-431.
13. Forsen T, Eriksson JG, Tuomilehto J, Osmond C, Barker DJP. Growth in uteroand during childhood among women who develop coronary heart disease. BMJ.1999;319:1403-1407.
14. Forsen T, Eriksson JG, Tuomilehto J, Teramo K, Osmond C, Barker DJP. Moth-er’s weight in pregnancy and coronary heart disease in a cohort of Finnish men.BMJ. 1997;315:837-840.
15. Central Statistical Office of Finland. Classification of Socio-economic Groups. Hel-sinki, Finland: Central Statistical Office of Finland; 1983. Handbook 17.
16. Keskimaki I, Aro S. The accuracy of data on diagnoses, procedures and accidentsin the Finnish Hospital Discharge Register. Int J Health Serv. 1991;2:15-21.
17. MakikyroT, IsohanniM,MoringJ,HakkoH,HovattaI,LonnqvistJ.Accuracyofregister-based schizophrenia diagnoses in a genetic study. Eur Psychiatry. 1998;13:57-62.
18. RoystonP.Constructing time-specific referenceranges.StatMed.1991;10:675-690.19. Helsingin kaupungin tilastollinen vuosikirja 1934 [Statistical Yearbook of City of
Helsinki 1934]. Helsinki, Finland: City of Helsinki; 1934:66-67.20. Verdoux H, Geddes JR, Takei N, Lawrie SM, Bovet P, Eagles JM, Heun R, McCreadie
RG, McNeil TF, O’Callaghan E, Stober G, Willinger MU, Wright P, Murray RM.Obstetric complications and age of onset in schizophrenia. Am J Psychiatry. 1997;154:1220-1227.
21. Lehtinen V, Joukamaa M, Jyrkinen E, Lahtela K, Raitasalo R, Maatela J, AromaaA. Need for mental health services of adult population in Finland. Acta PsychiatrScand. 1990;81:426-431.
22. Suvisaari JM, Haukka JK, Tanskanen AJ, Lonnqvist JK. Decline in the incidenceof schizophrenia in Finnish cohorts born from 1954 to 1965. Arch Gen Psychia-try. 1999;56:733-740.
23. Hultman CM, Ohman A, Cnattingius S, Wieselgren IM, Lindstrom LH. Prenataland neonatal risk factors for schizophrenia. Br J Psychiatry. 1997;170:128-133.
24. Kunugi H, Takei N, Murray RM, Saito K, Nanko S. Small head circumference atbirth in schizophrenia. Schizophr Res. 1996;20:165-170.
25. Hoek HW, Brown AS, Susser E. The Dutch famine and schizophrenia spectrumdisorders. Soc Psychiatry Psychiatr Epidemiol. 1998;33:373-379.
26. Karjalainen J. Kovia aikoja [Hard times]. In: Heikkila M, Hanninen S, KarjalainenJ, Kontula O, Koskela K, eds. Nalka. Helsinki, Finland: Stakes; 1994:1-16.
27. Wolfe H. High prepregnancy body-mass index. N Engl J Med. 1998;338:191-192.28. Cnattingius S, Bergstrom R, Lipworth L, Kramer M. Pregnancy weight and the
risk of adverse pregnancy outcomes. N Engl J Med. 1998;338:147-152.29. Kallen K. Maternal smoking, body mass index, and neural tube defects. Am J
Epidemiol. 1998;147:1103-1111.30. Queisser-Luft A, Kieninger-Baum D, Menger H, Stolz G, Schlaefer K, Merz E. Does
maternal obesity increase the risk of fetal abnormalities? Ultraschall Med. 1998;19:40-44.
31. Goldberg EM, Morrison SL. Schizophrenia and social class. Brit J Psychiatry.1963;109:785-802.
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, JAN 2001 WWW.ARCHGENPSYCHIATRY.COM52
©2001 American Medical Association. All rights reserved.Downloaded From: http://archpsyc.jamanetwork.com/ on 03/17/2013