-
ESSENTIAL TREMORReferat 6 / Tahun IIIOleh: Meilia M.
SuriadiPembimbing: dr. Djadjang Suhana, SpS(K)
-
TREMOR Osilasi ritmis involunter bagian tubuh tertentu dalam
dataran tertentuKontraksi otot agonis & antagonis Simultan atau
alternansPola sinyal berasal dari osilator sentral
-
ESSENTIAL TREMORGangguan gerak Sering terjadi pada
dewasaPengaruh terhadap tampilan aktivitas fungsional &
sosial.Diferensiasi terhadap sindroma tremor lain penting edukasi
& terapi
-
Essential Tremor
-
EPIDEMIOLOGIPrevalensi: 0,3-5,6% populasi umum0,5-11,1%:
pertolongan medisPria = wanita usiaUsia awitan: Bimodal (15-20 th
& 50-70 th)Rata-rata: 35-45 th
-
EPIDEMIOLOGIAmplitudo tremor: usiaFrekuensi tremor: usiaDewasa
muda: 8-12 HzLanjut usia: 6-8 HzDisabilitas 85%: perubahan
signifikan dalam kehidupan sosial15%: disabilitas serius akibat
ET
-
Essential Tremor2 bentuk ET:Familial ETSporadic ETKlinis: tak
ada perbedaanUsia awitan:Familial ET: dekade 2 / 3Sporadic ET:
dekade 6 / 7
-
ETIOLOGIEsensial: bawaan / diturunkanFamilial ET: 50-70%
kasusAutosomal dominanGen: kromosom 3q (FET1) & 2p
(ETM)Sporadic ET: etiologi ?
-
PATOFISIOLOGILesi struktural spesifik belum
diidentifikasiMekanisme patofisiologi belum jelasPencitraan
Metabolik: kerusakan neuronal serebelumFungsional: keterlibatan Nc
olivarius inferior & serebelum dalam generasi dan propagasi
aktivitas osilasi abnormal perifer: tremor
-
Perubahan konsentrasi penanda biokimia sentral & perifer
GABA, glisin, serin LCS ringan glutamat LCS Abnormalitas reseptor
GABAA thalamus epinefrin pada daerah spesifik otakLocus ceruleus
5x, nc dentatus 130x, korteks serebelum 2x
-
GAMBARAN KLINISTremor 1 extremitas superior sisi lainGerakan:
fleksi-ekstensi pergelangan tanganAsimetri ringanIntermiten (saat
aktivasi emosional) persistenAmplitudo : aktivitas emosional:
aktivitas manual terampilHilang saat tidur
-
Essential TremorMonosymptomatic Abnormalitas langkah &
keseimbanganTremor postural & kinetik, frekuensi 4-12 HzTremor
hilang saat relaksasi bagian tubuhTonus & refleks normal
-
Essential TremorTremor kepalaPola horizontal atau vertikalTremor
suara, lidah, palatumDisartria Palatum: clicking dalam telinga
-
Kriteria Diagnostik ET
Inclusion criteria:Bilateral, largely symmetric postural or
kinetic tremor involving hands and forearms that is visible and
persistentPossible additional or isolated tremor in head but
absence of abnormal posturing Exclusion criteria:Other abnormal
neurologic signs, especially dystonia The presence of known causes
of enhanced physiologic tremor, including current or recent
exposure to drugs that are known to cause tremor or a
drug-withdrawal stateHistoric or clinical evidence of psychogenic
tremor Convincing evidence of sudden onset or evidence of stepwise
deteriorationPrimary orthostatic tremorIsolated voice
tremorIsolated position-specific or task-specific tremors,
including occupational tremors and primary writing tremorIsolated
tongue or chin tremorIsolated leg tremor
-
WHIGET Tremor Rating Scale
ScoreDefinition0Absolutely no visible tremor 1Mild tremor,
intermittent or continuous; similar to normal or enhanced
physiologic tremor 2Obvious tremor that is expected in patients
with essential tremor. Must meet all the following
criteria:Moderate amplitudeUsually presentClearly oscillatory (hand
not just a little shaky or unsteady but clearly oscillates between
2 extremes) 3Large-amplitude, jerky tremor. Examples include:When
handling liquids (pouring, drinking, using a spoon), patient spills
but is able to complete the task without spilling all the
liquid.When touching finger to nose, patient has difficulty hitting
examiners finger and circles around it many times.When drawing a
spiral, large-amplitude wavy tremor present, but patient able to
draw spiral. 4Extremely large-amplitude, jerky tremor. Examples
include:When handling liquids (pouring, drinking, using a spoon),
patient unable to attempt the task or to perform the task without
spilling all the liquid.When touching figner to nose, patient has
difficulty hitting examiners finger and circles around it many
times; patient reluctant to touch own face for fear of
self-injury.When drawing a spiral, patient unable to make or
maintain pen to paper contact; unable to draw a spiral.
-
PEMERIKSAAN PENUNJANGDiagnosis ET: klinisTak ada penanda
biologisCT scan & MRI normalPemeriksaan laboratorium &
pencitraan: bila riwayat keluarga & pemeriksaan ETEMG /
akselerometri: bukan pemeriksaan rutin
-
DIAGNOSIS BANDINGMultiple sclerosisPenyakit WilsonChorea
HuntingtonPenyakit degeneratif serebelumTremor dipresipitasi obat
& toksnTremor dipresipitasi penyakit sistemik
-
PENATALAKSANAANTujuan: Minimalisasi disabilitas
fungsionalMengurangi hambatan sosialMeningkatkan kualitas hidup
penderitaJenis:FisioterapiIntervensi tingkah laku &
psikologisPerubahan gaya hidupFarmakoterapiTindakan bedah
-
Pemilihan jenis kebutuhan & keadaan penderitaKeparahan
tremorPenyakit koeksistenTerapi obat saat iniRespons terhadap
terapi sebelumnyaTidak perlu penatalaksanaan bila tak ada keluhan
disabilitas fungsional / psikososialTerapi farmakologisMengurangi
amplitudo tremor & disabilitasTerapi simptomatikJangan berharap
eradikasi tremor menyeluruhTidak mengobati, mencegah, memperlambat
progresi penyakit
-
Fisioterapi & Intervensi Tingkah LakuTeknik pembelajaran
adaptifET ringanMinimalisasi disabilitas fungsional, social
embarrassment, & jejas personalContoh:Gunting ujung
tumpulSerbet di bawah cangkir
-
FarmakoterapiET ringan:Minimalisasi paparan stres emosional
& makanan-minuman tremorogenikReassurance-blocker / alkohol;
intermitenET mengganggu aktivitas harian:Farmakoterapi jangka
panjangPilihan kondisi komorbid, keamanan, efikasiPenilaian
efektivitas obat: menulis, menuang, minum
-
-blockerTerapi lini pertamaPropranolol: Terpilih efikasi telah
terbuktiMekanisme belum diketahuiDiduga: via hambatan reseptor 2
perifer dalam serabut / gelendong ototDosis: 120-240 mg/hariDurasi
efek 4 jamPropranolol lepas lambatMetoprolol, timolol, atenolol,
sotalol
-
-blockerEfek samping: BronchospasmeDepresi, insomniaDisfungsi
ereksiKontraindikasi relatif:Gagal jantung berat, blok konduksi
jantungBronchospasmePenderita DM tipe II
-
PrimidonStruktur analog fenobarbitalMetabolit utama: PEMA &
fenobarbitalMekanisme kerja: belum diketahuiEfektivitas
propranololObat lini pertamaDosis < 250 mg/hariDurasi 24 jam
-
PrimidonEfek samping:Terutama saat awal terapiNausea,
malaiseAtaxia, dizziness, sedasi, bingungKontraindikasi:Kehamilan,
menyusui, porfiria
-
GabapentinMekanisme kerja: belum diketahuiDiduga: peranan tonus
GABAergik sentralTerapi jangka pendek 1200-1800 mg/hari pada lanjut
usiaDapat ditoleransi sebagai terapi jangka panjang pada dewasa
mudaTerapi alternatif untuk ET Efek samping: Ataxia, iritabilitas,
sedasi, kenaikan berat badan
-
AlkoholEfek tremorolitik temporerPET: alkohol hiperaktivitas
serebelum, mungkin dimediasi mekanisme GABAergik
-
BenzodiazepinMekanisme kerja: belum diketahuiDiduga augmentasi
GABAergikEfek ansiolitik penderita cemasHati-hati: lanjut usia efek
samping sentralAlprazolamEfektivitas primidonDosis 0,75
mg/hariKlonazepam: 1-6 mg/hariLorazepam: 0,25-0,5 mg prn
-
Botulinum toxin ATremor kepala & suara yang resisten
terhadap obat-obatan oralTerbatas untuk tremor ekstremitas
superiorKontraindikasi:Miastenia gravis, sindroma
Eaton-LambertPenyakit motor neuron, sindroma pascapolioAntibiotika
aminoglikosidaKehamilan
-
Intervensi bedahPenderita dengan disabling
tremorTeknik:Thalamotomi stereotaktikChronic thalamic deep brain
stimulation (DBS)Kontraindikasi:Keadaan umum burukGangguan
kognisiDapat bersifat kuratif
-
Thalamotomi stereotaktikThermokoagulasi Nc. Ventralis
intermedius (Vim) thalamusDisrupsi aktivitas tremorogenik abnormal
di sirkuit serebelum-thalamusUnilateral, kontralateral tremor
extremitasEfikasi tinggiMorbiditas persisten & berat <
2%
-
Thalamic Deep Brain Stimulation (DBS)Penderita dengan disabling
tremor tak terkontrol adekuat dengan farmakoterapiNonablatif &
dapat disesuaikanUnilateral atau bilateralMorbiditas permanen
rendahMekanisme kerja: belum diketahuiDiduga: supresi tremor ec
chronic artificial neural noise disrupsi aktivitas siklik sirkuit
motorik
-
Thalamic Deep Brain Stimulation (DBS)Efikasi thalamotomiTremor
extremitas, kepala & suaraEfek samping: (jarang)Penurunan
kognitif, disartria, paresis facialGait imbalance, ataxia
lenganKekurangan:BiayaRisiko respons inflamasi & infeksi
-
Practice ParameterAmerican Academy of NeurologyPropranolol &
primidon mengurangi tremor extremitasBotulinum toxin A mungkin
mengurangi tremor kepala & suaraChronic DBS & thalamotomi
memberikan efikasi tinggi dalam mengurangi tremor
-
ESSENTIAL TREMOREducation & SupportFunctional
impairmentSocial embarrassmentYesPrimidone
orGabapentinNoPropranololCombination therapy Thalamotomy or Vim DBS
for upper extremityBotulinum toxin for disabling head & voice
tremormonitorYesNoContraindications to -blockers?
-
THANK YOU
-
Samuel Adams American Revolutionist 1722-180340 yo
-
71 yo
-
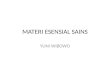
Deep brain stimulation (DBS) electrode implanted intracranially
with wires connecting to pulse generators in the intraclavicular
region. DBS electrode has four platinum/ridum contacts. Sagittal
MRI shows electrode implanted in subthalamic nucleus of patient
with Parkinsons disease.
-
Figure 2. A deep brain stimulator electrode is placed in the
desired structure of the brain. The electrode is connected to a
battery implanted under the skin below the collarbone. The patient
is able to turn the generator off and on with a handheld control
magnet Figure 3. A stereotactic head frame is attached to the
patient's head with four pins. A localizer cage is placed on top of
the frame during the MRI scan.
-
Figure 4. An electrode is precisely positioned in the desired
brain area with the aid of a stereotactic head frame. Once the
exact nerve cells are located, the surgeon can pass a heating
current to destroy those cells or insert a stimulator to regulate
those cells
-
DBS of the VIM nucleus relieves tremor for PD and also patients
suffering from essential tremor. DBS of one or both STN nuclei
provides excellent control of all PD symptoms, including L-dopa
related dyskinesia. The Procedure Stereotactic frame placement
under local anaesthesia. MR targetting. Calculation of co-ordinates
of the target. Burr-hole under local anaesthesia. Insertion of
electrode to the target, guided by macro-stimulation and or
micro-electrode recordings. The patient stays awake and interacts
continuously with the neurologist and neurosurgeon to find the best
location (within 1 or 2 mm) to achieve maximum benefit. Under
general anaesthesia, the electrode is connected to the programmable
pulse generator placed under the skin of the chest wall. The
movement disorder team will activate the generators and determine
the correct settings to obtain the maximum clinical benefit with
minimal side effects. Once the optimal settings have been
determined, the patients can turn stimulation on and off with a
small magnet. For example, some patients may turn the generator off
at bedtime. Risks of DBS is small in experienced hands for suitably
selected patients. There is a 2% risk of serious bleeding inside
the brain, and a small chance of infection plus other possible
remote risks of burr-hole and anaesthesia.
-
In 1997, the FDA approved the marketing of the implanted device
to suppress tremor in people with essential tremor and Parkinson's
disease. This system includes an insulated wire lead that is
surgically implanted deep within the thalamus. The lead is
connected by an extension wire passed under the skin to a pulse
generator implanted near the collarbone. Patients control the
stimulation by passing a hand-held magnet over the implanted pulse
generator to turn it on or off, or to increase or decrease
stimulation depending on their tremor suppression needs. To achieve
maximum tremor suppression, physicians program the generator to
deliver the precise stimulation needed for each individual patient.
In clinical studies, more than 80 percent of essential tremor and
Parkinson's patients had total or significant suppression o f their
disabling tremor and significant reduction in disability. Patients
in clinical studies have resumed daily life activities that were
previously difficult or impossible, such as writing, pouring
liquids, feeding and dressing themselves. Tremor medications often
can be reduced or discontinued. Tremor control therapy is indicated
for patients whose drugs are ineffective in controlling their
disabling tremor. The most common potential side-effects of
stimulation include paresthesia, paresis, dysarthria and
disequilibrium, but these generally are reduced or disappear when
stimulation is decreased or stopped. Risk typically associate with
this surgery includes loss of effect and intracranial
hemorrhage.