Embed Size (px)
Citation preview

INTERVENTIONAL NEPHROLOGY AND DIALYSIS
Chronic Peritoneal Dialysis Catheters: Overview of Design,Placement, and Removal Procedures
Stephen R. AshDialysis Center for Greater Lafayette, Arnett Clinic, and HemoCleanse, Inc., Lafayette, Indiana, and PurdueUniversity, West Lafayette, Indiana
ABSTRACT
The success of chronic peritoneal dialysis (PD) depends to alarge extent on the success of the chronic PD access device. Forthe nephrologist placing and removing PD catheters, or for thenephrologist advising surgeons in this role, this article providesa review of designs of PD catheters and differences in functionand complications, methods of insertion of PD catheters andrelation to catheter outcomes, techniques for ‘‘burying’’ theexternal portion of the PD catheter and benefits of this
technique, and techniques for removing PD catheters. Asnephrologists become more closely involved in the creation,monitoring, and maintenance of access devices for end-stagerenal disease (ESRD) patients, the successful function of thesedevices will increase. Nephrologists should make the criticaldecisions regarding the choice of access devices and methods forplacement as they do for the choice to remove such accessdevices.
Types of Chronic Peritoneal Catheters
Chronic peritoneal dialysis (PD) catheters are the mostsuccessful of all transcutaneous access devices, withlongevity and successful function measured in yearsrather than days to months. They are constructed of softmaterials like silicone rubber or polyurethane. Theintraperitoneal portion usually contains 1 mm side holes,but one version has linear grooves or slots rather thanside holes. All chronic PD catheters have one or twoextraperitoneal Dacron cuffs that promote a localinflammatory response. In a unique example of beneficialbioincompatibility, the sclerotic process produces afibrous plug to fix the catheter in position, prevent fluidleaks, and prevent bacterial migration around thecatheter. In spite of general success, peritoneal accessfailure is still a source of frustration for all PD programs,and catheter failure is the reason for ‘‘dropout’’ fromsuch programs in about 25% of patients. Increasing thesuccess of a continuous ambulatory peritoneal dialysis(CAPD) program requires optimizing the function ofperitoneal catheters. Currently the method of placementof the catheter has more effect on the outcome of thecatheter than its choice (1,2).
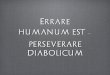
As shown in Fig. 1, there appears at first to be abewildering variety of chronic peritoneal catheters.However, each portion of the catheter has only a few
basic design options (3). There are four designs for theintraperitoneal portion: straight Tenckhoff, with an 8 cmportion containing 1 mm side holes; curled Tenckhoff,with a coiled 16 cm portion containing 1 mm side holes;straight Tenckhoff, with perpendicular discs (Toronto-Western, rarely used); and T-fluted catheter (AshAdvantage) with grooved limbs positioned against theparietal peritoneum. There are three basic shapes forthe subcutaneous portion between the muscle wall andthe skin exit site: straight, or gently curved; a 150-degreebend or arc (Swan Neck), and a 90-degree bend, withanother 90-degree bend at the peritoneal surface (Cruz‘‘Pail Handle’’ catheter). There are three positions anddesigns for Dacron cuffs: a single cuff around thecatheter, usually placed in the rectus muscle but some-times on the outer surface of the rectus; dual cuffs aroundthe catheter, one in the rectus muscle and the other in thesubcutaneous tissue; and a disc-and-ball deep cuff, withparietal peritoneum sewn between the Dacron disc andsilicone ball (Toronto-Western and Missouri catheters).There are three internal diameters of PD catheters, eachhaving an outer diameter of approximately 5 mm (seeFig. 2): 2.6 mm, the standard Tenckhoff catheter size; 3.1mm, the Cruz catheter; and 3.5 mm, the Flexneckcatheter. There are two materials of construction:silicone rubber (nearly all catheters) and polyurethane(Cruz catheter).
The various intraperitoneal designs were all created todiminish outflow obstruction due to the normal diminu-tion in flow that occurs as peritoneal surfaces approachthe catheter or due to omental attachment to the catheter.The shape of the curled Tenckhoff catheter and the discsof the Toronto-Western catheter to some degree holdvisceral peritoneal surfaces away from the side holes of
Address correspondence to: Stephen R. Ash, MD, FACP,HemoCleanse, Inc., 3601 Sagamore Pkwy. N, Lafayette,IN 47904, or e-mail: [email protected].
Seminars in Dialysis—Vol 16, No 4 (July–August) 2003pp. 323–334
323

the catheter. The grooves of the Advantage catheterdistribute flow over the surface of the limbs that contactthe parietal peritoneum, providing a much larger surfacearea for drainage than side holes provide. An irritatedomentum attaches firmly to side holes of a catheter butonly weakly to grooves on a catheter (as demonstrated bythe Blake surgical drain, with grooves on the cathetersurface).
The subcutaneous portion all of PD catheters providesa lateral or downward direction of the exit site. A lateralor downward direction minimizes the risk of exitinfection. An upward-directed exit site collects debrisand fluid, increasing the risk of exit site infection.
The optimal location for the standard deep cuff iswithin the rectus muscle (described below). The subcu-taneous cuff provides additional protection from bacter-ial contamination of the subcutaneous tunnel. Thedisc-and-ball deep cuff provides security of catheterposition security since, with the peritoneum sewnbetween the Dacron disc and intraperitoneal ball, thecatheter is fixed in position and cannot migrate outward.
Similarly the T shape of the Advantage catheter placesthe intraperitoneal limbs against the parietal peritoneum,preventing outward migration of the catheter.
The larger internal diameter of the Cruz and Flexneckcatheters provides lower hydraulic resistance and morerapid dialysate flow during the early phase of outflow. Inthe latter part of outflow, the resistance to flow isdetermined mostly by the spaces formed by peritonealsurfaces as they approach the catheter. The Advantagecatheter provides much larger entry ports for drainage ofperitoneal fluid, and limited clinical studies have dem-onstrated faster drainage of the peritoneum in the earlyand late phases of outflow and a decrease in residualperitoneal volume at the end of outflow.
Changing the construction material of peritonealcatheters has not changed the incidence of cathetercomplications. Polyurethane catheters do not have alower incidence of peritonitis or omental attachmentleading to outflow failure. Polyurethane catheters gener-ally have a weaker bond to the Dacron cuff, andloosening of this bond can create pericatheter leaks.
Fig. 1. Currently available peritoneal cath-
eters: combinations of intraperitoneal and
extraperitoneal designs.
Ash324

Proper Location of Chronic Peritoneal CatheterComponents
There is general agreement on the proper location ofchronic peritoneal catheter components (see Fig. 3):• The intraperitoneal portion should be between the
parietal and visceral peritoneum and directedtoward the pelvis to the right or left of the bladder.
• The deep cuff should be within the medial or lateralborder of the rectus sheath.
• The subcutaneous cuff should be approximately 2cm from the skin exit site.
Placing the deep cuff within the rectus musclepromotes tissue ingrowth and therefore avoids pericath-eter hernias, leaks, catheter extrusion, and exit siteerosion (2–4). At the parietal peritoneal surface, thesquamous epithelium reflects along the surface of thecatheter to reach the deep cuff. If the deep cuff is outsidethe muscle wall, the peritoneal extension creates apotential or actual pericatheter hernia. At the skin
surface, the stratified squamous epithelium follows thesurface of the catheter until it reaches the superficial cuff.If the tunnel from the subcutaneous cuff to the exit site islonger than 2 cm, the squamous epithelium disappearsbefore reaching the cuff and granulation tissue is left,leading to an exit site with continued ‘‘weeping’’ of serousfluid, and the potential for exit site infection is increased.If the subcutaneous cuff is too close to the exit site thenthe cuff will irritate the dermis and the exit site will becontinually reddened and inflamed.
Some peritoneal catheters have components thatprovide greater fixation of the deep cuff within themusculature. When the Missouri and Toronto-Westerncatheters are placed, the parietal peritoneum is closedbetween the ball (inside the peritoneum) and disc (outsidethe peritoneum). When the T-fluted (Ash Advantage)catheter is placed, the wings open in position adjacent tothe parietal peritoneum and perpendicular to the pene-trating tube. With these two catheters, outward migra-tion of the catheter is impossible.
When placing peritoneal catheters, especially by blindor peritoneoscopic approaches, it is best to choose a deepcuff location that is free of major blood vessels (Fig. 4).The superficial epigastricarteries course fromthe femoralartery and ligament toward the umbilicus, anterior to therectus sheath. The inferior epigastric arteries lie behindthe rectus muscles, roughly in the middle of the rectussheath. Considering the position of these arteries, thesafest locations for inserting a needle or cannula to placethe catheter are in the medial or lateral borders of therectusmuscle.Byphysical examination, the lateralborderof the rectus can be determined by asking the patient totense theabdomenandpalpatingthe lateralborder,or forpatients with weaker abdominal muscles this border isalways locatedhalfwaybetweentheanteriorsuperior iliac
Fig. 3. The proper relationship of peritoneal cuffs to abdominal
musculature and skin exit site for a straight Tenckhoff catheter.
Fig. 2. Comparison of cross-sectional dimensions of the intra-
peritoneal portion of several peritoneal catheters: (A) Flexneck
Tenckhoff catheter (silicone), (B) Cruz Tenckhoff catheter (polyur-
ethane), (C) standard Tenckhoff (silicone), and (D) one intraperito-
neal limb of the T-fluted catheter (Ash Advantage, silicone).
Fig. 4. Major blood vessels and landmarks of the anterior
abdominal wall. Open squares represent the preferred and safest
points for locating the deep cuff of a chronic peritoneal catheter
within the medial or lateral border of the rectus muscle. Solid squares
indicate the external landmarks used during blind insertion of a
needle or cannula at the start of peritoneoscopic or blind catheter
placement: half the distance between the anterior superior iliac spine
for the lateral border of the rectus, and 2 cm below the umbilicus for
the medial border of the rectus. (Adapted from Ash SR, Daugirdas
JT: Peritoneal access devices. In: Daugirdas JT, Ing TS (eds).
Handbook of Dialysis, 2nd ed. New York: Little, Brown, 1994:274–
300; with permission.)
CHRONIC PD CATHETERS 325

spine and the midline. The medial border is locatedapproximately 1 cm from the midline, below the umbi-licus. The exact location of the medial and lateral borderof the rectus muscle can be determined more preciselyusing ultrasound (such as with the Site-Rite) by movingthe probe laterally from midline to flank. Positioning theprobe over potential sites for catheter placement in anorientation todetectverticalmovementof thevisceraalsoallows a qualitative assessment of motion and a deter-mination of which sites are most freely mobile andtherefore less likely to contain dense adhesions.
PD Catheter Implantation Methods
Chronic PD catheters are placed by one of threemethods. In each case, the abdomen is thoroughlyprepped, carefully draped, and general sterile techniqueis used (cap, mask, gown, gloves, etc.).
Dissection
Dissection is a surgical technique in which layers oftissue are separated under direct vision. A 3–5 cm‘‘primary’’ skin incision and a 2–3 cm incision throughthe rectus muscle (5,6) are made. The parietal peritoneumis identified, incised, and lifted to create an air spacebetween parietal and visceral peritoneum. The catheterand internal stylet are advanced by feel into theperitoneum, until the deep cuff is within the rectusmuscle (for Tenckhoff-type catheters). For the Missouriand Toronto-Western catheters, the ball is advanced intothe abdomen and the parietal peritoneum sewn betweenthe ball and Dacron disc (5). Dissective placement isgenerally performed under light general anesthesia, butcan be done with local anesthesia if desired.
Blind Puncture
The abdomen is first prefilled with fluid, and a needle isinserted through the muscle wall. Then a guide wire isplaced, the tract is dilated, and the catheter is insertedthrough a split-sheath (similar to that used for IJcatheters). When the deep cuff stops at the externalrectus, the split-sheath is separated and removed, leavingthe deep cuff in a location just outside the abdominalmusculature. Blind placement is done with localanesthesia. Only Tenckhoff-type catheters can be placedby blind techniques (not Missouri, Toronto-Western, orAdvantage catheters).
Peritoneoscopy
Peritoneoscopy, in which a 2.2 mm diameter, 15 cmlong peritoneoscope (Y-Tec) is used to inspect theperitoneum and choose the proper location of theperitoneal catheter, which follows the same course whenthe scope is removed. A cannula, internal trocar, andsurrounding Quill guide are inserted into the abdomen,the intraperitoneal position confirmed using the scope,and then about 1 L of air is manually injected to create apneumoperitoneum. The cannula is advanced between
the visceral and parietal peritoneum under vision, thescope and cannula are removed, the Quill is expandedwith dilators, and the peritoneal catheter is advancedthrough the Quill. The deep cuff enters the musculatureby expanding the Quill, with the Cuff Implanter tooladvancing the cuff so that the outer portion is just belowthe external rectus sheath (Fig. 5). Peritoneoscopicplacement is also used for placement of the Advantagecatheter, though the catheter can also be placed bydissection. A second spiral guide encloses the catheterwith the intraperitoneal limbs folded forward. This spiralguide is advanced through the Quill guide, and when theQuill guide and spiral guide are retracted, the limbs openagainst the parietal peritoneum. The deep cuff isautomatically positioned within the rectus muscle.Peritoneoscopic placement of Tenckhoff and Advantagecatheters is generally done with local anesthesia (asopposed to laparoscopic placement).
Tunneling the catheter is similar for each method ofinsertion. The exit site is determined by laying thecatheter over the skin in a gentle downward bend (forstraight subcutaneous segment catheters) or in an arcuatecourse (for Swan Neck catheters). The exit site is chosenat a point 2 cm external to the subcutaneous cuff
Fig. 5. Steps for implantation of a Tenckhoff peritoneal catheter
using the Y-Tec system including the Quill, Peritoneoscope, Cuff-
Implanter, and Tunnelor Tool.
Ash326

(if present). A ‘‘secondary’’ incision is made by inserting ano. 11 scalpel blade to the hub. A Tunnelor Tool orsimilar device is advanced through the subcutaneous fatfrom the secondary incision to the primary incision. Thetip of the catheter is attached to the Tunnelor, and the tipbrought through the secondary incision. Hemostats arelightly applied to the catheter tubing (outside thesuperficial cuff) and the tips of the hemostats are drawninto the tunnel. When the tips of the hemostats reach thedesired position of the subcutaneous cuff, the tips arespread and the hemostat removed. The catheter is pulledthrough the exit site and the subcutaneous cuff is drawninto the tunnel, to rest 2 cm from the exit site.
There are advantages and disadvantages of eachtechnique of catheter placement, and the overall successof the catheter is highly dependent upon the method ofplacement. Dissective techniques securely place the deepcuff within the abdominal musculature. However, theincision in the abdominal musculature requires sur-rounding tissues to first close the wound, then grow intothe deep cuff before the deep cuff is secure. Pericatheterleaks are frequent if the catheter is used immediately afterplacement. The dissective approach provides very littlevisualization of the peritoneal surfaces and no visualiza-tion of adhesions or assessment of spaces free ofadhesions within the peritoneum. The catheter may beadvanced into loops of bowel, or near adhesions, andearly outflow failure of the catheter may result.
Blind placement procedures are convenient, can beperformed anywhere in a hospital, and have theadvantage of being low cost. Bowel perforation is anoccasional complication (about 1 in 100 placements) andno visualization of the peritoneal space is provided toavoid impinging the catheter tip on adhesions or visceralsurfaces. The standard procedure leaves the deep cuffoutside of the abdominal musculature, not within therectus sheath, unless specific further steps are taken, suchas grasping the cuff with hemostats and driving the cuffinto the rectus muscle.
Peritoneoscopic placement allows the best visualiza-tion of the peritoneal space. This avoids placing thecatheter under bowel loops, under omentum or againstadhesions. The Quill expands to allow the deep cuff toadvance into the musculature. The Y-Tec procedure canbe performed in any room in the hospital. Specializedequipment must be purchased, however, and the physi-cian must have some training in peritoneoscopic tech-niques. A number of publications have described usingstandard laparoscopic equipment to place peritonealcatheters. The visualization of the peritoneum by usingthese laparoscopes is actually better than with the Y-Tecscope. Tenckhoff catheters can be placed by any of themethods described above. The disc-and-ball, Missouri,or Toronto-Western catheters, however, can only beplaced by dissection techniques.
Effects of Placement Techniqueson the Success of Chronic PD Catheters
The success of peritoneal catheters depends more onplacement technique than on their design (1,3,7,8).
Peritoneoscopic placement results in the lowest inci-dence of catheter complications and a catheter half-lifeof more than 3 years (3). Randomized, controlledstudies have confirmed that catheter survival isapproximately twice as long for those placed byperitoneoscopy versus catheters placed by dissectivetechniques (9,10). In these studies nephrologists placedthe catheters peritoneoscopically and surgeons placedthe catheters by dissection. Table 1 summarizes theresults of more than 70 studies on the incidence ofserious catheter complications (infection, outflow fail-ure, and pericatheter leak) during an average follow-upof 13 months after catheter placement. Cathetersincluded all types of Tenckhoff-type catheters andToronto-Western catheters. Infectious complicationsare defined as any peritoneal or catheter infectionexcept randomly occurring peritonitis. Results areorganized according to the type of catheter andmethod of placement (1,3,7).
Among the methods of placement, the peritoneo-scopic method (generally performed by nephrologists)has the lowest incidence of infectious complicationsover the life of the catheter. The decreased incidence ofcatheter infection may relate to the decreased amountof tissue trauma and smaller incision size of theperitoneoscopic placement versus dissective placement,and better assurance that the cuff is placed within themuscle versus blind placement. Outflow failure andleaks are comparable between peritoneoscopic place-ment and surgical dissection, but are higher with blindplacement. This relates to the lack of peritonealvisualization during positioning of the catheter withblind techniques and the usual position of the cuffoutside the rectus sheath rather than within the rectusmuscle.
There are also differences in the ability for early useof catheters for supportive dialysis according to themethod of placement. Peritoneoscopically placed cath-eters may be used for PD treatments immediately tosupport the patient without need for HD in almostany schedule that does not include the full volume ofthe peritoneum during times of activity. This includesnight-time cycler therapy or overnight exchanges, butexcludes full-volume CAPD (3). Surgically placedcatheters can also be used immediately if the deepcuff is secured by sutures within the rectus muscle, butin general, PD is delayed for 2 weeks after placement.Catheters placed by blind techniques can be used forimmediate dialysis in the immobile patient (as in ahospital bed), but a delay of 1–2 weeks is necessary inmost patients before beginning PD.
TABLE 1. Incidence of complications leading to removal of chronic
PD catheters during the lifetime of the catheter, arranged according to
method of placement (fraction of catheters placed)
Insertion method Infections Outflow failure Leaks
Blind: trocar or guide wire 0.24 0.16 0.17Surgical: dissection 0.35 0.07 0.06Peritoneoscopic 0.13 0.06 0.06
Summary of 70 published studies on all types of catheters (1).
CHRONIC PD CATHETERS 327

Effects of Catheter Design on the Successof the Catheter
Randomized, prospectively controlled studies havegenerally shown little effect of catheter design on thesuccess of peritoneal catheters. One study by Nielsenet al. (11) demonstrated a longer 3-year survival of coiledversus straight Tenckhoff catheters. If properly placed,dual-cuff Tenckhoff catheters have a lower incidence ofexit site infection and longer life span than single-cuffcatheters (1,2,12), though properly placed single-cuffcatheters can work as well (13). Curled Tenckhoffcatheters have a lower incidence of outflow failure thanstraight catheters in some studies (2,11). Swan Neckcatheters have a lower incidence of exit site infection thanthose with straight subcutaneous segments (14). Non-randomized studies of specific catheters have indicatedvarious advantages, including that catheters with the bestfixation of the deep cuff (such as the Missouri andAdvantage catheters) have a very low incidence of exitsite infection (7).
Some Tenckhoff catheters, such as the silicone rubberFlexneck, have a larger internal diameter and thinnerwalls than standard catheters (Fig. 2). Flexneck cathetersare more pliable and create less tension between deep andsuperficial cuffs during normal patient activities. Thisdecreased tension may result in a lower incidence ofpericatheter leaks and hernias, and fewer exit site andtunnel erosions over time, but this benefit has not beenproven. These catheters, like the Cruz catheter, create ahigher rate of inflow and initial outflow versus thestandard Tenckhoff catheters with smaller internaldiameters. Rapidity of flow at the end of outflow forthe Cruz catheter is also aided by the 90-degree angle ofthe catheter at the parietal surface, which positions thecoiled portion next to the parietal peritoneal surface (2).Catheters constructed from polyurethane (such as theCruz) have excellent strength and biocompatibility.However, the glue bonding of the Dacron cuff to thecatheter may fail over 1–2 years of use, resulting in leaksand infections (3). A problem with Flexneck catheters isthat they are also prone to crimping in the subcutaneoustunnel if they are angled sharply. If physicians follow atemplate to create a subcutaneous tunnel with a gentledownward curve, crimps in the subcutaneous tract areeliminated.
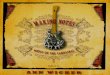
The Advantage catheter contains a straight portionwhich is adjacent to the parietal peritoneum, ensuring astable position without extrusion of the deep cuff or exitsite erosion (similar to the disc-and-ball catheters and theolder Lifecath catheter) (15). Further, the grooves of thecatheter allow fluid inflow from every direction overevery part of the intraperitoneal portion. Advantagecatheters placed in patients beginning PD and those withprevious Tenckhoff failures demonstrate a 1-year survi-val of 90%, higher than the 50–80% survival forTenckhoff catheters in numerous other studies (Fig. 6).During follow-up of 30 patients with Advantagecatheters in place for up to 4 years, only 1 patientdeveloped a pericatheter leak (resolved by delayingCAPD), and no patient developed a pericatheter hernia
or late exit infection. Pericatheter leak with the Advant-age catheter has only occurred in patients with evidenceof catheter infection and subsequent lack of ingrowth tothe catheter cuffs. The outflow rate of PD fluid is onaverage equal to the best functioning Tenckhoff catheters(including the large internal diameter Flexneck cathe-ters). Outflow volume is more consistent with theAdvantage catheter. In CAPD exchanges with the sameglucose concentration and dwell time, the Advantagecatheter has a standard deviation of 2%, versus 10% forTenckhoff catheters. The consistent peritoneal outflow isprobably due to more complete drainage of the perito-neum, with a diminished residual volume. Diminishedresidual volume is important, since if residual volume isdecreased by 300–500 ml, the inflow volume can beincreased by the same amount, thus increasing theperitoneal clearance by 10–20% without increasingpatient discomfort by overfilling the abdomen.
Advantage peritoneal catheters diminish the risk ofoutflow failure, but do not eliminate this risk. Themechanism of outflow failure is different from Tenckhoffcatheters. Omentum does not directly attach to theintraperitoneal portion of the catheter, but rathersurrounds the long, slotted intraperitoneal catheter limbsand traps them against the parietal peritoneum. Infusionof iodine dye during fluoroscopy demonstrates that thedye does not pass freely in many directions out of thegrooves of the catheter, but rather stays near the catheterand exits from the ends of the intraperitoneal limbs.Laparoscopic removal of adhesions from around thecatheter can often result in a perfectly functioning PDcatheter.
There are two major challenges remaining for alltranscutaneous catheters: to diminish infection of thecatheter and the surrounding biofilm and to avoidoutflow failure due to adhesions. A variety of antibac-terial coatings have been developed for central venouscatheters, but these coatings have not demonstrated alower infection rate. To prevent exit site infection andcatheter seeding that results in persistent peritonitis,antibacterial materials must be applied to the inside andoutside of the peritoneal catheter. In long-term use, silverand sulfa compounds tend to disappear from the surfaceof the catheters, diminishing effectiveness. Impregnationof the catheter with silver can also cause local irritation of
Lifetable Analysis of Production Advantage CathetersDialysis Center for Greater Lafayette, IN, 2000-2001
0
0.2
0.4
0.6
0.8
1
0 6 12 15 18 21 24
Months of Followup
Fra
ctio
n R
emai
nin
g W
ith
ou
t F
ailu
re
(30) (5)(14)
(2)
3 9
Fig. 6. Life table analysis of survival of the Advantage PD
catheter placed in patients with previous Tenckhoff catheter failures
and in patients new to PD.
Ash328

the exit site and simulate peritonitis. Peritoneal catheterswith a long-term and effective antibacterial surface arestill an elusive goal, but several new approaches tosterilization of biofilm are now being evaluated. A finalchallenge is to limit the growth of adventitial tissuearound and onto catheters, such as in fibrous sheathingof central venous catheters and omental attachment toperitoneal catheters. Some new materials are beingevaluated that are both bactericidal and mildly cytocidalto determine whether these can prevent fibrous attach-ment and sterilize catheter surfaces and biofilm. Thesematerials must be applied to the catheter body and notthe cuffs, so that tissue ingrowth can occur normally tothe cuffs while the catheter body avoids such ingrowth.
New Placement Techniques
Several recent publications have described the use oflaparoscopic techniques for the placement of peritonealcatheters. These techniques use 5–10 mm diametertrocars generally used for laparoscopic surgery. Theseare much larger than the 2.2 mm peritoneoscope used inthe Y-TEC system, and provide much better visualiza-tion of the peritoneal space. However, there are severaldisadvantages to laparoscopic placement: the procedureusually requires general anesthesia, the CO2 used toinflate the abdomen is more irritating to the peritoneumthan air, the procedure usually requires two punctures tothe peritoneum (one for the scope and one for thecatheter), and placement of the deep cuff is notautomatically ensured to be within the rectus. If thecatheter is advanced through a 5 mm split sheath,the deep cuff will be outside the external rectus sheath. Ifthe catheter is advanced through a 10 mm cannula, thedeep cuff will end up within the intraperitoneal space oroutside the rectus muscle. Some adjustment of cuffposition is almost always necessary after the catheter isfirst placed. As opposed to catheters placed with speciallydesigned equipment, those placed by the laparoscopictechnique have no advantage in longevity over thoseplaced by dissection.
Burying the PD Catheter
Traditional surgical implantation of Tenckhoff cath-eters involves immediate exteriorization of the externalsegment through the skin, so that the catheter can be usedfor supportive PD or for intermittent infusions duringthe ‘‘break-in’’ period. In order to prevent blockage andto confirm function, the catheter is flushed weekly withsaline or dialysate; each exchange carries the same risk ofperitonitis as in CAPD therapy. The catheter must alsobe bandaged and the skin exit site must be kept clean inthe weeks after placement to avoid bacterial contamin-ation of the exit site. The patient must therefore betrained in some techniques of catheter care. It has alwaysbeen difficult to decide when to place a PD catheter in apatient with chronic renal insufficiency. If the catheter isplaced too early, the patient may spend weeks to monthscaring for a catheter that is not used for dialysis. If the
catheter is placed after the patient becomes uremic, thenit is often used for PD therapy without a ‘‘break-in’’period.
Moncrief et al. (16) devised a placement technique inwhich the entire peritoneal catheter can be buried underthe skin some weeks to months before it is used. Thecatheter burying technique was first described forplacement of a modified Tenckhoff catheter with a 2.5cm long superficial cuff, but the technique has beenadopted for standard dual-cuff Tenckhoff catheters(17–19). In the original technique the external portionof thecatheterwasbrought througha2–3cmskinexit site(much larger than the usual 0.5 cm incision). The catheterwas tied off with silk suture, then coiled and placed into a‘‘pouch’’ created under the skin. The skin exit site wasthen closed. Weeks to months later, the original skin exitsite was opened and the free end of the catheter wasbrought through the original skin exit site (16,17).
The goal of burying the PD catheter was to allowingrowth of tissue into the cuffs of the catheter withoutthe chance of bacterial colonization, and to create atranscutaneous exit site after tissue had fully grown intothe deep and subcutaneous cuffs. Burying the cathetereffectively eliminated early pericatheter leaks anddecreased the incidence of peritonitis. In 66 months offollow-up, patients with the buried Tenckhoff catheterhad peritonitis infection rates of 0.017–0.37 infections peryear, versus 1.3–1.9 infections per year in control patients(16). In a study of 26 buried Tenckhoff catheters, theincidence of infections during PD was 0.8 infections/yearand the incidence of catheter-related peritonitis was only0.036/patient-year (17). A retrospective study confirmedsignificantly lower catheter infection and peritonitis ratesin patients with buried catheters and a significantlylonger catheter life (20), although the procedure was noteffective when used for single-cuff catheters (21).
Exit site infections were not decreased with buriedcatheters, but this is understandable, since a large exit siteis created when the catheter is buried, and a similarlylarge site is re-created when the catheter is exteriorized(22,23). Creating the ‘‘pouch’’ under the skin requires aconsiderable amount of dissection and trauma near theexit site. The size of the pocket limits the length of thecatheter that can be coiled and buried under the skin,limiting the external length of the catheter after exteri-orization. The exit site must be opened widely to removethe catheter, because the coil rests in a position distantfrom the skin exit site. Subcutaneous adhesions to the silksutures around the catheter further restricts removal.Increased trauma near the exit site during placement andremoval of the catheter have caused an increasedincidence of early exit infection with this technique(1–4). In one study of ‘‘embedded’’ catheters in 26 adultpatients (with mean subcutaneous residence of79.5 days), 2 patients developed local seromas and12 developed subcutaneous hematomas (5 of which wererevised surgically) (7). At catheter ‘‘activation’’ therewere a number of flow problems: nine patients developedfibrin thrombi (two requiring operative clearance) andfour patients had omental catheter obstruction (fourrequiring omentectomy). When burying the Tenckhoffcatheter by standard techniques, there were a total of
CHRONIC PD CATHETERS 329

27 complications in 26 catheter placements, with 13 ofthese complications requiring corrective surgery.
When catheters are placed by the Y-Tec procedure,the Quill and cannula of the system can be reassembledand used to bury the external portions of dual-cuffTenckhoff and Advantage catheters. The catheter exitsite is made slightly larger than the standard exit site. TheQuill and cannula are inserted through this exit site tocreate a long, straight tunnel for the external end of thecatheter. The catheter is blocked with an internal plugrather than an external silk suture. Using this technique,we have buried and then removed more than 40Tenckhoff and Advantage catheters. There have beenfew early complications of hematoma, seroma, exitinfection, or outflow failure, and all catheters havefunctioned after exteriorization.
The first portion of the Y-Tec placement procedure isexactly as usual for a dual-cuff Tenckhoff catheter(9,10,12,13). The only difference is that the skin exit site ischosen slightly more distal from the subcutaneous cuffthan usual and the exit site incision is made slightly larger(1 cm, or two widths of the no. 11 scalpel blade ratherthan the usual 0.5 cm stab wound). After the catheter istunneled and exteriorized through the exit site, the stepsfor burying the catheter are as follows:1. Reattach the Quill guide to the cannula, first
inserting the trocar to ‘‘lock’’ the tab into placeand then ‘‘clicking’’ the body of the Quill over thecannula (Fig. 7A).
2. Lay the Quill guide and cannula over the skin, in theproper direction just below the umbilicus (forlaterally placed catheters), then cut the catheter sothat the free end of the catheter reaches the end ofthe Quill guide (Fig. 7B).
3. Inject 10 ml of sterile saline with 1000 U of heparininto the catheter, then insert the ‘‘bullet’’ end of theTunnelor tool and break off the tip by rotating thetool backwards and forwards. Advance the outerend of the bullet into the catheter a few millimetersusing hemostats (Fig. 7C).
4. Insert the Quill/trocar assembly into the skin justnext to the catheter, at an angle to reach the middleof the subcutaneous space (Fig. 7D).
5. Advance the Quill in a direction parallel to the skinsurface, directing it into the subcutaneous space justbelow the umbilicus. Keep the tip of the Quill in themiddle of the subcutaneous tissue, between themusculature and the skin. If pain develops, redirectthe Quill to avoid the muscle layer, the dermis, orfibrous adhesions (Fig. 7E).
6. Remove the trocar and cannula from the Quill andgrasp the tab of the Quill with a hemostat. Dilate theQuill with the small dilator, then the larger 6 mmdilator (Fig. 7F).
7. Gently grasp the catheter with nontoothed forcepsor a hemostat and advance the free end of thecatheter into the Quill guide (Fig. 7G).
8. Continue to advance the catheter into the Quillguide until the bend of the catheter reaches the skinlevel. Then hold the bend of the catheter under theskin with forceps and withdraw the Quill guide fromaround the catheter (Fig. 7H).
9. Close the skin exit site with an absorbable suture;point the needle tip upward, away from the catheter,when advancing it through the subcutaneous tissue(Fig. 7I).
To exteriorize the catheter some weeks to monthslater, our current technique is the following:1. Anesthetize the original skin exit site, taking care
not to inject too deeply (raise the edges of theincision with toothed forceps, if necessary).
2. Open the original exit site skin incision usingmosquito hemostats (if less than 2 months havepassed since placement) or a scalpel (if more than2 months of healing). Using larger hemostats,spread the exit site and subcutaneous tissue to theoriginal 1 cm width.
3. Using a hemostat, probe the wound to find thecatheter in its tunnel.
4. Spread the tissue parallel to the tunnel, freeing thetunnel from the subcutaneous tissue along its medialand lateral borders.
5. Advance the tip of the hemostat under the tunneland lift the tunnel and catheter until at skin level.
6. If the tunnel is very thin and wispy, break it open bygrabbing with toothed forceps and pulling portionsoff the catheter. If the tunnel is thick and substantial,grasp it with small-toothed forceps and cut thegrasped portion just below the forceps with Met-zenbaum scissors.
7. Advance one jaw of a smooth-tipped forceps underthe catheter, grasp and lift the catheter, and pull itthrough the skin exit site. Hold the outside portionwith your fingers, grab the tunneled portion, andpull out a portion. Repeat until the tunneled portionis completely removed.
8. By pressing on the sides of the catheter, express theplug outward and remove it.
9. Attach a suitable long-term connector to the end ofthe catheter, inject 50 ml of sterile saline, and checkfor free outflow of fluid and a change in the air-fluidlevel with respiration, indicating that it is completelyopen.
10. Do not close the exit site with sutures. Apply abandage and nonocclusive dressing over the cath-eter exit site as is done for chronic catheter care inCAPD.
Our technique for exteriorization of the first 20catheters included a method for creating a tighter exitsite near the original exit site. The catheter wasexteriorized through the original exit site just as above.Using a scalpel, a stab wound (0.5 cm) was made throughthe skin just 1 cm lateral to the original exit site.Hemostats were advanced through the new exit site,under the skin and through the original exit site. The tipof the external portion of the catheter was grasped withthe hemostats and brought back under the skin andthrough the new exit site. The original skin exit site wasclosed with subcutaneous sutures.
We have buried dual-cuff Tenckhoff and Advantagecatheters after placement since 1993. Patients selected forthis type of placement were those with a trend of renalfunction that indicated a need for PD in 1–6 months, andwe placed peritoneal catheters when the PD therapy was
Ash330

anticipated, rather than when it was immediatelynecessary. The first 30 catheters placed by this techniquewere studied, with time from placement to exteriorizationbeing 1 week to 1 year. On exteriorization, all of theburied catheters were immediately used for PD, and nopatient required HD while awaiting tissue ingrowth tothe catheter cuffs or resolution of problems with the PDcatheter. Follow-up analysis of these catheters rangedfrom 3 to 12 months.
Previous publications regarding burying of PD cath-eters have indicated a number of minor complicationsfollowing the procedure. Complications seen with these30 catheters are shown in Table 2.
Long-term peritonitis rates for these patients havebeen compared to those of patients with cathetersexteriorized immediately on implantation. Peritonitisrates are lower for patients with buried catheters, thoughnot statistically different from patients with immediatelyexteriorized catheters.
In planning for HD of patients with end-stage renaldisease (ESRD), it is common practice to place a fistulaor graft several months before the need for initiation ofdialysis, so that they can ‘‘mature’’ before use. PDcatheters also ‘‘mature’’ after placement, with fibroustissue ingrowth into the cuffs and development of afibrous tunnel. The fully ingrown catheter is more
E
Fig. 7. (A–I) Steps for ‘‘burying’’ the external portion of a PD catheter after bringing the external portion through the skin exit site, using the
Cannula and Quill components of the Y-Tec system for placement of PD catheters.
CHRONIC PD CATHETERS 331

resistant to infection of cuffs and the surface of thecatheter. The technique of burying PD catheters afterplacement allows this maturation to occur before use ofthe catheter, much as with fistulas and grafts. It alsoallows the time of catheter insertion to be separated fromthe time of use, without requiring the patient to learn howto care for the catheter site or observe the catheter site forpotential complications. At initiation of dialysis, thepatient and physician can focus attention on the properperformance of the technique and patient response ratherthan on function of the catheter. The patient can betrained in full-volume CAPD techniques rather than in‘‘break-in’’ or cycler techniques used for immediatelyexteriorized catheters.
A curious aspect of the burying technique is that itseems contrary to ‘‘the rules’’ of catheter break-in. Inimmediately exteriorized catheters, it is necessary toinfuse and drain dialysate or saline (with or withoutheparin) at least weekly to prevent outflow failure orobstruction of the catheter. However, with the com-pletely buried catheter, there is no infusion of any fluidfor periods up to 1 year. Why is this possible? It may bethat in the exteriorized catheter, stress and strain on thecatheter allows some fluid to enter and exit the side holesduring patient movement. The buried catheter has lessmotion, and with a secure blockage, there is very littlefluid inflow/outflow through the holes during normalactivity.
Further, the infusion of saline or dialysate duringbreak-in adds a bioincompatible fluid to the abdomen ata time before the catheter is ‘‘biolized’’ or protein/lipidcoated. The catheter becomes biolized in the absence ofdialysate or saline in the peritoneum. When PD is begun,the catheter is already biolized and less likely to developomental attachment, even in patients with active omen-tum. Studies of catheters buried after surgical placementhave still shown some early loss due to outflow failure,but the rates are not higher than in immediatelyexteriorized catheters (7,8). In our study, the peritoneo-scopic technique was used for placement of the intra-peritoneal portion of the catheter. This method places thecatheter against the parietal peritoneum in an area free ofadhesions or bowel loops, and this method for placementhas already shown a very low incidence of outflow failure
on immediately exteriorized catheters. Outflow failure isnot increased in incidence by burying the catheter forweeks to months.
Removing Chronic PD Catheters
In general, if a physician places a device, the samephysician is expected to be responsible for following theoperation of the device and for removing it whencomplications require removal or when it is no longerneeded. Therefore nephrologists placing peritoneal cath-eters should also learn to remove them. The techniques ofremoval are summarized elsewhere (5). For catheters inplace less than 1 month or those with infection of the deepor superficial cuffs, the original incision can often beopened by a combination of sharp and blunt dissection.The tunnel may be less well formed and easier to enter.Removal of the cuffs can usually be done with bluntdissection (separating the deep cuff from the surroundingmuscle or subcutaneous fibrous tissue with hemostats).
For catheters in place more than 1 month, sharpdissection is necessary to free the cuff and cut thereflecting peritoneal surface (using Metzenbaum scissorsand occasionally a scalpel). All Tenckhoff-type andAdvantage catheters can be removed without significantdiscomfort using only local anesthesia, though Toronto-Western catheters require more dissection and mayrequire conscious sedation. The procedure should bedone only with sterile technique, good lighting, antisepticskin preparation (including the catheter near the skin),and draping typical of a procedure done in a surgicalsuite or outpatient surgery room (drape to cover theprimary incision and purposefully exclude the exit site,since the site and catheter, even when treated withantiseptic, cannot be considered clean). Exposure of thedeep cuff area is required, so vicryl purse-string suturescan be placed to close the external rectus sheath afterremoval of the deep cuff and bleeding vessels can bevisualized within fibrous tissue. Suction and cauteryshould be ready for use if needed.
The steps for removing a dual-cuff Tenckhoff orAdvantage catheter with solid ingrowth of fibrous tissueto the cuff are as follows:1. Anesthetize the original primary incision (over the
deep cuff).2. Using a scalpel, make an incision through the
primary incision, but extend it on each end so thatthe incision is about as long as the subcutaneous fatlayer is deep (determined by ultrasound before theprocedure or by physical examination).
3. Dissect down through subcutaneous fat and occa-sional fibrous bands to identify the subcutaneoustunnel, then use blunt dissection to separate oneportion of the tunnel from the surrounding tissue.
4. Place hemostats under the tunnel and lift the tunnelto the skin surface, securing the tunnel at the skinsurface by advancing the hemostats across theincision.
5. Using toothed forceps and Metzenbaum scissors,lift and cut the tunnel layers, eventually exposing thecatheter.
TABLE 2. Complications of temporarily buried Tenckhoff catheters
ComplicationIncidence
(percent of catheters)
Subcutaneous seroma 0%Hematoma 3% (in one patient with
low platelet count)Bruising over buried portion 6%Tenderness of buried portion 3%Outflow failure on exteriorization 0%Outflow failure within 4 weeks of use 3%Exit site redness within 4 weeks of use 33% (using a second
small exit site)10% (using original
exit site)Exit site infection within 4 weeks of use 3%Peritonitis within 4 weeks of use 3%Pericatheter leaks within 4 weeks of use 0%
Ash332

6. Clamp the catheter with hemostats, place a nylonsuture through the catheter just outside the hemo-stats (as a tag), then cut the catheter just outside thehemostats.
7. Lift the deep portion of the catheter with hemostats,grab one edge of the remaining tunnel with toothedforceps, and cut it longitudinally with Metzenbaumscissors. Repeat this step until the scissors reach thelevel of the outside of the deep cuff.
8. Anesthetize the rectus sheath and muscle at fourpoints around the deep cuff, then use Metzenbaumscissors to cut the fibrous adherent tissue from thedeep cuff (keeping the cuts parallel to and as close aspossible to the cuff, and upward tension on thecatheter). Observe each cut fibrous layer for anybleeding.
9. When the lower edge of the cuff is visible or palpablewith the tip of the Metzenbaum scissors, thereflected parietal peritoneal surface will be seensurrounding the inner part of the catheter. Cut oneside of the parietal peritoneal surface with a scalpel,then extend the incision about halfway around thecatheter, ensuring that the catheter itself is partlyvisible.
10. Place a two-point wide vicryl purse-string suturearound the deep cuff, starting with the point of thecurved needle pointing horizontal and pushing theneedle down to the external rectus sheath while stillplacing traction on the catheter. Do not tie the freeends of the suture.
11. Cut the remaining parietal peritoneal surface free,making sure not to cut the suture, and then removethe internal portion of the catheter while graspingthe body with a gauze (to prevent a coiled Tenckhofffrom ‘‘flipping’’ PD fluid when it is free). ForAdvantage catheters, merely grasp the deep cuff andpull upward.
12. Tie the vicryl suture snugly into a purse string andcut the needle from the suture. Lift the free ends ofthe purse string, and place another two-point pursestring of vicryl. Cut both purse-string sutures nearthe knots.
13. Lift an edge of one of the drapes and cut the catheterat the exit site with scissors (do not use these scissorsagain in the procedure as they may be contaminatedat the exit site).
14. Pull the nylon tag to expose the cut surface of theouter catheter segment within the primary incisionand grasp the catheter segment with hemostats.
15. Apply traction to the catheter segment, grasp theremaining portion of the subcutaneous tunnelwith toothed forceps, and cut the tunnel longi-tudinally with Metzenbaum scissors. Continue tocut the tunnel and apply traction until thescissors meet the medial portion of the superficialcuff.
16. Use Metzenbaum scissors to cut connecting fibroustissue from the cuff, keeping the cuts as close aspossible and parallel to the cuff. Observe cut fibroustissue for signs of bleeding.
17. When the outer portion of the cuff is felt or is visible,it will be attached to the reflected skin exit site
tunnel. Cut one portion of the tunnel and useMetzenbaum scissors to circumferentially cut therest of the tunnel, freeing the cuff and cathetersegment.
18. Close the primary incision with subcutaneous vicryl,then with nylon skin sutures. Do not close the exitsite; if there is bleeding or infection in the subcuta-neous space, the catheter tract serves as an effectivedrainage route.
Removal of Missouri or Toronto-Western-type cath-eters is a little more complicated, since the Dacron discrests next to the peritoneum and develops fibrousadhesion to the peritoneum and the posterior rectussheath. These catheters are generally placed by surgeonsand should be removed by the same surgeons that placedthem (5).
References
1. Ash SR: Chronic peritoneal dialysis catheters: effects of catheter design,materials and location. Semin Dial 3:39–46, 1990
2. Gokal R, Alexander S, Ash S, Chen TW, Danielson A, Holmes C, Joffe P,Moncrief J, Nichols K, Piraino B, Prowant B, Slingeneyer A, Stegmayr B,Twardowski Z, Vas S: Peritoneal catheters and exit site practice: towardoptimum peritoneal access: 1998 update. Perit Dial Int 18:11–33, 1998
3. Ash SR, Carr DJ, Diaz-Buxo JA: Peritoneal access devices: hydraulic func-tion and biocompatibility. In: Nissenson AR, Fine RN, Gentile DE, eds.Clinical Dialysis.Norwalk, CT: Appleton & Lange, 1995:295–321
4. Eklund BH: Surgical implantation of CAPD catheters: presentation ofmidline incision-lateral placement method and review of 100 procedures.Nephrol Dial Transplant 10:386–390, 1995
5. Ash SR, Nichols WK: Placement, repair and removal of chronic peritonealcatheters. In: Gokal R, Nolph KD, eds. Textbook of Peritoneal Dialysis.Dordrecht, The Netherlands: Kluwer Academic, 1994:315–333
6. Ash SR, Daugirdas JT: Peritoneal access devices. In: Daugirdas JT, BlakePG, Ing TS, eds. Handbook of Dialysis, 3rd ed. Philadelphia: LippincottWilliams & Wilkins, 2000:309–332
7. Ash SR: Bedside peritoneoscopic peritoneal catheter placement of Tenckhoffand newer peritoneal catheters. Adv Perit Dial 14:75–79, 1998
8. Lye WC, Kour NW, van der Straaten JC, Leong SO, Lee EJ: A prospectiverandomized comparison of the Swan Neck, coiled, and straight Tenckhoffcatheters in patients on CAPD. Perit Dial Int 16(suppl 1):S333–S335, 1996
9. Gadallah MF, Pervez A, el-ShahawyMA,Sorrells D, Zibari G, McDonald J,Work J: Peritoneoscopic versus surgical placement of peritoneal dialysiscatheters: a prospective randomized study on outcome. Am J Kidney Dis33:118–122, 1999
10. Pastan S, Gassensmith C, ManatungaAK, Copley JB, Smith EJ, HamburgerRJ: Prospective comparison of peritoneoscopic and surgical implantation ofCAPD catheters. Trans Am Soc Artif Intern Organs 37:M154–M156, 1991
11. Nielsen PK, Hemmingsen C, Friis SU, Ladefoged J, Olgaard K: Comparisonof straight and curled Tenckhoff peritoneal dialysis catheters implanted bypercutaneous technique: a prospective randomized study. Perit Dial Int15:18–21, 1995
12. Kim D, Burke D, Izatt S, et al.: Single- or double-cuff peritoneal catheters? Aprospective comparison.Trans AmSocArtif InternOrgans 30:232–235, 1984
13. Eklund B, Honkanen E, Kyllonen L, Salmela K, Kala A-R: Peritonealdialysis access: prospective randomized comparison of single-cuff and dou-ble-cuff straight Tenckhoff catheters.Nephrol Dial Transplant 12:2664–2666,1997
14. Eklund BH, Honkanen EO, Kala A-R, Kyllonen LE: Peritoneal dialysisaccess: prospective randomizedcomparisonof the Swan Neck andTenckhoffcatheters. Perit Dial Int 15:353–356, 1995
15. Ash SR, Janle EM:T-flutedperitoneal dialysis catheter.AdvPeritDial9:223–226, 1993
16. Moncrief JW, Popovich RP, Broadrick LJ, He ZZ, Simmons EE, Tate RA:The Moncrief–Popovich catheter: a new peritoneal access technique for pa-tients onperitoneal dialysis.TransAmSocArtif InternOrgans 39:62–65, 1994
17. Moncrief JW, Popovich RP, Simmons EE, Moncrief BA, Dasgupta MK,Costerton JW: Peritoneal access technology. Perit Dial Int 13:S112–S123,1993
18. Moncrief JW, Popovich RP, Oreopoulos DG, Dombros NV, Digenis GE:Continuous ambulatory peritoneal dialysis. In: Gokal R, Nolph KD, eds.Textbook of Peritoneal Dialysis, 1st ed. Dordrecht, The Netherlands: KluwerAcademic, 1994:357–398
19. Moncrief JW, Popovich RP, Seare W, Sorrels PA, Moncrief DB, Settle SM,Simmons E: Peritoneal dialysis access technology: the Austin DiagnosticClinic experience. Perit Dial Int 16:S327–S329, 1996
CHRONIC PD CATHETERS 333

20. Caruso DM, Gray DL, Kohr JM, Rodgers LL, Weiland DE, VanderWerfBA: Reduction of infectious complications and costs using temporarysubcutaneous implantation of PD catheters. Adv Perit Dial 13:183–189,1997
21. Stegmayr BG, Wikdahl AM, Arnerlov C, Petersen E: A modified lateraltechnique for the insertion ofperitoneal dialysis catheters enabling immediatestart of dialysis. Perit Dial Int 18:329–331, 1998
22. Prischl F, Wallner M, Kalchmair H, Povacz F, Kramar R: Initial Subcuta-neous embedding of the peritoneal dialysis catheter-a critical appraisal ofthis new implantation technique. Nephrol Dial Transplant 12:1661–1667,1997
23. Esson ML, Quinn MJ, Hudson EL, Teitelbaum I: Subcutaneously tunneledperitoneal dialysis catheters with delayed externalization: long-term follow-up. Adv Perit Dial 16:123–128, 2000
Erratum
Rajiv Agarwal: Systolic Hypertension in Hemodialysis Patients. Semin Dial 2003;16:208–213.
Due to a production error, the legends for figures 1 and 2 were transposed. The Publisher regrets the error. Thefollowing are the corrected figures and accompanying legends.
Fig. 1. Distribution of ambulatory systolic and diastolic hyper-
tension in chronic HD patients. Only 3% of the patients had isolated
diastolic hypertension. The major burden of hypertension in HD
patients is systolic. (Agarwal R, Lewis RR.Kidney Int 60:1982–1989,
2001.)
-20
-10
0
10
20
30
Pulse Pressure
Mean PressureA
djus
ted
rela
tive
% in
crea
se (
95%
CI)
inha
zard
rat
e as
soci
ated
with
10
mm
Hg
incr
ease
in P
ulse
Pre
ssur
e or
Mea
n A
rter
ial
Pres
sure
TotalMortality
CardiovascularMortality
CardiovascularEnd Points
Stroke Coronary EndPoints
Fig. 2. Mortality and cardiovascular morbidity in trials of
isolated systolic hypertension treated with dihydropyridine calcium
channel blockers (in Syst-Eur and Syst-China trial) or diuretics (in
European Working Party on High Blood Pressure in the Elderly
Trial). Data are adjusted for sex, age, previous cardiovascular
complications, smoking, and active treatment. Pulse pressure
analyzes are adjusted for mean arterial pressure and mean arterial
pressure analyzes are adjusted for pulse pressure, Data demonstrate
the predictive value of pulse pressure, but not mean arterial pressure,
in predicting cardiovascular endpoints in elderly patients. (Data
adapted from Blacher J, et al.Arch InternMed 160:1085–1089, 2000.)
Ash334