Embed Size (px)
Citation preview

Equity on the Path to UHCDeliberate Decisions for Fair Financing
Background Report (Conference Version)
Greater Equity for Better Health and Financial ProtectionWashington, D.C. • April 19–20, 2018

DRAFT:Notforattribution
1

DRAFT:Notforattribution
2
Thisisaforumpaper(conferenceversion)tothe“ThirdAnnualUHCFinancingForum:GreaterEquityforBetterHealthandFinancialProtection”.Thispapersetsthestageforthe
presentationsanddiscussionsattheForumandwaspreparedundertheguidanceoftheForumTechnicalWorkingGroup.Theinformationprovidedinthisdocumentdoesnotnecessarily
representtheviewsorpositionoftheorganizationsrepresentedontheTechnicalWorkingGroup

DRAFT:Notforattribution
3

DRAFT:Notforattribution
4
Section1:Introduction
In2016,theWorldBankGroupandUSAIDestablishedtheAnnualUHCFinancingForum,whichtakes
placeattheWorldBankGroup/IMPSpringMeetings.Thesemeetingsarestrategicplatformswhere
thousandsoffinanceanddevelopmentleadersfrommembercountriesdiscuss,analyzeanddebate
goalsforendingextremepovertyandboostingsharedprosperity.
TheUHCFinancingForumisembeddedintheselargerdiscussionstodivedeeplyintotheprocessesfor
acceleratingcountryprogresstowardsustainablefinancingofUniversalHealthCoverage—whichis
integraltoreachingtheSpringMeetings’largergoals.
Thisyearmarksthethirdtimeinwhichover400policymakersandotherexpertshaveconvenedto
analyzeandcriticallydiscussthehealthfinancingrealitiesthatcountriesface.Inoneoftheonlyglobal
spacesforthesenecessarydiscussions,participantsusetheforumtohelpshapeacollectiveagendafor
tacklingkeyfinancingchallengesposedbysomeofthetrickiestproblems.
TheThirdAnnualUHCFinancingForumexaminesequityforbetterhealthandfinancialprotection.It
complementsandbuildsonthetopicsandpapersofthe1stand2
ndforum,whichfocusedonhowto
generaterevenuestomeetfinancingneedsforqualityhealthservicesandfinancialprotection,andhow
touseavailableresourcesinthemostefficientway.
Eachyearourdebatesareinformedbyabackgroundreportthatexamineswhatworksanddoesn’t
work,whiletakingstockofwhatiscontroversial,innovative,ofhighimpactorinneedofclarity.
Thisyear,wetakeadifferentapproachbyaskingpolicymakerstoconsiderequitymoredeliberatelyin
theirhealthfinancingchoices.Whenpolicy-makersaimtoredressinequitiesinfinancingoutcomes,
theycandrawuponawell-establishedbodyofliteraturethatevaluatesandoffersguidanceonhowbest
toapproachpolicychoices.Butwhenpolicy-makerspursuestrategiestoaccelerateprogresstoward
UHC,theyseematalosstofullyconsidertheequityimplicationsoftheirfinancingdecisions.Oratleast
thatiswhattoday’sdeepinequitiesinhealthfinancingsuggest.Wethinkthat,perhaps,equityasa
criterionfordecision-makingisfallingthroughthecracks.
Placingtheblameonpolicymakerswouldmissthemark.ThemainproblemisthatprogresstoUHC
doesnotnecessarilyleadtoimprovementsforallandtheworse-off.This,wethink,isbecausepolicy-makersgrapplewithhowbesttoreachtheequitableendpointofUHCwhilealsoworkingonhigher
priorityobjectives,likeimprovingefficiency,overallpopulationhealth,employmentoreconomic
growth.Littleguidanceisavailabletohelpmanagedifficulttrade-offsbetweencompetingneeds.
Thispaperandthisyear’sforumaimtoclosesomeoftheinformationandguidancegaps,andfacilitate
thechangesnecessarytomoveequityconsiderationstotheforefrontofhealthfinancingpolicy
development.Weseethisasathree-prongedprocesswithafocusoni)identifyingpolicydecisionsthat
aredeemed“unacceptable”;ii)establishingwhatwecall“fairnessofprocess”indecision-making;and
iii)monitoringtheoutcomestohelpidentifywherepoliciesneedtobeadjustedforequity.
Theproposedframeworkbuildsonalargebodyofworkthathasexploredthemeaningofequityand
fairnessinhealthfinancingandfiscalpolicy.(e.g.,Wagstaff&VanDoorslaer2000;Murrayetal.2003;
Xuetal.2007;O’Donnelletal.2008;VanDoorslaer&O’Donnell2011;Bastagli,Coady&Gupta2012;
Ottersen&Norheim2014;Clements,Gaspar&Gupta2015;Mulenga&Ataguba2017;Fleurbaey&

DRAFT:Notforattribution
5
Maniquet2017;Wooetal.2017;Evanetal,2001).Morerecently,thisworkhasbeenappliedtoUHC
(WHO2014).However,noconsensushasdefinedtheboundariesandcontentoftheterms“equity”and
“fairness”andwhetherandhowtheyaredifferent.So,followingontheWHOConsultativeGroupon
MakingFairChoicesonthePathtoUHC,weusethetermsinterchangeablyinthispaper.(WHO2014).
Thescopeofourframeworkisbrokendownintothefollowingsections.
InSection2,wedescribethechallengesthatcountriesfaceastheyprogresstowardsUHCwhilealsostrugglingwithvastinequitiesinservicecoverageandfinancialprotection.
Section3mapsoutwhyhealthfinancingandtheoutcomestheyproducematter,andhowandwhy
policiesthatmakeUHCagoal—evenifit’sfarfromareality—areworthwhile.
Section4isreallythemeatofthisreport.Itidentifiesunacceptablepolicychoices,mapsout
approachestoestablishfairprocesses,anddiscussesthevalueofandneedformonitoring.
Section5outlineswhatcountriescandotofundamentallychangethewaytheyincorporateequity
concernsintotheirhealthfinancingpoliciesandstrategies.
Section2:SettingtheStageforUHC
In1978,theAlmaAtaDeclarationarticulatedanambitiousextensiontotheWorldHealthOrganization’s
constitutionbydeclaringprimaryhealthcareasabasichumanright.InwhatisnowKazakhstan,world
leaderssignedontonewoperatingprinciples,declaringthatallpeoplehadarighttopersonalhealth
andpublichealth,withaccesstotraineddoctors,nurses,midwivesandtraditionalhealers,andto
sanitation,cleanwater,essentialdrugs,immunizationsandmore.Andtheyproclaimedthatthese
servicesmustbeavailable“ascloseaspossibletowherepeopleliveandwork.”
Signatoriesgavethemselvesuntiltheyear2000—22years—andimploredactiononthepromisethat
healthforallwouldalloweveryonetoleadsociallyandeconomicallyproductivelives.
Now,40yearslater,wenotonlymissedthemark,butwemisseditbyawidemargin.Thegoodnewsis
thatthefastestprogresseverinextendinghealthservicecoverageoccurredduringtheeraofthe
MillenniumDevelopmentGoals.Thebadnewsisthat,atthecloseoftheMDGin2015,onlyabouthalf
theworld’spopulationenjoyedthebasicbenefitsenvisionedforallinAlmaAta.
ThenewtargetdateoutlinedbytheSustainableDevelopmentGoalsandtheWHOConsultativeGroupis
toreachUniversalHealthCoverage—withaccesstoservicesaccordingtoneedandwithoutfinancialhardship—by2030.Ifwearetotakethisseriously,countriesneedtobeontherightpathandstay
there.
Wehave12yearstodoalotofwork.Oneofthebiggesthurdlesisreplacingout-of-pocketpayments,
whichlimitaccessibility,withotherformsofhealthfinancing.Onlymodestprogresshasbeenmadein
reducingthesepayments,andnocleartrendshowstheiroverallburdenislightening.Tothecontrary,
everyyearapproximately100millionpeoplefallintopovertybecauseofout-of-pocketpayments.
Thetragedyisthatwehavefailed,eventhoughthemeansexisttomakehugeleapstowardUHCby
2030,andeliminatethepaymentconditionsthatknockthese100millionpeopleannuallyintopoverty.

DRAFT:Notforattribution
6
Multipleglobalestimatesshowthatthecostofapackageofessentialhealthservicesshouldrunno
morethan$90perpersonperyear.Globaldomesticpublicspendingstoodat$3.9trillionin2015,
enoughtofinancetheseessentialpackagesformorethan40billionpeople,oroversixtimestheworld’scurrentpopulation.
Theproblemiswehavevastlyinequitableinvestmentsinhealthfinancing,coverageandaccessto
services.Inthewealthiest5percentofcountrieswiththehighestpublicinvestmentsinhealth,the
averagespentonhealthperpersonis$4,600.Andforthetop10percentofcountriestheaverageis
$4,100perperson.
Butinthepoorest5percentofcountries,theaveragespentperpersononhealthisjust$4.Andforthe
bottom10percent,theaverageis$5perperson.Evenwhenadjustingforcostofliving,thedisparitiesin
healthinvestmentsarestunning.
Thebiggestchallengenowistofigureouthowtoboosthealthfinancingacrosslow-andmiddle-income
countriesinwaysthatmakehealthcoverageapriorityandareconsistentwiththegoalsofUHC.
Thisreport,andthisyear’shealth-financingforum,asksallparticipantstoseethispointintimeas
pivotal—asamomentoftruth.Ifcountriescontinueattheslowrateofprogressthatwesawinthelast
40years,wewillfailtoevencomeclosetoourgoalsby2030.
CountriesmustaccelerateprogresstowardsUHCbysystematicallytacklingfundamentalshortcomings
inhealthfinancing.Thisreportandthisyear’sforumhoneinonprovenandleadingedgeapproaches,
whichincludegivingprioritytotheworse-off(thesickestandthepoorest);reducingandultimately
eliminatinginequalitiesinhealthinvestmentsacrosscountriesandwithincountries;protectingpeople
fromfinancialruinlinkedtoOOPsbyphasingoutOOPsasameansforhealthfinancing;increasing
prepaidandpooledfinancing;andincrementallyincreasingguaranteedpackagessothatcoverageof
services,andtheirquality,improveforeveryoneovertime.
CountriesmustmakefasterprogresstowardUHC.Theinequitiesthatweseeglobally,however,exist
alsowithincountries.Ascountriesaccelerateprogress,theyruntheriskofdeepeningtheseinequities.
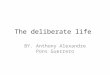
Figure1:Incidenceandinequalityinskilledbirtha7endance,Threshold:10%oftotalconsump6on(n=120countries)Inequali)es,
Concentra6onindex
SOURCE:HEFPI2018Database
Notes:Basedonlatestavailablesurveyyear;circlesizeispropor)onaltototalpopula)on
Popula)onincidence,%30 40 60 80 10050 70 900 10 20
0.3
0.2
0.0
-0.1
-0.2
0.1
0.4

DRAFT:Notforattribution
7
Onthebenefits,side,thenatureofthegameisthatthehigherthecoverage,thelowertheinequities.
Likewise,thehighertheaveragecoverage,thelessthevariation.Forexample,lookingatSkilledBirth
Attendance(SBA),aservicecommonlyincludedinessentialservicepackages,countrieswithservice
coverageabove80percent,haveconcentrationindiceslowerthan0.1.Incontrast,countrieswith
averageinservicecoveragebetween30and50percent,haveconcentrationsindicesbetween0.1(e.g.,
Indonesia)tocloseto0.5(e.g.,Nigeria).Theconcentrationindexmeasuresinequalitiesbysocio-
economicstatus(SES).Theindexrangesfrom-1to1,withzeromeaningnoinequalitiesincoverage
acrossincomegroupsinthiscase,andinequalitiesincreasingastheindexapproaches1.Byconvention,
pro-richinequalitieshavepositiveindices,whilepro-poorinequalitiesshownegativeindices.
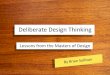
Whiletheconcentrationindexisanabstractconcept,theillustrationofcoveragebyincomequintile
providesabettersenseofthedepthoftheinequalities.Forexample,theconcentrationindexof0.47
forNigeriameansthatSBAcoveragewas87.5percentinthehighestincomequintile,butonly6.7
percentforthelowestincomequintile.
Figure2:Incidenceofskilledbirtha7endance:Nigeria(2014),%
6.7
18.8
41.6
64.1
87.5
0102030405060708090
Q1 Q2 Q4Q3 Q5
SOURCE:HEFPI2018Database
Incidence,%
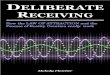
Figure3:Incidenceandinequalityincatastrophicpayments,Threshold:10%oftotalconsump6on(n=136countries)
SOURCE:HEFPI2018DatabaseNotes:Basedonlatestavailablesurveyyear;circlesizeispropor)onaltototalpopula)on,n
Inequali)es,Concentra6onindex
0.6
0.4
0.0
-0.2
-0.4
Popula)onincidence,%5 10 20 30 4015 25 350
0.2

DRAFT:Notforattribution
8
Source:Urquieta-SalomonandVillarreal,2016
Ontheburdenside,thepictureislessclear.Dataareonlyavailableforasmallersetofcountries.
Multiplemeasuresoffinancialprotectionexist,producingdifferentpatterns.Moreover,patternsneed
tobecarefullyinterpretedagainstinformationonservicecoverage.Forexample,adeclineinservice
coveragemayresultinreductionsofOOPexpendituressotheindicesoffinancialprotectionmightseem
toimprove.Nevertheless,weseedeepinequalitiesinmanycountries.Forthepurposeofillustration,
weusecata10consumption.Inmostcountries,inequalitiestendtobeoverwhelminglyconcentrated
amongthepoor.
Likeonthebenefitsside,theillustrationoftheincidenceoffinancialcatastrophe(inthiscasemeasured
asout-of-pockethealthexpendituresexceeding10%oftotalexpenditures,calledcata-10)byincome
quintileprovidesabetterillustrationofthedepthoftheinequalities.
Forexample,theconcentrationindexof37.39forIndiameansthattheincidenceofcata10wasin15
percenthigheramongthelowestincomequintilecomparedtothehighestquintile.
InequalitiesinUHCoutcomesoftenreflectdifferencesinthelevelofinvestmentorotherhealth
financingoutcomesandfunctions.Forexample,attheturnofthecentury,servicecoveragevariedin
Mexicosignificantlybetweenpeoplewithandwithoutsocialhealthinsurance.
Table1:Coverageofeffectiveaccesstopreventivehealthinterventions
Uninsured Insured
Skilledbirthattendance 88.91% 94.78%
Basicvaccinationschedule 71.39% 73.18%
Adultsover20withhighbloodpressure
control
47.73% 67.72%
Figure4:Incidenceandinequalityincatastrophicpayments:RepublicofKorea(2011)Threshold:10%oftotalconsump6on
37.4
17.212.8
8.25.7
0
10
20
30
40 Q1 Q2 Q4Q3 Q5
SOURCE:HEFPI2018Database
Incidence,%

DRAFT:Notforattribution
9
Whilecoverageforessentialservicessuchasmaternalandchildhealthwashighindependentof
affiliation,starkdifferencesprevailedinthecoverageofservicesfornon-communicablediseases(table
1).Effectivecoveragewithhighbloodpressurecontrolwas20percentagepointshigheramongthe
insured.
Similarly,thelikelihoodofthosewithsocialhealthinsurancetosufferfromcatastrophichealth
expenditures(frominpatientvisits)overayearwasfourtimeslower(Knauletal,2006).These
differencesinUHCoutcomescorrespondedtothelevelsofgovernmentfinancialcontributions.For
peoplewithsocialhealthinsurance,itwasfivetosixtimeshighercomparedtothecontributionsfor
governmenthealthservicesusedbytheuninsured.
Section3:TheGoal
ThedefinitionofUHCholdsthatallpeopleshouldreceivepromotive,preventive,curative,rehabilitative
andpalliativehealthservicescovered,basedonhealthneeds.Thoseservicesshouldbeofsufficient
qualitytobeeffective,whilealsoensuringthatpeopleareprotectedfromfinancialhardshipswhen
usingtheservices(WHO2010).
ThegoalofUHCexpandsontheconceptofqualityhealthcareforallasabasichumanright,asoutlined
intheWHOconstitution,theAlmaAtaDeclarationonHealthforAllandanumberofhumanright’s
treaties,addingprotectionfromfinancialhardship.
ThefirstcriticalpartofUHCisaboutbenefits,ensuringpeoplearecoveredbasedonneed.Healthy
people—thebetter-off—needlessservicesfromthesystem.Andunhealthypeople—theworse-off—
needmorefromthesystem.Thespectrumofneedshoulddeterminethebenefits,settingupservicesto
berenderedinanunequal,butequitableway.Thiswecallverticalequity;thehighertheneedthe
greaterthebenefits.Butcoverageshouldalsotreatallpeoplewiththesamehealthneedsequally,so
thateveryonewithkidneyfailureinneedofhemodialysisreceivesit(iftheywant).Thiswecall
horizontalequity;acrossanygivenneed,everyoneiscovered.
Butwithinhorizontalequityistheaddeddimensionofqualityoreffectivenessoftheavailableservices.
Theeffectivenessofthoseservicesisequallyasimportant.Thatis,servicecoverageandquality
combinedresultineffectivecoverage,orthecapacitytoachievethedesiredresults.
ThesecondpartofUHCisaboutfinancialburdens,ensuringpeopleareprotectedfromseverefinancial
hardshipwhenpayingout-of-pocketforhealthservices.Thesekindsofhardshipshavetwowidely-
accepteddefinitions:out-of-pocketpayments(OOPs)thatpushpeopleintopovertyordeeperinto
poverty,andOOPsthatarenotimpoverishingbutnonethelessprovecatastrophicforthehousehold
becausetheyleadtoexcessiveborrowingorassetdepletion,orcuttingbackonessentialneedslike
education,clothing,housingandfood.UHCisclearthatnooneshouldsufferthesekindsoffinancial
hardshipsfromOOPs.
Equity in UHC outcomes matter
UHCisimportanttoimprovinghealthandreducingpoverty.Weseethiswherepeoplelackaccessto
healthservices.Theyoftentakelongertorecoverfromanillnessorinjury,orneverrecover,leadingto
lossofincome.Incountrieswithsocialsafetynets,thiscanendupcostingmoreinservicesthanthe

DRAFT:Notforattribution
10
originaltreatmentwouldhavecost(thepenny-wise,pound-foolishproblem).Wherenosocialsafety
netsexist,healthcostsareknowntotumblefamiliesintopovertyandholdthemthere.Forexample,the
compoundingeffectsofpovertyforcefamiliestoforegothecostofeducation,eitherbecausetheyhave
nomoneyforthefeesortheyneedtheirchildrentostayhomeandhelpearnincome.Wherethesick
areexpectedtopayforhealthservices,familiesmayendupborrowing,incurringdebtthatcanget
passeddownfromgenerationtogeneration.
Werecognizethatsocialdeterminantsalsoplayanimportantroleinhealth.Thatis,peoplewithperfect
healthcoverageataffordablecostswholiveinacommunitywithgunviolencearestillsusceptibleto
beingshot.Butwherethetwomeet,iswhereUHCmakeshealthcoveragereliableandaffordable.
Peoplehavemoremoneytopayforotherthings,likebettereducation,nutritionandlivingconditions
(tomoveawayfromthegunviolence).Andthatcanimprovehealthoutcomesandhelpliftpeoplefrom
poverty,oratleastnotexacerbateit.
WeseeUHCasleadingtooutcomesthatreachbeyondthepopulation’soverallphysicalhealth,because
theyplayaroleinreducingfinancialstresses.Theexplicitpovertyaversionaspectofthisholdsthe
potentialofpositivelyripplingout.Thatis,inadditiontogroundinghealthsystemsintheidealthat
healthisahumanright—asmuchasdecentlivingconditionsare—equitablefinancingthatprotects
peoplefromeconomichardshipensuresthatthehealthsectorplaysnopartinincreasingpoverty.
Wealsoseethatreducinginequalitiesinhealthoutcomeshelpsreduceincomeinequalities.Andbetter
healthtranslatesintohigherincome.Thisistrueofhealthservicesandsocialdeterminantsofhealth.So
wehavetwostrands.Financialprotectionimprovesincomeinequality,andhealthoutcomesreduce
incomeinequalitywhenoutcomesimprovethehealthofthepoor.Weknowreducedincomeinequality
promotesgrowth,andthatincomeinequalityhasa“negativeandstatisticallysignificantimpacton
subsequentgrowth.”(Cinganro,F.,2014)
Importantlessonscanalsobelearnedfromseveralhigh-incomecountriesthattodayfacegrowing
inequitiesinhealthoutcomesandincreasingratesofpoverty,andthathavecorrespondingerosionof
socialcohesion,advancedpoliticalpolarization,andslowereconomicgrowth.(IMFFiscalMonitor,
October2017)Closingthesegapsshouldbethegoalofallcountries,andhealth-financingchoicescan
help.
Dramaticglobalhealthsecuritylessonsalsocanbelearnedfromlower-incomecountriesthathavebeen
unableorunwillingtoworkequitablytowardUHC,orotherwisestrengthentheirentirehealthsystems.
Intheseplaces,infectiousdiseasesspreadmorerapidlyinareaswithweakcorepublichealthfunctions,
sometimesindramaticwaysthatputimmensefinancialandpoliticalstressontheentireglobalhealth
system.The2014EbolaoutbreakinWestAfricaservesasoneofthemostrecentacuteexamples.We
canbegintohead-offthesekindsofoutbreaksbybringingequitytohealthfinancingsothathealth
systemsare,attheveryleast,abletodeliverbasicdiagnosticanddiseasesurveillancetoolseverywhere.
Journeying to UHC
AchievingUHCisthegoal.Butnocountryisallthewaythere,withcompletecoverageofhighquality
servicesthatareaccessibleandaffordableforall.Somewealthycountriescomeclosewithrelatively

DRAFT:Notforattribution
11
largeguaranteedcoveragepackagesthatincludeabroadrangeofhealthservicesavailableforloworno
out-of-pocketpayments.
Formanycountries,however,UHCisinthedistantfuture.Toofewcanaffordthesuiteofhealth
interventionsthatareknowntoprolongandimprovelife,whilealsoensuringfinancialprotectionforall
users.ThegoalforthemistoseeUHCasajourney,tostartwithatleastasmallerguaranteedpackage
withabaselineofessentialservicesthatareavailabletoall,ofequalqualityforallandaffordable.Then,
overtime,thesizeandscopeofthepackagesshouldexpand—allthewhilekeepingasagoal
improvementsinequitability,availabilityandaffordabilityofservices.Bystartingoutsmall,these
countriesarestrategicallyandtacticallysetuptocontinuethejourneytoUHC.
Signposts show the way
CountriesthathavesetUHCasatargetandmadetheobligationtoprogressivelystayonthejourney,
however,areunabletolooktotheUHCgoalsforguidanceonmakingpolicychoicestohelpkeepthem
oncourse.Indeed,assomecountriesmadeprogressonservicecoverageoverall,inequitieswidened.
Andduringtimesofcrisis,servicecoveragedroppedandfailedtoprotectthepoor.
SoUHCshowstheobjectiveofthejourney,nothowtogetthere.Weattempttofillsomeofthosegaps
inguidancebyofferingpolicy-makerswhatwecallsignposts.Theyaredesignedtoprovidenecessary
directionsforstayingoncourse.
Onthebenefitsside,UHCrequiresdistributionofhealthservicesaccordingtoneed.Ontheburden
side,financingsystemsthereforecannotputupfinancialbarriertoaccessthebenefits.Andthatis
wherehealthfinancingofUHCextendsbeyondfinancialprotectiontoprovidingservicesregardlessof
theabilitytopay.Sothesetwocomponentshavetobeseparated.
Wecallitdecoupling.Policy-makersforUHCmustdevelopauniversalguaranteedcoveragepackage
accordingtotheircountry’sfinancingcapacities.Whatisincludedinthepackagewillbebasedon
Inequali)es,Concentra6onindex
Figure5:Servicecoveragevs.inequality,Concentra6onindex(-1=skewtopoorto1=skewtorich)
0.3
0.2
0.1
0.0
-0.1 30 40 50 60 70
Servicecoverage,%
SOURCE:WorldBankHEFPI2017

DRAFT:Notforattribution
12
whatevercountryfinancingwillallow,startingwithacoresetofhealthservicesandexpandingitover
time.
Onaseparatetrackpolicy-makersmustraisethefinancing.Butthismustbedoneinawaythatremoves
thefinancialburdenforpeoplewhoareunabletopay.Theonlywaytodothisisthroughprepaidand
pooledfinancing.Inpractice,thismeanspublicfinancing--taxesandcontributionstosocialhealth
insurance.Tosubsidizethepoor,andthosewithlargehealthneeds,publicfundsshouldingeneralbe
raisedbasedontheabilitytopaywithsomedegreeofprogressivity,thatis,therichercontributea
highershareoftheirincome.
Socountriesestablishaguaranteedpackagewithhealthservicesthatareavailabletoallatan
affordableprice(UHC).Whoutilizestheservicesisseparatedfromwhopaysforthem.Utilizationis
basedonhealthserviceneed.Payingintoprepaidandpooledsystemsisbasedontheabilitytopaywith
OOPsminimized.
ThisprovidestwoguidepostswhendevelopingpoliciestowardUHC:healthservicesaccordingtoneed
andcontributionstoprepaidandpooledfinancingbasedonabilitytopay.Twotrackswithseparate
directionsforstayingonthepathtoUHC.
OnthejourneytoUHCcomefurtherconsiderationswithinthesetracks.Thereisbroadconsensusthat
someprioritymustbegiventotheworse-off.Onthebenefitsside,thismeansgivingprioritytothe
sickestandthosewiththelowestservicecoverage;ontheburdenside,thismeansgivingprioritytothe
poor.1Inthisway,UHCdirectspolicy-makerstopayspecialattentiontothemostdisadvantaged
segmentsoftheirpopulations,andmakedecisionsdesignedtoreachthem.
Incountrieswithlittlepotentialforraisingenoughprepaid,pooledfundstocoverabroadsuiteof
healthservices,effortshavefocusedonidentifyingpackagesofsufficientserviceswithguaranteed
accessandfinancialprotectionwithinthelimitationsofavailablepublicfinancingandservicedelivery
capacities.ThesepackagesconstitutethestartingpointfortheprogressiverealizationofUHC.Decision-
makersthenfacethechallengeofdefiningwhatis“sufficient”inabasicpackage,andwhatshouldbe
addedasthepackageexpandsovertime.
ThechallengescountriesfacestayingonthepathtoUHCaremany.Thefollowingarefourinterrelated
butdistinguishablechoicesthatmakepolicydecisionsdifficult.
First,theprinciplesofbenefitsandburdenarenotabsolute.Forinstance,withrespecttobenefits,
shouldcountriesgiveprioritytoexpandingtherangeofservicesavailabletoall,basedonneed,or
shouldtheyfocusonimprovingthequalityofexistingservices?Likewise,ontheburdenside,shouldthe
principleofabilitytopaybeinterpretedastherichpaymorethanthepoororthattherichpayahigher
proportionoftheirincomesthanthepoor?Eveniffaircontributionsareunderstoodasthelatter,i.e.
progressivecontributionswheretherichpayahigherproportionoftheirincome,policymakersmust
stilldeterminehowmuchmoretherichshouldpay.
1
Oneformalizationofthisapproachisinherentintheidealsofprogressiveuniversalism,whichdictatethatateverystageon
thepathtoUHC,topoor—whoasagroupareinthemostneedofhealthservicesandfinancialprotection—shouldbenefitat
leastasmuchastherich.

DRAFT:Notforattribution
13
Second,decisionsoftenpitbenefitsagainstburden.Often,decision-makershavetodecidebetweenthe
twocompetinginterests:expandingandimprovinghealthservicesontheonehand,andextending
financialprotectionontheother.Shouldcountriesprioritizetheexpansionofeffectiveservicesfor
thosewiththegreatesthealth-serviceneeds,ortheextensionoffinancialprotectiontothosewiththe
leastabilitytopay?Moreover,ifcountriesdecidetofocusonamixofhealthserviceexpansionand
financialprotection,howmuchweightshouldbegiventoeachcomponent?And,ofcourse,theyhaveto
figureouthowtopayforeverything—whichcirclesbacktothefirstdifficulty.
Third,prioritizingtheworse-offrequiresdata,whicharescarce.Whilemanycountriesaresettingup
systemstoidentifytheworseoff,lackofsufficientsurveydatahasmadeidentifyingthosewithgreater
healthcoverageneedsandlowestactualcoveragedifficult.Oneansweristofocusfirstonuniversal
coveragetocastawidenetthatcoversabasicsetofservicesthatreacheveryone,includingtheworse-
offandpoorestpeople.Thisensuresthatthepoorgainatleastasmuchasthebetter-offduringservice
coverageexpansions,onthewaytoUHC.
Thefourthdifficultyweseeis,perhaps,thetrickiest.Thisiswhenpolice-makersmustdecidebetween
improvingequityinhealthfinancingandreachingothersocialgoals—suchasstimulatingeconomic
growthorraisingadditionalrevenuerapidly.Thisisthefocusofthenextsection.
Section4
ChartinganequitablepathforwardinfinancingUHCincludesthreepolicyanglesthatthispaperdefines
andofferssuggestionsfor.Thefirstisidentifyingunacceptablepolicychoicesthatshouldbeavoided.Thesecondisestablishingcriteriaforfairprocessesthatwillengagethepublicandkeeppolicydecisionsoncourse.Andthethirdismonitoringimpactsbyusingavailabledatatohelpinformpolicy
choicesandleadtoequitableoutcomes—notexacerbateexistinginequitiesorleadtonewones.
UnacceptablePolicyChoicesinFinancingUHC
Decisionsthatdeepeninequitiesinhealthfinancingneedtobeidentifiedandavoidedascountries
moverclosertoUHConaggregate.Broadlyspeaking,an“unacceptablepolicychoice”isonethatcreates
orexacerbatesanexistingunfairinequalityandcannotbejustifiedbytrade-offsagainstotherpolicy
objectives.Herewearetalkingaboutincrementalpolicychoiceswithinthethreehealthfinancing
functions:revenuegeneration,poolingandpurchasing.
WearrivedattheseunacceptablepolicychoicesbybuildingonthelogicoftheWHOConsultativeGroup
onEquityandUniversalHealthCoverage,whichfocusedonfairchoicesintheprioritizationofservicesin
theprogressiverealizationofUHC.Here,welookmorebroadlyatfinancingUHC.
WhileexaminingoptionsforimprovingUHCoutcomes(everyonegetsthehealthservicestheyneed,of
goodquality,andwithfinancialprotection),weidentifiedpotentialinequalitiesamongindividualsand
groups(differingbyincome,gender,geographicregion,ethnicorigin,affiliationwithpooling
arrangements,legalstatusofresidency,andhealthordiseaserelatedproblem).Wethendrilleddown
tounderstandtheinequalitiesacrossthethreehealthfinancingfunctionsthatcontributetoinequalities
inhealthoutcomes.

DRAFT:Notforattribution
14
Fromthereweestablishedprinciplesoffairnessinthedistributionofbenefitsandburdens,basedon
thevaluesinherentinUHCandthemorewidelyacceptedprinciplesoffairnessandequity.Wethen
scrutinizedtheinequalitiesinUHCoutcomesandthoserelatedtoeachhealthfinancingfunction;
measuredthoseinequalitiesagainsttheprinciplesoffairness;determinedwhethertheywere
inequitable(i.e.inequalitiesthatareinherentlyunfair);identifiedpolicychoiceslikelytodeepen
inequities,andconcludedthatsuchchoices—unlessjustifiedbytheneedtopursueotherpolicy
objectives—are“unacceptable”.
Thepolicychoicesthatwedeem“unacceptable”inallthreefinancingfunctions,basedontheapproachdescribedabove,meettwocriteria:
1) TheydeepeninequalitiesidentifiedasunfairintheUHCprinciplesforbenefitsandburden.
2) Theycannotbejustifiedbytheneedtopursueotherpolicyobjectives.Examplesinclude
stimulatingemployment,maximizingrevenues,controllinginflation,orstimulatingeconomic
growth.
Bothcriteriainvolvevaluejudgmentsthatreasonablepeoplecandebate.Whatwefocusonispolicy
decisionsthatincreaseinequity,butthatcannotbejustifiedbyotherpolicyobjectivesthatoffer
counterbalancingtrade-offs.
TenUnacceptableChoices
Thefollowingareten“unacceptable”choices,byhealthfinancingfunction(revenuegeneration,pooling
orpurchasing)outlinedintable1ofAnnex1
Thefirstthreeunacceptablechoicesrelatetorevenuegeneration,whichisdefinedasraisingfinancialresourcesneededtodevelopandrunahealthsystem.
Broadconsensusisthatguaranteedservicesmustbefinancedlargelywithcompulsoryprepaid
resourcesandnotout-of-pocketpayments.Thisprovidesbetterfinancialprotectionandpreventsthat
tumbling-into-povertyeffectthatOOPstoooftencause.Wearguethattheequitabilityofhowthese
prepaidfundsareraisedmattersonlytotheextentthatthechoicesaffectthefairnessoftheentire
publicfinancingsystem,includingbothcontributionsandexpenditures.Soweseehealthfinancingasa
partofpublicfinancing—fromindividualtaxrevenuestofirmsthatpaydedicatedtaxesordirectlyfund
employeehealthservices.Howrevenuesareraisedandspent,onthewhole,iswhatmattersmost.
UnacceptablechoiceNo.1:Raiseadditionalrevenuesforhealththatmakecontributionstothepublic
financingsystemlessprogressivewithoutcompensatorymeasuresthatensurethatthepost-tax,post-
transferdisposableincomedistributionisnotlessequal.

DRAFT:Notforattribution
15
Atfirstglance,thePhilippines’2012decisiontoraiseamajorityofrevenuesforthenationalinsurance
programthroughtaxesontobaccoandalcoholmighthavebeenseenasanunacceptedpolicydecision
becausesintaxesareknowntoberegressive.2However,thegovernmentusedaportionofthetaxesto
payhealthinsurancepremiumsforthebottom40percentofthepopulation(Kaiseretal,2016).From
2012to2014,theprogramexpandedhealthinsurancecoverageamongthepoorto14.71million
households,upfrom4.61million—a300percentincreaseinjusttwoyears.
Datahasyettobecomeavailabletoconfirmthattheexpansioncounter-balancedtheregressivityofthe
taxmeasure.Butresultsfromothercountriesthathavemadesimilarchoicesareencouraging.For
example,Indonesiareliesheavilyonregressivetaxestoraiserevenue,butthenetfiscalincidenceis
progressivethroughmostlyin-kindtransfersforhealthandeducationforthepoor(Jellemaetal,2017).
Thecountryhassinceseenadeclineinincomeinequities,asmeasuredbyadropintheGINIcoefficient
from0.394to0.370(whichmeasureschangesonscalefrom0to1,with0indicatingperfectequality
and1beingperfectinequality.
UnacceptablechoiceNo.2:Increaseout-of-pocketpaymentsforuniversallyguaranteedpersonalhealth
serviceswithoutanexemptionsystem3orcompensatingmechanisms.
Debatesoverout-of-pocketpaymentsariseintwocategoriesofcountries:thepoorestandthosein
crisissituations.Extremelypoorcountrieswithlimitedresourcesfacethemostdifficulttrade-offs.Their
limitedoptionsforraisingfinancescanhemthemintouserfees,iftheyseenootherpathtofinancing
government-sponsoredhealthservices.Doministriesofhealthrelyonuserfeesorletservicedelivery
falter(withnomedicinespurchasedtorestockshelves,nonewhealthworkerstofillshortages,andno
capitaltorepaircrumblinghealth-relatedinfrastructure)?Withlittleevidencethatexemptionsystems
work,mostlookforalternativefinancingmechanisms.
Eveninhigher-incomeOECDcountries,whenfacedwiththe2008financialcrisis,one-thirdofthem
(includingGreeceandIreland)introducedorincreaseduserfeestoshoreuphealthfinancingshortfalls.
Greeceoffersaparticularlyvividexampleofwhatcanhappenwithoutexemptionsforthepoor.There,
userfeeswereincreasedforoutpatientcare.Buteventhoughsomevulnerablegroupswereexempted
fromthecharges,unforced4unmetneedforhealthservicesincreasedfrom7.5percentto11.7percent
forthepoorestpeople(OECD,2015andEuropeanCommission,2013).
2Tobaccotaxesareregressiveintheburdenspacesincesmokingprevalenceisconsistentlyfoundtobehigher
amongthepoor,theycontributeadisproportionallyhigherproportionoftheirincomestothesetaxesthanthe
rich.Ontheotherhand,theimpactofthesetaxesisprogressiveinthebenefitsspace–thepoorgain
disproportionallymorethantherichintermsofsubsequenthealthbenefits(Summers,2018).
3
Giventhelimitedevidence-baseinsupportofsuchpolicies,proofthatthesesystemsandmechanismsiscritical4
Unforcedunmeetreferstotheproportionofpeoplewhoreportanunmetneedforhealthcareduetothree
reasons:(i)affordability,(ii)waitinglist,and(iii)distancetohealthfacility/nomeansoftransport

DRAFT:Notforattribution
16
UnacceptablechoiceNo.3:Raiseadditionalrevenuesforuniversallyguaranteedpersonalhealthservicesthroughvoluntary,prepaidandpooledfinancingarrangementsbasedlargelyonhealthstatus,
includingpre-existingconditionsandriskfactors.
Countrieswithnoorlimitedgovernment-sponsoredservicepackagesrelyonprivatehealthinsurance,
whichhavebeenknowntosetpremiumsbasedonvariablessuchasage,genderandpre-existinghealth
conditions.Thesepremiumschedulesmakeinsuranceunaffordableforthosewhoarepoorandsick.
Peopledon’tgetcareaccordingtoneed.Yet,somecountriesencouragesuchcoveragethroughtax
exemptions.
Thenextthreeunacceptablechoicesrelatetopoolingresources,whichmeansspreadingcontributions
acrossindividualsandgroupsinawaythatreducesthefinancialriskassociatedwithmedicalexpenses.
Healthsystemstendtobehighlyfragmentedintopoolsoffundsforhealthfinancingschemes,
administrativeterritorialunits,orhealthprograms.Healthfinancingschemesarethefinancing
arrangementsthroughwhichhealthservicesarepaidforandobtainedbypeople.Examplesinclude
nationalhealthservices,socialhealthinsuranceandvoluntaryinsurance,includingcommunity-based
healthinsurance.Administrativeterritorialunitswithinhealthfinancingschemesmayconstitute
separatepools,wherelowerlevelsofgovernmentareresponsibleforservicedeliveryandreceive
transfersfromhigherlevelsofgovernmentandsometimesalsoraiselocaltaxesandotherrevenues.
Financingsystemsmaybefurtherfragmentedintoprogramsthattargetcertainpopulationsand
diseases,withring-fencedfundinginlessdevelopedcountries,oftenco-financedfromDAH,whether
passingthroughgovernmentbudgetsoradministeredseparately.
Theproblemsweseearelargelyassociatedwithallocatingpublicmoniesinawaythatmakesexisting
inequitiesintheavailabilityoffundsperpersonacrosspoolsworse,thatis,inequalitiesinthe
availabilityoffundsunlesstheyarejustifiedbydifferentneeds.Inequities,though,mayalsoarisefrom
exclusionbecausepeopleareineligibleorfaceotherbarrierstotheirparticipationinpools.
UnacceptablechoiceNo.4:Changepercapitaallocationsoftaxrevenue5ordonorfundsacrossprepaidandpooledfinancingschemesinwaysthatexacerbateinequities,unlessjustifiedbydifferencesinneed
ortheavailabilityoffundsfromothersources.
Priorto2003,Mexicohadthreemajorfinancingschemes,twoofthemsocialhealthinsuranceschemes
paidforbyemployeeandemployercontributions.Andthethird,paidforthroughgeneralgovernment
revenues,servedtheuninsured.Thetwosocialhealthinsuranceschemesspentnearlyfivetosixtimes
morepercapitaonbeneficiariesthanthegovernment-fundedprogram.(WorldBank,2012).
5
Taxrevenueexcludessocialhealthinsurancecontributions

DRAFT:Notforattribution
17
Whenthetwoemployment-relatedschemesfacedshortfalls,theyreceivedbailoutmoneywithno
increasesinallocationtothethirdscheme.So,ineffect,thetwoplansservicingwealthierpeoplewith
broaderpackagesweregivenadditionalresourcesfromthesamepotofmoneythatunderfundedand
providedfewerservicestothegeneralpopulation.Theseallocationsdeepenedinequitiesandwerenot
justifiedbyanyotherpolicyobjectives.
MexicorectifiedtheentirefundinglevelsbylaunchingtheSocialProtectionSysteminHealth(SPSS),
widelyreferredtoasSeguroPopular.Thisprogramdirectsfederalandstatecontributionstoincrease
financingforthenationalhealthscheme,sothatthepercapitaspendingisnowmoreeven.
UnacceptablechoiceNo.5:Withinfinancingschemes,changepercapitaallocationsfromhigherto
loweradministrativelevelsinwaysthatexacerbateinequities,unlessjustifiedbydifferencesinneedor
theavailabilityoffundsfromothersources.
Infederalsystems,centralgovernmentstypicallytransferblockgrantstosubnationalentities.InNigeria,
thesizeoftheseblockgrantsislargelydeterminedbywhatiscalled“principleofequality,”whichmeans
allstatesreceiveanequalshareoftherevenues(WorldBank,forthcoming).Population,size,levelof
socialdevelopment,andfiscalcapacityplayonlyminorrolesindeterminingeachstate’sshare.6This
formulaforresourceallocationalsofailstoaccountforthelargevariationsinrevenuegeneratedbythe
states.7
Undertheassumptionthatallstatesgivethesameprioritytohealth,disparitiesinavailablerevenues
leadtosignificantinequalityinpercapitaallocationsforhealth.Moreover,poorerstateswithsmaller
overallbudgetsoftentendtogivelowerprioritytohealthdespitehigherneeds,furtherexacerbating
inequalities.
Toaddressthisproblem,thegovernmentproposedtheBasicHealthCareProvisionFund(BHCPF),which
seekstorectifythedifferencesbyofferingadditionalfinancingtostatesproportionaltotheir
populations.Thefundsarechanneleddirectlytofrontlineserviceswiththeaimtoexpandcoveragewith
theBasicMinimumPackageofHealthServices.
Thenextfourunacceptablechoicesrelatetopurchasing,whichisconcernedwithdecisionsmadeon
whatandhowtopayfor,includingservicesandinputs(coveringhumanresources,equipment,supplies
andinfrastructure).
Herewemakethreeprincipledistinctions.First,wedifferbetweenpersonalhealthservices(suchas
treatment,rehabilitation,palliationaswellaspreventionandpromotionatthepersonallevel)andnon-
6
Forinstance,populationestimatesonlyaccountfor25.6%oftheformula.7
StategeneratedrevenuesrangefromNRA1000percapitainNigerstatetoNRA25000percapitainLagos

DRAFT:Notforattribution
18
personalhealthservices(suchasessentialpublichealthfunctions,includingpopulation-based
preventionandpromotionaswellassystemgovernance).
Amongpersonalhealthservices,wedistinguishbetweenentitlementsandtheservicesthataredefacto
available.Ontheentitlementside,forexample,socialhealthinsuranceservicepackagestypically
guaranteefortheformalsectorabroaderrangeofservicesthanthoseguaranteedbygovernment
fundingorinsuranceschemesdesignedspecificallyfortheinformalsectororthepoor.Onthe
availabilityside,guaranteedhealthbenefitspackagesareinprincipleavailabletoeverypoolmember,
but,inreality,contractingandpaymentsystemsmaynotmaketheseservicesavailableforeveryone.
Finally,forservicesthatareactuallyavailable,wemustlookatkeyinputs(humanresources,medicines,
othersupplies,equipmentandinfrastructure)Thedefactoavailabilityofserviceshingesontheactual
availabilityoftheseinputs,whichoftendiffersinqualityandrangeacrossurbanandruralareas.
UnacceptablechoiceNo.6:Withinschemesorpools,changeallocationsoffundsacrossdiseasesin
waysthatexacerbateinequities,unlessjustifiedbydifferencesinneedortheavailabilityoffundsfrom
othersources.
Acommonexampleiswheregovernmentsincreasefundingforparticulardiseaseprogramsthatare
alreadywell-fundedthroughexternaldonorfinancing,perhapsaspartofcounterpartfunding
requirements,leavingotherdiseasesprogramsaddressingpriorityhealthproblemswithseverefunding
shortages.
UnacceptablechoiceNo.7:Introducehigh-cost,low-benefitinterventionstoauniversallyguaranteedservicepackagebeforeachievingclosetofullcoveragewithlow-cost,high-benefitservices.
Inmanycountries,publicsectorresourcesaredirectedtowardshospitalizationbenefitsbeforefull
coverageofbasichealthserviceisachieved.Forexample,in2008,IndialaunchedtheRashtriya
SwasthyaBimaYojana(RSBY)toprovideinsurancecoveragetohouseholdslivingbelowthepovertyline.
RSBYismeanttoaddressthehighincidenceofOOPsamongthepoor.Theschemeoffershospitalization
benefitswithcompletecoverageinbothprivateandpublichospitals,whichwouldpreviouslyhavebeen
inaccessibletothepoor.Theprogramhasenrolledover36millionhouseholdslivingunderthepoverty
line(RSBY,2018).
WhileRSBYsignificantlyimprovedfinancialprotectionfromhospitalizationamongthepoorest,itdidnot
addresstheneedforlow-costinterventionslikeprimaryandpreventivecare.Toaddressthisgap,the
governmentsimultaneouslyexpandedsignificantresourcesdirectedtowardstheNationalRuralHealth
Mission(NRHM)throughConditionalCashTransfers(CCTs)andcommunityhealthvolunteers.Andin
February2018,thegovernmentalsoannouncedtherolloutoftheNationalHealthProtectionScheme

DRAFT:Notforattribution
19
(NHPS),whichwillincludeinpatientandoutpatientcare,andbuild150,000newhealthandwellness
centerstoincreaseaccesstocareinunderservedareas.
UnacceptablechoiceNo.8:Increasetheavailabilityandqualityofpersonalhealthservicesthatareuniversallyguaranteedinwaysthatexacerbateexistinginequalitiesunlessjustifiedbydifferencesin
need.
Governmentstendtoprioritizeinvestmentsinhospitalinfrastructuretoensureaminimumaccessto
life-savingservicesaswellastotraintheirfuturehealthworkers.Thesehospitalstendtobe
concentratedinurbanareas,whilepeopleinruralareasoftenlackaccesstothemostbasicservices.
UnacceptablechoiceNo.9:Increasetheavailabilityandqualityofcorepublichealthfunctionsinwaysthatexacerbateexistinginequalitiesunlessjustifiedbydifferencesinneed.
Priorto2013,Brazilhadhugedifferencesinthedensityofskilledhealthprofessionals.Thiswaslargely
becausethedecentralizedsystemthatallowedsub-nationalentitiestosettheirownsalariesfor
physicianshadinadvertentlycreateddisincentivesfordoctorstoworkinareaswheresalarieswere
lower.WealthierstatesandcitiesinBrazilthatpaidhigherwagesendedupwithahighernumberof
physicians,whileotherpartsofthecountryexperiencedsignificantshortages.
Acrossthecountrymorethan20percentofmunicipalitieshadashortageofphysiciansinpublicsector
facilities,whilemorethan10percentofmunicipalitieshadnodoctorsatall.ThepooreststatesofBrazil
hadthehighestshortageofhealthworkers,forcingpatientstorelyonnurse-associatesandcommunity
healthworkerswithrelativelylowerlevelsofhealthtraining.(Ref:MonitoringInequalitiesintheHealth
Workforce:TheCaseStudyofBrazil1991-2005,PLOS1,2012).
Then,in2013,Brazillaunchedthemaismedicosprogram,whichofferedfinancialandcareer
advancementincentivesfordoctorstoacceptpostsinunderservedlocations.Thisnewpolicyaddressed
significantdisparitiesinthedistributionofphysiciansinthecountryandmadethecountry’sallocations
forstaffacceptable.
UnacceptablechoiceNo.10:Increasetheavailabilityandqualityofcorepublichealthfunctionsinwaysthatexacerbateexistinginequalities,unlessjustifiedbydifferencesinneed.

DRAFT:Notforattribution
20
Failurestopreventtherapidspreadofthe2014Ebolaoutbreakgrewoutofseveralweaknessesin
Liberia’shealthsystem.Thecountry’slimitedsurveillancecapacitytoidentifyandreportanoutbreak
wasconcentratedinurbanareas,andalmostnon-existentinruralareas,whereEbolawasspreading
fast.ThispostponeddetectionofthediseaseuntilitwasfinallydiagnosedforthefirsttimeinMonrovia.
Skewingresourcestocitiesallowedadeadlyvirustokillpeoplebeforeitwasfinallydetected.
Sincethen,Liberiahasmadesignificantinvestmentsinstrengtheningcorepublichealthfunctions,while
addressingexistinginequalitiesincommunity-levelsurveillanceanddiseasereporting.Theresultshave
alreadybeenfelt.Duringthe2018Lassafeveroutbreakthere,CommunityBasedEventSurveillance
reportingshowedmarkedimprovementswithcompletenessandtimelinessofreporting.Healthofficials
estimatedthatnearlyallLassacaseswerereported.
Fairnessofprocessandaccountability:Aframeworkformakingdecisions
Certainprocessesmustbeestablishedtoclaimfairnessandaccountabilityinpolicymaking.Thisisas
trueinhealthpolicyasitisinanyotherareaofsocialpolicy.Werecognizethatcompleteagreementon
the“fairness”oftheoutcomesofpolicydecisionsisunachievablebecausepeople’sperceptionsofsocial
justicevary.Butwecanagreeonafairprocessformakingthosedecisionsthatthepublicseesas
legitimate.Sopublicparticipationandsomelevelofaccountabilityarenecessary,becausetheyhelp
leadtodecisionsthatcreateageneralsenseoffairnessintheprocess,eventhoughsomepeoplemay
disliketheoutcome.
Hereweteaseoutdifferentstrandsofhealth-financing-relateddecisionsastheyrelatetopublic
involvementandaccountabilityforreasonableness.
Thesefirsttworefertopublicinvolvementandpurchasingdecisions(whattobuy):
• Publicinvolvementinmakingone-offdecisionssuchaswheretolocateanewhealthcenter
oftentakestheshapeofopendiscussionsordebateinconsensusconferences,townmeetings,
orcitizenjuriesorpanels.(Rowe&Frewer2005;Abelsonetal.2008;Mittonetal.2009;WHO
2014).
• Publicinputstolonger-termdecision-makinghave,insomecountries,beenformalizedthrough
representationonbodiessuchashospitalboards,localgovernmenthealthauthorities,priority-
settingcommitteesandinstitutions,ortheboardsofhealthinsurancefunds(Sabik&Lie2008;
Glassman&Chalkidou2008;Stewartetal.2016;Byskovetal.2017;Giedion&Guzman2017;
Simonet2017).
Thesenexttworefertopublicinvolvementandallocationdecisions(howtospend):
• Furtherupstreaminfinancingfunctions,citizenshavebeeninvitedtoparticipateinformal
decisionsonhowtoallocategovernmentbudgetsacrosscompetingneeds.Thishashappened

DRAFT:Notforattribution
21
inplacesasdiverseasBrazil,Cameroon,Europe,Peru,SriLankaandNewYorkCity(WHO2014;
Kasdan&Markman2017).
• Lessdirecteffortsbycivilsocietyorganizationsinclude,forexample,theAfricanHealthBudget
Network.Thisnetworkofgroupshasinfluencedgovernmentallocationstohealththrough
advocacyandbyencouragingAfricangovernmentstoadheretotheagreementmadeinAbuja
Declarationof2001toallocate15%oftheirbudgetstohealth(AfricaHealthBudgetNetwork
2018).
Thesekindsofcitizenengagementcaninfluencedecisions,thoughtheyareonarelativelylimitedscale.
Forexample,withformaldecisions,citizeninvolvementinbudgetinghasbeengenerallylimitedtolower
levelsofgovernment–e.g.municipalities–andusuallyrestrictedtoarelativelysmallproportionofthe
budget(Shapiro&Talmon2017).Withone-offdecisions,limitedevidencesuggeststhatthingslike
townmeetingsandjuriesinfluencethepublic’ssenseofinclusion,eitherwithrespecttothequalityof
publicdebateortheresultingdecisions.Andthoseonhospitalboardsorcitizenpanelstendtobewell
educatedandmaybelimitedintheirabilitytoreflecttheviewsofthebroadercommunity(Campbell,
Craig&Escobar2017).
Thesefinalpointsrefertotheneedforaccountability(transparencywithfairprocess):
Answerabilityandenforceabilityarefundamentaltoaccountability.Sodecisionsthataffectthe
population’swellbeingmustbetransparentandjustified.Andindividualsandinstitutionsengagedin
fraudorothermisconductmustfacecensureorsanctions,perhapsbackedbythejudiciary(Schedler
1999;WHO2014,Gruskin&Daniels2008;Rumboldetal.2017;Yamin2017).
Acommonmotivationforestablishingaccountabilitycomesfromthehumanrightsframework,which
seestheStateasactingonbehalfofitscitizens(Yamin2000;Farmer2003).Informedpublicscrutiny,in
turn,requiresareliablemonitoringsystem,meaningfulpublicparticipationinprocesses,and
transparencyandaccesstoinformation(Yamin2008).
Agrowingbodyofliteraturepointstotheadvantageofinfusingdecisionswithaccountabilityand
transparency.ForemostistheAccountabilityforReasonablenessframeworkappliedtotherationalefor
purchasingservicesinpooledfunds(Daniels2000;Daniels2008;DanielsandSabin2008;Daniels2016;
WHO2014;Petricca&Bekele2017).Thisframeworkestablishesfourconditions:
1. Publicity:Detailsofdecisionsmadeneedtobereadilyavailabletothepublic,alongwiththe
justificationforthosedecisions;
2. Relevance:Theorganizationorauthoritymakingthedecisionmustprovideareasonable
explanationofthecriteriaitusestomakedecisions;
3. Revisionandappeals:Mechanismsforchallengeandappealneedtobeavailablewith
opportunitiestomodifydecisionsovertime,forexample,whennewevidencebecomes
available(whichrequiresadequatedatacollection,discussedinthenextsection);
4. Regulation:Formalrulesareneededtoensurethefirstthreeconditionsarefulfilled.

DRAFT:Notforattribution
22
Whilemostoftheseconditionsarerelativelystraightforward,therelevanceconditioncanbetricky.On
thewholeitsimplymeansthatfair-mindedpeoplecanandshouldagreeondecision-makingcriteria
thatareclearandeasytounderstand—andbeaccessibletothepublic.Thisapproachisincreasingly
usedfordecisionsonbudgetallocationsduringscarcityandforotherdifficultdecision-makingareas,
likepolicyresponsestoclimatechange.Butnoteveryonewillagreeonwhatconstitutesreasonable
criteria.Andevenwhenthecriteriaareacceptedasreasonable,decision-makersmayreasonably
disagreeonhowtoweighthedifferentcriteria.Forexample,“valueformoney”(orbangforthebuck)
asacriterionforallocatingscarceresourcesmightshortchangeequityconsiderations.Inthiscase,
additionalcriteria(cost-effectivenessversusequity)areneededtofullyinformrationingdecisions(e.g.
WHO2014;Baltussenetal.2017;Badano2018).
But,onthewhole,havingdecision-makingbodiesexplainthecriteriafortheirdecisionsfeedsintothis
greatersenseoffairnessinprocess.Box1and2offergoodexamples.
Box1:ParticipatoryBudgetinginBrazil
AprocesspioneeredinPortoAlegrein1989,called“participatorybudgeting”(WHO2014-Makingfair
choices),invitedthepublicintothedecision-makingprocessandexplicitlyprioritizedimprovinghealth
servicesinpoorercommunities.Civilsocietyorganizationshaddemandedgreaterrepresentationin
thesedecisionstobringbalancetowhattheyperceivedasacorruptpoliticalestablishment.Within10
yearsofitsimplementation,publicparticipationinthemunicipality’sbudgetprocessesforthingslike
howtousebondsforcapitalimprovementsincludedover40,000peopleeachyear.[Bhatnagar,Prof.
Deepti;Rathore,Animesh;Torres,MagüiMoreno;Kanungo,Parameeta(2003),ParticipatoryBudgeting
inBrazil(PDF),Ahmedabad;Washington,DC:IndianInstitutesofManagement;WorldBank.]Andthe
shareofthetotalbudgetdedicatedtohealthandeducationtripledto40percentby1996,upfrom13
percentin1985.(RebeccaAbers,“FromClientelismtoCooperation:LocalGovernment,Participatory
Policy,andCivicOrganizinginPortoAlegre,Brazil,”Politics&Society26(1998),pp.511–538.)
Sincethen,participatorybudgetinghasspreadtoBrazil’spublichealthsystem,calledSistemaÚnicode
Saúde(SUS).HalfofthehealthcouncilssetupinnearlyallBrazilianmunicipalitiesareregularcitizens
whoareusersofSUS(mainlypatients).Theremainderincludeshealthworkers,administrators,and
managers.Thesecouncilsareresponsibleforoversightfunctionsthatincludestrategicplanning,
approvingtheannualhealthbudget,andmonitoringthedisbursementoffunds.(MartinezMG&Kohler,
JC.Civilsocietyparticipationinthehealthsystem:thecaseofBrazil'sHealthCouncils.Globalizationand
Health2016.)Thisdrovechangeandpeople’spreferencesarenowreflected.
Absentfromthisframeworkisthequestionofoversight.
Thatis,doesanorganizationorbodyneedtobecreatedtoensurefairnessinthedecision-making
process?Forexample,theWHOConsultativeGrouparguedthatoneoptionwouldbetoestablisha
“standingnationalcommitteeonprioritysettingtohandleparticularlydifficultcases”(WHO2014).
Thesekindsofbodiescanensurepublicdebateandinvolvementwhencombinedwiththeprinciples
behindtheAccountabilityforReasonablenesscriteria.
Publicinvolvementandaccountabilityforreasonablenesscouldbeappliedtoanyofthekeyhealth
financingdecisionsaroundrevenuegeneration,poolingorpurchasing.Thiswouldincludeinvolvingthe

DRAFT:Notforattribution
23
publicindecisionmaking;makingpublicallinformationaboutthedecisionsandmotivationsbehind
them;creatingappealandreviewprocesses;andsettingclearcriteriathatlayoutwhatfactorsshould
influencedecisionoutcomes.Criteriaforreasonableness,however,woulddifferdependingonthe
question.Forexample,decisionsoncontracting(whichhealthservicesorinputsshouldbepurchased
andatwhatprice)aredrivenbyfactorssuchasefficiency,thecostsofadministrationandenforcement,
incentivesforquality,andtheriskoffraud.Theextenttowhichthepubliccouldfeasiblybeengagedin
eachtypeofdecisionwouldneedtobedeterminedonacase-by-casebasis.Butbroadpublicdebate
wouldbewarranted.
Thequestionofoveralltaxpolicy—decisionsabouthowmuchtoraise,whoshouldcontributeand
when—isevenmorecomplicatedandrequiresdeeperconsideration.Thesedecisionsareusuallymade
inparliament,byelectedrepresentativeswhotheoreticallyactonbehalfofcitizens.Changestotax
policyusuallygeneratewidepublicreaction.Anddecisionsmadeusuallyfollowwidelypublicized
debatesamongmembersofparliaments.Buttheoutcomes—thewaythevotestally—donot
necessarilyrepresentpublicsentiment.Viewsvaryonwhetherthisissufficienttoensureaccountability
andfairnessinprocesses.Forexample,addinganadditionallayerofcomplexitytore-enforceprocess
fairnessmaynotbejustifiedwhenthepurposeofaparliamentistorepresentthepeople.However,
manycountrieshaveelectedofficialswhoarerelativelywealthyandwhorepresentwealthy
constituencies.Theywilloftenhaveaconflictofinterestwhenitcomestoraisingmoretaxesormaking
ataxsystemmoreequal.Sootherwaysofinfluencingthesedecisionsneedtobefound.
Box2:SocialAccountabilityinEthiopia
Ethiopiaisnowinitsthirdphaseofalongprocessthatisbringingthepublicintogovernmentdecisions
onhealth,education,agriculture,ruralroadprojects,andwaterandsanitation.Since2011,theEthiopia
SocialAccountabilityProgramhashelpedsetupSocialAccountabilityCommittees(SACs)in223ofthe
country’s770localdistricts,calledworedas.
Thecommitteesaremadeupinequalpartsoflocallyelectedcouncilmembers,locallyappointed
administratorsandcivilsocietyorganizations.Theirmainpurposeistoensurethatlocaladministrative
unitsaretransparentandheldaccountabletocitizens.
TheseSACshelpbuildstrongsystemsforevidence-basedserviceperformancemeasures,usingfive
socialaccountabilitytools:CommunityScoreCards(CSCs)thatusefocusgroupsforself-assessments;
CitizenReportCards(CRCs)thatsurveyhouseholdstoassesthelevelofservicestheyarereceiving;
ParticipatoryPlanningandBudgeting(PPB)andGenderResponsiveBudgeting(GRB)forcitizen
engagementinbudgetplanning;andthePublicExpenditureTrackingSurvey(PETS)forassessmentof
budgetexecution.
Oneexampleofawell-functioningSACisinMalgaWoreda,insouthwesternEthiopia.TheSACthere
startedbyusinghouseholdsurveysandmeasuredaninsufficientnumberofhealthworkerstoservethe
community.Thatputpressureonthelocalgovernmenttoallocatemoreresources.And,asaresult,
healthcentersrecruitedandtrainedadditionalmidwives,healthofficers,andrecordofficers.Through
purchasing,clinicsreceivedneededmedicalequipmentandmedicines.Andinfrastructuremoneywas
allocatedtobuildroadstohealthcentersinTenkaroandHaro,andcreateanewwatersourcein
Manichotown.
TheseSACs,aswithparticipatorybudgetinginBrazil,createinclusionandbringfairnesstotheprocess,

DRAFT:Notforattribution
24
whichmakethelocalgovernmentsaccountabletothecitizenstheyrepresent.
Monitoring
TrackingProgressisaMust
Countriesmustgetmoreseriousaboutdatacollection,orthequestforequitywillbemeaningless.This,
ofcourse,requirestrackingUHCoutcomes.Butitalsorequirestrackinginequitiesinthethree
componentsofhealthfinancing(revenuegeneration,poolingandpurchasing)thatcanaffectUHC
outcomes.
Decisionmakerscannotadjusttheirpoliciesovertimeunlessknowledgeisavailableonwherehealth-
relatedoutcomesaregettingbetterand,moreimportantly,wheretheyaregettingworse.Thisrequires
trackingthosewhoarecovered,thequalityofhealthservicestheyarereceiving,andtheextentto
whichtheyareprotectedfromfinancialhardship.Withouttheseaggregateddata,policymakersare
unabletofocusonthemostdisadvantaged—whichtheymustdotoremaininkeepingwiththegoalsof
UHC.
Ataminimum,policymakersneedregularlycollecteddatadisaggregatedbygender,income(orwealth),
andgeographicallocation(forexample,ruralorurban).Countriesshouldaddonotherdeterminants
thatapplytotheiruniquepopulations,like,forexample,ethnicity,age,familystructure,typeofhealth
problem,andcapacitytodeliver.Theimportantpointhereisthatdisaggregateddatawillallowthe
healthfinancing-relatedinequitiestobemeasuredandtrackedovertime,whichissocriticalto
producingequityduringpolicyadjustments,andkeepinghealthfinancingdecisionsontrackforUHC.
Forexample,onrevenuegeneration,dataneedstobecollectedtounderstandwhoissufferingsevere
financialhardshipfromout-of-pocketpaymentsforwhichtypeofservice,andwhetheradjustmentsto
policiesarereducingtheburden.Onpooling,dataisneededtotrackhowdomesticrevenuesare
allocatedtofinancingschemestoensuretaxmoneyisusedequitablyandnottosubsidizealreadywell-
endowedpools.Andonpurchasing,inequitiesinthedistributionofhealthworkersandotherinputs
suchasessentialmedicinesneedtobemonitored,becausethisfunctiondetermineswhetherthe
servicespeopleneedareavailable,closetothem,andofgoodquality.
Tosupportfairnessofprocess,thesedatathenmustbeanalyzedaccuratelyandpresentedtopolicy
makersinaneasy-to-understandformat(seeHosseinpooretal2018).Theotherhalfofsupporting
fairnessofprocessistoalsoensurethatdataaresharedwiththepublicandotherstakeholdersinaway
theycandigest.
Thismeansmanycountrieswillhavetochangethewaytheymonitor,shareandevaluateprogressin
theirhealthsystems.Neededarerecordsofpatientattendanceandtreatmentathealthfacilities.These
canbecollectedthroughhouseholdsurveys,butareroutinelyavailableiftheyaresystematicallyand
accuratelycollectedatthetimeofserviceandquicklyaggregatedandreported.Theserecordsmaybe
supplementedbyothersources,suchascancerregistries.Buttheyvaryacrosscountriesinnumberand
qualityandgenerallyfailtoprovideinformationonqualityofservices,levelsoffinancialprotection,and
abaseline(whoneedsservices).

DRAFT:Notforattribution
25
Apushisbeingmadenowtouseelectronicmedicalrecordsandspecificallyinputsystems,which
capturecomprehensiveinformationonpatientcare,includingsymptoms,diagnoses,etiologies,
proceduresandoutcomes.(“Towardgreaterintegrationofcareandimprovedefficiency:Acritical
reviewofEHIF’spaymentsystem,WorldBank2017,page46.)
Othermethodsforundertakingtherequiredanalysisincludetrackingoutcomesofadult,maternaland
childmortality(e.g.Marmotetal1991;Mackenbacketal.1997;Gwatkin2000;Victora2003;Moseret
al.2005;Barrosetal.2010;Bendavid2014;Wagstaff,Bredenkamp&Buisman2014;Gwatkin2017).
Theyalsoincludemeasuringprogressinincreasingoverallcoverageandreducinginequalitiesin
coveragewithcorehealthinterventions,largelyfocusedontargeteddiseasesoftheMDGs(e.g.Raoet
al.2014;Alkenbracketal.2015;Restrepo-Méndezetal.2016;Hoganetal.2017;WHO&WorldBank
2017;Wongetal.2017;Victoraetal.2017).
AnumberofdifferentmethodshavebeenusedtodocumentOOPs-relatedfinancialcatastropheand
impoverishment,whichhashelpedpolicymakersunderstandwhoissufferingthemost(e.g.Xuetal.
2003&2006;Wagstaff&Lindelow2014;Bredenkamp&Buisman2016;Khan,Ahmed&Evans2017;
Wagstaffetal.2017aandb;Ghimireetal.2018).Disagreementoverwhichonesworkbesthaveledto
studiesthatincluderesultsfromtwoormoreofthesemethods(forexample,WHOandWorldBank
2017).
AshortcomingintheoverallapproachtotrackingprogresstowardsUHC,asitrelatestoservice
coverageandfinancialprotection,isthatthemethodsdevelopedfailtodrilldowndeepenoughto
unearthalltheinequalitiesassociatedwithhealth-financingfunctions(e.g.Boermaetal.2014;WHO
andWorldBank2017).Improvementsthathavebeenmaderelateto:
• examiningwhetherfiscalpolicyispro-poor,whiletakingintoaccountthenetimpactofwhat
theypayinandwhattheyreceiveincashorin-kindbenefits(e.g.Lustig2016&2017;Jellemaet
al.2017;Lustig2018).
• inequalitiesintheavailabilityofservicesandinkeyinputs,suchashealthworkers(e.g.O’Neillet
al.2013;WHO2015;Speybroecketal.2012).
Toolstohelpcountryanalystsundertakethisworkarenowbeingdeveloped.Theyaredesignedtogive
guidanceon1)estimatingtheabsenceoffinancialprotectionandinequalitiesinthehealthfinancing
functions(Wagstaffetal.2007;Wagstaff2008;Saksena,Hsu&Evans2014;Wagstaff&Eozenou2014;
WorldBank2018a),and2)analyzinginequalitiesinhealthoutcomesandhealthservicecoverage
(Hosseinpoor2016&2018;WorldBank2018).
Forcountrieswithresourcestodohouseholdexpendituresurveys,theWorldBankhasestablishedthe
ADePTResourceCenterwithsoftwarethatallowsanalyststouploadtheirsurveydataandproduce
indicatorsofinequalitiesandunsustainablehealth-relatedfinancialburdens.(WorldBank2018a).
Approachestorapidserviceavailabilityandreadiness,whichcanbeusedtotrackgeographic
inequalities,havealsobeendeveloped,includingtheServiceAvailabilityandReadinessTool(WHO
2018b).
Butforcountrieslackingtheresourcesfortheseexpensive,time-consumingandlabor-intensive
householdsurveys,theWorldBankhasdevelopedtheSwiftSurveyapproach.Thisisalowcost,rapid

DRAFT:Notforattribution
26
wayofmeasuringincomesandtrackingprogressinthereductionofpoverty(WorldBank2018b).This
approachoffershopeoflower-costandtimelywaysofobtainingthenecessarydataforUHCtracking.
Themainmessagehereisthattoolsareavailabletohelpcountries.Butwerecognizethatfindingfunds
topayformonitoringischallenging,especiallyinlow-incomecountries.Thisareaofhealthsystemsis
generallyunderfunded.MostOECDcountriesinvestlessthan4percentoftotalhealthexpendituresin
informationsystems,andlow-andmiddle-incomecountriesinvestlessthan1percent.(WHO,OECD,
WorldBank,2018)
Robustinformationsonecessarytomonitoring,whichprovidespolicymakersandthepublicwith
neededdatatohelpestablishfairprocessesandassesswhetheradecisionisunacceptable,mustbea
priority.
Section5:SeeingtheWayForward
ThisexerciseinmappingoutwhatequityinfinancingUHCmeansistoshowtheneedforafundamental
shiftinpolicymaking.Weknowthatmany,manycountrieshavecommittedtoUHC.Wearestillseeing
deepinequitiesinservicecoverageandfinancialprotectionthatareassociatedwithequityinfinancing.
Thistellsusthatsomethingisgoingwrongindecision-makingprocesses.Webelievethattakingamore
mindfulapproach—applyingthethreeprongsoutlinedinthispaper—willmakeadifference.Thereward
willbemoreequitableUHCoutcomesandgreatersocietalandeconomicbenefits.
Countriesmustchartawayforward.Whetheralreadyontherightpathortryingtoafindawaythere,
theapproachmappedoutinthisreportshouldhelp.Itisdesignedtofillsomegapsinguidanceforthose
whohavecommittedtoUHC.Andwhilemosttechnicaldetailsofwhatcanandshouldbedonehaveto
bedomesticallydetermined,weknowhealthassistanceplaysarole.Theprincipleslaidoutherealso
applytodevelopmentassistance;theyshowthatequitableoutcomesmustbetheultimategoal.
Soforcountryministriesandpolicymakers,thestartingpointistoestablishorexpandbasicguaranteed
packages,withprogressiverealization(expandingthereachovertimetoincludemoreandbetter
services).BasedonanextensionofthelogicofUHC,everycountryshouldstartwithsomelevelof
guaranteedcoveragewithsomeprioritygivetotheworse-off,financedbyprepaidandpooledsystems,
accordingtoabilitytopay.OncecommittedtothisUHCpolicy-makingpath,webelievethethree-
prongedapproachmappedoutinthisreportwillbringclaritytodifficultdecisions.
Onlycountriescanknowwhatneedstobedone,andinwhatorder—identifyingandavoiding
unacceptabledecisions,invitingincivilsocietyandestablishprocessesthatcommunitiescanagreeare
fair,orsettingupdatacollectionprocessesforbettermonitoring.
Thesethreeprongsareintrinsicallylinked.Whenthepublicparticipatesindecisionsandfeelsthat
processesarefair,alldecisionsmovingforwardcarrythatimportantquality.Decisions,ofcourse,are
bestmadebasedonevidence,whichrequiresdatacollectionandmonitoring.Butpolicy-makersneedto
moveforwardwithpublicinvolvementasameansforestablishingprocessfairness,regardlessofwhere
theyareindatacollection.Slowprogressononeshouldnotleadtoslowprogressontheother.
Likewise,countriescangothroughthisprocessandlookforward—andmaybeaddtothelistof10
unacceptableoutcomeswe’veidentifiedthusfar—regardlessofwheretheyareinsettinguppublic

DRAFT:Notforattribution
27
involvementordatacollectionandmonitoring.Theseothertwoprongswilleventuallypropupthe
abilitytoidentifyunacceptabledecisionssotheymaybecorrected,andwillhelpavoidmakingfuture
decisionsthatleadtoinequities.
Theglobalcommunityshouldhelpfacilitatethisshiftusingaparallelthree-prongedapproach.
Aswithcountrydecisions,developmentpartnersshouldsystematicallyintroduceequityconsiderations
intoallengagementsonhealthfinancingpolicies,andassesstheequityimplicationsoftheirfinancial
support.Thegoalhereisthesame:toseewhetherhealthsectorfinancialsupportisleadingcountriesto
makeunacceptablechoices.Developmentpartnersalsoshouldusetheirfinancialandtechnicalsupport
toincreasinglybuildcountrycapacitiesandinstitutionsthatproduceandsupportprocessestoteaseout
unacceptablechoices,establishfairnessinprocess,andcreatebetterdatacollectionandmonitoring.
And,finally,developmentpartnersshoulddevelopthetools,methodsandapproachesessentialto
carryingouttheseworkstreams—asglobalpublicgoods.

AN
NEX
1
Tabl
e 1:
Ineq
ualit
ies
and
Ineq
uitie
s in
UH
C O
utco
mes
and
UH
C F
inan
cing
, Inc
ludi
ng U
nacc
epta
ble
UH
C F
inan
cing
Pol
icy
Cho
ices
UHC
Outc
omes
Outc
omes
In
equa
lities
In
equi
ties
Effec
tive C
over
age w
ith
Need
ed H
ealth
Ser
vices
Diffe
renc
es ac
ross
peop
le or
grou
ps in
eff
ectiv
e cov
erag
e with
healt
h ser
vices
(p
erso
nal h
ealth
servi
ces,
publi
c hea
lth
(inclu
ding n
on-p
erso
nal h
ealth
servi
ces)
and
gove
rnan
ce fu
nctio
ns
Diffe
renc
es in
the e
ffecti
ve co
vera
ge of
he
alth s
ervic
es (in
cludin
g non
-per
sona
l he
alth s
ervic
es) a
nd go
vern
ance
func
tions
un
less j
ustifi
ed by
diffe
renc
es in
healt
h ne
eds1
No
diffe
renc
es in
effec
tive c
over
age o
f he
alth s
ervic
es w
hen t
here
are d
iffere
nces
in
healt
h nee
ds2
Cove
rage
with
Fina
ncial
Pr
otecti
on
Some
peop
le or
grou
ps ar
e pus
hed i
nto
pove
rty or
furth
er in
to po
verty
due t
o out-
of-po
cket
paym
ents
(OOP
s) for
healt
h ser
vices
Some
peop
le or
grou
ps ar
e pus
hed i
nto
pove
rty, o
r dee
per in
to po
verty
due t
o OOP
s be
caus
e of la
ck of
acce
ss or
in us
ing qu
ality
servi
ces g
uara
nteed
by co
mpuls
ory p
repa
id an
d poo
led fin
ancin
g arra
ngem
ents
Diffe
renc
es ac
ross
peop
le or
grou
ps in
the
incide
nce o
r exte
nt of
catas
troph
ic OO
Ps fo
r he
alth s
ervic
es
Diffe
renc
es ac
ross
peop
le an
d gro
ups i
n the
inc
idenc
e or e
xtent
of ca
tastro
phic
OOPs
be
caus
e of la
ck of
acce
ss or
in us
ing qu
ality
servi
ces g
uara
nteed
by co
mpuls
ory p
repa
id an
d poo
led fin
ancin
g arra
ngem
ents
1 Hor
izonta
l equ
ity
2 Ver
tical
equit
y

Healt
h Fi
nanc
ing
Func
tions
In
equa
lities
3 In
equi
ties4
Un
acce
ptab
le Fi
nanc
ing
Polic
y Cho
ices5
Reve
nue G
ener
atio
n
Di
ffere
nces
acro
ss pe
ople
and g
roup
s in n
et co
ntribu
tions
to th
e pub
lic fin
ance
syste
m (in
cludin
g, bu
t not
limite
d to h
ealth
) 6
Reve
nue g
ener
ation
syste
ms w
ith
differ
ence
s acro
ss pe
ople
and g
roup
s in n
et co
ntribu
tions
to th
e pub
lic fin
ance
syste
m (in
cludin
g, bu
t not
limite
d to h
ealth
) whic
h ma
ke th
e pos
t-tax
, pos
t-tra
nsfer
disp
osab
le inc
ome d
istrib
ution
less
equa
l than
the p
re-
tax di
stribu
tion
1. Ra
ise ad
dition
al re
venu
es fo
r hea
lth th
at ma
ke co
ntribu
tions
to th
e pub
lic fin
ancin
g sy
stem
less p
rogr
essiv
e with
out
comp
ensa
tory m
easu
res t
hat e
nsur
e tha
t the
post-
tax, p
ost-t
rans
fer di
spos
able
incom
e dist
ributi
on is
not le
ss eq
ual.
Di
ffere
nces
acro
ss pe
ople
and g
roup
s in t
he
incide
nce o
f OOP
s for
healt
h ser
vices
Some
peop
le or
grou
ps ar
e pus
hed i
nto
pove
rty, o
r dee
per in
to po
verty
due t
o OOP
s be
caus
e of la
ck of
acce
ss or
in us
ing qu
ality
servi
ces g
uara
nteed
by co
mpuls
ory p
repa
id an
d poo
led fin
ancin
g arra
ngem
ents
Diffe
renc
es ac
ross
peop
le an
d gro
ups i
n the
inc
idenc
e or e
xtent
of ca
tastro
phic
OOPs
be
caus
e of la
ck o
f acc
ess o
r in us
ing qu
ality
servi
ces g
uara
nteed
by co
mpuls
ory p
repa
id an
d poo
led fin
ancin
g arra
ngem
ents
Diffe
renc
es ac
ross
peop
le an
d gro
ups i
n the
inc
idenc
e of O
OPs t
hat d
eter t
hem
from
using
quali
ty se
rvice
s gua
rante
ed by
co
mpuls
ory p
repa
id an
d poo
led fin
ancin
g ar
rang
emen
ts
2. Inc
reas
e out-
of-po
cket
paym
ents
for
unive
rsally
guar
antee
d per
sona
l hea
lth
servi
ces w
ithou
t an e
xemp
tion s
ystem
7 or
co
mpen
satin
g mec
hanis
ms.
3 Link
ed to
UHC
outco
mes
4 Link
ed to
UHC
outco
mes
5 Una
ccep
table
as th
ey ex
acer
bate
inequ
ities i
n UHC
outco
mes
6 Net
contr
ibutio
ns ar
e gro
ss co
ntribu
tions
minu
s tra
nsfer
s rec
eived
in ca
sh or
kind
7 G
iven t
he lim
ited e
viden
ce-b
ase i
n sup
port
of su
ch po
licies
, pro
of tha
t thes
e sys
tems a
nd m
echa
nisms
is cr
itical

Healt
h Fi
nanc
ing
Func
tions
In
equa
lities
3 In
equi
ties4
Un
acce
ptab
le Fi
nanc
ing
Polic
y Cho
ices5
Di
ffere
nces
acro
ss fir
ms in
their
net
contr
ibutio
ns to
the p
ublic
finan
ce sy
stem8
Reve
nue g
ener
ation
syste
ms w
ith
differ
ence
s acro
ss fir
ms in
their
net
contr
ibutio
ns to
the p
ublic
finan
ce sy
stems
tha
t can
not b
e jus
tified
by so
me
comp
ensa
ting b
enefi
t for t
he ec
onom
y
Di
ffere
nces
acro
ss in
dividu
als or
grou
ps in
co
ntribu
tions
to vo
luntar
y pre
paid
and
poole
d fina
ncing
arra
ngem
ents
Diffe
renc
es ac
ross
indiv
idual
or gr
oups
in
contr
ibutio
ns to
volun
tary p
repa
id an
d po
oled f
inanc
ing ar
rang
emen
ts ba
sed
large
ly on
healt
h stat
us, in
cludin
g pre
-ex
isting
cond
itions
and r
isk fa
ctors
3. Ra
ise ad
dition
al re
venu
es fo
r univ
ersa
lly
guar
antee
d per
sona
l hea
lth se
rvice
s thr
ough
volun
tary,
prep
aid an
d poo
led
finan
cing a
rrang
emen
ts ba
sed l
arge
ly on
he
alth s
tatus
, inclu
ding p
re-e
xistin
g co
nditio
ns an
d risk
facto
rs.
Pool
ing
Func
tion
Ine
ligibi
lity ac
ross
peop
le an
d gro
ups t
o pa
rticipa
te in
any p
ool o
r diffe
renc
es in
eli
gibilit
y acro
ss pe
ople
and g
roup
s to
partic
ipate
in po
ols
Inelig
ibility
of pe
ople
and g
roup
s to
partic
ipate
in an
y poo
l or d
iffere
nces
in
eligib
ility a
cross
peop
le an
d gro
ups t
o pa
rticipa
te in
pools
unles
s jus
tified
by
differ
ence
s in n
eed9
,10
Diffe
renc
es ac
ross
peop
le an
d gro
ups i
n en
rolm
ent w
ith pr
ivate
healt
h ins
uran
ce
includ
ing in
sura
nce f
or se
rvice
s not
guar
antee
d by c
ompu
lsory
prep
aid an
d po
oled f
inanc
ing ar
rang
emen
ts
Diffe
renc
es ac
ross
peop
le an
d gro
ups i
n en
rolm
ent w
ith pr
ivate
healt
h ins
uran
ce
includ
ing in
sura
nce f
or se
rvice
s not
guar
antee
d by c
ompu
lsory
prep
aid an
d po
oled f
inanc
ing ar
rang
emen
ts un
less
justifi
ed by
diffe
renc
es in
need
8 For
exam
ple, ta
x holi
days
, exe
mptio
ns fr
om so
cial c
ontrib
ution
s, pr
ofit s
hiftin
g, etc
.) 9 D
iffere
nces
in ne
ed in
clude
both
healt
h and
inco
me. T
hose
with
lowe
r hea
lth ne
ed m
ore h
ealth
servi
ces,
and t
hose
that
are p
oor a
re le
ss ab
le to
pay f
or ne
eded
healt
h ser
vices
. 10
It is
acce
ptable
whe
n elig
ibility
is re
strict
ed to
the w
orse
off (
sicke
r and
poor
er),
but n
ot the
bette
r off (
healt
hier a
nd ric
her).

Healt
h Fi
nanc
ing
Func
tions
In
equa
lities
3 In
equi
ties4
Un
acce
ptab
le Fi
nanc
ing
Polic
y Cho
ices5
Diffe
renc
es in
per
capit
a allo
catio
ns (o
f do
mesti
c gen
eral
gove
rnme
nt re
venu
e or
dono
r fun
ds) t
o pre
paid
and p
ooled
healt
h fin
ancin
g sch
emes
(inclu
ding p
ublic
ly fun
ded h
ealth
servi
ces,
socia
l hea
lth
insur
ance
, volu
ntary
insur
ance
)11
Diffe
renc
es in
per c
apita
alloc
ation
s (of
dome
stic g
ener
al go
vern
ment
reve
nue o
r do
nor f
unds
) acro
ss pr
epaid
and p
ooled
sc
heme
s unit
s unle
ss ju
stifie
d by d
iffere
nces
in
need
or th
e ava
ilabil
ity of
fund
s fro
m oth
er
sour
ces
4. Ch
ange
per c
apita
alloc
ation
s of t
ax
reve
nue1
2 or
dono
r fun
ds ac
ross
prep
aid
and p
ooled
finan
cing s
chem
es in
way
s tha
t exa
cerb
ate in
equit
ies, u
nless
justi
fied
by di
ffere
nces
in ne
ed or
the a
vaila
bility
of
funds
from
othe
r sou
rces.
W
ithin
finan
cing s
chem
es, d
iffere
nces
in pe
r ca
pita a
lloca
tions
from
high
er to
lowe
r au
tonom
ous,
admi
nistra
tive u
nits
With
in fin
ancin
g sch
emes
, diffe
renc
es in
per
capit
a allo
catio
ns fr
om hi
gher
to lo
wer
auton
omou
s, ad
minis
trativ
e unit
s unle
ss
justifi
ed by
diffe
renc
es in
need
or th
e av
ailab
ility o
f fund
s fro
m oth
er so
urce
s
5. W
ithin
finan
cing s
chem
es, c
hang
e per
ca
pita a
lloca
tions
from
high
er to
lowe
r ad
minis
trativ
e lev
els in
way
s tha
t ex
acer
bate
inequ
ities,
unles
s jus
tified
by
differ
ence
s in n
eed o
r the
avail
abilit
y of
funds
from
othe
r sou
rces.
W
ithin
sche
mes o
r poo
ls, di
ffere
nces
in
alloc
ation
s of fu
nds a
cross
dise
ases
With
in sc
heme
s or p
ools,
diffe
renc
es in
all
ocati
ons o
f fund
s acro
ss di
seas
es th
at ar
e no
t justi
fied b
y diffe
renc
es in
need
or th
e av
ailab
ility o
f fund
s fro
m oth
er so
urce
s
6. W
ithin
sche
mes o
r poo
ls, ch
ange
all
ocati
ons o
f fund
s acro
ss di
seas
es in
wa
ys th
at ex
acer
bate
inequ
ities,
unles
s jus
tified
by di
ffere
nces
in ne
ed or
the
avail
abilit
y of fu
nds f
rom
other
sour
ces.
Purc
hasin
g Fu
nctio
n
Di
ffere
nces
in en
titlem
ents
of gu
aran
teed
servi
ce pa
ckag
es, im
plicit
or ex
plicit
, acro
ss
peop
le an
d gro
ups1
3
Diffe
renc
es in
entitl
emen
ts of
guar
antee
d se
rvice
pack
ages
acro
ss pe
ople
and g
roup
s un
less j
ustifi
ed by
diffe
renc
es in
need
9
7. Int
rodu
ce hi
gh-co
st, lo
w-be
nefit
inter
venti
ons t
o a un
iversa
lly gu
aran
teed
servi
ce pa
ckag
e befo
re ac
hievin
g clos
e to
full c
over
age w
ith lo
w-co
st, hi
gh-b
enefi
t se
rvice
s.
11 H
ealth
care
finan
cing s
chem
es ar
e the
main
type
s of fi
nanc
ing ar
rang
emen
ts thr
ough
whic
h hea
lth se
rvice
s are
paid
for an
d obta
ined b
y peo
ple. H
ere w
e refe
r to p
ooled
sche
mes r
ather
than
to
OOPs
, inclu
ding n
ation
al or
sub-
natio
nal h
ealth
servi
ces f
unde
d fro
m go
vern
ment
reve
nues
(som
etime
s with
dono
r fun
ds as
well
), so
cial h
ealth
insu
ranc
e, vo
luntar
y ins
uran
ce (O
ECD
2011
).
12 T
ax re
venu
e exc
ludes
socia
l hea
lth in
sura
nce c
ontrib
ution
s 13
Enti
tleme
nts re
flect
the se
rvice
s and
leve
ls of
finan
cial p
rotec
tion t
o whic
h peo
ple ar
e enti
tled
de ju
re. W
hethe
r peo
ple re
ceive
thes
e enti
tleme
nts de
facto
is a
matte
r for
purch
asing
.

Healt
h Fi
nanc
ing
Func
tions
In
equa
lities
3 In
equi
ties4
Un
acce
ptab
le Fi
nanc
ing
Polic
y Cho
ices5
Di
ffere
nces
acro
ss pe
ople
or gr
oups
in th
e av
ailab
ility a
nd qu
ality
of pe
rsona
l hea
lth
servi
ces1
4
Diffe
renc
es ac
ross
peop
les an
d gro
ups i
n the
avail
abilit
y and
quali
ty of
unive
rsally
gu
aran
teed p
erso
nal h
ealth
servi
ces u
nless
jus
tified
by di
ffere
nces
in ne
ed15
8. Inc
reas
e the
avail
abilit
y and
quali
ty of
perso
nal h
ealth
servi
ces t
hat a
re
unive
rsally
guar
antee
d in w
ays t
hat
exac
erba
te ex
isting
ineq
ualiti
es un
less
justifi
ed by
diffe
renc
es in
need
.
Di
ffere
nces
acro
ss pe
ople
or gr
oups
in th
e av
ailab
ility o
f key
servi
ces i
nputs
16
Diffe
renc
es ac
ross
peop
le or
grou
ps in
the
avail
abilit
y of k
ey in
puts
to pr
oduc
e a
unive
rsally
guar
antee
d set
of pe
rsona
l he
alth s
ervic
es un
less j
ustifi
ed by
dif
feren
ces i
n nee
d
9. Inc
reas
e the
avail
abilit
y and
quali
ty of
core
publi
c hea
lth fu
nctio
ns in
way
s tha
t ex
acer
bate
exist
ing in
equa
lities
unles
s jus
tified
by di
ffere
nces
in ne
ed.
Di
ffere
nces
acro
ss pe
ople
and g
roup
s in t
he
avail
abilit
y and
quali
ty of
core
publi
c hea
lth
functi
ons1
7
Diffe
renc
es ac
ross
peop
le an
d gro
ups i
n the
av
ailab
ility a
nd qu
ality
of co
re pu
blic h
ealth
fun
ction
s unle
ss ju
stifie
d by n
eed
10.
Incre
ase t
he av
ailab
ility a
nd qu
ality
of co
re pu
blic h
ealth
func
tions
in w
ays t
hat
exac
erba
te ex
isting
ineq
ualiti
es un
less
justifi
ed by
diffe
renc
es in
need
.
14 A
vaila
bility
mea
ns th
at se
rvice
s exis
t and
peop
le ca
n use
them
. 15
As f
or he
alth s
ervic
es, th
is inc
ludes
both
horiz
onal
and v
ertic
al eq
uity c
onsid
erati
ons –
e.g.
wher
e nee
ds di
ffer,
the av
ailab
ility a
nd qu
ality
of a s
et of
servi
ces s
hould
diffe
r.
16 F
or ex
ample
, hea
lth w
orke
rs, eq
uipme
nt, m
edici
nes,
and i
nfras
tructu
re et
c. 17
For
exam
ple, p
opula
tion-
base
d hea
lth pr
omoti
on, s
urve
illanc
e, ou
tbrea
k con
trol e
tc.

References
Abelson,J.,Giacomini,M.,Lehoux,P.,andGauvin,F.P.2007.“Bringing‘thePublic’intoHealthTechnologyAssessmentandCoveragePolicyDecisions:FromPrinciplestoPractice.”HealthPolicy82:37-50.
AfricaHealthBudgetNetwork.2018.http://africahbn.info
AlkenbrackS,ChaitkinM,ZengW,CoutureT,SharmaS.DidequityofreproductiveandmaternalhealthservicecoverageincreaseduringtheMDGera?Ananalysisoftrendsanddeterminantsacross74low-andmiddle-incomecountries.PLoSOne2015;10:e134905.
Badano,G.,2018.”IfYou’reaRawlsian,HowComeYou’reSoClosetoUtilitarianismandIntuitionism?ACritiqueofDaniels’AccountabilityforReasonableness.”HealthCareAnalysis26(1):1-16.
Baltussen,R.,Jansen,M.P.,Bijlmakers,L.,Tromp,N.,Yamin,A.E.,andNorheim,O.F.2017.“ProgressiveRealisationofUniversalHealthCoverage:WhataretheRequiredProcessesandEvidence?”BMJGlobalHealth2(3),p.e000342.
Barros,F.C.,Victora,C.G.,Scherpbier,R.andGwatkin,D.,2010.Socioeconomicinequitiesinthehealthandnutritionofchildreninlow/middleincomecountries.RevistadeSaúdePública,44(1),pp.1-16.
Bastagli,F,Coady,D.,andGupta,M.S.2012.“IncomeInequalityandFiscalPolicy.”InternationalMonetaryFundStaffDiscussionNote12/08.
Bendavid,E.,2014.Changesinchildmortalityovertimeacrossthewealthgradientinless-developedcountries.Pediatrics,134:e1551–59.
Byskov,J.,Maluka,S.O.,Marchal,B.,Shayo,E.H.,Bukachi,S.,Zulu,J.M.,Blas,E.,Michelo,C.,Ndawi,B.,andHurtig,A.K.2017.“TheNeedforGlobalApplicationoftheAccountabilityforReasonablenessApproachtoSupportSustainableOutcomes:CommentonExpandedHTA:EnhancingFairnessandLegitimacy".InternationalJournalofHealthPolicyandManagement6(2):115.
Campbell,M.,Craig,P.,andEscobar,O.2017.“ParticipatoryBudgetingandHealthandWellbeing:ASystematicScopingReviewofEvaluationsandOutcomes.”TheLancet390:S30.
Cevik,S.andCorrea-Caro,C.2015.“Growing(Un)equal:FiscalPolicyandIncomeInequalityinChinaandBRIC.”IMFWorkingPaper15/68,Washington,DC.
Chaumont,C.,Hsi,J.,Bohne,C.,Mostaghim,S.andMoon,S.,2017.“ANewGoldenAge?ProposalforanInnovativeGlobalHealthFundingMechanismforMiddle-IncomeCountries.”GlobalChallenges1(7).
Chima,C.C.andFranzini,L.,2015.“SpilloverEffectofHIV-specificForeignAidonImmunizationServicesinNigeria.”InternationalHealth8(2):108-115.
Clements,B.,Gaspar,V.,andGupta,S.2015.“TheIMFandIncomeDistribution.”InequalityandFiscalPolicy,page21.

Daniels,N.2000.“AccountabilityforReasonableness.EstablishingaFairProcessforPrioritySettingisEasierthanAgreeingonPrinciples.”BritishMedicalJournal321:1300-1301.
Daniels,N.2008.“Justhealth:meetinghealthneedsfairly.”Cambridge:CambridgeUniversityPress.
Daniels,N.andSabin,J.E.,2008.“SettingLimitsFairly:LearningtoShareResourcesforHealth.”2ndedition.Oxford:OxfordUniversityPress.
Daniels,N.2011.“AgingandIntergenerationalEquity.”InGlobalPopulationAgeing:PerilorPromise,editedbyJ.R.Beard,S.Biggs,D.E.Bloom,L.P.Fried,P.Hogan,A.Kalache,andS.J.Olshansky.Geneva:WorldEconomicForum.
Daniels,N.2016.“AccountabilityforReasonablenessandPrioritySettinginHealth.InPrioritizationinMedicine,editedbyE.NagelandM.Lauerer.Springer,Cham.
EuropeanCommission.2013.“TheImpactoftheFinancialCrisisonUnmetneedsforHealthcare
Evans,T.,Whitehead,M.,Diderichsen,F.,Bhuiya,A.andWirthM.2001.ChallengesInequitiesinHealth:FromEthicstoAction.NewYork:TheRockefellerFoundation,NewYork:OxfordUniversityPress.
Farmer,P.2004.“PathologiesofPower:Health,HumanRights,andtheNewWaronthePoor.”Volume4.Berkeley:UniversityofCaliforniaPress.
Fleurbaey,M.andManiquet,F.2017.“OptimalIncomeTaxationTheoryandPrinciplesofFairness.”CentreforOperationalResearchandEconometricsDiscussionPaper,UniversitéCatholiquedeLouvain.https://uclouvain.be/en/research-institutes/immaq/core/discussion-papers.html
Ghimire,M.,Ayer,R.andKondo,M.,2018.Cumulativeincidence,distribution,anddeterminantsof catastrophic health expenditure in Nepal: results from the living standards survey.Internationaljournalforequityinhealth,17(1),p.23.
Giedion,U.andGuzman,J.2017.“DefiningtheRulesoftheGame:GoodGovernancePrinciplesfortheDesignandRevisionoftheHealthBenefitsPackage,”inWhat'sIn,What'sOut:DesigningBenefitsforUniversalHealthCoverage,editedbyA.Glassman,U.Giedion,andP.C.Smith.Washington,DC:BrookingsInstitutionPress.
Glassman,A.andChalkidou,K.2012.“Priority-settinginHealth:BuildingInstitutionsforSmarterPublicSpending.”Washington,DC:CenterforGlobalDevelopment.
Gruskin,S.andDaniels,N.2008.“JusticeandHumanRights:PrioritySettingandFair,DeliberativeProcess.”AmericanJournalofPublicHealth98:1573-7.
Gwatkin,D.R.,2000.Healthinequalitiesandthehealthofthepoor:Whatdoweknow?Whatcanwedo?.Bulletinoftheworldhealthorganization,78(1),pp.3-18.
Gwatkin,D.R.,2017.Trendsinhealthinequalitiesindevelopingcountries.TheLancetGlobalHealth,5(4),pp.e371-e372.

Hogan,D.R.,Stevens,G.A.,Hosseinpoor,A.R.andBoerma,T.,2017.MonitoringuniversalhealthcoveragewithintheSustainableDevelopmentGoals:developmentandbaselinedataforanindexofessentialhealthservices.TheLancetGlobalHealth.
Hosseinpoor,A.R.,Bergen,N.,Barros,A.J.,Wong,K.L.,Boerma,T.andVictora,C.G.,2016.Monitoringsubnationalregionalinequalitiesinhealth:measurementapproachesandchallenges.Internationaljournalforequityinhealth,15(1),p.18.DHS,comparemethods
Hosseinpoor,A.R.,Bergen,N.,Schlotheuber,A.andBoerma,T.,2018.Nationalhealthinequalitymonitoring:currentchallengesandopportunities.Globalhealthaction,11(sup1),p.1392216.
International MonetaryFund (IMF).2017. FiscalMonitor: Tackling Inequality.WashingtonDC.October2017
Jellema, J., Wai-Poi, M. and Afkar, R., 2017. The Distributional Impact of Fiscal Policy inIndonesia. The Distributional Impact of Taxes and Transfers, p.149. CEQ Commitment toEquity,TulaneUniversity,WorkingPaper40.
Kaiser,K.,Bredenkamp,C.,andIglesias,R.2016.SinTaxReforminthePhilippines:TransformingPublicFinance,Health,andGovernanceforMoreInclusiveDevelopment.DirectionsinDevelopment.Washington,DC:WorldBank.doi:10.1596
Kasdan, A. andMarkman, E., 2017. “Participatory Budgeting and Community-Based Research:Principles,Practices,andImplicationsforImpactValidity.”NewPoliticalScience,39(1):143-155.
Khan, J.A.,Ahmed,S.andEvans,T.G.,2017.“Catastrophichealthcareexpenditureandpovertyrelatedtoout-of-pocketpaymentsforhealthcareinBangladesh—anestimationoffinancialrisk protection of universal health coverage.”Health policy and planning. 32(8), pp.1102-1110.
Knaul,F.M.,Wong,R.,Arreola-Ornelas,H.,Méndez,O.,Bitran,R.,Campino,A.C.,FlórezNieto,C.E.,Giedion,U.,Maceira,D.,Rathe,M.,andValdivia,M.2011.“HouseholdCatastrophicHealthExpenditures:AComparativeAnalysisof12LatinAmericanandCaribbeanCountries.SaludPúblicadeMéxico53:s85-s95.
Knaul,F.M.,Arreola-Ornelas,H.,Mendez-Carniado,O.,Bryson-Cahn,C.,Barofsky,J.,Maguire,R.,Miranda,M.andSesma,S.2006.“Evidenceisgoodforyourhealthsystem:policyreformtoremedycatastrophicandimpoverishinghealthspendinginMexico.”TheLancet,368:1828-41
Kotlikoff,L.J.2018.“MeasuringIntergenerationalJustice.”IntergenerationalJusticeReview11(2).
Lu,J.F.R.,Leung,G.M.,Kwon,S.,Tin,K.Y.,vanDoorslaer,E.,andO’Donnell,O.“HorizontalEquityinHealthCareUtilization:EvidencefromThreeHigh-IncomeAsianEconomies.”EQUITAPProject:WorkingPaperNo.6.
Lustig,N.,etal.2013.“TheImpactofTaxesandSocialSpendingonInequalityandPovertyinArgentina,Bolivia,Brazil,Mexico,PeruandUruguay:AnOverview.”CEQWorkingPaperNo.13.NewOrleans:TulaneUniversity.
Lustig,N.2016.“InequalityandFiscalRedistributioninMiddleIncomeCountries:Brazil,Chile,Colombia,Indonesia,Mexico,PeruandSouthAfrica.”JournalofGlobalizationandDevelopment7(1):17-60.

Lustig,N.2017.“TheImpactofTaxesandSocialSpendingonIncomeDistributionandPovertyinLatinAmerica:AnApplicationoftheCommitmenttoEquity(CEQ)Methodology.”No.1714.NewOrleans:TulaneUniversity,DepartmentofEconomics.
Mackenbach,J.P.,Kunst,A.E.,Cavelaars,A.E.,Groenhof,F.,Geurts,J.J.andEUWorkingGrouponSocioeconomicInequalitiesinHealth,1997.SocioeconomicinequalitiesinmorbidityandmortalityinwesternEurope.Thelancet,349(9066),pp.1655-1659.
Marmot,M.G.,Stansfeld,S.,Patel,C.,North,F.,Head,J.,White,I.,Brunner,E.,Feeney,A.andSmith,G.D.,1991.HealthinequalitiesamongBritishcivilservants:theWhitehallIIstudy.TheLancet,337(8754),pp.1387-1393.
MartinsenL.etal.2017.“DoLessPopulousCountriesReceiveMoreDevelopmentAssistanceforHealthperCapita?Longitudinalevidencefor143countries,1990–2014.”BMJGlobalHealth2018,(3).doi:10.1136/bmjgh-2017-000528
Mitton,C.,Smith,N.,Peacock,S.,Evoy,B.,andAbelson,J.2009.“PublicParticipationinHealthCarePrioritySetting:AScopingReview.”HealthPolicy,91:219-28.
Moser,K.A.,Leon,D.A.andGwatkin,D.R.,2005.Howdoesprogresstowardsthechildmortalitymillenniumdevelopmentgoalaffectinequalitiesbetweenthepoorestandleastpoor?AnalysisofDemographicandHealthSurveydata.Bmj,331(7526),pp.1180-1182.
Mulenga,A.andAtaguba,J.E.O.2017.“AssessingIncomeRedistributiveEffectofHealthFinancinginZambia.”SocialScience&Medicine189:1-10.
Murray,C.J.,Xu,K.,Klavus,J.,Kawabata,K.,Hanvoravongchai,P.,Zeramdini,R.,Aguilar-Rivera,A.M.,andEvans,D.B.2003.“AssessingtheDistributionofHouseholdFinancialContributionstotheHealthSystem:ConceptsandEmpiricalApplication.”HealthSystemsPerformanceAssessment:Debates,MethodsandEmpiricism12.Geneva:WorldHealthOrganization.
O’Donnell,O.,VanDoorslaer,E.,Rannan-Eliya,R.P.,Somanathan,A.,Adhikari,S.R.,Akkazieva,B.,Harbianto,D.,Garg,C.C.,Hanvoravongchai,P.,Herrin,A.N.,andHuq,M.N.2008.“WhoPaysforHealthCareinAsia?”JournalofHealthEconomics27(2):460-475.
O'Neill,K.,Takane,M.,Sheffel,A.,Abou-Zahr,C.andBoerma,T.,2013.Monitoringservicedeliveryforuniversalhealthcoverage:theServiceAvailabilityandReadinessAssessment.BulletinoftheWorldHealthOrganization,91(12),pp.923-931.
OECD.2015.“FiscalSustainabilityofHealthSystems:BridgingHealthandFinancingPerspectives.”
Ottersen,T.andNorheim,O.F.2014.“MakingFairChoicesonthePathtoUniversalHealthCoverage.”OnbehalfoftheWorldHealthOrganizationConsultativeGrouponEquityandUniversalHealthCoverage.BulletinoftheWorldHealthOrganization2014(92):389.doi:http://dx.doi.org/10.2471/BLT.14.139139
Ottersen,T.,Moon,S.,andRøttingen,J.A.2017.“TheChallengeofMiddle-IncomeCountriestoDevelopmentAssistanceforHealth:Recipients,Funders,Both,orNeither?”HealthEconomics,PolicyandLaw12(2):265-284

Ottersen,T.,Kamath,A.,Moon,S.,Martinsen,L.,andRøttingen,J.A.2017.“DevelopmentAssistanceforHealth:WhatCriteriadoMulti-andBilateralFundersUse?”HealthEconomics,Policy,andLaw12(2):223-244.
Ottersen,T.andSchmidt,H.2017.“UniversalHealthCoverageandPublicHealth:EnsuringParityandComplementarity.”AmericanJournalofPublicHealth17(2):248-250.
Petricca,K.andBekele,A.2017.“ConceptualizationsofFairnessandLegitimacyintheContextofEthiopianHealthPrioritySetting:ReflectionsontheApplicabilityofAccountabilityforReasonableness.”DevelopingWorldBioethics00:1–8.https://doi.org/10.1111/dewb.12153
Pietschmann,E.2014.“ForgottenorUnpromising?TheElusivePhenomenonofUnder-aidedCountries,SectorsandSub-NationalRegions.”GermanDevelopmentInstitute,Studies80.http://edoc.vifapol.de/opus/volltexte/2015/5612/pdf/Studies_80.pdf
Rao,M.,Katyal,A.,Singh,P.V.,Samarth,A.,Bergkvist,S.,Kancharla,M.,Wagstaff,A.,Netuveli,G.andRenton,A.,2014.ChangesinaddressinginequalitiesinaccesstohospitalcareinAndhraPradeshandMaharashtrastatesofIndia:adifference-in-differencesstudyusingrepeatedcross-sectionalsurveys.BMJopen,4(6),p.e004471.
RashtriyaSwasthyaBimaYojana(RSBY).2018.OverviewofStateWiseenrolment.http://www.rsby.gov.in/statewise.aspx?state=4
Rechel,B.,Thomson,S.,andVanGinneken,E.2010.“HealthSystemsinTransition:TemplateforAuthors.”WHOfortheEuropeanObservatoryonHealthSystemsandPolicies,Copenhagen.
Resnik,D.B.,MacDougall,D.R.,andSmith,E.M.2018.“EthicalDilemmasinProtectingSusceptibleSubpopulationsfromEnvironmentalHealthRisks:Liberty,Utility,Fairness,andAccountabilityforReasonableness.”TheAmericanJournalofBioethics18(3):29-41.
Restrepo-Méndez,M.C.,Barros,A.J.,Wong,K.L.,Johnson,H.L.,Pariyo,G.,França,G.V.,Wehrmeister,F.C.andVictora,C.G.,2016.Inequalitiesinfullimmunizationcoverage:trendsinlow-andmiddle-incomecountries.BulletinoftheWorldHealthOrganization,94(11),p.794.
RoweG.andFrewerL.J.2005.“ATypologyofPublicEngagementMechanisms.”Science,Technology,andHumanValues30:251-90.
Rumbold,B.,Baker,R.,Ferraz,O.,Hawkes,S.,Krubiner,C.,Littlejohns,P.,Norheim,O.F.,Pegram,T.,Rid,A.,Venkatapuram,S.,andVoorhoeve,A.2017.UniversalHealthCoverage,PrioritySetting,andtheHumanRighttoHealth.TheLancet390(10095):712-714.
Sabik,L.M.andLie,R.K.2008.“PrioritySettinginHealthCare:LessonsfromtheExperiencesof
EightCountries.”InternationalJournalforEquityinHealth7:4.
Saksena,P.,Hsu,J.andEvans,D.B.,2014.Financialriskprotectionanduniversalhealthcoverage:evidenceandmeasurementchallenges.PLoSmedicine,11(9),p.e1001701.
Schedler,A.1999.“ConceptualizingAccountability.”InTheSelf-restrainingState:PowerandAccountabilityinNewDemocracies,editedbyA.Schedler,L.Diamond,andM.F.Plattner.Boulder,Co:LynneRiennerPublishers.

Shapiro,E.andTalmon,N.2017.“ACondorcet-ConsistentParticipatoryBudgetingAlgorithm.”
Simonet,D.2017.“PublicValuesandAdministrativeReformsinFrenchHealthCare.”JournalofPublicAffairs17(3).
Skirbekk,V.,Ottersen,T.,Hamavid,H.,Sadat,N.,andDieleman,J.L.2017.“VastMajorityofDevelopmentAssistanceforHealthFundsTargetThoseBelowAgeSixty.”HealthAffairs36(5):926-930.
Sousa,A.,Dal,M.andCarvalho,C.2012.“Monitoringinequalitiesinthehealthworkforce:thecasestudyofBrazil1991-2005”PLoSOne.7(3):e33399.doi:10.1371/journal.pone.0033399.
Speybroeck, N., G. Paraje, A. Prasad, P. Goovaerts, S. Ebener, D.B. Evans, 2012. "Inequalityindicators of access to human resources for health: measurement issues", GeographicalAnalysis,44(2):151-161,2012.
Steele,C.A.2017.“PublicGoodsandDonorPriorities:ThePoliticalEconomyofDevelopmentAidforInfectiousDiseaseControl.”ForeignPolicyAnalysisp.orx002.
Stewart,E.A.,Greer,S.L.,Wilson,I.,andDonnelly,P.D.2016.“PowertothePeople?AnInternationalReviewofTheDemocratizingEffectsofDirectElectionstoHealthcareOrganizations.”TheInternationalJournalofHealthPlanningandManagement31(2).
Summers,L.2018.“Taxesforhealth:Evidenceclearstheair.”CommentaryinTheLancetTaskforceonNCDsandeconomics.
UnitedNations.2018.“TheSustainableDevelopmentGoals:17GoalstoTransformOurWorld.”http://www.un.org/sustainabledevelopment/sustainable-development-goals
Urquieta-Salomon,JandVillarreal,H.2016.“EvolutionofhealthcoverageinMexico:evidenceofprogressandchallengesintheMexicanhealthsystem.”HealthPolicyandPlanning31,28-36doi10.1093/heapol/czv015
VanDoorslaer,E.andO’Donnell,O.2011.“MeasurementandExplanationofInequalityinHealthandHealthCareinLow-IncomeSettings.InHealthInequalityandDevelopment.London:PalgraveMacmillan.
VanMinh,H.,Phuong,N.T.K.,Saksena,P.,James,C.D.,andXu,K.2013.“FinancialBurdenofHouseholdOut-of-PocketHealthExpenditureinVietNam:FindingsfromtheNationalLivingStandardSurvey2002–2010.”SocialScienceandMedicine96:258-263.
Vassall,A.,Shotton,J.,Reshetnyk,O.K.,Hasanaj-Goossens,L.,Weil,O.,Vohra,J.,Timmermans,N.,Vinyals,L.,andAndre,F.2014.“TrackingAidFlowsforDevelopmentAssistanceforHealth.”GlobalHealthAction7(1):23510.
Verbist,G.andFigari,F.2014.“TheRedistributiveEffectandProgressivityofTaxesRevisited:AnInternationalComparisonAcrosstheEuropeanUnion.”FinanzArchiv:PublicFinanceAnalysis70(3):405-429.
Victora,C.G.,Wagstaff,A.,Schellenberg,J.A.,Gwatkin,D.,Claeson,M.andHabicht,J.P.,2003.Applyinganequitylenstochildhealthandmortality:moreofthesameisnotenough.TheLancet,362(9379),pp.233-241.

Victora,C.G.,Barros,A.J.,França,G.V.,daSilva,I.C.,Carvajal-Velez,L.andAmouzou,A.,2017.Thecontributionofpoorandruralpopulationstonationaltrendsinreproductive,maternal,newborn,andchildhealthcoverage:analysesofcross-sectionalsurveysfrom64countries.TheLancetGlobalHealth,5(4),pp.e402-e407.
Wagstaff,A.andVanDoorslaer,E.,2000.Equityinhealthcarefinanceanddelivery.Handbookofhealtheconomics,1,pp.1803-1862.
Wagstaff,A.,O'Donnell,O.,VanDoorslaer,E.andLindelow,M.,2007.Analyzinghealthequityusinghouseholdsurveydata:aguidetotechniquesandtheirimplementation.WorldBankPublications.
Wagstaff,A.,2008.Measuringfinancialprotectioninhealth(Vol.4554).WorldBankPublications.
Wagstaff,A.andEozenou,P.,2014.CATAmeetsIMPOV:aunifiedapproachtomeasuringfinancialprotectioninhealth[PolicyResearchWorkingPaperSeries:6861].WashingtonDC:TheWorldBank
Wagstaff,A.andLindelow,M.,2014.Arehealthshocksdifferent?EvidencefromamultishocksurveyinLaos.Healtheconomics,23(6),pp.706-718.
Wagstaff,A.,Bredenkamp,C.andBuisman,L.R.,2014.Progressonglobalhealthgoals:arethepoorbeingleftbehind?.TheWorldBankResearchObserver,29(2),pp.137-162.–healthoutcomes;coverage.
Wagstaff,A.,Flores,G.,Smitz,M.F.,Hsu,J.,Chepynoga,K.andEozenou,P.,2017a.Progressonimpoverishinghealthspendingin122countries:aretrospectiveobservationalstudy.TheLancetGlobalHealth.
Wagstaff,A.,Flores,G.,Hsu,J.,Smitz,M.F.,Chepynoga,K.,Buisman,L.R.,vanWilgenburg,K.andEozenou,P.,2017b.Progressoncatastrophichealthspendingin133countries:aretrospectiveobservationalstudy.TheLancetGlobalHealth.
WorldBank.2012.“Mexico’sSocialProtectionSysteminHealthandtheFinancialProtectionofCitizenswithoutSocialSecurity”.WashingtonDC
WorldHealthOrganization.2010.“TheWorldHealthReport2010:HealthSystemsFinancing,thePathtoUniversalCoverage.”Geneva:WHO.
WorldHealthOrganization.2014.Makingfairchoicesonthepathtouniversalhealthcoverage.FinalreportoftheWHOConsultativeGrouponEquityandUniversalHealthCoverage,WHO,Geneva.http://www.who.int/choice/documents/making_fair_choices/en/
WorldHealthOrganizationandtheInternationalBankforReconstructionandDevelopment.2017.“Trackinguniversalhealthcoverage:2017globalmonitoringreport.”TheWorldBank,WashingtonDC.
WorldBank.NigeriaHealthFinancingSystemAssessment-WorldBankDiscussionpaper(forthcoming).WorldBank:Washington,DC

Wong,K.L.,Restrepo-Méndez,M.C.,Barros,A.J.andVictora,C.G.,2017.Socioeconomicinequalitiesinskilledbirthattendanceandchildstuntinginselectedlowandmiddleincomecountries:Wealthquintilesordeciles?.PloSone,12(5),p.e0174823.
Woo,J.,Bova,E.,Kinda,T.,andZhang,Y.S.2017.“DistributionalConsequencesofFiscalAdjustments:WhatDotheDataSay?”IMFEconomicReview,pages1-35.
Xu, K., Evans, D.B., Kawabata, K., Zeramdini, R., Klavus, J. andMurray, C.J., 2003. Householdcatastrophichealthexpenditure:amulticountryanalysis.Thelancet,362(9378),pp.111-117.
Xu, K., Evans, D.B., Kawabata, K., Zeramdini, R., Klavus, J. andMurray, C.J., 2003. Householdcatastrophichealthexpenditure:amulticountryanalysis.Thelancet,362(9378),pp.111-117.
Xu,K.,Evans,D.,Carrin,G.,Aguilar-RiverA.M.,Musgrove,T.,andEvans,T.2007.“ProtectingHouseholdsfromCatastrophicHealthSpending.”HealthAffairs26(4).
Yamin,A.E.,2008.Sufferingandpowerlessness:thesignificanceofpromotingparticipationinrights-basedapproachestohealth.HealthandHumanRights,11:5-22.
Yamin,A.E.2010.“TowardTransformativeAccountability:ApplyingRights-BasedApproachtoFulfillMaternalHealthObligations.”SUR-InternationalJournalonHumanRights,12:95.
Yamin,A.E.2017.«TakingtheRighttoHealthSeriously:ImplicationsforHealthSystems,Courts,andAchievingUniversalHealthCoverage.”HumanRightsQuarterly39(2):.341-368.

#UHCfinance
For more information about theAnnual UHC Financing Forum please visit
http://worldbank.org/uhcfinancingforum