Embed Size (px)
Citation preview

EVAE Q U I N E V I R A L A R T E R I T I S
A MANAGEABLE PROBLEM
UNITED STATES DEPARTMENT OF AGRICULTURE
ANIMAL AND PLANT HEALTH INSPECTION SERVICE
PROGRAM AID NO. 1566

The U.S. Department of Agriculture (USDA) prohibits discrimination in all its programs and
activities on the basis of race, color, national origin, sex, religion, age, disability, political
beliefs, sexual orientation, or marital or family status.
(Not all prohibited bases apply to all programs.) Persons with disabilities who require
alternative means for communication of program information (Braille, large print,
audiotape, etc.) should contact USDA’s TARGET Center at (202) 720–2600 (voice and TDD).
To file a complaint of discrimination, write
USDA, Director, Office of Civil Rights,
Room 326-W, Whitten Building,
1400 Independence Avenue, SW, Washington, DC 20250–9410
or call (202) 720–5964 (voice and TDD).
USDA is an equal opportunity provider and employer.
Mention of companies or commercial products does not imply recommendation or
endorsement by USDA over others not mentioned. USDA neither guarantees nor warrants
the standard of any product mentioned. Product names are mentioned solely to report
factually on available data and to provide specific information.
Issued April 2001
Photo credits:
The horse images on the front cover, page 2 and 3, and the image of the virus vaccine
materials on p.8 were taken by Bob Langrish and are reproduced by permission. The photo-
graph of the depressed horse on p. 6 was taken by coauthor Peter Timoney, of the University
of Kentucky, and is reproduced by permission. On p. 8, the image of the male horse was
taken by Gemma Giannini and that of the female horse, by Martha Bell; both shots are
reproduced by permission. All these images remain under copyright held by the
photographers themselves.
EVAE Q U I N E V I R A L A R T E R I T I S
A MANAGEABLE PROBLEM
1 Dr. Timoney is Director and Frederick Van Lennep Chair in Equine Veterinary Science at
the Maxwell H. Gluck Equine Research Center, Department of Veterinary Science,
University of Kentucky, Lexington, KY 40546. He can be reached via the Internet at
[email protected] or by telephone at (859) 257–1531.
2Dr. Cordes is a Senior Staff Veterinarian with the National Animal Health Staff, Veterinary
Services, Animal and Plant Health Inspection Service, U.S. Department of Agriculture, 4700
River Road, Riverdale, MD 20737. He can be reached via the Internet at
[email protected] or by telephone at (301) 734–3279.
3Dr. McCollum is a professor in equine viral diseases at the Maxwell H. Gluck Equine
Research Center, Department of Veterinary Science, University of Kentucky, Lexington, KY
40546. He can be contacted by telephone at (859) 257–3620.
Peter J. Timoney, M.V.B., M.S., Ph.D., FRCVS1
Timothy R. Cordes, D.V.M.2
William H. McCollum, M.S., Ph.D.3

2 3
T A B L E O F C O N T E N T S
Introduction
Facts and Fiction About EVA
Geographic Distribution of Equine Arteritis Virus
Clinical Outcome of Equine Arteritis Virus Infection
How Equine Arteritis Virus Is Spread
Persistent Equine Arteritis Virus Infection in the Stallion
Economic Significance of EVA
How To Confirm a Diagnosis of Equine Arteritis Virus Infection
Preventing the Spread of Equine Arteritis Virus
Immunization Against EVA
Conclusions
Acknowledgments
Suggested Readings
4
5
9
9
12
13
13
14
16
20
21
24
22
In the past 15 years, few equinediseases have stimulated moreinterest or gained greater interna-tional notoriety than equine viralarteritis (EVA).
The disease was thrust into thelimelight of industry attention following a 1984 epidemic on alarge number of Thoroughbredbreeding farms in Kentucky. Nooutbreaks of EVA had previouslybeen reported in Thoroughbreds in North America. At the time,many people feared that a strain of the causative agent, equinearteritis virus (EAV), had emergedthat was likely to spread withinthe largely antibody-negativeThoroughbred population, causingdisease and extensive outbreaks of abortion. The internationalcommunity took the threat posed by EVA so seriously that itplaced major restrictions on themovement of horses from theUnited States. Many of theserestrictions are still in force. EVAremains a considerable impedi-ment to international trade inequids and semen.
In contrast to how EVA hasbeen regarded internationally, theU.S. horse industry has traditional-ly attached relatively little signifi-cance to this disease. Over the
past several years, however, theAmerican Horse Council,American Association of EquinePractitioners, and United StatesAnimal Health Association havestressed the importance of con-trolling EVA at the national level.Their efforts have been hamperedby the lack of awareness of thedisease and its potential economicconsequences among most sectorsof the Nation’s horse industry.Recent findings from the U.S.Department of Agriculture’s(USDA) National Animal HealthMonitoring Systems Equine ’98Study have confirmed that thegreat majority of those surveyedhad little if any knowledge aboutEVA itself, let alone why it shouldbe prevented or how to do so.
This brochure and companionvideo, produced and directed bythe USDA’s Animal and PlantHealth Inspection Service(APHIS), aim to educate you—the horse owners and breeders ofthe United States—about EVA.Your involvement and support arecritical to the effectiveness of anyindustry-driven disease-controlprogram. We hope you will usethese materials to increase yourgeneral awareness of EVA, gain aclearer understanding of its true
4
I N T R O D U C T I O N
equine viral
arteritis
equine arteritis
virus
EAV vs EVA
is the virus that
causes
E A VE A V
E VA
veterinary medical and economicimportance, and above all, recog-nize that much of what has beensaid about this disease since 1984was misinformation. Based onwhat is currently known about EVAand how to prevent it, spread ofthe disease can be controlled. Tobe successful, however, a controlprogram must be a cooperativeeffort involving members of thehorse industry, private-sector vet-erinarians, and Federal and Stateanimal health officials.
5
FA C T S A N D FI C T I O NAB O U T EVA
Few equine diseases have beenthe subject of more misinforma-tion or misperception than EVA.It is an acute, contagious viral disease known to affect horsesand other members of the equidfamily only. EVA is not transmissi-ble to humans or other domesticspecies. Like influenza andrhinopneumonitis, it is consideredprimarily a viral infection of theequine respiratory tract.
Contrary to the opinion ofsome at the time, the 1984 epi-demic in Kentucky was not thefirst in North America or else-where. The veterinary literaturedetails outbreaks of a clinicallyindistinguishable disease inGermany and Great Britain in thelatter part of the nineteenth cen-tury. The first virologically con-firmed outbreak of EVA in theworld occurred on a Standardbredbreeding farm near Bucyrus, OH,in 1953. Little concern wasexpressed at the time or indeedover the subsequent 30 years inspite of the fact that the virus hadbeen shown to be capable of caus-ing contagious respiratory diseaseand abortion in mares.
In contrast to the mispercep-tion that prevails in some coun-

6
• fever• loss ofappetite• depression
• skin rash, often localized to thecheeks or sides ofthe neck but some-times all over thebody
• nasal discharge
• conjunctivitis
• abortion• pneumonia or pneumoniawith enteritis invery young foals
SIGNS OF EVA
• swelling, most notablyof the legs, scrotum,sheath or mammaryglands or other depend-ent parts of the body
tries, EVA is not a disease thatoccurs primarily in the UnitedStates. Nor is the causal agent,EAV, particularly limited in its dis-tribution in horse populationsthroughout the world.
Considerable confusion stillexists over the incidence of out-breaks of EVA and the clinical out-come in cases of naturally acquiredinfection with the virus. In spite ofits relatively widespread global dis-tribution, EAV is seldom associatedwith outbreaks of disease in sus-ceptible populations of horses orother species of equids. Detailedinvestigation of outbreaks of EVAover the years has confirmed thatthe vast majority of cases of acuteinfection with EAV are asympto-matic. That is, most infections arenot associated with the develop-ment of any observable clinicalsigns of disease. There are indica-tions, however, that the incidenceof EVA has increased over the past10–15 years, due in part to greaterindustry awareness of the disease,more widely available laboratorycapability to diagnose this infec-tion, and continued expansion ininternational trade in horses and semen.
Confusion also prevails over theveterinary medical importance ofEVA. First, it should be empha-sized that most horses naturally
7
infected with EAV display no visible signs of disease. The termEVA refers to a specific diseasesyndrome—a particular set ofclinical signs that certain horsesor other equines acutely infectedwith EAV may develop. The termis not applicable to cases of acuteEAV infection where there is noclinical evidence of disease.
Much misinformation aboutthe medical significance of EVAcan be traced back to reports inthe earlier veterinary literaturethat describe severe disease with acase-fatality rate as high as 40–60 percent, even in older horses. What is frequently notrealized is that these descriptionsrefer to infection in horses with anexperimentally derived variant ofthe virus isolated in 1953. They donot represent the type and severityof clinical disease observed in fieldoutbreaks of EVA. Mortality is veryinfrequent in the field. Mortalityhas been reported in neonatalfoals congenitally infected withthe virus and, uncommonly, infoals up to a few weeks of age.
The vast majority of animalsaffected with EVA make total clini-cal recoveries. In the 40–50 yearssince EVA was first identified, nonaturally occurring, highly patho-genic strains of the virus havebeen reported or isolated.

8
THE MOST COMMON MEANS OF EAV TRANSMISSION
respiratory system
reproductive tract
male female
The virus can betransmitted viafresh-cooled orfrozen semenused in artificialinsemination.
BY BREEDING—Stallions and maresacutely infected with EAVcan also pass the virus totheir breeding partners.This is the only route oftransmission of the virusby the persistently infect-ed carrier stallion.
across the placenta
BY AIR—The respiratory secre-tions of horses acutely infected with EAV carry large quantities of the virus
BY MARE TO UNBORN FOAL—EAV can pass across the placentafrom an infected mare to the foal inher uterus.
GEOGRAPHICDISTRIBUTION OF EAV
EAV is distributed in varioushorse populations throughout theworld. It has been reported fromcountries in North and SouthAmerica, Europe, Africa, Asia,Australia, and New Zealand.Outbreaks of EVA, though rela-tively infrequent, are often associ-ated with the movement of horsesor shipment of semen.Widespread dissemination of thevirus can occur on breeding farmsand at racetracks, sales, or horseshows, where horses are closelycongregated. The global distribu-tion of EAV has been and contin-ues to be influenced significantlyby the international movement ofstallions that are carriers of thevirus and by the shipment ofinfective, fresh-cooled or frozensemen.
The prevalence of EAV infec-tion differs considerably bothamong countries and among par-ticular horse breeds in the samecountry. Various serological sur-veys carried out in the UnitedStates have shown that infectionwith EAV can be endemic in somebreeds (e.g., Standardbreds) butnot in others (e.g., Thoroughbredsand Quarter Horses). There is noevidence, however, that different
9
breeds vary in their inherent sus-ceptibility to infection with EAV.
CL I N I C A L OU T C O M EO F EAV IN F E C T I O N
EVA is principally a disease of therespiratory system that can affecthorses of any age. Importantly,most horses that are naturallyexposed to EAV develop no signsof disease and are consideredasymptomatically infected withthe virus. The clinical outcomefollowing infection with EAV isinfluenced by a variety of virus,host, and environmental factors.Severity of disease is likely to begreater in very young or old horsesand in debilitated animals.
In cases where illness devel-ops, the incubation period is usually 3–7 days but can belonger. Clinical signs vary inrange and severity. Affected ani-mals may exhibit some or most ofthe following:■ Fever;■ Swelling (edema), most notablyof the legs, scrotum, sheath ormammary glands or other depend-ent parts of the body;■ Loss of appetite (anorexia);■ Depression;■ Nasal discharge, initially watery(serous) but frequently becomingmucoid later;
10
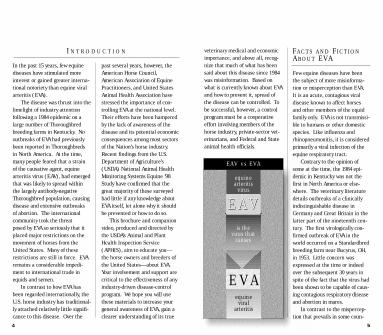
Equine arteritis virus is foundin various horse populationsthroughout the world. It has beenreported from countries in Northand South America, Europe,Africa, Asia, Australia and NewZealand. EVA outbreaks don’toccur often, but when they do,they are frequently associated withthe movement of horses or ship-ment of semen.
Widespread dissemination ofthe virus can occur
on breeding farms and at race-tracks, sales or horse shows,where horses are closely congre-gated. There is growing evidencethat the global distribution of EAVhas been, and continues to be,influenced significantly by theinternational movement of stal-lions that are carriers of the virusand by the shipment of infective,fresh-cooled or frozen semen.
The prevalence of EAVinfection differs con-
I N C I D E N C E
GEOGRAPHIC DISTRIBUTION OF EQUINE ARTERITIS VIRUS
NORTH AMERICA
EUROPE
AFRICA
SOUTHAMERICA
With the increase in internationaltrade of horses andsemen for artificialinsemination, therisk of spreadingequine arteritis virusfrom one equinepopulation to another has grown.
11
■ Conjunctivitis that may beaccompanied by tearing down theface and swelling above or aroundthe eyes;■ Skin rash (urticaria), oftenlocalized to the cheeks or sides ofthe neck but sometimes general-ized over the body;■ Abortion; and■ Pneumonia or pneumonia withenteritis in very young foals.
Many strains of EAV can causeabortion in pregnant mares, withabortion rates varying from 10percent to as high as 70 percent.Abortion occurs late in the acutephase or early in the convalescentphase of the infection and not, assome would believe, months aftervirus exposure has taken place.Abortion has been observed as asequel to either clinical or asymp-tomatic infection with EAV. It isoften the result when an unpro-tected or first-time EVA-vaccinat-ed mare that has very recentlybeen bred with virus-infectivesemen is commingled with one ormore pregnant mares.
Stallions acutely affected withEVA may experience a period oftemporary subfertility that canlast up to 8 weeks. No long-termadverse effects on fertility havebeen reported in recovered stal-lions or in stallions that remainpersistently infected with the
siderably both between countriesand between particular horsebreeds in the same country.Various serological surveys car-ried out in the United States haveshown that infection with EAV canbe endemic in some breeds, suchas Standardbreds, but not in oth-ers, such as Thoroughbreds andQuarter Horses. There is no evi-dence, however, that differentbreeds vary in their inherent sus-ceptibility to infection with EAV.
ASIA
AUSTRALIA
NEWZEALAND

virus. Similarly, there is no scien-tific evidence that mares infectedwith EAV experience any short- orlong-term, virus-related fertilityproblems. Horses in training canexperience a period of impairedperformance while acutely infect-ed with the virus, but fortunatelythis is brief.
Except for EVA in youngfoals—and this occurs very infre-quently—the vast majority ofhorses affected with the diseasemake total clinical recoveries,with or without symptomatic treat-ment. Where indicated, treatmentof cases of EVA is symptomatic andaimed primarily at alleviating theseverity of some of the clinicalsigns of the disease (e.g., controlof fever and reduction of depend-ent edema). Adequate rest duringthe recovery period is important,especially for breeding stallionsand horses in training.
HO W EAV IS SP R E A D
While EAV can be spread amonghorses in a number of ways, themost common routes are respirato-ry (by the acutely infected ani-mal) and venereal (by the acuteor chronically infected stallion).
Large quantities of EAV areshed into the respiratory tract ofacutely infected horses, and the
12
virus spreads to other animalsthrough direct contact withexhaled infective respiratory secre-tions. This is the principal meansof dissemination of EAV during out-breaks at racetracks, shows, sales,and veterinary hospitals. It is alsoan important means of transmis-sion on breeding farms. In addi-tion, EAV can be spread throughvenereal contact with the semen ofan acutely infected stallion or thereproductive tract secretions of anacutely infected mare. A teaserstallion or nurse mare can be apotential sources of infection foroutbreaks on breeding farms.
The chronically infected or car-rier stallion plays a major role invenereal transmission of the viruswhether mares are bred by “livecover” or by artificial insemination.Another danger is venereal spreadof EAV through the use of infective,fresh-cooled or frozen semen.
Mechanical spread of EAV canoccur, though this route is believedto be less common. Virus-contami-nated tack or equipment sharedamong horses can be a source ofthe virus for new hosts, and EAVcan also be transported on thehands or clothing of personnelhandling the animals.
Finally, EAV can be transmittedacross the placenta from an infect-ed pregnant mare to her unborn
foal. In such cases, the fetus, fetalfluids, placenta, and placental flu-ids are plentiful sources of virus.
PE R S I S T E N T EAVIN F E C T I O N I N T H ESTA L L I O N
A variable percentage of stallionsinfected with EAV may becomelong-term carriers and reservoirsof the virus. The carrier state hasbeen identified only in stallionswhose blood is positive for antibod-ies to the virus. Such animalsshow no clinical signs of diseasenor any adverse effects on fertility,in spite of harboring the virus incertain of the accessory sex glands.Duration of virus persistence canvary greatly in individual stallions,ranging from a period of severalmonths to many years. A smallpercentage of carrier stallions suc-cessfully clear the virus from theirreproductive tract and are nolonger a source of infection. EAVis shed constantly in the semen ofcarrier animals, and transmissionof the virus occurs solely by thevenereal route. Transmission ratesas high as 100 percent can takeplace in mares bred by live coveror artificial insemination.
Currently, there is no provennonsurgical means of eliminatingEAV from a carrier stallion’s
reproductive tract.The carrier state has never
been confirmed in stallions vacci-nated with the current modifiedlive-virus vaccine against EVA.Furthermore, mares, geldings, orsexually immature colts do notbecome persistently infected orcarriers of EAV.
EC O N O M I CSI G N I F I C A N C E O F EVA
EVA can have economic conse-quences for both breeding andperformance sectors of the horseindustry.
Direct financial losses result-ing from outbreaks of the diseaseon breeding farms can be summa-rized as follows: ■ Losses due to abortion and/ordisease and death in young foals,■ Decreased commercial value ofstallions that become persistentlyinfected with the virus,■ Reduced demand to breed tocarrier stallions because of theadded expense and inconvenienceinvolved in vaccinating and isolating mares before and afterbreeding,■ Denied export markets for carri-er stallions or virus-infectivesemen, and■ Reduced export markets for fillies, mares, colts, and geldings,
13
14
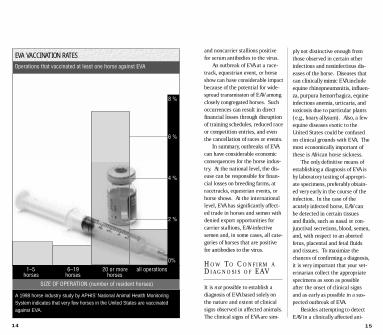
A 1998 horse industry study by APHIS’ National Animal Health MonitoringSystem indicates that very few horses in the United States are vaccinatedagainst EVA.
8 %
6 %
4 %
2 %
0%
1–5 6–19 20 or more all operationshorses horses horses
SIZE OF OPERATION (number of resident horses)
Operations that vaccinated at least one horse against EVA
EVA VACCINATION RATESand noncarrier stallions positivefor serum antibodies to the virus.
An outbreak of EVA at a race-track, equestrian event, or horseshow can have considerable impactbecause of the potential for wide-spread transmission of EAV amongclosely congregated horses. Suchoccurrences can result in directfinancial losses through disruptionof training schedules, reduced raceor competition entries, and eventhe cancellation of races or events.
In summary, outbreaks of EVAcan have considerable economicconsequences for the horse indus-try. At the national level, the dis-ease can be responsible for finan-cial losses on breeding farms, atracetracks, equestrian events, orhorse shows. At the internationallevel, EVA has significantly affect-ed trade in horses and semen withdenied export opportunities forcarrier stallions, EAV-infectivesemen and, in some cases, all cate-gories of horses that are positivefor antibodies to the virus.
HO W TO CO N F I R M ADI A G N O S I S O F EAV
It is not possible to establish adiagnosis of EVA based solely onthe nature and extent of clinicalsigns observed in affected animals.The clinical signs of EVA are sim-
15
ply not distinctive enough fromthose observed in certain otherinfectious and noninfectious dis-eases of the horse. Diseases thatcan clinically mimic EVA includeequine rhinopneumonitis, influen-za, purpura hemorrhagica, equineinfectious anemia, urticaria, andtoxicosis due to particular plants(e.g., hoary allysum). Also, a fewequine diseases exotic to theUnited States could be confusedon clinical grounds with EVA. Themost economically important ofthese is African horse sickness.
The only definitive means ofestablishing a diagnosis of EVA isby laboratory testing of appropri-ate specimens, preferably obtain-ed very early in the course of theinfection. In the case of theacutely infected horse, EAV can be detected in certain tissues and fluids, such as nasal or con-junctival secretions, blood, semen,and, with respect to an abortedfetus, placental and fetal fluidsand tissues. To maximize thechances of confirming a diagnosis,it is very important that your vet-erinarian collect the appropriatespecimens as soon as possibleafter the onset of clinical signsand as early as possible in a sus-pected outbreak of EVA.
Besides attempting to detectEAV in a clinically affected ani-

mal, your veterinarian can confirma diagnosis of EAV infection bytesting paired blood samples forthe presence of antibodies to thevirus. Have your veterinarian col-lect the initial blood sample asearly as possible in the course ofthe disease and obtain a secondsample 3–4 weeks later. Althoughhighly reliable, laboratory exami-nation of paired (acute and conva-lescent) blood samples suffersfrom the disadvantage of not pro-viding a rapid diagnosis of EVA.
Screening of a stallion for thecarrier state initially involves hav-ing your veterinarian take a bloodsample for laboratory testing todetermine if the animal is positiveor negative for serum antibodies toEAV. Only stallions testing positive(neutralizing antibody level ortiter of 1:4 or greater) without anyhistory of previous vaccinationagainst EVA should be consideredpotential carriers of the virus. Allantibody-positive nonvaccinatedstallions should be screened forpresence of the carrier state byeither (1) attempting detection ofEAV in semen in the laboratory, or(2) subjecting them to a test-breeding program involving twoseronegative mares and monitor-ing the mares for the developmentof serum antibodies to the virus upto 28 days after breeding. Virus
16
detection in the laboratory is inexpensive and safe and providesa timely result. It can be attempt-ed at any time before, during, orafter the breeding season becausecarrier stallions shed EAV con-stantly in their semen. It shouldbe reemphasized that semen col-lected for virological examinationmust contain the sperm-rich frac-tion of the ejaculate.
Specimens from a suspectedoutbreak of EVA or from a stallionthat is a putative carrier of EAVshould be appropriately handledas advised by your veterinarianand submitted to a laboratoryknown to have the diagnosticcapability and proficiency in test-ing for this infection.
PR E V E N T I N G T H ESP R E A D O F EAV
Control ProgramsAlthough not generally realized
by many in the horse industry, EVAis a very controllable disease.Controlling its spread involvesminimizing or eliminating direct or indirect contact of susceptible horses with varioussecretions, excretions, or tissuesof infected horses.
Based on the outcome of agreat deal of scientific investiga-tion of the natural and experimen-
tally reproduced disease and thecausal agent, EAV, various industrygroups have developed effectiveprograms for the prevention andcontrol of EVA. Integral to the success of such programs isthe availability of a safe and effective vaccine (ARVAC®, Ft.Dodge Animal Health) that stimu-lates a high level of protectionagainst the disease.
Current control programs arefocused primarily on restrictingspread of the virus in breedinghorse populations to (1) preventoutbreaks of EAV-related abortionand/or illness and death in veryyoung foals and (2) minimize therisk of establishment of the carrierstate in stallions. Notwithstandingthe potential economic conse-quences involved, there are noongoing programs targeted at pre-venting the introduction orrestricting the spread of EAVamong performance horses eitherat racetracks, equestrian events,or horse shows.
EVA can be effectively con-trolled if you observe sound man-agement practices and implementa selective vaccination programagainst the disease. Current pro-grams have centered largelyaround the importance of the car-rier stallion as a reservoir of EAVand the means whereby the virus
17
can be widely disseminated in sus-ceptible breeding populations.The following specific preventiveand control measures can help youminimize the spread of EVA:■ Isolate all new arrivals and
horses returning from other farms,sales, or racetracks for 3 to 4weeks.■ If at all possible, segregate preg-nant mares from other horses onthe farm and maintain mares insmall groups until they havefoaled.■ Prior to the start of each breed-ing season, blood-test all newbreeding stallions for the presenceof antibodies to EAV.■ Have the semen of any antibody-positive, nonvaccinated stallionlaboratory-tested to identify anycarrier animals.■ Annually vaccinate all noncarri-er breeding stallions at least 4weeks prior to the start of eachbreeding season.■ Maintain any EAV carrier stal-lions in physical isolation.■ Observe strict hygienic precau-tions when breeding or collectingfrom carrier stallions to avoid therisk of inadvertent transfer ofinfection through indirect contactwith virus-contaminated objects.■ Restrict breeding EAV carrierstallions to only vaccinated maresor mares that have previously test-

ed positive for naturally acquiredantibodies to the virus.■ Vaccinate EAV antibody-negativemares against EVA at least 3 weeksprior to breeding to a known carri-er stallion or with virus-infectivesemen. Mares do not have to berevaccinated if they require to berebred to the same or another car-rier stallion.■ For 3 weeks after they havebeen bred to a carrier stallion, iso-late mares vaccinated for the firsttime against EVA from all butknown EAV antibody-positive ani-mals. It is especially important toavoid contact between such maresand other pregnant mares, towhich they can spread the virus bythe respiratory route.
In breeds in which EAV infection is endemic (e.g.,Standardbreds or variousWarmblood breeds), we stronglyrecommend that you vaccinate allcolts (immature male foals)between 6 and 12 months of ageagainst EVA. This practice willminimize, if not eliminate, the riskof their becoming carriers of thevirus at a later date. If rigorouslyimplemented over a period ofyears, such a vaccination strategywill lead to a very significantreduction in the number of carrierstallions and largely eliminate theprimary reservoir of EAV.
18
There is a very real danger of introducing EAV into a suscepti-ble horse population through the use of infective, fresh-cooledor frozen semen. In light of thesignificant risk involved, it isimportant that you take the pre-liminary step of determining thevirus infectivity status of semenused for artificial insemination,especially if it has been importedfrom abroad. The precautions youshould take with mares artificiallyinseminated with EAV containingsemen are identical to those rec-ommended for mares bred by livecover to a carrier stallion.
In an effort to promote greaternational control of EVA, and bear-ing in mind the important rolethat the carrier stallion plays inthe dissemination of EAV, theAmerican Horse Council formed a working group in September1996 to develop guidelines forbreeding a mare to an EVA-shed-ding stallion. The working groupincluded representation from thefollowing breed organizations: theAmerican Quarter Horse Associa-tion, the U.S. Trotting Association,the Tennessee Walking HorseBreeders & Exhibitors Association,the International Arabian HorseAssociation, the Appaloosa HorseClub, the Federation of NorthAmerican Sport Horse Registries,
and the Jockey Club. The groupalso included Dr. Ralph Knowles,of the Maryland Department ofAgriculture and chairman of theUnited States Animal HealthAssociation’s Committee onInfectious Diseases of Horses; Dr. Don Lein, director of theVeterinary Diagnostic Laboratoryat Cornell University; and Dr. Don L. Notter, Kentucky State Veterinarian.
The overall goal of the working group was to develop avoluntary, industry-driven protocolto assist breeders in preventingthe spread of EVA. The guidelines,released in August 1997, were sub-sequently endorsed by theAmerican Association of EquinePractitioners and the UnitedStates Animal Health Association.They are available at theAmerican Horse Council’s Website(www.horsecouncil.org). Click on the Equine HealthAdvisory button.
Action To Be Taken in theEvent of an Outbreak of EVA
When dealing with a suspectedoutbreak of EVA, you should makeevery effort to restrict spread ofthe virus and minimize potentialeconomic losses from the disease.Take the following measures inthe case of an outbreak on abreeding farm:
19
■ Promptly isolate all affectedhorses.■ Notify your veterinarian imme-diately.■ In consultation with your veteri-narian, seek laboratory confirma-tion of a diagnosis as soon aspossible.■ In the case of abortion or deathin a newborn foal, place the pla-centa, fetus, or foal in a leak-proofbag, keep cold (not frozen), anddispatch to the nearest qualifieddiagnostic laboratory.■ Disinfect stall, any equipment,or other potentially contaminatedfacilities using a phenolic disinfec-tant. After treatment with disin-fectant, dispose of any bedding bycomposting in an area away fromother horses.■ Using the antiseptic recommend-ed by your veterinarian, wash downthe hindquarters and tail of anymare that has aborted and isolateher from other horses for 4 weeks.■ Restrict movement of horsesonto or off the affected premises. ■ Suspend breeding operationsuntil the outbreak is over and noti-fy owners of mares on the affectedpremises. You can safely breedmares affected with EVA later inthe same breeding season oncethey have fully recovered from thedisease and there is laboratoryconfirmation the outbreak is over.

20
■ Vaccinate all at-risk horses.■ Notify the State Veterinarian orappropriate regulatory agency ofthe outbreak.
Measures to be taken in theevent of an outbreak of EVA at aracetrack, equestrian event, orhorse show are broadly similar tothose recommended for dealingwith an outbreak on a breedingfarm. Place major emphasis onisolating affected animals,restricting movement in and outof the facility, and vaccinating allat-risk animals at the earliestopportunity as advised by yourveterinarians, working in consul-tation with the State Veterinarianand other regulatory officials.
IM M U N I Z AT I O NAG A I N S T EVA
In sharp contrast to the vastmajority of other equine infectious diseases, infection withEAV stimulates a very strong anddurable protective immunityagainst EVA. This immunity canresult from natural exposure tothe virus or from vaccinationagainst the disease.
At the present time, there isonly one commercially availablevaccine against EVA in NorthAmerica. ARVAC is a modified
live-virus vaccine containing anexperimentally derived, highlyattenuated strain of EAV that issafe and very effective when usedin accordance with the manufac-turer’s recommendations. Haveyour veterinarian administer thevaccine to stallions at least 4weeks prior to the start of thebreeding season. Extensive use of the vaccine since 1985 hasfailed to reveal any evidence thatthe vaccine virus is shed in thesemen or that it can establish thecarrier state in the vaccinatedstallion. We do not recommendthat you use the vaccine in preg-nant mares or in foals less than 6weeks of age unless the risk fornatural infection with EAV is high,and then only on the advice ofyour veterinarian.
Horses immunized with themodified live-virus vaccine againstEVA on two or more occasionsdevelop high antibody titers to thevirus equivalent to those observedin cases of naturally acquiredinfection. Protection afforded byvaccination is considered to lastfor at least several years.
21
We hope that the information inthis brochure and in the compan-ion video will help promote greaterindustry awareness of EVA and dis-pel much of the misinformationthat has prevailed since the epi-demic in Kentucky in 1984. EVAcan be a source of considerableeconomic loss, especially for thehorse breeding industry. It is hightime, therefore, that a more rigor-ous effort be made to achievegreater control over this infectionat the national level.
The success of any voluntaryprevention and control programagainst EVA, however, will be criti-cally dependent on your involve-ment and support and that of othermembers of the horse industryworking in cooperation with veteri-narians and Federal and State ani-mal health officials. The organiza-tions and individuals who producedthis brochure and companion videodid so to convince you of the needto participate in such a programand reduce the prevalence of whatis a very controllable disease in theU.S. horse population.
CO N C L U S I O N S

Cole, J. R.; Hall, R. F.; Gosser, H. S.,et al. 1986. Transmissibility andabortigenic effect of equine viralarteritis in mares. Journal of theAmerican Veterinary MedicalAssociation 189(7): 769–771.
Collins, J. K.; Kari, S.; Ralston, S. L.,et al. 1987. Equine viral arteritis ata veterinary teaching hospital.Preventive Veterinary Medicine 4:389–397.
Glaser, A. L.; de Vries, A.A.F.;Rottier, P.J.M., et al. 1996. Equinearteritis virus: a review of clinicalfeatures and management aspects.The Veterinary Quarterly 18(3):95–99.
Golnik, W.; Michalska, Z.; Michalak,T. 1981. Natural equine viral arteri-tis in foals. Schweizer Archiv FurTierheilkunde 123: 523–533.
McCollum, W. H. 1970. Vaccinationfor equine viral arteritis. In: Equineinfectious diseases II, proceedingsof the 2nd international conference;16–18 June 1969; Paris, France.Basel, SW: Karger: 143–151.
22
McCollum, W. H.; Swerczek, T. W.1978. Studies of an epizootic ofequine viral arteritis in racehorses.Journal of Equine Medicine andSurgery 2: 293–299.
McCue, P. M.; Hietala, S. K.;Spensley, M. S., et al. 1991.Prevalence of equine viral arteritisin California horses. CaliforniaVeterinarian March–April: 24–26.
Scollay, M. C.; Foreman, J. H. 1993.An overview of the 1993 equineviral arteritis outbreak at ArlingtonInternational Racecourse. In: 39thannual convention, proceedings;5–8 December 1993; San Antonio,TX. Lexington, KY: AmericanAssociation of Equine Practitioners:255–256.
Timoney, P. J. 1984. Clinical, viro-logical and epidemiological fea-tures of the 1984 outbreak ofequine viral arteritis in theThoroughbred population inKentucky, USA. In: Proceedings ofthe Grayson Foundation interna-tional conference of Thoroughbredbreeders organizations on equineviral arteritis; 31 October – 1 November 1984; DromolandCastle, Co. Clare, Ireland.Lexington, KY: Grayson Jockey ClubResearch Foundation: 24–33.
SU G G E S T E D RE A D I N G S
Timoney, P. J. 1999. Equine viralarteritis in perspective: fact vs. fic-tion. In: Proceedings of the sixthWorld Equine Veterinary Congress;30 September–3 October 1999;Paris, France. Reims, FR:Boehringer Engelheim: 167–170.
Timoney, P. J.; McCollum, W. H.1993. Equine viral arteritis.Veterinary Clinics of North America:295–309.
Timoney, P. J.; McCollum, W. H.;Murphy, T. W., et al. 1987. The carri-er state in equine arteritis virusinfection in the stallion with specif-ic emphasis on the venereal modeof virus transmission. Journal ofReproduction and Fertility 35:95–102.
Timoney, P. J.; McCollum, W. H.;Roberts, A. W. 1987. Detection ofthe carrier state in stallions persist-ently infected with equine arteritisvirus. In: Proceedings of the annualmeeting of the American Associa-tion of Equine Practitioners; 29November–3 December 1986;Nashville, TN. Lexington, KY:American Association of EquinePractitioners: 57–65.
23
Timoney, P. J.; McCollum, W. H.;Vickers, M. L. 1998. The rationalefor greater national control of EVA.Equine Disease Quarterly 7(1):2–3.
Timoney, P. J.; Umphenour, N. W.;McCollum, W. H. 1988. Safety eval-uation of a commercial modifiedlive equine arteritis virus vaccinefor use in stallions. In: Powell, D. G., ed. Equine infectious dis-eases V. Proceedings of the 5thinternational conference; 7–10October 1987; Lexington, KY.Lexington, KY: The UniversityPress of Kentucky: 19–27.
U.S. Department of Agriculture,Animal and Plant Health Inspec-tion Service. 2000. Equine viralarteritis (EVA) and the U.S. horse industry. N315.0400. Ft.Collins, CO: U.S. Department ofAgriculture, Animal and PlantHealth Inspection Service,Veterinary Services, Centers forEpidemiology and Animal Health,National Animal Health MonitoringSystem. 34 p.

We wish to thank those individuals and groups who provided valuable suggestions and support during the develop-ment of the video “Equine ViralArteritis: A Manageable Problem,”especially: Amy Mann and theAmerican Horse Council’s EVAworking group; Ralph Knowles and the United States AnimalHealth Association’s InfectiousDiseases of Horses Committee;Rusty Ford, manager of equine programs at the Kentucky
Department of Agriculture’sDivision of Animal Health; andUSDA’s EVA review committee.
24
Funding to produce the videoand this brochure was provided byUSDA, APHIS, Veterinary Services.We gratefully acknowledge the sup-port of Primedia Publications, pub-lishers of EQUUS magazine, in sup-plying the artwork used in thebrochure and on the video case andin preparing the layout of thesepublications. All illustrations arecopyrighted by PrimediaPublications, Gaithersburg, MD,and may not be reproduced withouttheir written permission. Thehorse images used in some of theseillustrations remain under copy-right by the original photographers.
AC K N O W L E D G M E N T S
![[Product Monograph Template - Schedule D] · The S/D treatment step is effective at inactivating known lipid-enveloped viruses such as equine encephalitis, equine arteritis, West](https://img.dokumen.tips/doc/110x75/5f4ad3e18e18f130307ec42c/product-monograph-template-schedule-d-the-sd-treatment-step-is-effective-at.jpg)