Embed Size (px)
Citation preview

1
REQUEST FOR PROPOSALS
SAYANA PRESS SELF-INJECTION STUDY IN MALAWI
RFQ Date of Issuance: 09/ 3 / 14
Due Date for Questions: 09/ 15 / 14
Due Date for Proposals: 09/ 25 / 14
Period of Performance: October 15, 2014 – December 30, 2016 Background
Sayana® Press is a subcutaneous formulation of depot medroxyprogesterone acetate (DMPA) in a
prefilled, auto-disabled injection system called Uniject (Pfizer, Inc., USA). Sayana Press was registered
with the Medicines and Health Care Products Regulatory Agency (MHRA) and several other national
regulatory agencies. Recent FHI 360 studies in Uganda and Senegal found that a high percentage (≥80%)
clients and providers preferred Sayana Press over the usual DMPA intramuscular (DMPA-IM) injection
[1,2]. These studies provided evidence that Sayana Press can be safely introduced into family planning
programs and administered by trained community health workers, with expectation of client uptake.
Work is currently underway to introduce the delivery of Sayana Press through health care providers in
Uganda, Senegal, and other select countries. The potential advantages of Sayana Press include:
Ease of administration—to allow use by health workers who do not normally give injections
Single dose—to minimize wastage and facilitate outreach to individual clients
Prefilled—to ensure the correct dose is given and simplify procurement and logistics
All in one—to eliminate need to bundle vials and syringes and to prevent potential mismatches at the service delivery point
Nonreusable—to minimize patient-to-patient transmission of blood borne pathogens through needle reuse
Compact size—for easy transport, storage, and disposal
The addition of this method is anticipated to aid in improving provision of family planning services in
low-resource settings. As such, Sayana Press could be particularly useful in a country such as Malawi
where injectable contraception is the most common method used but the contraceptive prevalence rate
for modern methods is currently only 42% and the total fertility rate has only declined from 6.7 in 1992
to 5.7 in 2010 [3,4] due to a number of factors affecting access to family planning services, including
distance to clinics and health care worker shortages.

2
A barrier to rapid programmatic uptake of Sayana Press is its anticipated higher cost relative to DMPA-
IM. Costs can be significantly reduced if Sayana Press is self-administered, a viable practice given its
simplified delivery system and subcutaneous administration route. Self-administration may attract new
family planning users, including through the private sector, and reduce costs to serve existing DMPA
users through decreased operational costs and more efficient use of resources such as providers’ time.
Moreover, the opportunity costs for women would be reduced because they would not need to travel as
often to receive a re-injection from a health care provider.
DMPA clients and providers are ready to explore the potential of self-injection of Sayana Press. After
administering Sayana Press during the FHI 360 acceptability studies providers spontaneously discussed
the potential for self-injection of this method [1]. Additionally, almost half of Ugandan clients who
received Sayana Press (45%) were moderately or very willing to self-inject the method. In Senegal,
where all the clients were recruited at clinics, over a fifth (22%) said they were moderately or very
willing to self-inject [2].
Previous research showed that self-injection of subcutaneous (SC) DMPA in a pre-filled glass syringe
(known as Sayana®, also manufactured by Pfizer, Inc. USA) was feasible and safe. In a trial conducted in
New York City, women were randomized to self-administration or clinic administration of DMPA-SC. All
participants but one eligible for enrollment were successful at self-administering DMPA-SC and
uninterrupted continuation rates were high (47% at 12 months) compared to typical DMPA continuation
rates. Continuation rates and DMPA serum levels were similar in the self-administered and clinic
administered groups [5].
A study conducted in a large family planning clinic in Edinburgh, Scotland found self-administration of
DMPA-SC feasible and associated with similar continuation rates and satisfaction to clinician-
administered DMPA-IM [6]. In this study, all self-injections were given within the appropriate interval.
A non-comparison study conducted in Planned Parenthood clinics in Florida found continuation of self-
injected DMPA-SC high (74%) at the fourth injection [7]. Participants in this study reported the injection
to be easy and convenient and were likely to recommend self-administration to other women.
Given this body of data, self-injection of Sayana Press appears to be a feasible method of birth control
that may be adopted by a significant number of users which in turn, may drive down the cost, a
significant factor in the adoption of any contraception in low-resource settings such as Malawi.
However, the feasibility of Sayana Press self-injection and the potential for this practice to increase
contraceptive continuation has never been assessed in family planning programs in low-resource
settings. The Malawi Ministry of Health (MOH) and the United States Agency for International
Development (USAID) Malawi Mission requested the Advancing Partners and Communities (APC) project
to assess self-injection of Sayana Press to inform their decision-making for procurement of Sayana Press
and distribution through the health system in Malawi. This research in Malawi is timely given that
injectables are the most popular method [3,8], but so is discontinuation with 33% of injectable users
stopping use of the method within the first 12 months while still in need of family planning [8]. While
side effects are the main reason for discontinuation (14% of all DMPA users discontinue due to side
effects in Malawi), service delivery factors, especially in rural areas, impede access to DMPA re-injection

3
[8]. If self-injection is found feasible, the results from this research will inform self-injection training
materials, messages for providers and clients, and future scale-up efforts in Malawi and elsewhere in
sub-Saharan Africa.
Approach and Objectives
FHI 360, through the Advancing Partners and Communities (APC) Project, will conduct a study in Mangochi District Malawi with the primary objective to compare continuation rates between women who self-inject Sayana Press compared to women who receive Sayana Press injections from a provider. Secondary research objectives include:
1) To compare reported side effects between the two study groups 2) To compare pregnancy rates between the two study groups 3) To describe experiences of women who self-inject Sayana Press 4) To describe experiences and recommendations of family planning providers who train
women to self-inject Sayana Press Under the guidance of FHI 360, the Service Provider will implement a randomized control trial in Mangochi district of Malawi. The trial will be conducted in full compliance with Good Clinical Practice (GCP) standards. 734 eligible women attending Ministry of Health (MOH) family planning clinics or seeking family planning services from clinic family planning providers or Health Surveillance Assistants (HSAs) involved in the study will be randomized to receive either: (1) Sayana Press administered by a family planning provider, or (2) training on how to self-inject Sayana Press and the opportunity to self-inject the method at home. The eligibility criteria will be: women, aged 18-40, in general good health, able to understand and willing to sign an informed consent document, willing to provide contact information for follow-up visits and participate in up to 4 follow-up visits over the course of a year, medically eligible to receive Sayana Press according to the WHO Medical Eligibility Criteria, interested in using DMPA and willing to take Sayana Press, and willing to be randomized into one of two study arms. To enroll, new DMPA users will need to have a menstrual period that started within the past 7 days. During the enrollment visit women in the self-injection arm will be trained by family planning providers (including HSAs) to self-inject Sayana Press and will self-inject Sayana Press under supervision. Participants who successfully self-inject Sayana Press under supervision will then be given three Sayana Press units to take home. The study family planning providers will collect baseline data at the enrollment visit for all participants. In both arms, trained data collectors will collect data regarding continuation status, acceptability, adverse events, and experiences with side effects every three months for a year. These follow-up interviews will occur shortly after participants’ re-injection date (post 3-, 6-, and 9-months). 12-month continuation rates will be calculated using survival analysis methods. We will also track the numbers of women: invited to participate in the study, participated in the study, self-injected at the enrollment visit, and self-injected on-time during the three follow-up interviews. Approximately 12 months after the enrollment visit injection, or when participants discontinue use of Sayana Press (whichever event occurs first), data collectors will conduct a final visit to assess whether

4
the participants had any medical problems since their last visit and to have the participant take a pregnancy test. In addition to this quantitative data, qualitative interviews will be conducted with 30 randomly selected participants in the self-injection arm to understand participants’ strategies for remembering when to re-inject, fidelity to Uniject activation procedures, safe injection practices, and storage and waste disposal procedures. We will also conduct interviews with 12 randomly selected family planning providers to describe their techniques and recommendations for training and supporting women to self-inject Sayana Press.
Scope of Work
The Service Provider will be responsible for all coordination and logistical tasks related to the planning, scheduling, and relationship-building necessary for successful completion of data collection. It is expected that the Service Provider will provide a site Principal Investigator , Study Coordinator, Field Medical Monitor (must have a current license to practice as a nurse/midwife or MD) and data collectors to complete the data collection and data transfer to FHI 360. While we require the Study Coordinator and Field Medical Monitor be physically present in the study district during the data collection period and the Study Coordinator to provide frequent updates to FHI 360, the Service Provider may suggest an alternative staffing plan with appropriate justification. The Service Provider will make arrangements for the training of all study personnel, including study providers which will be recruited from select MOH family planning clinics in the study district. The master training will be led by FHI 360, but the trainings for the study providers will be led by the Service Provider. The Service Provider will also provide logistical support to FHI 360 personnel who will make regular visits to the study clinics. Project deliverables include electronic copies of all documents and notes, all data, audio recordings, and meeting notes. Specific responsibilities and tasks include:
Provide feedback on protocol, 6 Case Report Forms (CRFs), and 2 interview guides
Translate 3 informed consent forms (1 ICF of 7 pages, 2 ICFs of 3 pages each), 6 CRFs (ranging from approximately 1- 9 pages), and two qualitative interview guides (of approximately 2 pages each) into local language(s) as necessary
Prepare and submit local IRB application and follow-up as necessary until approval is obtained. Please budget for applicable IRB fees.
Facilitate appropriate insurance coverage for clinical trial participants according to national guidelines. Please budget for applicable insurance fees.
Recruit and supervise study staff
FHI 360 will work with the MOH to identify 6 family planning facilities to participant in the study (the District Hospital in Mangochi and 5 other MOH health facilities that provide family planning services in Mangochi). The Service Provider will be responsible for recruiting a total of 20 clinic-based family planning providers from these 6 study clinics. Ten providers should be from the District Hospital and two providers from each of the 5 other health facilities. We estimate that the District Hospital can enroll about 300 participants in 3 months and the rest of the sample could be shared amongst the 5 health facilities (average of 87 women for 3 months).
Recruit 20 Health Surveillance Assistants (HSAs) who work in the communities surrounding the 6 study clinics.

5
Submit copies of certificates proving all study staff, including data collectors, Field Medical Monitor, Study Coordinator, site Principal Investigator and study providers (clinic-based providers and HSAs), completed and passed the tests for research ethics (RE) and ICH Good Clinical Practice (GCP). The RE and GCP curriculums have to be approved by FHI 360. Examples of acceptable curriculums include Collaborative Institutional Training Initiative (CITI) Program (available at: https://www.citiprogram.org/) and online FHI 360 online research ethics training curriculum (available at: http://www.fhi360.org/sites/all//libraries/webpages/fhi-retc2/index.html). The Service Provider is expected to provide this training to any study staff who do not have current (within the last three years) certificates.
Submit copies of medical credentials or certificates for all study providers, the Field Medical Monitor, and site Principal Investigator (if applicable).
All study specific training will occur after RE and GCP training certificates and medical credentials are approved by FHI 360.
Arrange for FHI 360-led master training of the site Principal Investigator, Study Coordinator, Field Medical Monitor, and data collectors
o 2 weeks (10 consecutive business days) in length o The first 5 days will be classroom-based o Arrange for a pretest of the instrument in field sites during the last 5 days
Conduct the provider trainings (we recommend this training is led by the Study Coordinator and Field Medical Monitor) on the following topics:
o RE and GCP, if they don’t currently have this training o Study protocol (we suggest 1.5 days) o Sayana Press self-injection (we suggest 0.5 days) o We recommend conducting this training separately for the clinic-based providers and
the HSAs
Introduce study to the communities by providing a study overview in the communities surrounding the 6 study clinics
Enrollment interview – ensuring study providers conduct enrollment/eligibility interview and self-injection training (when applicable) to enroll 734 participants.
Follow-up, behavioral interviews conducted by data collectors (3 interviews for each of the 734 participants, occurs every 3 months at study clinic or at the place of the participants’ choosing, but should all be in Mangochi District)
Final visits for each participant, with final questions asked and pregnancy test conducted at study clinic or at the place of the participants’ choosing
Double data entry for up to 2,202 Follow-Up Interview Behavioral Forms (734 participants x 3 interviews) into EpiData data entry program. The data entry program (for the Follow-Up Interview Behavioral Form) will be developed by FHI 360 in English, but Service Provider needs to supply computers for data entry and download the EpiData program from the Internet (http://www.epidata.dk/download.php) prior to the master training
Perform data quality checks and back-up data onto thumb drive daily
Send EpiData datasets to FHI 360 on a weekly basis via Leapfile
Conduct, verbatim transcribe and translate into English (if necessary) in-depth interviews with 12 study providers (one hour in length, conducted at study clinic or at the place of the participants’ choosing)
Conduct, verbatim transcribe and translate into English (if necessary) in-depth interviews with 30 randomly selected participants from the self-injection arm (1 hour in length, conducted at study clinic or at the place of the participants’ choosing)

6
Scan and email completed Case Report Forms (CRFs) to FHI 360 on a weekly basis. We anticipate having 5 CRFs for each enrolled participant that will need to be scanned and emailed (Enrollment, Follow-Up Clinical Form, Final, Adverse Events, and Pregnancy). The Follow-Up Interview Behavioral Form will be entered into the EpiData program rather than scanned and emailed.
Collect adverse event data, at scheduled and unscheduled visits, from enrollment through until 3 months after the participant’s last Sayana Press injection. Data collectors will collect AE information (except for relatedness) and the site Principal Investigator or appropriate designee evaluate all reported or observed AEs and assure that appropriate health care or referral is provided. All AEs will be assessed for seriousness and severity, relationship to study drug, and outcome to date.
Report serious adverse events (SAEs) and pregnancies to FHI 360 within 24 hours of learning about the event
Arrange for dissemination meeting (1 day meeting with 20 stakeholders)
The Service Provider should budget for the following supplies:
Six (6) Locked File Cabinets (one in each study clinic)
Twenty (20) locking supply storage boxes for HSAs to store Sayana Press and study documents
Cost for printing of the following IDI guides and ICFs:
o IDI guide 1: 12 x 2 pages = 24 pages
o IDI guide 2: 30 x 2 pages = 60 pages
o Main study ICF: 807 x 7 pages = 5,395 pages
o IDI 1 ICF: 15 x 3 pages = 45 pages
o IDI 2 ICF: 39 x 3 pages = 117 pages
o Total = approximately 5,644 pages
Printing costs for all training materials
Small cardboard sharps disposal boxes for study participants enrolled in the self-injection arm
Pregnancy tests for use at final visit and where appropriate throughout the study for cases
where participants return to the clinic with a suspected pregnancy
Study participant compensation – 734 participants x 5 interviews x $3 = $11,010
In-depth interview compensation – 12 study providers x $6 =$72
In-depth interview compensation – 30 self-injector participants x $6 = $180
Provider Incentives for recruitment - $10/month for 3 months x 40 study providers = $1,200
Responsibilities of FHI 360:
1. Creation and provision of electronic version of protocol, study manual, all CRFs, interview guides and consent forms, in English
2. Selection of 6 study clinics 3. Provision of EpiData data entry program (for the Follow-Up Interview Behavioral Form) 4. Provision of randomization envelopes 5. Provision of printed Case Report Forms (CRFs) in English 6. Trainers for master training of the site Principal Investigator , Study Coordinator, Field
Medical Monitor, and data collectors 7. Provision of electronic training materials for use during the study provider trainings (to be
conducted by Service Provider)

7
8. Provision of electronic version of Sayana Press self-injection training materials (Service Provider needs to make copies)
9. Provision of study product (Sayana Press units) Additional duties and responsibilities In conducting the field implementation, the Service Provider will:
abide by any required guidelines for human subjects research as determined by either FHI 360 or local, provincial or national governmental bodies; and
ensure professional and friendly behavior during interactions with study participants. FHI 360 reserves the right to modify the assessment strategy (and this SOW) at any time, based on results and experience. Expected Timeline
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9
Review
protocol/instruments
X
Obtain IRB approval X
Obtain RE, GCP and
medical certificates
for study staff
X
Conduct study staff
trainings
X
Recruit and Conduct
Enrollment
interviews
X X
Conduct Follow-up
interviews (3 visits
per participant)
X X X X
Conduct Final Visits X X X X X
Scan and email CRFs
weekly
X X X X X X
Enter data into
EpiData and email
X X X X
8
weekly
Conduct interviews
with providers
X
Conduct interviews
with self-injectors
X
Transcribe, translate
and transmit in-
depth interview data
X X X X
Review study
findings
X
Disseminate findings
in Malawi
X
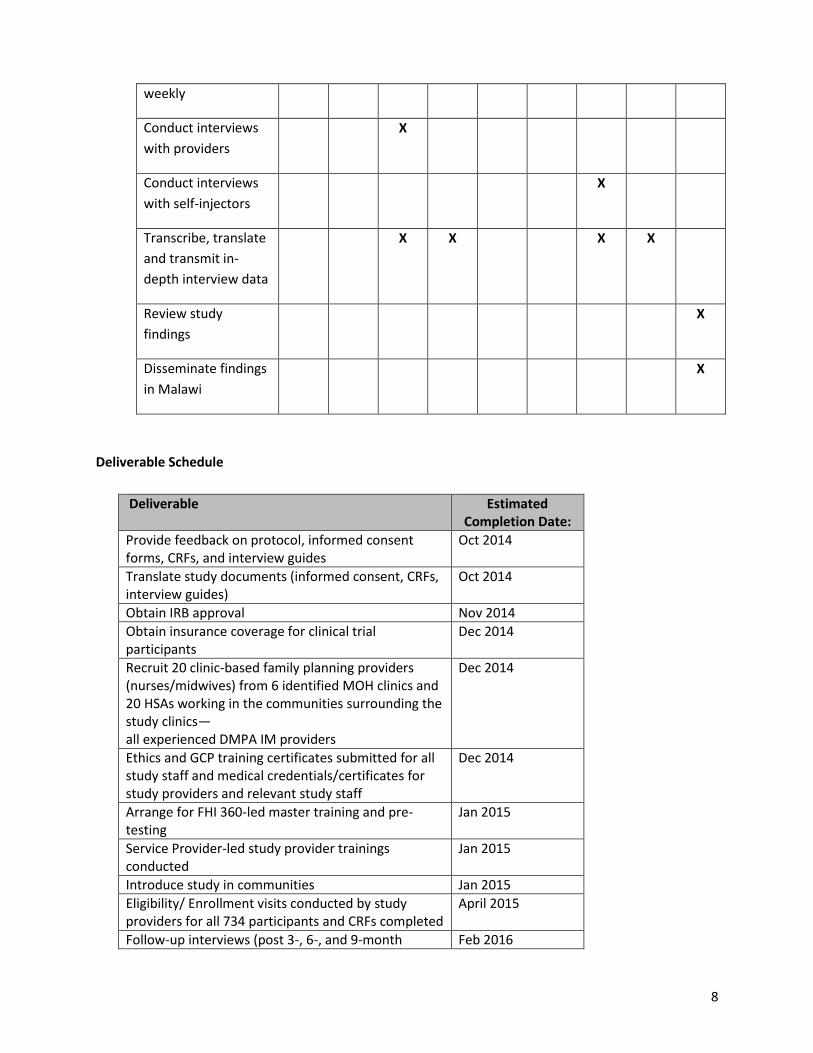
Deliverable Schedule
Deliverable Estimated Completion Date:
Provide feedback on protocol, informed consent forms, CRFs, and interview guides
Oct 2014
Translate study documents (informed consent, CRFs, interview guides)
Oct 2014
Obtain IRB approval Nov 2014
Obtain insurance coverage for clinical trial participants
Dec 2014
Recruit 20 clinic-based family planning providers (nurses/midwives) from 6 identified MOH clinics and 20 HSAs working in the communities surrounding the study clinics— all experienced DMPA IM providers
Dec 2014
Ethics and GCP training certificates submitted for all study staff and medical credentials/certificates for study providers and relevant study staff
Dec 2014
Arrange for FHI 360-led master training and pre-testing
Jan 2015
Service Provider-led study provider trainings conducted
Jan 2015
Introduce study in communities Jan 2015
Eligibility/ Enrollment visits conducted by study providers for all 734 participants and CRFs completed
April 2015
Follow-up interviews (post 3-, 6-, and 9-month Feb 2016

9
injections) conducted by data collectors and CRFs completed
Final visits conducted by data collectors and CRFs completed
June 2016
Scanned CRFs sent weekly through secure transmission
Jan 2015 – June 2016
Double data entry of Follow-Up Interview Behavioral Forms into EpiData
April 2015 – Feb 2016
EpiData datasets sent to FHI 360 through secure transmission
April 2015 – Feb 2016
IDIs conducted with 12 study providers May 2015
Provider IDIs transcribed and translated May 2015
IDIs conducted with 30 self-injecting participants June 2016
Participant IDIs transcribed and translated July 2016
All IDI transcript sent to FHI 360 through secure transmission
July 2016
Hold 1-day dissemination meeting November 2016
Review presentations and reports of study findings prepared by FHI 360
November 2016
Final Report on data collection experience submitted November 2016
Duration and Location
The work is expected to span 26 months, beginning in the fall of 2014. The anticipated study duration is
18 months. The training and study will be conducted in Mangochi, Malawi.
Qualifications and Experience
The Study Coordinator must have the following qualifications and experience:
Speak and write fluent English
10+ years of experience coordinating large-scale research projects for international clients
Demonstrated experience following specific research protocols
Post-graduate education
Available to work on the study full-time for the entire duration
The Field Medical Monitor must have the following qualifications and experience:
Speak English and a local language if necessary in the study district
A current license to practice medicine as a nurse/midwife or MD in the study district
Must be physically present in study district to be able to respond to SAEs
Experience in providing family planning, including DMPA to clients
Experience teaching other providers about family planning methods
Have demonstrated experience following specific research protocols
The Data Collectors must have the following qualifications and experience:

10
Speak English and a local language if necessary in the study district
Have experience collecting quantitative survey data and conducting qualitative in-depth interviews (Service Provider may propose separate individuals for the quantitative and qualitative data collection activities)
Have demonstrated experience following specific research protocols
University-level education
SUBMISSION REQUIREMENTS
To be considered, bidders must provide the following:
1. Description of methodology and proposed approach for the research as described in the Scope of Work section above (max 3 pages). Agencies should demonstrate:
a. solid experience in conducting public health studies, including GCP randomized clinical trials. b. the ability to submit and obtain ethics approval for similar research. c. the ability to reach and connect with ethics committees, regulatory agencies, and
government officials (to obtain necessary authorizations for data collection). Agencies must also provide a description of location(s) of presence relevant to this RFP. Agencies with research experience in identified regions are preferred.
2. Company profile with solid background/knowledge in public health, particularly family planning in
Malawi (and/or other neighboring countries).
3. CV or resumes for key personnel 4. Budget, including proposed labor costs, expenses, and other direct costs. All quotes should be in
local currency with the appropriate conversion to USD outlined.
To the extent that indirect costs are applicable, they are subject to the following limits:
0% for government agencies, other private foundations and for-profit organizations
up to 10% for U.S. universities and other academic institutions
Up to 15% for all other non-U.S. academic institutions and all private voluntary and non-government organizations, regardless of location.
Indirect cost rates (and the limitations) apply both to the primary applicant organization and any sub-grantees and/or sub-contractors that are part of the proposal.
5. Three references, including contact information for each. The references should be for past
customers for whom similar work was done.
6. An email address where we may send a confirmation of receipt of your submission.
7. If available, include a financial statement audit of the organization’s most recent fiscal year, conducted by a third-party accounting firm.
CRITERIA FOR EVALUATION

11
Bids will be evaluated and ranked by a committee on a best-value basis according to the criteria
below. Only offers’ able to provide all of requirements listed above will be considered.
Selection shall be based on the following weighted categories: 1. Methodology and Proposed Approach for the Research: 30% 2. Capacity and Experience: 20% 3. Completeness and Appropriateness of the Budget: 30% 4. References: 20%
NOTE: FHI 360 will not compensate the company for its preparation of response to this RFP nor is the
issuing of this RFP a guarantee that FHI 360 will award a contract.
Instructions and Deadline
Responses to this RFP should be submitted by email to Dr. Holly Burke ([email protected]) and Ms.
Jennifer Headley ([email protected]) no later than September 25th. Please follow the instructions
carefully. Proposals which do not follow these instructions will not be reviewed. Offers received after
this date and time will not be accepted for consideration. FHI 360 will acknowledge receipt of your
proposal by email. Proposals must be submitted in electronic format using Microsoft Office compatible
software.
FHI 360 will accept questions from interested parties through the date specified on page 1 via email at
[email protected] and [email protected].
Withdrawal of Proposals
Proposals may be withdrawn by written notice or email received at any time before award.
False Statements in Offer
Offers’ must provide full, accurate and complete information as required by this solicitation and its
attachments.
Proposals become property of FHI 360.
DISCLAIMERS AND FHI 360 PROTECTION CLAUSES
FHI 360 may cancel the solicitation and not make an award
FHI 360 may reject any or all responses received
Issuance of a solicitation does not constitute an award commitment by FHI Solutions
FHI 360 reserves the right to disqualify any offer based on offer or failure to follow solicitation instructions
FHI 360 will not compensate offers for response to solicitation

12
FHI 360 reserves the right to issue an award based on initial evaluation of offers without further discussion
FHI 360 may choose to award only part of the activities in the solicitation, or issue multiple awards based on the solicitation activities
FHI 360 may request from short-listed offerors a second or third round of either oral presentation or written response to a more specific and detailed scope of work that is based on a general scope of work in the original RFP.
FHI 360 has the right to rescind an RFP, or rescind an award prior to the signing of a subcontract due to any unforeseen changes in the direction of FHI 360’s client, be it funding or programmatic.
FHI 360 reserves the right to waive minor proposal deficiencies that can be corrected prior to award determination to promote competition
FHI 360 will be contacting offerors to confirm contact person, address and that bid was submitted for this solicitation.
REFERENCES 1. Burke HM, Mueller MP, Packer C, Perry B, Bufumbo L, et al. (2014) Provider acceptability of Sayana(R)
Press: results from community health workers and clinic-based providers in Uganda and Senegal. Contraception 89: 368-373.
2. Burke HM, Mueller MP, Perry B, Packer C, Bufumbo L, et al. (2014) Observational study of the acceptability of Sayana(R) Press among intramuscular DMPA users in Uganda and Senegal. Contraception 89: 361-367.
3. National Statistical Office, (NSO), and ICF Macro (2011) Malawi Demographic and Health Survey 2010. Zomba, Malawi, and Calverton, Maryland, USA: NSO and ICF Macro.
4. National Statistical Office, (NSO), and ICF Macro (1994) Malawi Demographic and Health Survey 1992. Zomba, Malawi, and Calverton, Maryland, USA: NSO and ICF Macro.
5. Beasley A, White KO, Cremers S, Westhoff C (2014) Randomized clinical trial of self versus clinical administration of subcutaneous depot medroxyprogesterone acetate. Contraception 89: 352-356.
6. Cameron ST, Glasier A, Johnstone A (2012) Pilot study of home self-administration of subcutaneous depo-medroxyprogesterone acetate for contraception. Contraception 85: 458-464.
7. Prabhakaran S, Sweet A (2012) Self-administration of subcutaneous depot medroxyprogesterone acetate for contraception: feasibility and acceptability. Contraception 85: 453-457.
8. National Statistical Office, (NSO), and ICF Macro (2005) Malawi Demographic and Health Survey 2004. Zomba, Malawi, and Calverton, Maryland, USA: NSO and ICF Macro.





























