Embed Size (px)
Citation preview

Epitrochlear lymph nodes: Anatomical basis, clinicalaspects, sonography findings, and cross-sectional imagingcorrelation
Poster No.: C-2431
Congress: ECR 2010
Type: Educational Exhibit
Topic: Musculoskeletal - Miscellaneous
Authors: O. Catalano, A. Nunziata, F. Laghi, A. Siani; Naples/IT
Keywords: Epitroclear lymph nodes, Ultrasound, Colour-Doppler ultrasound
Keywords: Musculoskeletal system
DOI: 10.1594/ecr2010/C-2431
Any information contained in this pdf file is automatically generated from digital materialsubmitted to EPOS by third parties in the form of scientific presentations. Referencesto any names, marks, products, or services of third parties or hypertext links to third-party sites or information are provided solely as a convenience to you and do not inany way constitute or imply ECR's endorsement, sponsorship or recommendation of thethird party, information, product or service. ECR is not responsible for the content ofthese pages and does not make any representations regarding the content or accuracyof material in this file.As per copyright regulations, any unauthorised use of the material or parts thereof aswell as commercial reproduction or multiple distribution by any traditional or electronicallybased reproduction/publication method ist strictly prohibited.You agree to defend, indemnify, and hold ECR harmless from and against any and allclaims, damages, costs, and expenses, including attorneys' fees, arising from or relatedto your use of these pages.Please note: Links to movies, ppt slideshows and any other multimedia files are notavailable in the pdf version of presentations.www.myESR.org
Page 1 of 20

Learning objectives
The objective of this exhibit is to illustrate, through a wide spectrum of drawings andillustrations, the normal and abnormal US and colour-Doppler findings encountered whenimaging the lymph nodes of the epitrochlear region.
Page 2 of 20

Background
The normal and abnormal aspects of the epitrochlear lymphatic station are not much wellknown by the radiologists. The axillary lymph node basin is commonly regarded as theprimary lymphatic target of upper limb disorders but this is not always true.
In this exhibit we illustrate, through a number of drawings and illustrations, the normal andabnormal sonography (US) and colour-Doppler US findings encountered when imagingthe lymph nodes of the epitrochlear region.
Page 4 of 20

Imaging findings OR Procedure details
Normal Findings
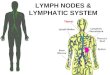
The epitrochlear lymph nodes (called also sovraepitrochlear or cubital lymph nodes)are part of the upper extremity lymphatic system. These lymph nodes range in numberbetween 1 and 3 (very rarely 4) and are located within the subcutaneous layer, along themedial aspect of the elbow, 4 to 5 cm proximal to the epitrochlear (Drawing 1 on page
). The epitrochlear collect the fluid from the last two or three fingers and from themedial aspect of the hand.
Nevertheless, it should be remembered that there is a relevant interindividual variationamong the drainage area. Consequently any disorder of the elbow, forearm, wrist, orhand could involve the epitrochlear lymph nodes and the radiologist must explore thisstation aside from the medial or lateral location of the primary disease.
The lymphatics originating from the epitrochlear lymph nodes reach the axillary station.In some instance both stations are jointly involved by inflammatory or tumour processes.
Fig.: Drawing 1References: Antonio Nunziata, [email protected]
Clinical Findings
The data from patient history and physical examination include: location, extension,colour of the overlying skin, size, consistence, pain, mobility, adhesion between thevarious nodes, and presence of other abnormalities in other body districts. This
Page 6 of 20

information is important prior to an US exploration and should be merged with the USand colour-Doppler findings to achieve a definitive diagnosis.
Imaging Findings
The morphologic, echostructural, and vascular findings are the same of all superficiallymphadenopaties. The most relevant aspects include: number, size and shape of thelymph nodes, border and appearance of the fat around the lymph node, measure andratio of the longitudinal and transverse diameter, appearance of the echoic hilum (large,reduced, displaced, inhomogeneous, and disappeared), thickness and texture of thecortex, angioarchitecture (hilar or capsular, normal or increased, etc.) (Drawing 2 on page
).
Fig.: Drawing 2References: Antonio Nunziata, [email protected]
We show a number of cases, including lymphadenitis of the IV drug abuser (Fig.1 onpage 9), cat-scratch disease (Fig.2 on page 9); Hodgkin disease (Fig.3 on page10); metastasis from upper limb cutaneous melanoma (Fig.4 on page 11), (Fig.5on page 12).
Page 7 of 20

In subjects with lymphomas, elbow lymphadenopaties can be the presentation site of thehaematological malignancy. In some case this is a solitary localization while in other thesubsequent work-up allows the detection of other superficial and deep lesions.
In melanoma patients the axillary lymph nodes are regarded as the regional basin of theupper limb. The epitrochlear lymph nodes (as well as the popliteal lymph nodes for thelower limb) are considered as "interval" lymph nodes, along the route from the primaryskin tumour and the axilla. Cutaneous melanoma is known to spread mostly along thelymphatic ducts, with the development of so-called in-transit metastasis and, as we saidbefore, of interval lymphadenopaties. Intriguingly, in one of our cases the patient hadalready undergone radical axillary lymphadenectomy from a shoulder melanoma andsubsequently developed an epitrochlear lymphadenectomy with an unusual descendingpath of the tumour cells.
Clearly, a differential diagnosis is needed with the other possible causes of epitrochlearand elbow swelling (Table 1 on page ).
Fig.: Table 1References: Dept of Radiology, National Cancer Institute, Naples, Italy
Page 8 of 20

Images for this section:
Fig. 0: Acute lymphadenitis in a subject with history of IV drug abuse. Palpable, painfulswelling. Single inflammatory lymphadenomegaly.
© Dept of Radiology, National Cancer Institute
Page 9 of 20

Fig. 0: Acute lymphadenitis in a veterinary (cat-scratch disease, subsequently provenat serology). Palpable, painful swelling. Single inflammatory lymphadenomegaly withintense hyperaemia.
© Dept of Radiology, National Cancer Institute
Page 10 of 20

Fig. 0: Hodgkin disease presenting as palpable epitrochlear mass. Multiplelymphadenopaties. Consequently, a brachial vein thrombosis is apparent.
© Dept of Radiology, National Cancer Institute
Page 11 of 20

Fig. 0: Single, partial, lymph node metastasis in a patient having undergone excision ofa cutaneous melanoma of the wrist one year before. Palpable, painless mass found bythe patient herself.
© Dept of Radiology, National Cancer Institute
Page 12 of 20

Fig. 0: Single lymph node metastasis in a patient with previous excision of shouldermelanoma and previous axillary lymphadenectomy. Probably this explains the unusuallymphatic spread to the elbow. US demonstrated the lymph node metastasis after thePET-CT detection o fan occult elbow lesion.
© Dept of Radiology, National Cancer Institute
Page 13 of 20

Conclusion
In conclusion, epitrochlear lymphadenopaties are uncommon but possible. Consequentlythis occurrence requires an adequate knowledge of the key points for recognition anddifferential diagnosis.
Page 14 of 20

Images for this section:
Fig. 0
© Ecr.org
Page 15 of 20

Personal Information
Orlando Catalano, MD, Dept of Radiology, National Cancer Institute "G.Pascale",Naples, Italy. [email protected]
Antonio Nunziata, MD, Dept of Radiology, P. "S.Bellone", DSB 30, ASL Napoli 1 Centro,Naples, Italy. [email protected]
Francesca Laghi, MD, Dept of Radiology, Second University, Naples, Italy.
Alfredo Siani, MD, Dept of Radiology, National Cancer Institute "G.Pascale", Naples,Italy.
Page 16 of 20

Images for this section:
Fig. 0
© Dept of Radiology, National Cancer Institute "G.Pascale, Naples, Italy
Page 17 of 20

Fig. 0
© ASL Napoli 1 Centro, Naples, Italy
Page 18 of 20

References
1. Catalano O, Nunziata A, Siani A. Fundamental in oncologic ultrasound onpage 20. Sonographic Imaging and Intervention in the Cancer PatientSpringer Italia, Milan 2009.
2. Hunt JA, Thompson JF, Uren RF et al. Epitrochlear lymph nodes as a siteof melanoma metastasis. Ann Surg Oncol 1998;5:248-252.
3. McMasters KM, Chao C, Wong SL et al. Sunbelt Melanoma Trial Group.Interval sentinel lymph nodes in melanoma. Arch Surg 2002;137:543-547.
4. Uren RF, Howman-Giles RB, Thompson JF. Failure to detect drainage tothe popliteal and epitrochlear lymph nodes on cutaneous lymphoscintigraphyin melanoma patients. J Nucl Med 1998;39:2195.
5. Uren RF, Howman-Giles R, Thompson JF et al. Interval nodes:the forgotten sentinel nodes in patients with melanoma. Arch Surg2000;135:1168-1172.
Page 19 of 20

Images for this section:
Fig. 0
© Springer, Milan, Italy
Page 20 of 20