Embed Size (px)
Citation preview

Epilepsy Update: Recognition and Acute Management of Different
Types of Seizures
Patricio Sebastian Espinosa, MD, MPH, FAAN.
Chief of Neurology
Marcus Neuroscience Institute

Outline
• Epilepsy
• Seizures and Epilepsy
• Classification and New Terminology
• Status Epilepticus
• Autoimmune Epilepsy
• Seizures in the ICU
• Epilepsy surgery (if time permits)
• Case Presentation Dr. Chaudhary

Epilepsy Facts
• Epilepsy is one of the most common and disabling public health problems.
• ~ 3.5 million people have epilepsy in the US.
• 10% of the population will have a seizure at some time in their lives.
References Kobau R, Luo Y, PhD, Zack M, Helmers S, Thurman D. Epilepsy in adults and access to care — United States, 2012. MMWR. 2012;61(45);909-913. . Accessed October 10, 2014. pdf [863KB]. US Census Bureau, Population Division [database online]. Annual estimates of the resident population by sex, age, race, and Hispanic origin for the United States, States, and Counties: April 1, 2010, to July 1, 2013. Release Date: June 2014. html. Accessed February 2, 2015. Russ SA, Larson K, Halfon N. A national profile of childhood epilepsy and seizure disorder. Pediatrics 2012;129:256–64. DOI: 10.1542/peds.2010-1371.
Institute of Medicine. Epilepsy Across the Spectrum: Promoting Health and Understanding. Washington, DC: The National Academies Press, 2012.

Epilepsy and mortality
• Mortality rates are higher in people with epilepsy than the general population – SUDEP accounts for 15% of all deaths in epilepsy
• People with Drug Resistant Epilepsy (DRE) are at special risk for SUDEP – SUDEP accounts for 50% of all deaths in DRE
– SUDEP: Sudden unexplained death in epilepsy
Thruman DJ, et al. Epilepsia 2014; doi: 10.1111/epi.12666. Scorza FA, et al. Epilepsy Behav 2014;37:75.
4


Seizures and epilepsy are not the same.
– An epileptic seizure is a transient occurrence of signs and/or symptoms due to abnormal excessive or synchronous neuronal activity in the brain.
– Epilepsy is a disease characterized by an enduring predisposition to generate epileptic seizures and by the neurobiological, cognitive, psychological, and social consequences of this condition.
• Translation: a seizure is an event and epilepsy is the disease involving recurrent unprovoked seizures.

Epilepsy
• Epilepsy is a disorder of the brain characterized by:
– (1) At least two unprovoked seizures occurring >24 h apart;
– (2) one unprovoked seizure and a probability of further seizures similar to the general recurrence risk (at least 60%) after two unprovoked seizures, occurring over the next 10 years;
– (3) diagnosis of an epilepsy syndrome.
1: Fisher RS, Acevedo C, Arzimanoglou A, Bogacz A, Cross JH, Elger CE, Engel J Jr, Forsgren L, French JA, Glynn M, Hesdorffer DC, Lee BI, Mathern GW, Moshé
SL, Perucca E, Scheffer IE, Tomson T, Watanabe M, Wiebe S. ILAE official report: a practical clinical definition of epilepsy. Epilepsia. 2014 Apr;55(4):475-82. doi:
10.1111/epi.12550. Epub 2014 Apr 14. Review. PubMed PMID: 24730690.

Psychogenic nonepileptic seizures (PNES)
• PNES are diagnosed in 20 to 30% of patients seen at epilepsy centers for intractable seizures.
• In the general population the prevalence rate is 2-33 per 100, 000.
Lesser RP. Treatment and Outcome of Psychogenic Nonepileptic Seizures.Epilepsy Currents. 2003;3(6):198-200. doi:10.1046/j.1535-7597.2003.03601.x.

PNES in History
PNES = Conversion Conversion disorder. Conversion disorder is a mental health condition in which a person can have blindness, paralysis, involuntary movements, or other nervous system (neurologic) symptoms that cannot be explained by medical evaluation. Conversion disorder:
MedlinePlus Medical Encyclopedia United States National Library of Medicine


ILAE 2017: The New Basic Classification of Seizures
• The basic classification is a simple version of the major categories of seizures.
1. Where seizures begin in the brain 1. Focal Seizures 2. Generalized Seizures 3. Focal to Bilateral 4. Unknown onset
2. Level of awareness during a seizure 1. Focal Aware 2. Focal Impaired awareness 3. Awareness unknow
Fisher, R. S., Cross, J. H., D'Souza, C. , French, J. A., Haut, S. R., Higurashi, N. , Hirsch, E. , Jansen, F. E., Lagae, L. , Moshé, S. L., Peltola, J. , Roulet Perez, E. , Scheffer, I. E., Schulze‐Bonhage, A. , Somerville, E. , Sperling, M. , Yacubian, E. M. and Zuberi, S. M. (2017), Instruction manual for the ILAE 2017 operational classification of seizure types. Epilepsia, 58: 531-542. doi:10.1111/epi.13671

Hx of Focal Epilepsy
• John Hughlings Jackson first describe focal seizures.
• Jacksonian march or Jacksonian seizure is a phenomenon where a focal seizure spreads from the distal part of the limb toward the ipsilateral face

Frequency and Type
• Seizures can be divided in 2 main types:
- Focal Seizures - Generalized Seizures

Management of First Seizure
• Assessment of the patient with a first seizure is a common and important neurologic issue.
• Less than 50% of patients who have a first unprovoked seizure have a second seizure; thus, the evaluation should focus on determining the patient’s risk of seizure recurrence.

Risk of subsequent seizure over 10 years
Copyright © 2019 American Academy of Neurology
15
Risk of subsequent seizure over 10 years after acute symptomatic seizure during acute illness (eg, stroke, central nervous system infection, traumatic brain injury) compared with risk of subsequent seizure in patients with remote symptomatic unprovoked seizure (ie, previous stroke, central nervous system infection, traumatic brain injury).Reprinted with permission from Hesdorffer DC, et al, Epilepsia.18onlinelibrary.wiley.com/doi/10.1111/j.1528-1167.2008.01945.x/full. © 2009 International League Against Epilepsy.

Risk of Recurrence with # of seizures at presentation.
Copyright © 2019 American Academy of Neurology
16
Data showing no difference in cumulative chance of seizure recurrence whether patients presented with a single seizure (n = 425) or multiple seizures (n = 72).Reprinted with permission from Kho LK, et al, Neurology.7www.neurology.org/content/67/6/1047. © 2006 American Academy of Neurology.

Management of First Seizure
• Provoked or acute symptomatic seizures do not confer increased risk for subsequent unprovoked seizure recurrence.
• Multiple seizures in a given 24-hour period do not increase the risk of seizure recurrence.

Management of First Seizure
• Remote symptomatic seizures, an epileptiform EEG, a significant brain imaging abnormality, and nocturnal seizures are risk factors for seizure recurrence.
• Antiepileptic drug therapy delays the time to second seizure but may not influence long-term remission.

Treatment goals for epilepsy
Treatment Goals
• No seizures
• No side effects
Kwan P, et al. Epilepsia 2009; doi: 10.1111/j.1528-1167.2009.02397.x Gilliam F. Neurology 2002;58:s9-s19. Faught E, et al. Epilepsia 2009;50(3):501-509.
Newly Diagnosed Epilepsy
Treatment Goals
• Optimize long-term seizure control
• Maximize quality of life
• Minimize side effects
• Maximize adherence
• Decrease seizure severity/postictal period
Drug-Resistant Epilepsy
19
VNSOV15-11-1000-WW

Epilepsy and drug-resistant epilepsy ILAE Consensus Statement
• The failure of two appropriately chosen and tolerated AEDs (whether as monotherapies or in combination) to control seizures when used for an adequate period of time1
1. Kwan P, et al. Epilepsia 2010;51:1069-77. 2. Mohanraj R and Brodie MJ. Eur J Neurol. 2006;13:277-282.
50%
11%4%
35%
Response with First Drug
Response with Second Drug
Response with Third Drug or
Multiple Drugs
Drug-Resistant Population
After adequate trials of at least 2 AEDs, overall response rates with subsequent treatment trials are dramatically decreased2
20

Treatment Outcomes in Patients With Newly Diagnosed Epilepsy Treated With Established and New Antiepileptic Drugs
A 30-Year Longitudinal Cohort Study
• Has the overall prognosis of epilepsy improved after the introduction of more than a dozen new antiepileptic drugs in the past 2 decades?
• NO
1: Chen Z, Brodie MJ, Liew D, Kwan P. Treatment Outcomes in Patients With Newly Diagnosed Epilepsy Treated With Established and New Antiepileptic Drugs: A 30-Year Longitudinal Cohort Study. JAMA Neurol. 2018 Mar 1;75(3):279-28

22
Comprehensive Epilepsy Evaluation
Neurostimulation • Vagus Nerve Stimulation
• Responsive Neurostimulation System
(RNS) • Deep brain • stimulation
Diet
• Ketogenic • Modified Atkins • Low glycemic
index
Clinical Trials • New AEDs • New Devices
Brain Surgery
• Resective surgery – Temporal
Lobectomy
– Corpus Callosotomy
– Hemispherectomy
– Multiple Subpial Transsections
• MR Laser Ablation
VNSOV15-11-1000-WW
Epilepsy Team

Autoimmune Epilepsy
“Epilepsy with evidence of autoimmune mediated CNS inflammation.”

History - Hashimoto encephalopathy
• Almost 50 years ago, the report of a syndrome of encephalopathy, seizures, and stroke like episodes associated with Hashimoto thyroiditis marked the first description of a possible link between the central nervous system (CNS) and an autoimmune process.
• Initially called Hashimoto encephalopathy and more recently referred to as steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT), is now known to be one of the many situations where seizures might complicate a systemic autoimmune disorder.
Brain L, Jellinek EH, Ball K. Hashimoto’s disease and encephalopathy. Lancet 1966; 2(7462): 512–514.

Examples of Autoimmune Epilepsy
• Paraneoplastic limbic encephalitis associated with onconeural antibodies
• Limbic encephalitis associated with antibodies against the voltage-gated potassium channel complex
• Encephalitis associated with n-methyl-d-aspartate receptor antibodies
• Encephalitis associated with antibodies against other neuronal surface antigens
• Limbic encephalitis associated with glutamic acid decarboxylase 65 antibodies
• Rasmussen encephalitis
• Syndromes of de novo febrile illness–related refractory seizures and status epilepticus
• Seizures in patients with other autoimmune and inflammatory disorders of the central nervous system
• Seizures and epilepsy in patients with systemic autoimmune disorders
• Antibodies in patients with isolated chronic epilepsy

Paraneoplastic Limbic Encephalitis Associated with Onconeural Antibodies
• Limbic encephalitis is characterized by cognitive, especially memory, impairment; behavioral changes; temporal lobe seizures; and sleep disturbance.
• Seizures can be dyscognitive or secondary generalized, and status epilepticus may occur.

Paraneoplastic, Autoantibody Evaluation, Serum

E – Protocol for Autoimmune Epilepsy
• Upon the suspicion of clinical suspicion of autoimmune epilepsy.
– History
– EEG
– Brain Imaging
• IV Steroids and +/- IVIG
• Thyroid antibodies and paraneoplastic panel in Serum/CSF

Epilepsy Emergencies
Status epilepticus is a neurologic emergency with a time-dependent impact on morbidity and mortality.

Why is important to tx?

Status Epilepticus: Time is brain
• Generalized convulsive status epilepticus is easily diagnosed as patients initially have generalized convulsions without return to neurologic baseline.
• Nonconvulsive status epilepticus, which may have no clinical manifestations and is only detectable through video-EEG monitoring, is also increasingly being recognized.
• Prognosis is dependent on the underlying etiology and time spent in status epilepticus.

Status Epilepticus - 5min.
• Generalized convulsive and nonconvulsive status epilepticus (SE) are neurologic and medical emergencies defined as 5 or more minutes of either continuous seizure activity or repetitive seizures with no intervening recovery of consciousness.
• Traditionally SE was defined as 30 or more minutes; however, this time frame has been reduced to 5 minutes to emphasize the seriousness of the condition and the need to treat it urgently.

DEFINITION OF STATUS EPILEPTICUS
• Refractory status epilepticus is defined as seizures that continue despite first- and second-line treatments.
• Super-refractory status epilepticus occurs when third-line agents (IV anesthetics) fail

EPIDEMIOLOGY
• The incidence of status epilepticus reportedly ranges from 10 per 100,000 to 40 per 100,000 in various databases.
• A peak incidence occurs at younger than 10 years of age (14.3 per 100,000) and at older than 50 years of age (28.4 per 100,000)
• Highest mortality in the elderly population.

DIAGNOSIS
• The diagnosis of generalized convulsive status epilepticus is fairly straightforward and based on clinical seizure activity.
• Generalized convulsive status epilepticus should be treated without delay.
• Once some type of treatment has been initiated and the intense motor convulsions are controlled, the etiology of the status epilepticus should immediately be sought.
• The most common etiologies include seizure breakthroughs in the context of a known chronic epilepsy, acute structural lesions, or acute metabolic derangements.

Causes of Status Epilepticus
1. Abrupt discontinuation of antiepileptic drugs in patient with epilepsy
2. CNS infections 3. Brain tumors or other mass lesions 4. Stroke (ischemic/hemorrhagic) 5. Traumatic head injury 6. CNS toxicity: certain medications, drugs, ethanol 7. Metabolic disturbances: hypoglycemia,
hyponatremia 8. Cryptogenic

EEG and MRI en la UCI


Work up for SE
Initial Assessment: • ABCs • ICU admission • Emergent electroencephalogram (EEG) • Continuous video EEG in refractory cases • Laboratory Tests
– Routine blood workup (CBC, CMP, glucose, electrolytes) – Urine drug screen – Lumbar puncture and CSF analysis in patients with suspected
meningitis
• Imaging Studies – Immediate CT scan of the head – MRI of the brain should be performed once the patient is in a stable
condition.

Table 9-1 General Do...
Table 9-1 General Dosing Recommendations for the Most Common First-, Second-, and Third-Line Medications Used in the Treatment of Status Epilepticus
Copyright © 2016 American Academy of Neurology . Published by Lippincott Williams & Wilkins. 40
Epilepsy Emergencies
Hantus, Stephen
CONTINUUM: Lifelong Learning in Neurology. 22(1, Epilepsy):173-190, February 2016.
doi: 10.1212/CON.0000000000000285

TREATMENT
• The treatment of status epilepticus should aim to achieve seizure control as promptly and as safely as possible.

TREATMENT: Standard Status
Epilepticus Treatment Protocol • The initial treatment protocol of status epilepticus has been
established by the US Department of Veterans Affairs (VA) Cooperative Study randomized controlled clinical trial in which IV lorazepam 0.1 mg/kg given at a rate of 2 mg/min was superior as compared to IV phenytoin as the first-line therapy in aborting status epilepticus.
• In the VA Cooperative Study, 64.9% of status epilepticus events were first aborted with IV lorazepam as opposed to 43.5% with IV phenytoin, establishing the superiority of IV lorazepam as first-line therapy.
• Beyond this Class I evidence favoring IV lorazepam, treatment recommendations have been essentially based on anecdotal evidence and small case series

Why levetiracetam as a first choice for seizures and status epilepticus?
• Levetiracetam has similar effectiveness in status epilepticus and epilepsy
• No hypotension
• No interactions
• Very low incidence of allergic reactions
• Non Sedative

E- Protocol
1. Ativan 2- 4 mg
2. Levetiracetam 1500 mg IV Stat
3. Lacosamide 200 mg IV Stat
4. Depacon 1000 mg IV
Highly effective non sedating treatment of status epilepticus (HENTSTAT)

ICU Monitoring

Video EEG in the ICU
Critically ill patients are at high
risk for a variety of neurologic
insults, including seizures,
ischemia, edema, infection, and
increased intracranial pressure,
which can result in permanent
neurologic disability if
untreated.

The Magnitude of the Problem
• In the ICU Seizures and Status epilepticus are
common findings and are associated with acute injury to the nervous system.
• Up to 34% of patients in coma are in non-convulsive status epilepticus.
Claaseen,Hirsh et al. NEUROLOGY 2004;62:1743-1748

EEG en la ICU
• Why is important to diagnosed seizures:
– High metabolic demand of the epileptogenic areas can cause more damage to the injured brain tissue
– NCSE has been associated with increased edema in patient with strokes.
Privitera M, Hoffman M, Moore JL, Jester D. EEG detection of nontonic-clonic status epilepticus in patients with altered consciousness. Epilepsy Res. 1994; 18: 155–166

CT
• 66 year old woman
• Acute stroke
• Hx of Epilepsy
• Becomes very lethargic

EEG

UCI Video EEG

UCI Video EEG

How long should we monitor:
Time needed to diagnosed a seizure
Hirsch LJ, J Clin Neurophysiol. 2004;21:332-340

Table 1
TABLE 1 Common Neurological, Medical, and Surgical Conditions Associated With High Likelihood of Recording Seizures on Critical Care Continuous EEG
Copyright © 2015 Journal of Clinical Neurophysiology. Published by Lippincott Williams & Wilkins. 54
Consensus Statement on Continuous EEG in Critically Ill Adults and Children, Part I: Indications Herman, Susan T.; Abend, Nicholas S.; Bleck, Thomas P.; Chapman, Kevin E.; Drislane, Frank W.; Emerson, Ronald G.; Gerard, Elizabeth E.; Hahn, Cecil D.; Husain, Aatif M.; Kaplan, Peter W.; LaRoche, Suzette M.; Nuwer, Marc R.; Quigg, Mark; Riviello, James J.; Schmitt, Sarah E.; Simmons, Liberty A.; Tsuchida, Tammy N.; Hirsch, Lawrence J. Journal of Clinical Neurophysiology. 32(2):87-95, April 2015. doi: 10.1097/WNP.0000000000000166

Among comatose patients in the
ICU, rates of nonconvulsive status epilepticus have been reported to
vary from 8% to 37% on cEEG monitoring.

END

Continuous EEG Monitoring
1. Epilepsy monitoring unit (EMU)
– Invasive Continuous EEG monitoring
2. Continuous EEG monitoring in the ICU
3. Ambulatory EEG with and with out video

Video EEG monitoing
• Video-EEG monitoring as an inpatient procedure has long been used for diagnostic purposes for patients with spells of uncertain etiology, for localization of seizure onset, or for classification purposes in patients with known epilepsy.
• Epilepsy monitoring unit (EMU) evaluation can be very helpful in distinguishing psychogenic nonepileptic seizures (PNES) and nonepileptic paroxysmal events from epileptic seizures.
• Studies show that among EMU admissions, about 25% of patients have PNES, whereas between 9% and 15% of patients have both epileptic seizures and PNES.

Video EEG

EEG

MRN Pre and Post

The evidende of epilepsy surgery

The Evidence for Surgery in Epilepsy - Temporary Lobe
• Randomized study of 80 patients
• 40 medical treatment and 40 surgery
• In the surgical group at one year 58% free of seizures (P <0.001)
• In the medical group at one year free 8% of seizures (P <0.001)
• Patients in the surgical group had fewer seizures and improved quality of life (P <0.001) than patients in the medical group
Wiebe S, et al. Effectiveness and Efficiency of Surgery for Temporal Lobe Epilepsy Study Group. A randomized, controlled trial of surgery for temporal-lobe epilepsy. N Engl J Med. 2001 Aug 2;345(5):311-8.

A RANDOMIZED, CONTROLLED TRIAL OF SURGERY FOR TEMPORAL-LOBE EPILEPSY
0%
10%
20%
30%
40%
50%
60%
70%
Surgical Group Medical Group
Patients with Epilepsy
Sz Free
58%
8%
1: Wiebe S, Blume WT, Girvin JP, Eliasziw M; Effectiveness and Efficiency of Surgery for Temporal Lobe Epilepsy Study Group. A randomized,
controlled trial of surgery for temporal-lobe epilepsy. N Engl J Med. 2001 Aug 2;345(5):311-8. PubMed PMID: 11484687.

Surgical Evaluation
Phase I Investigation
Phase II Intracranial
Fase III Surgery

Phases of Surgical Evaluation
• Phase I (non invasive) Initial evaluation – Video EEG
– MRI, PET, SPECT, MEG, fMRI
– Psychological, Psychiatric, Social Evaluation
• Phase II Presurgical (invasive) – Subdural Electrodes and or intra parenchymal
– Cortical Mapping
• Phase III Surgical – Resection
– Cortical mapping and corticography during surgery

Case 1
• 27 yo woman
• 8 complex partial seizures per month
• On Keppra 1500 mg BID
• Has tried over 10 drugs

Fase I: EEG: Ondas Epileptiformes Temporal derecha

EEG: Convulsión de Origen Temporal derecha

MRI Brain Epilepsy Protocol

RMN

PET: Hipometabolismo temporal derecho

WADA Inyección Izquierda

WADA Inyección Derecha

Phase I: Other studies
• MRI MTS
• Evaluation psychological
– Memory located in the left temporal
• Spect Inter ictus – Area de hipometabolismo derecho
• Test de Wada
– Left hemisphere was dominant for lenaguage
– 7/8 - Injection right
– 1/8 - Injection left

Surgical Evaluation
Phase I Investigación
Phase II Intracranial
Fase III Surgery

Phase II: Corticography – Subdural Electrods
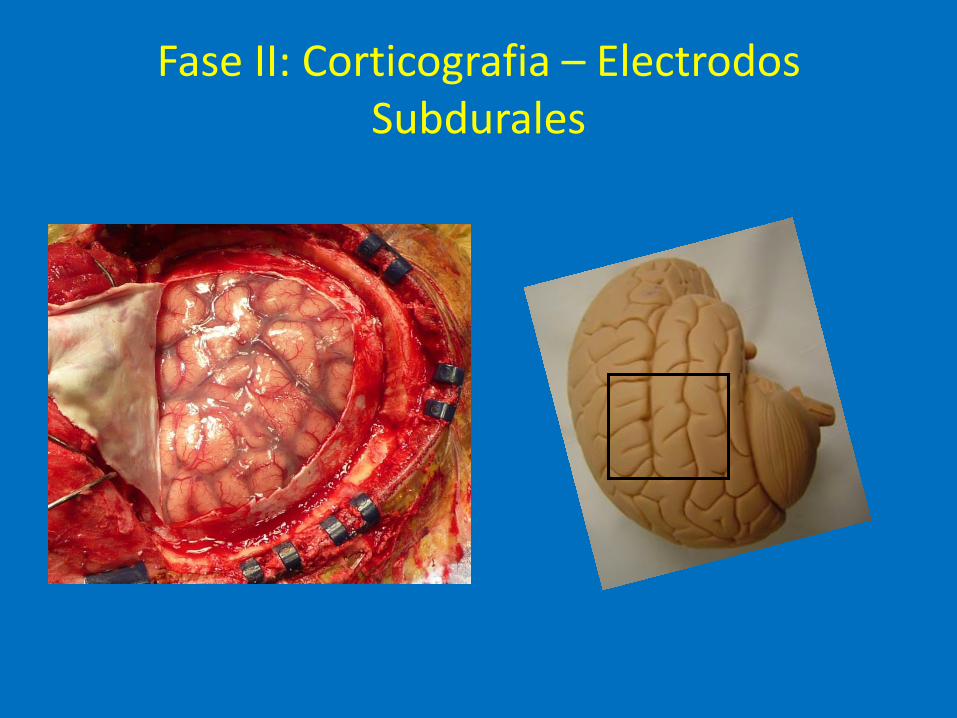
Fase II: Corticografia – Electrodos Subdurales

Phase II: Corticography – Subdural Electrods

Localization of the electrodes

Electrode Localization
Courthesy: Jong W Lee, MD, PhD. BWH – Harvard Medical School

Fase II: Corticografia

Fase II: Corticografia Espiga/Punta Mesial Temporal Derecha

Evaluación Quirúrgica
Phase I Investigation
Phase II Intracranial
Phase III Cirugía

Surgery for temporal-lobe epilepsy
Wiebe S, Blume WT, Girvin JP, Eliasziw M; Effectiveness and Efficiency of Surgery for Temporal Lobe Epilepsy Study Group. A randomized, controlled trial of surgery for temporal-lobe epilepsy. N Engl J Med. 2001 Aug 2;345(5):311-8.

Phase III: Temporal Lobectomy
Courtesy: Madsen MD, BWH, HMS

Fase III: Lobectomia temporal

Epilepsia Team

Other Surgical options

VNS Therapy US indication for use Indicated for use as an adjunctive therapy in reducing the frequency of seizures
– In adults and adolescents over 12 years of age
– With partial onset seizures that are refractory to antiepileptic medications
Contraindications – Contraindicated in patients with
a left vagotomy – Diathermy (shortwave,
microwave, ultrasound) should not be used after VNS Therapy implant
VNS Therapy Physician’s Manual. Houston, TX: Cyberonics, Inc.
90
VNSOV15-11-1000-WW

Neuropace
• Are 18 years or older • Have a diagnosis of partial-onset
seizures with 1 or 2 well-localized seizure foci identified
• Have an average of 3 or more disabling seizures per month over the prior 3 months.
• Are refractory to medical therapy (have failed 2 or more appropriate antiepileptic medications at therapeutic doses)
• Are not candidates for focal resection epilepsy surgery (e.g., have an epileptic focus near eloquent cerebral cortex; have bilateral temporal epilepsy)

Deep-brain thalamic stimulation.
• Deep-brain stimulation of the anterior nucleus of the thalamus resulted in a median 40.5% reduction in seizures compared with a 14.5% reduction in the nonstimulated group in a randomized, placebo-controlled, multicenter study.[2]

MRI pt with Status Epilepticus

Video EEG patient with SE

Patient with Myoclonic Jerks after CPR

• Adults with an unprovoked first seizure should be informed that their seizure recurrence risk is greatest early within the first 2 years (21%–45%) (Level A)
• The clinical variables associated with increased risk may include a prior brain insult (Level A), an EEG with epileptiform abnormalities (Level A), a significant brain-imaging abnormality (Level B), and a nocturnal seizure (Level B).
Neurology April 21, 2015 vol. 84 no. 16 1705-1713









Seizures
• Approximately 30–75% of patients with brain tumors present with seizures as the initial symptom.2, 3
• Seizures play a very important role in the quality of life, particularly in patients with slow-growing primary brain tumors, for whom seizure incidence reaches 80–90%.2, 4
• These seizures often manifest as focal seizures with secondary generalization and are often refractory to antiepileptic treatment.

Seizure Mechanisms
• Tumor factors
• Histology
• Tumor location
• Blood–brain barrier disruption
• Gap junctions
• Molecular genetic changes
• Peri-tumor
• Morphologic changes
• Hypoxia, acidosis and metabolic changes
• Ionic changes
• Changes in amino acids and neurotransmitter receptors
• Glutamate neurotransmission
• GABA neurotransmission
• Immunological and inflammatory changes

Treatment for tumor-related epilepsy
• Seizures caused by brain tumors often manifest as focal seizures with or without secondary generalization, and approximately one third of patients are refractory to antiepileptic medication treatment. 9
• Currently, the management of epilepsy in patients with a brain tumor mainly relies on antiepileptic drug therapy. – Antiepileptic drugs can be divided into two groups: first
generation drugs (e.g. phenytoin, carbamazepine, valproic acid, ethosuximide, benzodiazepines and barbiturates) and second generation drugs (e.g. levetiracetam, felbamate, gabapentin, lamotrigine, pregabalin, tiagabin, zonisamide, oxcarbazepine and topiramate).

Patient with aphasia

EEG

EL EEG continua…

EEG: Methods of Activation
• Photic stimulation is a useful method of activating epileptiform discharges primarily in patients with idiopathic generalized epilepsy, but also those with partial epilepsy.
• Hyperventilation is another procedure that can activate epileptiform abnormalities. Typically, absence seizures are activated with hyperventilation, although epileptiform discharges in focal epilepsies may be activated as well.
• Sleep Deprivation is an important tool when EEGs are unyielding in providing diagnostic information. In a review of all earlier studies, Ellingson and colleagues concluded that sleep deprivation increases the chances of finding interictal epileptiform discharges on an EEG in 30% to 70% of cases. Similarly, Fountain and colleagues reported an activation rate of 52% with sleep deprivation when baseline EEGs are normal. Furthermore, activation by sleep deprivation is more common in younger patients and those with primary generalized epilepsy syndromes.

Sources of Error in EEG interpretation
• Sources of error may come when EEGs are normal in patients with spells whose diagnosis is uncertain.
• Errors can also occur in patients with nonepileptic paroxysmal neurologic disorders when focal abnormalities are noted or when benign patterns are seen and misinterpreted as epileptiform activity.
• Lastly, patients may be misdiagnosed as having epilepsy when epileptiform like activity is due to drugs or metabolic disorders. Therefore, the EEG should always be correlated with the clinical history and imaging studies.

EEG
• The EEG offers high temporal resolution of brain activity.
• Understanding the physiologic basis for interictal and ictal EEG patterns provides insight to the pathophysiology and treatment approach used for the different epilepsies.
• The two main EEG hallmarks of epilepsy are the interictal spike or sharp wave in focal epilepsies and the frontocentral spike-wave discharges in the generalized epilepsies

Approach to the patient with epilepsy
• When evaluating a patient with possible epilepsy, the basic approach is as follows:
– Is this epilepsy, and, if so, is it focal or generalized?
– MRI
– EEG
– Video EEG

EEG
• The EEG is the defining study for epilepsy and is used to support the diagnosis of epilepsy and the epilepsy syndrome.
The first human EEG was recorded by Hans Berger in 1924 and demonstrated the occipital dominant alpha wave pattern associated with eye closure.

Spikes and Sharp waves
• The patterns of generalized spike-and-wave activity and focal spikes or sharp waves were defined as markers of epilepsy by Gibbs, Lennox, and Jasper in the 1930s.
• Since then the EEG has been invaluable to the study of epilepsy.


Sensitivity and Specificity of EEG
• The sensitivity of EEG in various studies had ranged from 29% to 55%, with studies showing an average of one-third of initial EEGs being abnormal.
• However, the sensitivity improves to about 80% to 90% if EEGs are repeated over time.
• Timing of EEG is important, with studies showing 51% of EEGs being abnormal if done within 24 hours of a seizure compared to 34% demonstrating abnormalities in later EEGs.

Case Example
• 18 yo patient presents first with tonic clonic seizure to the BRRH-ER.
• 1 year ago had 1 similar seizure. At that time the EEG and MRI were normal
• Patient EEG this time shows spike and slow wave discharges consistent with generalized in onset epilepsy.
• Patient also had staring spells, myoclonic jerks and tonic clonic seizures = …..



EEG Monitoring in the ICU


Other EEG modalities

USE OF AMBULATORY EEG MONITORING (WITH OR WITHOUT VIDEO) IN DIAGNOSIS OF EPILEPSY AND SPELLS
• The ILAE recommends long-term EEG monitoring in cases with spells; where diagnosis of epilepsy is uncertain; to classify the epilepsy syndrome in patients with known epilepsy; and for electroclinical localization among patients who are candidates for surgery.
• Several studies have examined the clinical utility of ambulatory EEG monitoring. In these studies, diagnosis was refined in anywhere from 50% to 75% of cases.

USE OF CONTINUOUS EEG MONITORING IN THE INTENSIVE CARE UNIT
• Continuous EEG (cEEG) monitoring is performed over hours or days to obtain information about cerebral function among patients who are critically ill:
• Who to monitor? – acute neurologic injury to monitor function,
– during treatment of status epilepticus to monitor treatment response,
– among patients with subarachnoid hemorrhage to monitor for vasospasm, and
– among patients with raised intracranial pressure after traumatic brain injury.

The first EEG - 1920
Berger H. Über das Elektrenkephalogramm des Menchen. Archives für Psychiatrie. 1929; 87:527-70.
• Prof. Hans Berger (1873-1941)

CONTINUOUS EEG MONITORING IN THE INTENSIVE CARE UNIT
• Similarly, nonconvulsive status epilepticus was found in up to 20% of patients with traumatic brain injury and 6% of patients with stroke or intracranial hemorrhage.
• In many institutions across the United States, cEEG monitoring is now performed routinely in patients with unexplained mental status or in obtunded patients with acute neurologic injury.