Embed Size (px)
Citation preview

Journal of Infection (2006) 53, 98e105
www.elsevierhealth.com/journals/jinf
Epidemiology, risk factors and outcome ofnosocomial infections in a RespiratoryIntensive Care Unit in North India
Ritesh Agarwal a,*, Dheeraj Gupta a, Pallab Ray b,Ashutosh N. Aggarwal a, Surinder K. Jindal a
a Department of Pulmonary Medicine, Postgraduate Institute of Medical Education and Research,Sector-12, Chandigarh-160012, Indiab Department of Medical Microbiology, Postgraduate Institute of Medical Education and Research,Sector-12, Chandigarh-160012, India
Accepted 26 October 2005Available online 15 December 2005
KEYWORDSNosocomial infections;Intensive care unit;Risk factors;Outcome
Summary Objective: To determine the epidemiology, risk factors and outcome ofinfections in a Respiratory Intensive Care Unit (RICU) of a tertiary care institute innorthern India.Methodology: Prospective, observational clinical study.Results: The study included 201 patients (1285 patient days) admitted to RICU overa period of one-and-a-half years. A total of 77 infections were identified in 67 pa-tients (33.5%). The infections included pneumonia (23%), sepsis of unknown origin(10.5%), bacteremia (7.5%), urinary tract infections (1.5%), catheter related bloodstream infections (1%) and Clostridium difficile colitis (1%). The most commonlyidentified organisms were the Acinetobacter species (34.8%), Pseudomonas aerugi-nosa (23.9%) and Escherichia coli (15.2%). The median length of stay in patientswith and without infection was 13 days (interquartile range, IQR, 28) and 4 days (in-terquartile range, IQR, 3), respectively (p< 0.0001). Multivariate analysis showedthe following risk factors for ICU-acquired infection: the admitting diagnosis of in-fection (odds ratio [OR] 3.3; 95% confidence intervals [CI] 1.06e10.1), length of stayin the RICU (OR, 1.2; 95% confidence intervals [CI] 1.1e1.33); renal failure (OR, 4.7;95% CI, 1.52e14.41) and institution of parenteral nutrition (OR, 16.9; 95% CI, 1.07e269.03). Multivariate analysis showed the following risk factors for death in ICU:APACHE II scores (OR, 1.06; 95% CI, 1.01e1.11), and endotracheal intubation (OR,5.07; 95% CI, 1.24e20.65).
* Corresponding author. Tel.: þ91 172 2756825x6076; fax: þ91 172 2745959.E-mail addresses: [email protected], [email protected] (R. Agarwal).
0163-4453/$30 ª 2005 The British Infection Society. Published by Elsevier Ltd. All rights reserved.doi:10.1016/j.jinf.2005.10.021

Nosocomial infections in a RICU in India 99
Conclusions: This study clearly documents a high prevalence rate of infections inthe ICU, and the data suggest that occurrence of infections was associated witha prolonged ICU stay but had no significant effect on the final outcome.ª 2005 The British Infection Society. Published by Elsevier Ltd. All rights reserved.
Introduction
Intensive care units (ICUs) have come to representthe most frequently identifiable sources of nosoco-mial infections within the hospital, with infectionand antimicrobial resistance rates several foldhigher than that in the general hospital setting.1e3
In fact, the likelihood of occurrence of infectionmay increase by 6% for each day spent in the hos-pital.4 Urinary tract infections, pneumonia and bac-teremia are currently the most common nosocomialinfections (NIs), and pneumonia is by far the leadingcause of death from nosocomial infection in theICU.4e6 The empiric treatment of infections in theICU demands an intimate knowledge of the epide-miology, the source, the type and the nature of in-fections as well as the antimicrobial resistancepatterns of the invading organisms.7 Some of thesefactors are unique to individual ICUs. The mortalityfrom infections in the ICU can be effectively re-duced by a timely and appropriate empiric antimi-crobial therapy. However, this requires knowledgeof local microbiological flora. Unfortunately, thereis a paucity of data on NIs from Indian ICUs. Resultsof Western studies cannot be directly applied in In-dia because of the differences in the case-mix, levelof intensive care, availability of resources and sev-eral other local factors. The present study was de-signed to look into the epidemiology, risk factorsand outcome of NIs in a Respiratory ICU at a largetertiary care institute in India.
Patients and methods
The study was conducted from July 2002 to Decem-ber 2003 for a period of 18 months in the RespiratoryIntensive Care Unit (RICU) of this institute, com-prising of six beds. The RICU serves to predominantlymedical patients of the hospital, and is a six-bedunit staffed by five physicians (four consultants andone resident specialized in Pulmonary medicine andIntensive Care). There are two cubicles with threebeds each, and there are 12 nurses with the nurseepatient ratio approximately 2e3:1. There are noroutine surveillance culture methods which arefollowed, and patients who are colonized withresistant bacteria are managed in the same cubiclewith barrier nursing, and at the earliest, the cubicle
undergoes chemical fumigation. Handwashing isroutinely followed with both alcohol and soapsolutions before and after contact with every in-dividual patient.
All patients admitted to the RICU for more than48 h were included in the study. An informed con-sent was taken from the patient or their relativesas applicable. Demographic information such asage and gender, operative status during the pre-ceding month, underlying and/or concomitant dis-eases, and clinical status at admission to ICUincluding the details of organ failure were recorded.The severity of the underlying illness was scoredusing the Acute Physiology and Chronic Health Eval-uation (APACHE) II scores.8 The details of intravas-cular or urinary catheters, tracheal intubation,tracheostomy,mechanical ventilation, surgicaldrains,peritoneal dialysis, hemodialysis or hemofiltration,nasogastric tubes, enteral or parenteral nutrition,were recorded. All patients with suspected infec-tion underwent liver and renal function test, com-plete blood count, urine examination, coagulationprofile, chest radiography, blood cultures e twofrom peripheral venous blood and one from centralvenous catheter, if present, tracheal aspirate cul-tures and urine cultures; other body fluids weresampled as clinically indicated. The decision of nos-ocomial infection (NI), and the need for starting an-timicrobial therapy was taken with both laboratoryand clinical findings. The infection should not havebeen present at ICU admission, even if not obviousat this time. The criteria suggested by the Centersof Disease Control (CDC)9 [http://www.cdc.gov/ncidod/hip/SURVEILL/NNIS.HTM] were used for de-fining specific infections modified as listed below.
Nosocomial pneumoniawas initially defined as theoccurrence of new and persistent infiltrates on chestX-ray plus two of the following three: fever> 38 �C,leucocytosis or leucopenia and purulent trachealaspirate. The diagnosis was subsequently confirmedwith quantitative tracheobronchial aspirates withcounts of �105 colony-forming units per milliliter(CFU/mL).
Urinary tract infection was diagnosed whenurine cultures grew organism� 105 CFU/mL andone of the following: (a) blood cultures growingthe same organism; (b) structural renal diseaseincluding renal stones, post-renal transplantation;and (c) urinary tract manipulation.

100 R. Agarwal et al.
Nosocomial primary bacteremia was diagnosedwith new onset of nonlocalizing sepsis with posi-tive blood cultures. Bacteremia was diagnosedwhen a blood culture grew an organism with orwithout any obvious focus of sepsis. Catheterrelated blood stream infection (CRBSI) was di-agnosed when blood culture from peripheral veinand central venous catheter (CVC) grew an organ-ism and CVC tip with quantitative bacterialcounts> 15 CFU (roll method of Maki et al.10).
Clostridium difficile colitis was diagnosed whenC. difficile toxin A or B was positive by ELISA and/or sigmoidoscopic evidence of colitis. Intra-abdominal sepsis was diagnosed with positive cul-ture of intra-abdominal fluid. Wound-infectionwas diagnosed with purulent exudates from woundand positive wound cultures.
The patient was said to have ‘‘sepsis of un-known origin’’, if the patient had suspected sepsiswith no apparent infection at any site and negativeblood cultures, along with the intensive carephysician’s decision to start empiric antibiotics.
Collection of blood, urine and other biomaterialfor microbiological examination was done underaseptic conditions as per CDC guidelines.9
Statistical analysis
Statistical analyses were performed using thestatistical software SPSS version 10.0 (SPSS Inc.,Chicago, IL, USA) software for MS-Windows. De-scriptive frequencies were expressed using mean(standard deviation) and median (range). Differ-ences between means of continuous variables werecompared using the unpaired student t test andanalysis of variance, as applicable, and that of cat-egorical variables with the Chi-square test. Riskfactors for developing hospital acquired infectionas well as mortality were evaluated using multivari-able logistic regression analysis. Initially the varia-bles were analyzed using univariate analysis toderive crude odds ratio and if found significant(p< 0.1) these variables were then entered ina multivariate logistic regression model to deriveadjusted odds ratio and confidence limits. Levelof significance was expressed as probability values(p value) and odds ratio (95% confidence intervals).Survival curves were constructed to study theeffect of infection on RICU stay using KaplaneMeieranalysis. Difference between two survival curveswas analyzed using the log-rank test.
Results
There were 278 admissions during the study periodof which 77 patients were excluded, as their
duration of stay was less than 48 h. The data con-sisted of 201 patients admitted in the RespiratoryIntensive Care Unit (RICU) during this period ofone-and-a-half years (1285 patient days). Therewere 128 male (63.7%) and 73 female (36.3%) pa-tients with the mean (standard deviation) age of41.4 (18.1%) years. The common admitting diagno-ses were community-onset infections (pneumonia,tuberculosis, malaria, typhoid fever, leptospirosis,etc.) (30.5%), neuromuscular diseases and res-piratory failure (28.5%) and the airway diseases(16.5%). The miscellaneous category (24.5%) in-cluded patients with obstructive sleep apneasyndrome, interstitial lung disease, cardiogenicpulmonary edema, pulmonary embolism, fat em-bolism syndrome and others. The baseline charac-teristics of patients with and without nosocomialinfection are shown in Table 1.
The prevalence of infection in our ICU was 33.5%(29.1 per 1000 patient days). There were 77episodes of infection in 67 of the 201 patients.Pneumonia was the most common infection (46/201 patients, 23%), which constituted 59.7% of all
Table 1 Baseline characteristics and outcome ofpatients admitted to the Respiratory Intensive CareUnit (RICU)
Characteristics Patientswith NI (%)(n¼ 67)
PatientswithoutNI (%)(n¼ 134)
Age less than65 years
63 (88) 116 (86.5)4 (12) 18 (13.5)
Male sex 42 (62.7) 86 (63.9)25 (37.3) 48 (36.1)
Admitting diagnosisCommunity-onset
infections36 (53.7) 25 (18.8)
Poisoning 1 (1.5) 3 (2.3)Airway disease 4 (6) 29 (21.8)Neuromuscular
disease16 (23.9) 37 (27.8)
Miscellaneous 10 (14.9) 40 (29.3)Antibiotics prior to
admission in RICU26 (38.8) 59 (44.4)
ICU parametersand outcome
APACHE II(median)
23 (IQR, 10) 15 (IQR, 4)
Time to 1st NI(median)
7 Days(IQR, 7)
e
Length of stay(median)
13 Days(IQR, 28)
8 Days(IQR, 7)
Mortality 38 (56.7) 30 (22.4)
Numbers in parentheses are percentages; IQR: interquartilerange.

Nosocomial infections in a RICU in India 101
nosocomial infections. This was followed by sepsisof unknown origin (21/201 patients, 10.5%). Therewere 15 patients with bacteremia, three withurinary tract infection and two each with catheterrelated blood stream infection and C. difficilecolitis. The median time to onset of infection was 7,22 and 35.5 days for 1st, 2nd and 3rd episodes ofinfections, respectively. Recurrences of infectiousepisodes were limited mostly to pneumonia. Therewere eight episodes of late-onset pneumonia (2ndepisode of NI). Two patients had 3rd episode of in-fection (one late-onset pneumonia and one CRBSI).Of the 77 episodes of infection, 40 (51.9%) wereculture positive, four (5.2%) were polymicrobial.Acinetobacter species was the most commonorganism followed by Pseudomonas aeruginosa.This was followed by Escherichia coli and otherswith different sensitivity patterns (Tables 2 and 3).
Sixty-one patients admitted with a diagnosis ofcommunity-onset infection; their median hospitalstay prior to RICU admission and total RICU staywas 4 (IQR, 1e10) and 5 (IQR, 3.5e8) days,respectively. All patients had received antibioticsprior to admission in the ICU. These patients werein general sicker than the other groups (APACHE IIscores, mean [SD]: community onset infections e19.6 [8.7], poisoning e 14.5 [3.4], airway diseases e16.3 [5.2], neuromuscular diseases e 9.6 [7.1] andmiscellaneous category e 16.2 [7.2]). Thirty-sixpatients developed an NI (median, 1; range, 1e3)with the median time to onset of infection being 8(IQR, 5e15) days.
The presence of various risk factors for acquir-ing infection such as admitting diagnosis of in-fection, endotracheal tube, invasive lines, surgicaldrains, parenteral feeding, renal failure, post-operative state, RICU stay and APACHE II scoreswere associated with significantly higher odds ofacquiring infection in RICU in univariate analysis(Table 4). In the multivariate model, after adjust-ment, the variables that predicted an increase risk
of infection in RICU were the presence of community-onset infection, length of RICU stay, presence ofrenal failure and institution of parenteral nutrition(Table 4).
Of the 201 patients, 133 survived and weredischarged from the RICU; 68 patients had died.The median APACHE II scores were 13 (interquar-tile range (IQR), 9) in patients who were dis-charged and 18 (IQR, 15) in patients who died(Table 5). We also studied the relationship be-tween various risk factors and ICU procedureswith outcome. In the multivariate model, after ad-justment, only the APACHE II scores and endotra-cheal intubation were predicting an adverseoutcome (Table 5). Survival curves were plottedfor patients with and without infection vis-a-visRICU stay (Fig. 1). The median RICU stay in pa-tients with infection was 13 days (IQR, 28) versus4 (IQR, 3) days in patients without infection. Thedifference between the curves was analyzed usingthe log-rank test and was found to be statisticallysignificant (p< 0.00001) (Fig. 1).
Discussion
The results of infection surveillance are importantprerequisites for the prevention and treatment ofnosocomial infections in any intensive care unit(ICU). However, there is hardly any published dataon surveillance of infection from India and most ofthe data on infection surveillance is from theWest.11e13 There is a great importance of interna-tional comparisons of results of infection surveil-lance data to prevent nosocomial infections andreach a quality of care.14 The results of differentICU studies yield different rates or types of nosoco-mial infection. The prevalence of infection in ourICU was 33.5% (29.1 per 1000 patient days). Thisis slightly high in comparison to the prevalence ofinfection in ICUs in Western countries, where it is
Table 2 Organisms isolated in nosocomial infection
Microorganisms Total Pneumonia Blood streaminfection
Urinary tractinfection
Others
Acinetobacter species 16 (34.8) 15 1 0 0Pseudomonas aeruginosa 11 (23.9) 11 0 0 0Escherichia coli 7 (15.2) 2 3 2 0MRSA 4 (8.7) 3 1 0 0Alcaligenes faecalis 2 (4.3) 2 0 0 0Klebsiella pneumoniae 1 (2.2) 0 0 1 0Candida species 2 (4.3) 0 2 0 0Others 3 (4.5) 1 0 0 2Total 46 (100) 34 7 3 2
Numbers in parentheses are percentages; MRSA: methicillin-resistant Staphylococcus aureus.

102 R. Agarwal et al.
Table 3 Sensitivity pattern of organisms isolated
Organism Antibiotic resistance (%)
Number Cefotaxime Amikacin Ceftazidime Ciprofloxacin Piperacillinetazobactam
Imipenem Methicillin
Acinetobacterspp.
16 100 75 94 50 44 8 (12) Not tested
Pseudomonasaeruginosa
11 100 27 82 28 9 16 (6) Not tested
Escherichiacoli
7 71 14 57 14 50 (4) 0 (3) Not tested
MRSA 4 100 100 Not tested 100 Not tested Nottested
100
Figure in parentheses denotes number tested, if not tested in all; MRSA: methicillin-resistant Staphylococcus aureus.
reported between 10 and 26%.4,5 There can be sev-eral reasons for this. One of the major factors isthe different case-mix; we had no post-operative,obstetric and cardiac patients, in whom the rateof infection per se is low. The ICU mainly catersto medically critically ill patients. Accordingly, in-fectious diseases (pulmonary or extrapulmonary)
were the most common indication for admissionin our ICU followed by respiratory failure second-ary to neuromuscular paralysis. Other common in-dications were acute severe asthma, exacerbationof chronic obstructive lung disease, bronchiectasisand a few others. This case-mix is obviously differ-ent from those reported from the West, with cases
Table 4 Risk factors and invasive procedures associated with nosocomial infection (NI) (multivariate analysis)
Patients withNI (n¼ 67)N (%)
Patients withoutNI (n¼ 134)N (%)
Crude OR(95% CI)
Adjusted OR(95% CI)
Admitting diagnosisCommunity-onset infections 36 (53.7) 25 (18.8) 4.9 (2.2e11.3)* 3.3 (1.06e10.1)*Poisoning 1 (1.5) 3 (2.3) 34.1 (6.7e173.3)* 3.7 (0.34e40.78)Airway disease 4 (6) 29 (21.8) 0.73 (0.25e2.1) eNeuromuscular disease 16 (23.9) 37 (27.8) 1.56 (0.66e3.66) eMiscellaneousa 10 (14.9) 40 (29.3) e ePossible risk factorsRICU stay, mean (SD), days 9.9 (10.2) 4.6 (2.6) 1.26 (1.14e1.4)** 1.2 (1.1e1.33)*APACHE II scores, median (IQR) 23 (10) 15 (4) 1.07 (1.03e1.1)** 1.01 (0.96e1.06)Gender (M/F) 42/25 86/48 0.63 (0.65e2.04) eGlucocorticoid therapy 11 (16.4) 11 (8.2) 2.18 (0.89e5.32) eImmunosuppressive therapy 8 (11.9) 7 (5.2) 2.44 (0.85e7.05) ePost-renal transplant 1 (1.5) 1 (0.75) 2 (0.12e32.48) eHematological malignancy 5 (7.5) 4 (2.9) 2.6 (0.68e10.02) eRenal failure 26 (38.8) 10 (7.5) 7.8 (3.47e17.54)** 4.7 (1.52e14.41)*Post-operative state 11 (16.4) 4 (2.9) 6.34 (1.93e20.75)* 2.5 (0.51e12.01)Diabetes mellitus 5 (7.5) 11 (8.2) 0.89 (0.3e2.7) eAIDS 2 (2.9) 1 (0.75) 0.99 (0.09e11.15) eAntibiotics prior
to RICU admission39 (58.2) 58 (43.3) 0.83 (0.54e1.27) e
Invasive proceduresEndotracheal intubation 59 (88.1) 67(50) 7.27 (3.22e16.37)** 1.78 (0.53e6.01)Reintubation 18 (26.9) 11(8.2) 2.24 (0.95e5.24) eInvasive lines 62 (92.5) 61 (45.5) 14.63 (5.58e38.7)** 3.02 (0.84e10.94)Nasogastric tube 63 (94.1) 80 (59.7) 10.64 (1.22e93.03)** 1.23 (0.26e5.81)Parenteral nutrition 5 (7.5) 1 (0.7) 10.6 (1.22e93.03)* 16.9 (1.07e269.03)*Surgical drains 9 (19.4) 9 (5.9) 2.14 (0.81e5.69) e
Univariate analysis done with chi-square test (Pearson test, Fisher’s exact test, and Yates’ continuity correction test). *p< .05,**p< .001.
a Reference category.
Nosocomial infections in a RICU in India 103
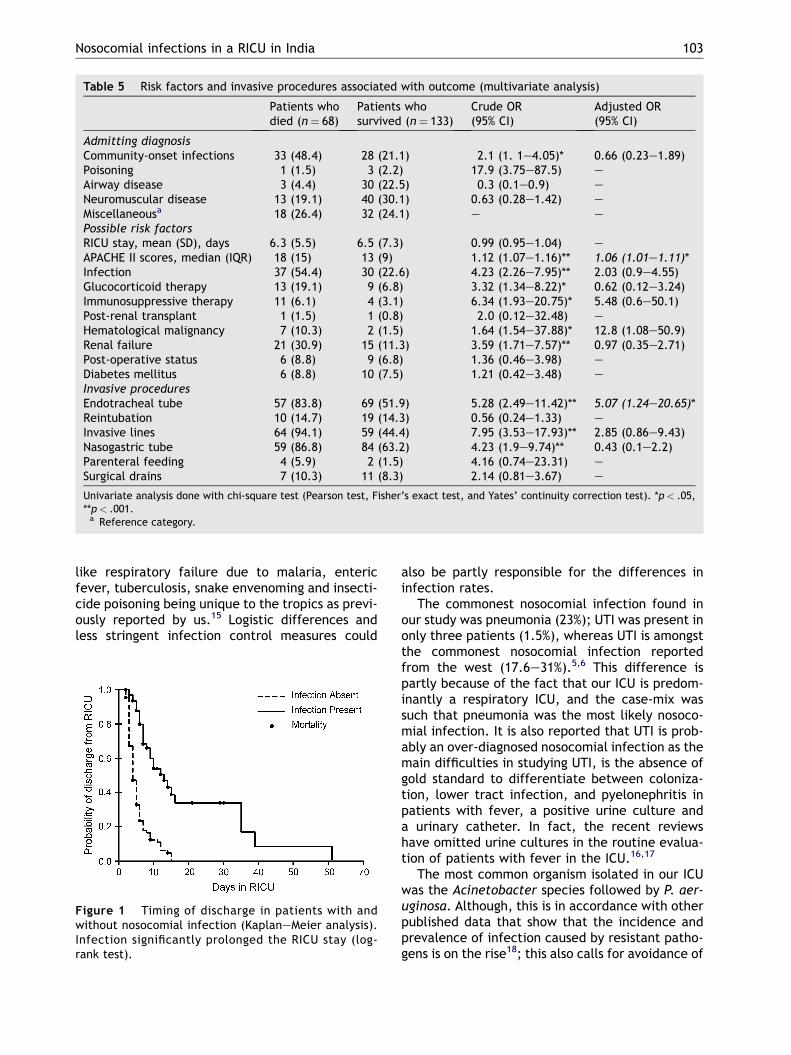
Table 5 Risk factors and invasive procedures associated with outcome (multivariate analysis)
Patients whodied (n¼ 68)
Patients whosurvived (n¼ 133)
Crude OR(95% CI)
Adjusted OR(95% CI)
Admitting diagnosisCommunity-onset infections 33 (48.4) 28 (21.1) 2.1 (1. 1e4.05)* 0.66 (0.23e1.89)Poisoning 1 (1.5) 3 (2.2) 17.9 (3.75e87.5) eAirway disease 3 (4.4) 30 (22.5) 0.3 (0.1e0.9) eNeuromuscular disease 13 (19.1) 40 (30.1) 0.63 (0.28e1.42) eMiscellaneousa 18 (26.4) 32 (24.1) e ePossible risk factorsRICU stay, mean (SD), days 6.3 (5.5) 6.5 (7.3) 0.99 (0.95e1.04) eAPACHE II scores, median (IQR) 18 (15) 13 (9) 1.12 (1.07e1.16)** 1.06 (1.01e1.11)*Infection 37 (54.4) 30 (22.6) 4.23 (2.26e7.95)** 2.03 (0.9e4.55)Glucocorticoid therapy 13 (19.1) 9 (6.8) 3.32 (1.34e8.22)* 0.62 (0.12e3.24)Immunosuppressive therapy 11 (6.1) 4 (3.1) 6.34 (1.93e20.75)* 5.48 (0.6e50.1)Post-renal transplant 1 (1.5) 1 (0.8) 2.0 (0.12e32.48) eHematological malignancy 7 (10.3) 2 (1.5) 1.64 (1.54e37.88)* 12.8 (1.08e50.9)Renal failure 21 (30.9) 15 (11.3) 3.59 (1.71e7.57)** 0.97 (0.35e2.71)Post-operative status 6 (8.8) 9 (6.8) 1.36 (0.46e3.98) eDiabetes mellitus 6 (8.8) 10 (7.5) 1.21 (0.42e3.48) eInvasive proceduresEndotracheal tube 57 (83.8) 69 (51.9) 5.28 (2.49e11.42)** 5.07 (1.24e20.65)*Reintubation 10 (14.7) 19 (14.3) 0.56 (0.24e1.33) eInvasive lines 64 (94.1) 59 (44.4) 7.95 (3.53e17.93)** 2.85 (0.86e9.43)Nasogastric tube 59 (86.8) 84 (63.2) 4.23 (1.9e9.74)** 0.43 (0.1e2.2)Parenteral feeding 4 (5.9) 2 (1.5) 4.16 (0.74e23.31) eSurgical drains 7 (10.3) 11 (8.3) 2.14 (0.81e3.67) e
Univariate analysis done with chi-square test (Pearson test, Fisher’s exact test, and Yates’ continuity correction test). *p< .05,**p< .001.
a Reference category.
like respiratory failure due to malaria, entericfever, tuberculosis, snake envenoming and insecti-cide poisoning being unique to the tropics as previ-ously reported by us.15 Logistic differences andless stringent infection control measures could
Figure 1 Timing of discharge in patients with andwithout nosocomial infection (KaplaneMeier analysis).Infection significantly prolonged the RICU stay (log-rank test).
also be partly responsible for the differences ininfection rates.
The commonest nosocomial infection found inour study was pneumonia (23%); UTI was present inonly three patients (1.5%), whereas UTI is amongstthe commonest nosocomial infection reportedfrom the west (17.6e31%).5,6 This difference ispartly because of the fact that our ICU is predom-inantly a respiratory ICU, and the case-mix wassuch that pneumonia was the most likely nosoco-mial infection. It is also reported that UTI is prob-ably an over-diagnosed nosocomial infection as themain difficulties in studying UTI, is the absence ofgold standard to differentiate between coloniza-tion, lower tract infection, and pyelonephritis inpatients with fever, a positive urine culture anda urinary catheter. In fact, the recent reviewshave omitted urine cultures in the routine evalua-tion of patients with fever in the ICU.16,17
The most common organism isolated in our ICUwas the Acinetobacter species followed by P. aer-uginosa. Although, this is in accordance with otherpublished data that show that the incidence andprevalence of infection caused by resistant patho-gens is on the rise18; this also calls for avoidance of

104 R. Agarwal et al.
unnecessary antibiotics and strict institution ofhandwashing which we have already instituted inour ICU.
As reported earlier,5,13,19e21 the main risk factorsfor development of infection in this study were thelength of ICU stay, renal failure and institution ofparenteral nutrition. We also found the admittingdiagnosis of community-onset infections as a signifi-cant risk factor for NI. The possible reason is that allthese patients are more critically ill and are thussubjected to a greater instrumentation than othergroups. Although it may initially seem that there isa disparity between the diagnoses of NI in patientswith community-onset infections, the occurrenceof NI was at a median of 8 days (IQR, 5e15) which in-dicates that an individual admitted with communi-ty-onset infection has gone on to develop an NI.Age and gender were not found to be significantrisk factors. Age as a risk factor for nosocomial in-fection has been debated in different studies bothin favor and against this association.13,19e22 In ourstudy, the APACHE II scores were not statisticallysignificant risk factors for development of nosoco-mial infection. It has been reported that highAPACHE II scores correlated with mortality but notwith infection.19,23 On the other hand, there are re-ports that the risk of developing nosocomial pneu-monia increased with increasing APACHE II scoresin surgical or general ICU patients.13 Also, endotra-cheal intubation was not found to be a significantfactor for infection on multivariate analysis despitemost studies showing it to be a risk factor. The rea-son for this could be the fact that it is also the con-comitant administration of antibiotics which couldhave some protective effect.
We also evaluated the factors affecting the out-come of patients in the RICU. Unlike infection, theRICU stay did not affect the outcome. In themultivariate analysis, the most important predic-tion of outcome was APACHE II score, with patienthaving an OR of dying of 1.1 (95% CI, 1.05e1.18) forevery unit rise in APACHE score. Thus, the higher theAPACHE II scores, the poorer the outcome. Theother factors associated with death were the pres-ence of invasive intravascular lines, which wererelated to the severity of illness of patients admit-ted in RICU. Infection was not associated witha poorer outcome possibly because of an aggressiveantibiotic policy, reiterating the view that early andadequate empirical antibiotic therapy is the mainfactor which affects the outcome of patients, ratherthan the diagnostic techniques used for the evalu-ation of infection.24e27 Other studies have alsofailed to demonstrate the impact of ICU-infectiononmortality rate in the ICU.5,6 KaplaneMeier survivalcurves constructed for patients with and without
infection showed that infection was associatedwith a prolonged stay in the RICU. In the reported lit-erature, the excess length of hospital stay due tonosocomial infection depends on the type of infec-tionandhasbeenestimatedtoadd1e4days forurinarytract infections and 7e30 days for pneumonia.28
The major limitations of our study include therelative small number of patients, and many of theconclusions regarding risk factors in our study havelimitations because of the small numbers of pa-tients in each group, as our data set did not allowfor a valid assessment, of whether, some of theserarer conditions in the study population may ormay not be a contributing factor. The modifica-tions of some of the definitions for the diagnosis ofinfections may also be regarded as another limi-tation although such limitations are likely to occurbased on the availability of resources.
Nosocomial infections, especially those causedby antibiotic-resistant pathogens, represent animportant source of morbidity for patients hospi-talized in an ICU. Evidence suggests that reducingthe use of certain antibiotics may lead to a de-creased prevalence of antibiotic-resistant patho-gens.18 The key to control antibiotic-resistantpathogens in the ICU is rigorous adherence to theinfection control guidelines and prevention of anti-biotic misuse.29
Conclusions
In conclusion, this study clearly documents a highprevalence rate of infections in the intensive careunit (ICU), the importance of pneumonia (which wasthe most common ICU-acquired infection), and therelative frequency of various infecting organisms.The study has identified the importance of certainrisk factors that increase the risk of developing ICU-acquired infection. However, it is not possible fromthis study to state categorically whether the de-velopment of an ICU-acquired infection increasedthe mortality rates in the critically ill. The results ofthis study should serve as a reference point forgreater surveillance and institution of greater pre-ventive measures. There is a considerable potentialfor reduction of morbidity, ICU stay and hospitalcosts, through introduction of well-implementedinfection control policies.
References
1. Brown RB, Hosmer D, Chen HC, Teres D, Sands M, Bradley S,et al. A comparison of infections in different ICUs within thesame hospital. Crit Care Med 1985;13:472e6.

Nosocomial infections in a RICU in India 105
2. Spencer RC. Epidemiology of infection in ICUs. IntensiveCare Med 1994;20(Suppl. 4):S2e6.
3. Craven DW, Steger KA. Nosocomial pneumonia in mechani-cally ventilated adult patients: epidemiology and preven-tion. Semin Respir Infect 1996;11:32e53.
4. Eggimann P, Pittet D. Infection control in the ICU. Chest2001;120:2059e93.
5. Vincent JL, Bihari DJ, Suter PM, Bruining HA, White J, Nicolas-Chanoin MH, et al. The prevalence of nosocomial infection inintensive care units in Europe. Results of the european prev-alence of infection in intensive care (EPIC) study. EPIC Inter-national Advisory Committee. JAMA 1995;274:639e44.
6. Richards MJ, Edwards JR, Culver DH, Gaynes RP. Nosocomialinfections in combined medicalesurgical intensive careunits in the United States. Infect Control Hosp Epidemiol2000;21:510e5.
7. Haley RW, Culver DH, White JW, Morgan WM, Emori TG,Munn VP, et al. The efficacy of infection surveillance andcontrol programs in preventing nosocomial infections in UShospitals. Am J Epidemiol 1985;121:182e205.
8. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHEII: a severity of disease classification system. Crit CareMed 1985;13:818e29.
9. Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM. CDCdefinitions for nosocomial infection. Am J Infect Control1988;16:128e40.
10. Maki DG, Weise CE, Sarafin HW. A semiquantitative culturemethod for identifying intravenous-catheter-related infec-tion. N Engl J Med 1977;296:1305e9.
11. Barsic B, Beus I, Marton E, Himbele J, Klinar I. Nosocomialinfections in critically ill infectious disease patients: resultsof a 7-year focal surveillance. Infection 1999;27:16e22.
12. Bouletreau A, Dettenkofer M, Forster DH, Babikir R,Hauer T, Schulgen G, et al. Comparison of effectivenessand required time of 2 surveillance methods in intensivecare patients. J Hosp Infect 1999;41:281e9.
13. Erbay H, Yalcin AN, Serin S, Turgut H, Tomatir E, Cetin B,et al. Nosocomial infections in intensive care unit in a Turk-ish university hospital: a 2 year survey. Intensive Care Med2003;29:1482e8.
14. Mertens R, Van den Berg JM, Veerman-Brenzikofer ML,Kurz X, Jans B, Klazinga N. International comparison ofresults of infection surveillance: The Netherlands versusBelgium. Infect Control Hosp Epidemiol 1994;15:574e8.
15. Aggarwal AN, Gupta D, Behera D, Jindal SK. Spectrum andoutcome of patients with acute respiratory failure admittedto respiratory critical care unit. Bull PGI 1999;33:20e6.
16. Marik PE. Fever in the ICU. Chest 2000;117:855e69.17. Rizoli SB, Marshall JC. Saturday night fever: finding and con-
trolling the source of sepsis in critical illness. Lancet InfectDis 2002;2:137e44.
18. Weber DJ, Raasch R, Rutala WA. Nosocomial infection in theICU: the growing importance of antibiotic-resistant patho-gens. Chest 1999;115:34Se41S.
19. Appelgren P, Hellstrom I, Weitzberg E, Soderlund V,Bindslev L, Ransjo U. Risk factors for nosocomial intensivecare infection: a long-term prospective analysis. ActaAnaesthesiol Scand 2001;45:710e9.
20. Stephan F, Cheffi A, Bonnet F. Nosocomial infections andoutcome of critically ill elderly patients after surgery.Anesthesiology 2001;94:407e14.
21. Legras A, Malvy D, Quinioux AI, Villers D, Bouachour G,Robert R, et al. Nosocomial infections: prospective surveyof incidence in five French intensive care units. IntensiveCare Med 1998;24:1040e6.
22. Craven DE, Kunches LM, Lichtenberg DA, Kollisch NR,Barry MA, Heeren TC, et al. Nosocomial infection and fatal-ity in medical and surgical intensive care unit patients. ArchIntern Med 1988;148:1161e8.
23. Kollef MH, Sherman G, Ward S, Fraser VJ. Inadequate anti-microbial treatment of infections: a risk factor for hospitalmortality among critically ill patients. Chest 1999;115:462e74.
24. Chastre J, Fagon JY. Ventilator-associated pneumonia. Am JRespir Crit Care Med 2002;165:867e903.
25. Iregui M, Ward S, Sherman G, Fraser VJ, Kollef MH. Clinicalimportance of delays in the initiation of appropriate antibi-otic treatment for ventilator-associated pneumonia. Chest2002;122:262e8.
26. Mehta R, Niederman MS. Adequate empirical therapy mini-mizes the impact of diagnostic methods in patients withventilator-associated pneumonia. Crit Care Med 2000;28:3092e4.
27. Heyland D, Ewig S, Torres A. Pro/con clinical debate: theuse of a protected specimen brush in the diagnosis of ven-tilator associated pneumonia. Crit Care 2002;6:117e20.
28. McCusker ME, Perisse AR, Roghmann MC. Severity-of-illnessmarkers as predictors of nosocomial infection in adult in-tensive care unit patients. Am J Infect Control 2002;30:139e44.
29. Garner JS. Guideline for isolation precautions inhospitals. The Hospital Infection Control PracticesAdvisory Committee. Infect Control Hosp Epidemiol 1996;17:53e80.
























![Bearman nosocomial infections[1]](https://img.dokumen.tips/doc/110x75/55499096b4c90583678b5577/bearman-nosocomial-infections1.jpg)


