Embed Size (px)
Citation preview
EPIDEMIOLOGYOutbreak Investigation
Sue Lindsay, Ph.D., MSW, MPH
Division of Epidemiology and Biostatistics
Institute for Public Health
San Diego State University

US Public Health Service Commissioned Corps
http://www.usphs.gov/
Citizen Emergency Response Teams
http://www.citizencorps.gov/cert/

The Natural History of Disease
Disease
Onset
Symptoms Seek
Care
Diagnosis/
Treatment
HealthyOutcome

Pre-Clinical Disease
• Incubation Period
• Latency Period

Incubation Period
• The period of time from exposure to infectious agent to the onset of detectable clinical illness
Factors that Affect Incubation Period
• Invasive ability of the infectious agent
• The time needed for replication and growth of the infectious organism until clinical disease is achieved and manifested
• The body site of infection
• Dose

The Epidemiologic Curve
• The distribution of number of new cases of a disease by date or time of onset
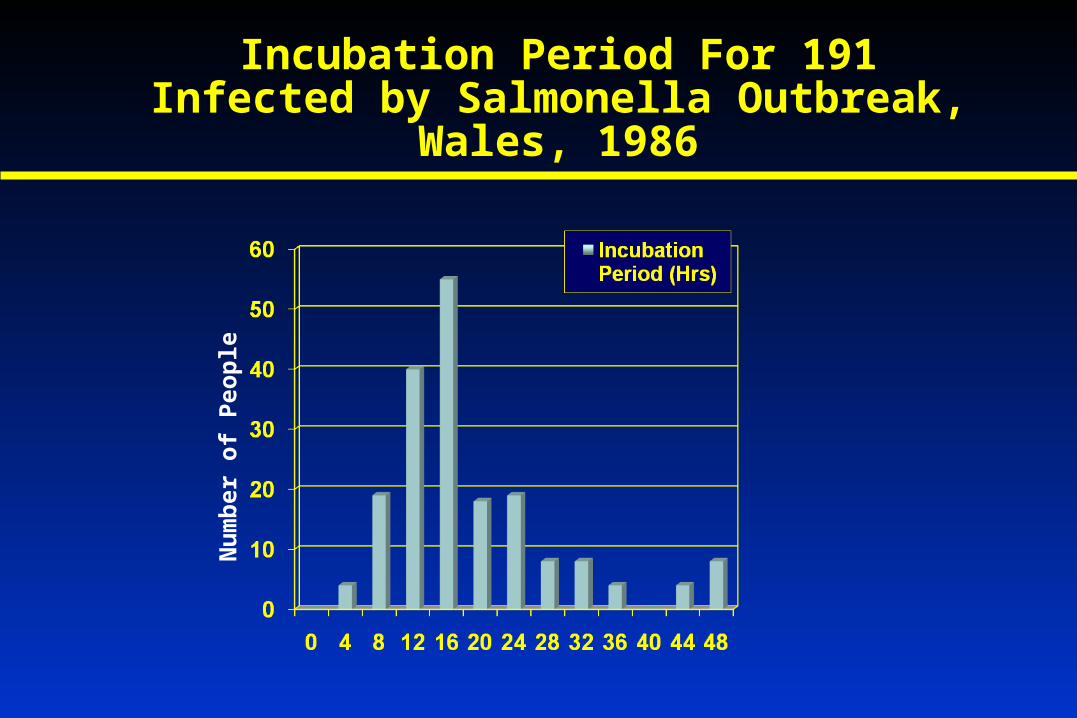
Incubation Period For 191 Infected by Salmonella Outbreak, Wales, 1986
Nu
mb
er o
f P
eop
le

Salmonella Outbreak, Wales, 1986
• Characterized by a rapid, explosive rise in the number of cases in first 16 hrs.
• This curve suggests a common-source, single-exposure epidemic
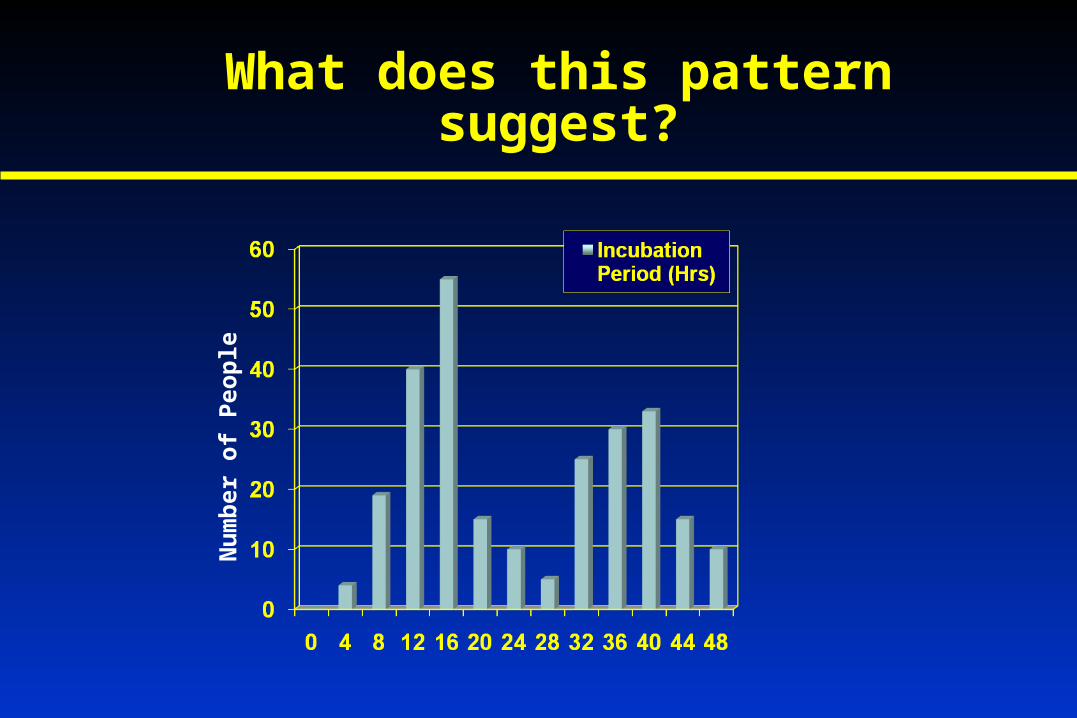
What does this pattern suggest?
Nu
mb
er o
f P
eop
le

Chronic Disease: Latency Period
• The analog for incubation period in non-infectious diseases is the latency period
• Example: The period of time from exposure to a carcinogen to the onset of cancer.

Annual Incidence Rate of Leukemia After Atomic Bomb Explosion
Hiroshima, Japan, 1945-1957In
cid
ence
Rat
e P
er 1
00,0
00

281 Cases of Bladder Tumors Among Dyestuff Workers
Nu
mb
er o
f C
ases

Emerging Infectious Diseases
“To write about infectious diseases is almost to write of something that has passed into history. The most likely forecast about the future of infectious disease, is that it will be very dull”
Natural History of Infectious Disease, 1962

Emerging Infectious Diseases
• Since 1975, previously unknown diseases have surfaced at an alarming pace, more than 30 new diseases in 30 years, most of them newly discovered viruses.
• These new viruses tend to come from other species – zoonosis
• Ebola, HIV, avian influenza
• Viruses are “masters of interspecies navigation”

What is Going On?
• Archeological evidence suggests that small, nomadic human groups hardly every suffered from contagious disease.
• Agriculture and the domestication of animals brought humans into close exposure to animals, animal and human waste, and reservoirs of disease.
Human Disease from Animals
• Tuberculosis goats
• Measles cows
• Smallpox cattle
• Whooping cough pigs
• Typhoid fever chickens
• Influenza ducks
• Leprosy water buffalo
• Common cold horses or cattle
• Peptic ulcer (helicobacter) sheep’s milk

What is Going On?
• The chief risk factor for emerging zoonotic diseases is environmental degradation by humans.
World Health Organization Coordinator for Zoonoses Control
• Global Climate Change
• Deforestation/Infringement on animal habitat
• Industrialization and intensification of the animal production sector (intensive factory farming)

Avian Influenza
• Natural reservoir is wild ducks
• Causes epidemics in poultry and other bird populations exposed to infected ducks
• Requires dense populations of birds, unsanitary and stressful conditions
• There has been a significant increase in bird flu epidemics with the advent of high density indoor poultry farming and the globalization of this type of poultry production
• Most avian influenza strains do not generally jump from birds to humans

Avian Influenza
• RNA virus with two types of enzyme spikes protruding from the surface of the virus, causing illness in birds
• 16 hemagglutinin enzymes (H1 to H16)
• 9 neuraminidase enzymes (N1 to N9)
Pandemic human infections began:
• 1918 Flu: H1N1, killed 100 million people “Spanish flu”
• 1957 Flu: H2N2, killed 1 million people worldwide “Asian flu”
• 1968 Flu: H3N2, 40% US adolescents sick “Hong Kong flu”
• Current H5N1 started in humans in 1997 in China…
Avian Influenza H5N1
• Spring 1997 in Hong Kong: thousands of chickens were dying from H5N1
• May 14 1997 Hong Kong: 3 year old boy died of multiple organ failure: H5N1
• 18 sick, 6 died in Hong Kong in 1997: all multiple organ failure, all had been exposed to chickens
• Hong Kong ordered the slaughter of more than a million birds
• Human infections ceased

Avian Influenza H5N1
• Early 2004: Widespread outbreaks of H5N1 in chicken flocks throughout eight countries in Southeast Asia with evidence that the virus was mutating to more virulent strains
• December 2007, 351 laboratory confirmed human cases, 217 deaths in twelve countries (62% mortality)
• December 2006, 263 laboratory confirmed human cases, 158 deaths in ten countries (60% mortality). Two cases of very close contact human-to-human transmission. No evidence of airborne human-to-human transmission.
• June 2008, 385 laboratory confirmed human cases, 243 deaths in twelve countries (63% mortality)
• August 2009, 438 laboratory confirmed human cases, 262 deaths in twelve countries (60% mortality)
Avian Influenza H5N1
• H5N1 has infected other mammals:
• Pigs
• Cats
• Tigers
• Leopards (more than 100 big cats at a Thailand zoo)
• Ferrets.
• These home and zoo outbreaks suggest viral infection in the meat of chicken used as feed.

Avian Influenza H5N1 - 2006
• “Recent laboratory and epidemiologic studies have yielded disturbing evidence that the H5N1 virus has become progressively more pathogenic in poultry, has increased environmental resistance, and is expanding its mammalian host range”
New England Journal of Medicine
• “The virus remains unstable, unpredictable and very versatile. Anything could happen. Judging from the way the virus has behaved, it may have new and unpleasant surprises in store for us”
World Health Organization
• “H5N1 is the one that scares us shitless”
Robert Webster, Chair of Virology, St Jude Children’s Research Hospital

H5N1 Epidemiologic Curve: August 11, 2009
China
VietnamThailand
Vietnam
Cambodia
Indonesia
China Thailand
Vietnam
Azerbaijan
Cambodia
China
Indonesia
Djibouti, Iraq, Turkey, Egypt
Thailand
Total = 438 cases, 262 deaths (60%)
Cambodia
China
Indonesia
Djibouti, Egypt, Iraq, Turkey
Thailand, Vietnam
Lao, Myanmar
Nigeria, Pakistan
Bangladesh
China
Egypt
Indonesia
Vietnam
Cambodia
China
Egypt
Indonesia
Vietnam
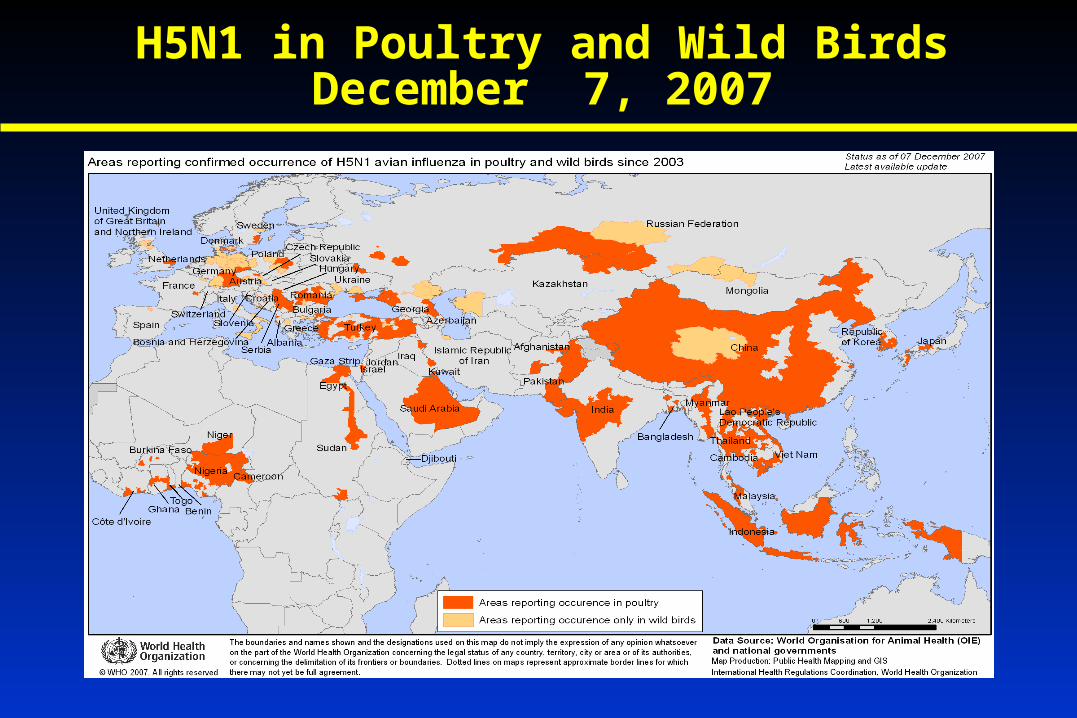
H5N1 in Poultry and Wild BirdsDecember 7, 2007

Human Cases of Avian H5N1As of May 6, 2009

Swine Influenza
• Natural reservoir is swine (pigs)
• Causes epidemics in pigs and are a challenge to the swine industry
• Swine have both avian and mammalian receptors, allowing viruses to exchange genetic material and produce new virus - “mixing vessels”. Swine flu is frequently found in farmed turkeys.
• Most outbreaks in swine herds occur in the fall and winter
• Swine flu in European herds differ genetically from North American Swine flu infections in herds.
• Most swine influenza strains do not generally jump from swine to humans, very rarely human infections

Swine Influenza
In Swine• A (H1N1) – 80 years in swine herds, very stable
• 1998 – H3N2 emerged in US swine. Contained avian, human, and swine viral genes
• Also H1N2 and H3N1 exists in swine herds
Human infections:
• 1976 Flu: Soldiers in Fort Dix, New Jersey, 1 death. The virus circulated for one month and then disappeared.
• Current H1N1 started in humans this year in North America

Novel A (H1N1)
• Contains human, avian, and swine genes. It has NEVER been identified in a swine herd. Can it be called swine?
• Human-to-human transmission with no proof of swine-person transmission.
• Contains gene segments from both European and North American swine genotypes.
• Morbidity is high and mortality is low compared to H5N1 avian influenza

http://id.uga.edu/docs/swine-flu-summary-genotype.pdf
Novel H1N1 Genotype

Novel H1N1 Influenza
• March 15, 2009. Infection in a young boy in Veracruz, Mexico
• March 17, 2009. Infection in Oaxaca, Mexico
• Between March 18th and April 18th, 47 cases
• March 28, 2009. Infection in a young girl in Brawley, California
• Younger sibling sick 10 days earlier
• No exposure to pigs/swine, travel to Mexico, or exposure to Mexican travelers
• CDC unable to type
Mexico
California

Veracruz, Mexico March 15th, 2009
Oaxaca, Mexico March 17th, 2009
Brawley, California March 28th, 2009

Novel H1N1 Epidemiologic Curve: August 23, 2009
11 countries
Total = 209,438+ cases, 2185+ deaths (1%)
51 countries 120 countries Africa
Americas
Eastern Med
Europe
Southeast Asia
Western Pacific
Africa
Americas
Eastern Med
Europe
Southeast Asia
Western Pacific

http://gamapserver.who.int/h1n1/cases-deaths/h1n1_casesdeaths.html
Novel H1N1 World Spread
Considerations for Pandemic Influenza
1. Pandemic influenza can have different origins (avian, swine)
2. Influenza pandemics are recurring events
3. The world is experiencing a new pandemic
4. Do we have adequate supplies of antiviral medicine and vaccines?
5. Humans have no immunity – widespread illness
6. Economic and social disruptions could be great

Mitigation
You need a balance between:
• Reducing illness and death through social distancing
• Minimizing social disruption
• Interventions shouldn’t be worse than the disease!

Steps in the Investigation of an Acute Disease Outbreak
I. Define The Epidemic
• Identify cases
• Clinical features
• Is this a known disease?
• Serology/Cultures
• Cause Understood?

II. Examine Time and Place
• Who is getting the disease? Specific populations?
• Plot onset times and number of cases
• Look for relationships between time and place
• Collect lots of information!
• If exposure known, calculate attack rates

III. Develop Hypotheses
• Use existing knowledge
• Analogy to diseases of known etiology

IV. Test Hypotheses
• Further analyze existing data
• Collect more data
V. Recommend Control Measures
• Control of present outbreak
• Prevention of future outbreaks

Etiologic Investigation of a Food-Borne Outbreak
• May 23, 1996, Charleston, South Carolina
• Luncheon – 64 attendees
• 39 persons developed diarrheal illness
• What is the overall attack rate?
• 39/64 = 61%

Etiologic Investigation of a Food-Borne Outbreak
Ate Sick AR Not eat Sick AR RR
Ham 25 11 37 26
P. Salad 19 16 42 20
Raspberries 37 33 24 4
44% 70%
84% 48%
89% 17%
Overall attack rate 61%
0.6
1.8
5.2

HomeworkChapter 2, page 35, Questions 2&3
Due September 25, 2009
Ate Sick AR Not eat Sick AR
Ate egg salad ___ ___ ____ ____ ____ ___
Ate tuna ___ ___ ____ ____ _____ ___
Ate both ___ ___ ____ ____ _____ ___
Use the information from the two tables in your text to populate this table and answer
the two questions. For full credit on your homework, we will need to see this table!





























