Embed Size (px)
Citation preview
Epidemiology of Epidemiology of Clostridium Clostridium
difficiledifficile infection (CDI)infection (CDI)Lyn Gilbert,Lyn Gilbert,
Sydney Institute for Emerging Sydney Institute for Emerging
Infectious Disease & CIDMInfectious Disease & CIDM-- Public Public
Health Health
Hospital Week 2010Hospital Week 2010

Clostridium difficile
- background
• 1st described 1935 – Bacillus difficilis
• 1978 - cause of: – (10-20%) antibiotic-associated diarrhoea
– pseudomembranous colitis
• Gram positive; spore-forming anae anaerobe
• Toxin-mediated disease
Distribution & acquisition
• Ubiquitous – environment (water), domestic animals
• Asymptomatic faecal carriage– 3% adults (~50% in LTCF) ; 66% infants
• Acquisition – ingestion– Spores widely disseminated
• Resistant to antiseptics
– Hand/skin contamination; fomites
• Major risks:– Hospital admission; prolonged stay
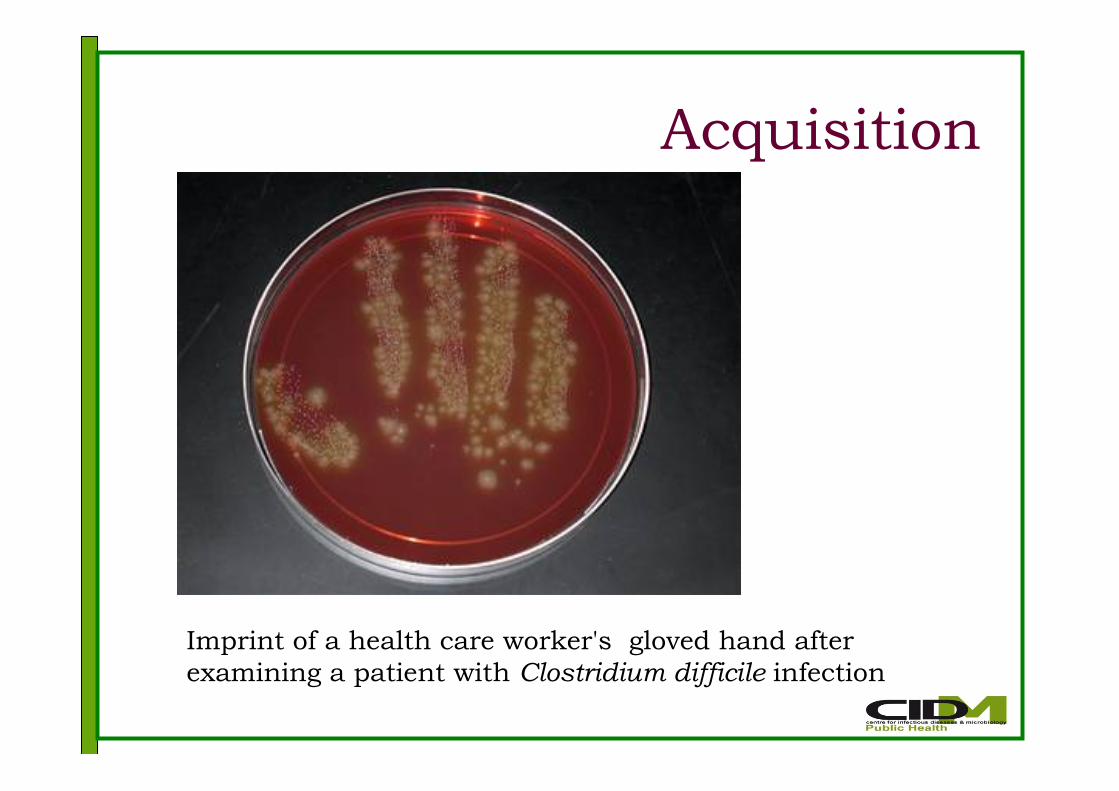
Acquisition
Imprint of a health care worker's gloved hand after
examining a patient with Clostridium difficile infection

Pathogenesis
• Acquisition of toxigenic strain– Reduced colonisation resistance
• e.g. ?gastric acid suppressants
• Altered bowel flora• Antibiotics – broad spectrum; prolonged;
polypharmacy
• GI surgery; procedures; co-morbidities; age
• Neonates resistant to disease
• Elderly most at risk
C. difficile toxins
• 19.6 kb pathogenicity locus (PaLoc)
– tcdA, tcdB – encode toxins A & B
– tcdR, tcdE – toxin regulation/secretion
• Produced during stationary phase
– tcdC – -ve regulator of toxin synthesis
• Produced during log phase
• Binary toxin - ?role; uncommon
– ?enhances bacteria adherence
• Most common:
– A+B+binary-ve; A-B+binary-ve

Risks for nosocomial CDIRisk factor Odds ratio P value
No acid suppression 1
H2RA only 1.53 .008
Daily protein pump
inhibitor (PPI)
1.74
<.001
>Daily PPI 2.36
Age, per year 1.01
No antibiotics 1
Low risk a/b 1.82 .008
High risk a/b 3.57
<.001Other co-morbidities 1.5-2.3
Howell et al. Arch Intern Med 2010; 170:784-90
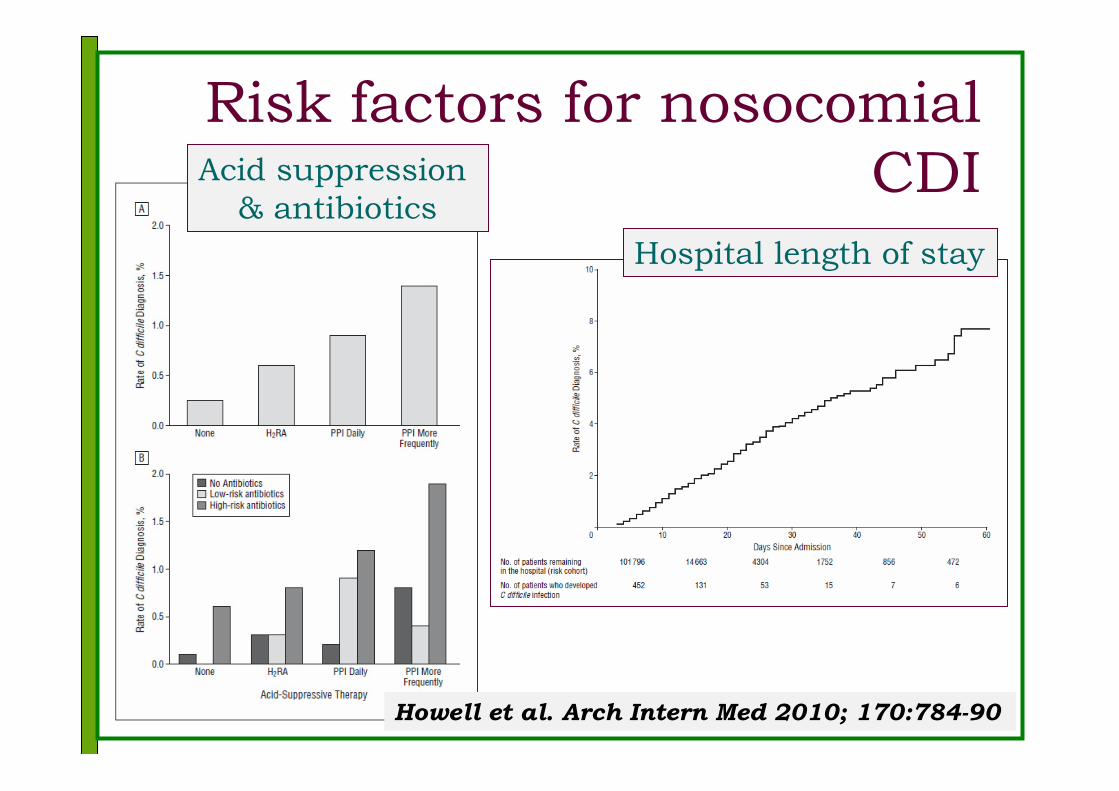
Risk factors for nosocomial
CDI
Howell et al. Arch Intern Med 2010; 170:784-90
Acid suppression
& antibiotics
Hospital length of stay
CDI in Canada
• 2003-4: CDI outbreaks
– Montreal (& other Quebec) hospitalsEggerston & Sibbald: CMAJ 2004;171:19-21
• Hypotheses Loo et al: CMAJ 2004;171:47-8
– Emergence of hypervirulent strain?
• 85% strains - clonal (by PFGE)
– More susceptible hosts?
• Older, sicker, immunocompromised; PPIs
– High risk antibiotics (fluoroquinolones)
– Poor housekeeping/infection control
--
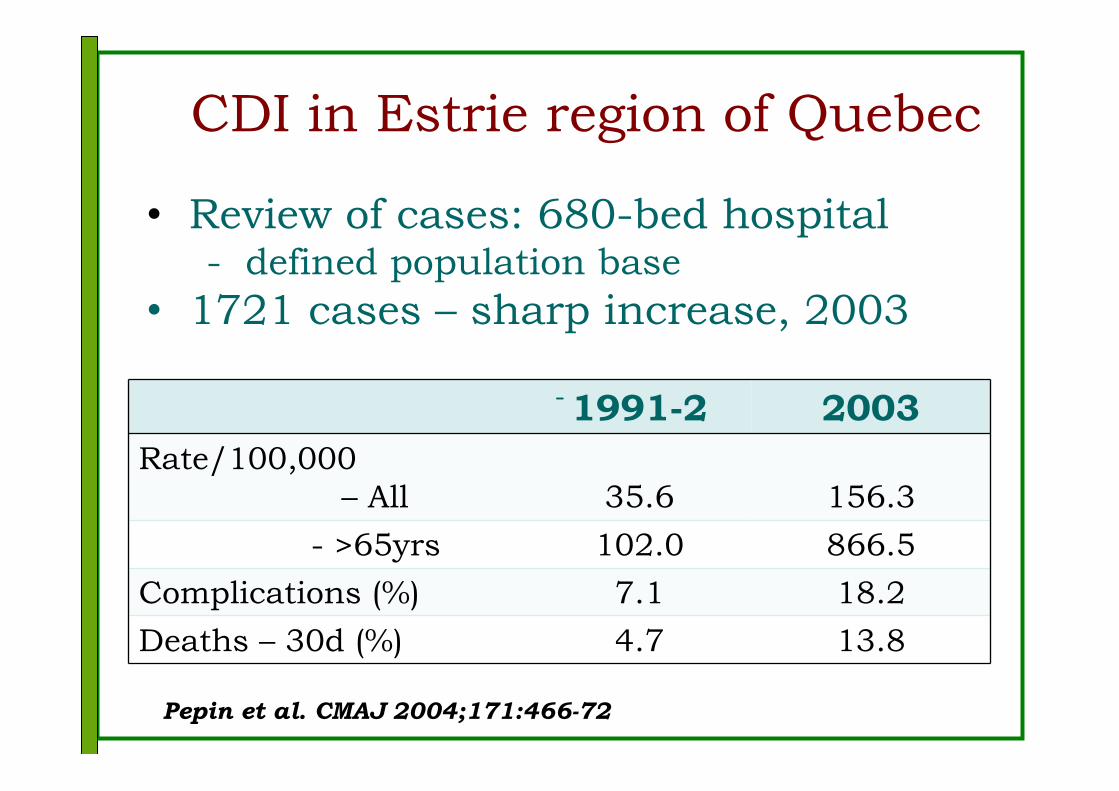
CDI in Estrie region of Quebec
1991-2 2003
Rate/100,000
– All 35.6 156.3
- >65yrs 102.0 866.5
Complications (%) 7.1 18.2
Deaths – 30d (%) 4.7 13.8
--
• Review of cases: 680-bed hospital - defined population base
• 1721 cases – sharp increase, 2003
Pepin et al. CMAJ 2004;171:466-72

Age-related incidence of CDI
Quebec 1991-2003
--
Pepin et al. CMAJ 2004;171:466-72
Epidemic C. difficile strain
• PFGE type NAP1; PCR ribotype 027
• Increased/prolonged toxin production
– tcdC - 18 bp deletion
• Most produce binary toxin
• Quinolone resistant
• Increased sporulation
• Spread widely in USA, Canada & UK

Risks for CDI (mainly 027)
Cohort study; inpatients 2003-4
• 7421 episodes of care; 5619 patients
• 293 CDI episodes
Risk factors: (adjusted hazards ratio; AHR)
• Increasing age (1.04 per year)
• Prolonged hospital stay (3-5)
• Quinolone Rx, incl. cipro. (3.44)
• BS β lactams; azithro, clinda (1.6-1.9)
• Longer duration of antibiotic Rx
Not significant: Use of PPIs; recent surgery
Pepin et al. CID 2005;41:1254-60
Is C. difficile 027 controllable?
• 2003-5 UK - serious hospital outbreaks
• 2004: mandatory hospital reporting
• 2004-7 steady increase in rates – x4 incr. in “CDI” on death certificate
• 2007: enhanced surveillance; ribotyping
• 2008: 29% decr. “CDI” deaths
• 2008-9: CDI rates falling – 19% fall in 027 (from 36% in 2007-8)
Freeman et al Clin Microbiol Rev 2010;23:529-49

Is C. difficile 027 controllable?
UK mandatory CDI reporting (www.hpa.org.uk
Is C. difficile 027 inevitable?
• European CDI hospital surveys:
– 2005: 2.45 (0.13-7.1)/10,000 patient days
– 2008: 5.5 (0-36) per 10,000 pd
• (106 hospitals; 34 countries)
• 395 isolates: 62 PCR ribotypes
– 014 (15%), 001 (10%), 078 (8%) 027 (5%)
• 80% hospital acquired; 79% antibiotics
• 7% ICU; ~9% attributable mortality
*Freeman et al Clin Microbiol Rev 2010;23:529-49
C. difficile in Australia • No evidence of increased incidence
– BUT - minimal surveillance;
– Variable diagnostic testing
• Various genotypes
– BUT – limited culture/typing of isolates
– 1 case of 027 in 2008 (imported)
– At least 7 027 cases in 2010 in Victoria
• Epworth Hospital & LTCF
• Fluoroquinolone res. rare (1-2%)
• Mandatory reporting – coming soon

Community-acquired (CA) CDI
• Not well recognised but not new:
• 1990s - CA CDI = 11-28% of CDI cases
• UK – GP-based study 1994-2004– CA-CDI– increased from 0 to 18/100,000
• Risk factors: hospital admission 2-6m ago
– 50% no antibiotics;
– 1/3 no antibiotics or hospital admission
– Younger patients (vs HA CDI)
• ?Recent increase (with 027) ?recognition

CDI in animals
• Various studies:– 10% dogs; 2-20% cats
– 40% calves with diarrhoea; 21% controls
• Various ribotypes – rarely 027– 078 found in piglets & calves (& humans)
• C. difficile isolates from meat (esp. 078)– no evidence of food-borne disease
• 078 – virulent– tcdC deletion & mutation; binary toxin +ve

Antibiotic use as risk factor
• Most frequently
– Broad spectrum (cephs; clindamycin - any)
– Fluoroquinolone use – esp. 027 (OR ~13)
– Prolonged use; combinations
• CDI rates reduced by restricting:– Use of high risk antibiotics
– (Duration of antibiotic Rx & combinations)
• e.g. IV penicillin for pneumonia;• Especially in the elderly
– Single dose/ <24 hr surgical prophylaxis
Summary
• Limited penetration of virulent strains in Australia so far (probably)
• Need to be prepared– Laboratory testing; typing; surveillance
• Can be prevented/controlled by– Continued improvement in
• Hand hygiene
• Patient isolation; contact precautions
• Environmental cleaning
• Antibiotic stewardship


C. difficile diagnosis in NSW*
• 13 labs surveyed - private and public
• 5 - GDH (+toxin tests) +/or PCR
• 7 toxin A/B EIA; 1 toxin A only
• 7 culture C. difficile
– 2 submit cultures for typing
• Of all stools submitted:
– 31% (11-61%) tested for C. difficile
– Of tested stools, 6.2% (3.3-10%) +ve
*John Ferguson, personal communication
Risks for complicated CDI (027)
• Definition:
– Megacolon, perforation, colectomy, shock
requiring vasopressors, +/or death within 30d
• Significant risk factors (adj. OR; p value)
– Age >65 yrs (3.4; <0.05)
– Hospital acquisition (4.6; <0.001)
– Tube feeding, 2 m (2.4; <0.001)
– Immunosuppression (2.3; <0.001)
– Leucocytosis – wcc >20 (3.8; <0.001);
– Renal failure - creat >200 (4.1; <0.001)
– Rx vanc vs metr (0.2; p=0.02)
Pepin et al. CMAJ 2004;171:466-72
Prevalence of CDI
• Limited, inconsistent surveillance
• Varied testing indications & methods
• Varied case definitions, denominators
• Europe 2004:
– Hospital incidence: 2.45 (0.13-7.1) per
10,000 patient days
• USA, Canada, UK: 2000-2005:
– increased rates/complications/deaths
--
Freeman et al Clin Microbiol Rev 2010;23:529-49





























