Embed Size (px)
Citation preview

Gut, 1986, 27, 1219-1222
Case report
Eosinophilic gastroenteritis presenting in anadolescent with isolated colonic involvementD MOORE, S LICHTMAN, J LENTZ, D STRINGER AND P SHERMANFrom the Division of Gastroenterology, Departments of Pediatrics, Pathology, and Radiology, The Hospitalfor Sick Children, University of Toronto, Toronto, Ontario, Canada.
SUMMARY Eosinophilic gastroenteritis most commonly involves the stomach and proximal smallintestine with eosinophilic inflammation of either the mucosa, submucosa or serosa. The patientreported here had isolated eosinophilic colitis. The initial presentation with iron deficiencyanaemia owing to occult gastrointestinal blood loss emphasises the need to evaluate the entiregastrointestinal tract in patients with eosinophilic gastroenteritis.
Eosinophilic infiltration of colonic mucosa can occuras a component of the inflammatory response inCrohn's disease, idiopathic ulcerative colitis,amoebic dysentery and milk protein induced colitis. 'In addition, tissue eosinophilia develops in eosino-philic gastroenteritis which is an uncommon dis-order of unknown aetiology that is typically associ-ated with peripheral eosinophilia, abdominal pain,nausea, vomiting, and diarrhoea.2 In eosinophilicgatroenteritis mucosal infiltration of eosinophilils ismost commonly limited to the antrum of thestomach and the proximal small bowel.3 We report acase of eosinophilic infiltration limited to the colonin a 17 year old boy who presented with irondeficiency anaemia.
Case report
A 17 year old white boy was referred for evaluationof iron deficiency anaemia. He complained oflethargy and reduced exercise tolerance but initiallydid not have gastrointestinal symptoms. There wasno history of weight loss, change in appetite, and heate a normal diet containing meat. He took aspirininfrequently for migraine headaches but had nottaken any other medication. There was a past
Address for correspondence: Dr P Sherman, Division of Gastroenterology,Department of Pediatrics, The Hospital for Sick Children, 555 UniversityAvenue, Toronto, Ontario, Canada MSG 1XX.Received for publication 4 February 1986.
history of infantile eczema and childhood asthma,but there was no history of specific food allergies.The family history was negative for inflammatorybowel diseases, coeliac disease and colonic poly-posis.On examination, he appeared pale but there was
no evidence of jaundice, digital clubbing, or perioralpigmentation. Abdominal examination did not re-veal hepatosplenomegaly, abdominal tenderness ormasses and there was no evidence of perianaldisease. The rectal examination was normal andleucocytes were not seen on stool microscopy. Thestool was positive, however, for occult blood(Hematest tablet, Ames).
Laboratory investigations included: Hb 106 g/l,MCV 70 fl, MCHC 303 g/dl, platelets 264x109/1,ESR 6 mm/h, WCC 5 8x109/1, eosinophilils0-58x109/1, serum ferritin 3.4 [tg/l (16-300 [tg/l),serum iron 3 [tmoUl (9-27 [tmol/l), TIBC 72 [tmol/l(45-72 [tmol/l), a normal haemoglobin elec-trophoresis, total protein 69 g/l and albumin 42 g/l.Serum antibody titres to Yersinia enterocolitica andEntamoeba histolytica were negative. Repeatedstool examinations were negative for known viral,bacterial, and parasitic enteric pathogens. Chestradiograph, electrocardiogram, and liver functiontests were normal. A Schillings test with intrinsicfactor was normal. Skin testing for possible allergicreactions to multiple inhalent and food antigenswere negative. Serum IgE concentrations werenormal. Radiologic investigations included a normal
1219
on May 14, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.27.10.1219 on 1 O
ctober 1986. Dow
nloaded from

Moore, Liclitunan, Leitz .SStringcr, and1b Slieritnani
barium study of the oesophagus, stomach, and smallbowel, and a normal ""9'Technetium-pertechnetatescan. Panendoscopy of the oesophagus, stomachand proximal duodenum was normal. Suctionbiopsies which were obtained from both the antrumand the proximal jejunum (Carey capsule. PreciseProducts Corp, USA) were histologically normal.After the subsequent onset of haemratochezia a99mTc labelled red blood cell scan was carried out.4The study indicated either blood loss or hyperaemiain the region of the transverse colon. A double
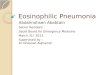
contrast barium enema showed mild mucosalirregularity in the distal transverse colon (Fig. 1).
Fibreoptic colonoscopy revealed an erythema-tous, granular and friable mucosa with changes mostmarked in the transverse colon. Biopsies of colonicmucosa showed an intense inflammatory infiltratewithin the lamina propria which was composedprimarily of eosinophils (Fig. 2). Mast cell numberswere not increased in the lamina propria of biopsyspecimens, and no microgranulomata or giant cellswere identified.
Fig. I Double contrast bariiui etion(a oftheidi.stal .sWrlemnI of tranosverse colon. The mnucosal pfaiierii appear.sirregu,lar (arrows).
1220
on May 14, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.27.10.1219 on 1 O
ctober 1986. Dow
nloaded from

Eosinophilic gastroenteritis presetititg iflinan adolescentt withl isOllted (OlOnlic in vol vemenlt
Six weeks later the patient was on prednisone(60 mg/day) and was completely asymptomatic andstools were negative for occult blood. The Ilb was165 g/l and the peripheral eosinophilia had resolved.After prednisone waIs discontinued he again de-veloped increased stool frequency aind haemato-chezia. Although the stools did not contain leuco-cytes or eosinophils (the latter evaluated after
Wright's stain), many Charcot-Leyden crystals werenoted. A peripheral eosinophilia was again noted(0(88x 109/1). Colonic biopsies revealed continuedmarked eosinophilic infiltration within the laminapropria.
Subsequently, he was started on ketotifen(2 mg/day) with symptomatic improvement andresolution of the peripheral eosinophilia. After
Fig. 2 Photomicrograph of a colonic biops5 which shows an inflamninatory infiltrate within the lamina propria.The infiltrate consists of eosinophil.y which are indicated by arrowheads (haemratoxsvlin and eosin).
1221
on May 14, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.27.10.1219 on 1 O
ctober 1986. Dow
nloaded from

1222 Moore, Lichtman, Lentz, Stringer, and Sherman
discontinuing ketotifen on two separate occasionsenteric blood losses and peripheral eosinophiliawere again noted which resolved after reintroductionof ketotifen.
Discussion
The unusual aspects of this case, in contrast with themore typical presentation of eosinophilic gastroen-teritis, are localisation of eosinophilic infiltrationexclusively in the colon and the initial presentationwith iron deficiency anaemia carried by occultgastrointestinal blood losses. The diagnosis ofeosinophilic colitis in our patient was based on thepresence of an extensive infiltrate of eosinophils inmultiple colonic biopsies in the presence ofperipheral eosinophilia. Interestingly, localisation ofpathology to the colon was first suggested by themTc labelled red blood cell scan. Subsequently,
colitis was confirmed by both colonoscopy andcolonic biopsies, whereas the changes noted ondouble contrast barium enema were subtle.
Eosinophilic infiltration of the gastrointestinaltract is seen in other gastrointestinal disorders suchas inflammatory bowel diseases, peptic ulcer dis-eases, granulomatous polyps, amoebiasis and otherenteroinvasive parasites, milk protein induced col-itis and the systemic hypereosinophilic syndromes.'Each of these conditions has been adequatelyexcluded in our patient.There are no standard criteria for assessing tissue
eosinophilia. Using the method previously describedby Tedesco et al,5 however, we determined thenumber of eosinophils which were present in colonicbiopsies that had been obtained from our patient.As shown in the Table, our patient had a pro-nounced infiltration of eosinophils within the col-onic mucosa compared with colonic biopsies whichhad been obtained from adolescents with Crohn's
Table Number of eosinophils per high poweredfield (HPF) in colonic biopsy specimens, X±SD. Numbersin parentheses indicate the range of eosinophils presentwithin 5 HPF counted for each subject. Five separatecolonic biopsies were reviewed for the patient reported
Pathology n EosinophilslHPF
Patient 1 60(8±8-6 (46-75)Normal 4 6-3±4-1 (1-14)Crohn's 4 7 6±6.7 (W-18)Polyposis coli 3 12-5±8+3 (3-28)
colitis, familial polyposis coli and from teenagerswith normal colonic histology. The degree of eosi-nophilic infiltration is the same as described byTedesco in an adult with eosinophilic ileocolitis.Tissue eosinophil counts in colonic and rectalbiopsies may prove to be a valuable method formonitoring the clinical course of such patients.
Eosinophilic gastroenteritis can affect the colon inaddition to the stomach and small intestine butisolated colonic involvement appears to be quiterare.6 We suggest that patients with eosinophilicgastroenteritis involving the stomach and smallbowel should have an assessment of possible colonicinvolvement.Although the role of allergic mechanisms in the
pathogenesis of eosinophilic gastroenteritis is con-troversial, therapy with oral sodium cromoglycatehas been attempted.7 x We report an apparentclinical response using ketotifen in the treatment ofeosinophilic colitis. Ketotifen is a benzocyclo-heptathiophene derivative which has been used inthe place of sodium cromoglycate for the treatmentof severe asthma.9 The improvement of our patienton ketotifen therapy is interesting but may, ofcourse, represent coincident spontaneous improve-ment of the colitis.
References1 Tavassoli M. Eosinophil. eosinophilia and eosinophilic
disorders. CRC Crit Rev, Clini Lab Sci 1981; 16: 35-83.2 Klein NC, Hargrove RI, Sleisenger MH, Jeffries GH.
Eosinophilic gastroenteritis. Medicine 1970; 49:299-3 19.
3 Katz AJ, Goldman H, Grand RJ. Gastric mucosalbiopsy in eosinophilic (allergic) gastroenteritis. Gas-troenterology 1977; 73: 705-9.
4 Winzelberg GG, Froelich JW, McKusick KA, StraussHW. Scintigraphic detection of gastrointestinal bleed-ing. A review of current methods. Am J Gastroenterol1983; 78: 324-7.
5 Tedesco FJ, Huckaby CB, Hamby-Allen M, EwingGC. Eosinophilic ileocolitis. Dig Dis Sci 1981; 26:943-8.
6 Naylor AR, Pollet JE. Eosinophilic colitis. Dis Colo,iRectum 1985; 28: 615-8.
7 Keshavarzian A, Saverymuttu SH. Tai PC et al.Activated eosinophils in familial eosinophilic gastroen-teritis. Gastroenterology 1985; 88: 1041-9.
8 Heatley RV, Harris A, Atkinson M. Treatment of apatient with clinical features of eosinophilic gastroen-teritis and polyarteritis nodosa with oral sodiumcromoglycate. Dig Dis Sci 1980; 25: 470-2.
9 MacDonald GF. An overview of ketotifen. Chest 1982;82: 303-25.
on May 14, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.27.10.1219 on 1 O
ctober 1986. Dow
nloaded from