Embed Size (px)
Citation preview

Enrico MiniDepartment of Pharmacology
University of Florence
Second primary cancer as late effect of cancer treatment

Introduction (I)
• Of the many late complications of treatment, second cancers are generally considered to be the most serious, not only for substantial morbidity but also for considerable mortality.
• Increased risks of second cancers have been observed after radiotherapy, chemotherapy, and combined modality treatment.
• Not all second cancers are due to therapy.

Schematic illustration of risk factors for second primary cancers
Travis LB, Acta Oncologica 41:323-333, 2002

Introduction (II)• In view of the high prevalence of cancer in the general
population and the increasing incidence of most cancers with age, it is important to exclude the role of chance in the development of second cancers.
• To this end, comparison with cancer incidence statistics derived from the general population is crucial.
• If a second malignancy is demonstrated to occur in excess, the contributions of other risk factors need to be ruled out convincingly before the increased risk can be attributed to treatment.
• The evaluation of the carcinogenic effects of therapy, however, is complicated by the fact that therapeutic agents are frequently given in combination.
• Appropriate epidemiologic and statistical methods are required to quantify the excess risk and to unravel the role of treatment and other factors.

Data sources to assess second cancer risk
• Population-based cancer registries• Hospital-based cancer registries• Clinical trial series• Epidemiologic study designs: – cohort studies– case-control studies.

Carcinogenicity of antineoplastic agents and their combinations
Group 1 – Drugs which are carcinogenic (sufficient human evidence of carcinogenesis)
• Busulfan• Chlorambucil• Cyclophosphamide• Melphalan • Semustine (Methyl-CCNU)• Thiotepa • Treosulphan • MOPP-combination therapy • Etoposide in combination with cisplatin and
bleomycin• Etoposide • Azathioprine • Methoxsalen, plus UV radiation• Tamoxifen• DiethylstilbestrolGroup 2A – Drugs which are probably
carcinogenic to humans (generally, limited human evidence, but sufficient animal evidence)
• Carmustine (BCNU) • Cisplatin• Doxorubicin• Lomustine (CCNU) • Mechlorethamine • Procarbazine • Teniposide
Group 2B – Drugs which are possibly carcinogenic to humans (generally, limited human evidence, but absence of animal evidence)
• Bleomycin • Dacarbazine• Daunorubicin • Medroxyprogesterone acetate• Mitomycin • Mitoxantrone • StreptozocinGroup 3 – Drugs which are not classifiable
as to its carcinogenicity to humans • Actinomycin D • 5-Fluorouracil • Metotrexate • Prednisone • Vinca alkaloids
IARC, 2011

Antineoplastic drugs and other drugs evaluated by the IARC Monograph Working Group (I)
Grosse Y et al., Lancet Oncol 10:13-14, 2009

Antineoplastic drugs and other drugs evaluated by the IARC Monograph Working Group (II)
Grosse Y et al., Lancet Oncol 10:13-14, 2009

Hormonal treatments assessed by the IARC Monograph Working Group
Grosse Y et al., Lancet Oncol 10:13-14, 2009

Therapy-related neoplasms• Acute myeloid leukemia (up to 10-20% of all AML cases)
• Other treatment-related leukemias:– ALL (5-10% of all secondary acute leukemia)
– chronic granulocytic leukemia (a small percentage of secondary leukemia)
• Solid tumors:– bladder cancer (induced by cyclophosphamide)
– bone sarcomas (linked to alkylating agents)
– lung cancer (linked to alkylating agents)
– endometrial cancer (associated to tamoxifen)
– contribution of chemotherapy to radiation-induced solid tumors to be investigated (e.g. doxorubicin potentiates the development of second solid tumors after radiation for Wilms’ tumor)

Secondary acute myeloid leukemia
• At least two major syndromes of treatment-related leukemia exist:– "classic" alkylating agent–induced AML – acute leukemia related to the
topoisomerase II inhibitors

Characteristics of therapy-related acute myelogenous leukemia
(alkylator versus topoisomerase inhibitor related)
From Borthakur G & Estey EE, 2007, and Meadows AT, 2001, modified
Features Alkylator related Topoisomerase II inhibitor related
Latency period 2-8 years 1-3 years
Morphology (FAB classification) M1/M2 M4/M5
Preceding AHD/MDS Frequent Rare
Chromosomal abnormalities Deletion/long arm deletion 5, 7 11q23, 21q22 and 3q23 translocations
Prevalence 1 to >20% 2 to 12%
Survival Poor Poor
AHD—antecedent hematologic disorder; MDS—myelodysplastic syndrome

Occurrence of therapy-related acute myelogenous leukemia and myelodysplastic
syndrome following common exposures
Borthakur G & Estey EE, Curr Oncol Rep 9:373-377, 2007
Disease Exposure Frequency, %
Hodgkin disease [Pedersen-Bjergaard J, Larsen SO, 1982]
Chemotherapy ± radiation 9.9 +/- 2.9
Germ cell tumor [Pedersen-Bjergaard J, et al., 1991]
Cisplatin, etoposide, bleomycin 4.7
Acute lymphoblastic leukemia [Pedersen-Bjergaard J, Larsen SO, 1982]
Combination chemotherapy 4.7
Breast cancer [Linassier C, et al., 2000] Mitoxantrone, cyclophosphamide, and 5-fluorouracil
2.9
Non-Hodgkin lymphoma (reviewed in Hake et al., 2007)
ASCT 3 to 13
Indolent lymphoma [Lenz G et al., 2004] ASCT 3.8
Chronic lymphocytic leukemia [Milligan DW, et al., 2006]
ASCT 12.4
ASCT—autologous stem cell transplant.
Alkylating agent-induced AML• Alkylating agents with known leukemogenic effects in humans
include mechlorethamine, chlorambucil, cyclophosphamide, melphalan, semustine, lomustine (CCNU), carmustine (BCNU), prednimustine, busulfan, and dihydroxybusulfan.
• Controversial findings have been reported with regard to procarbazine, which demonstrates an underlying mechanism of action similar to that of alkylating agents.
• Few studies have addressed the relative leukemogenicity of the various alkylating drugs, but a strong body of evidence to date suggests that, at doses of equal therapeutic effect, cyclophosphamide is substantially less leukemogenic than melphalan, mechlorethamine, chlorambucil, CCNU, and thiotepa.
• The risk of alkylating agent–related AML has been shown to increase with increasing cumulative dose, duration of therapy, and dose-intensity.
• Few studies have attempted to separate the effects of cumulative dose, duration of treatment, and dose intensity, which tend to be highly correlated, and the results of such analyses have been controversial.

Distribution and relative risk of acute or nonlymphocytic leukemia according
to overall treatment category
Kaldor JM et al., N Engl J Med 322:7-13, 1990

Distribution of cases of acute nonlymphocytic leukemia according to
type of chemotherapy*
Kaldor JM et al., N Engl J Med 322:7-13, 1990
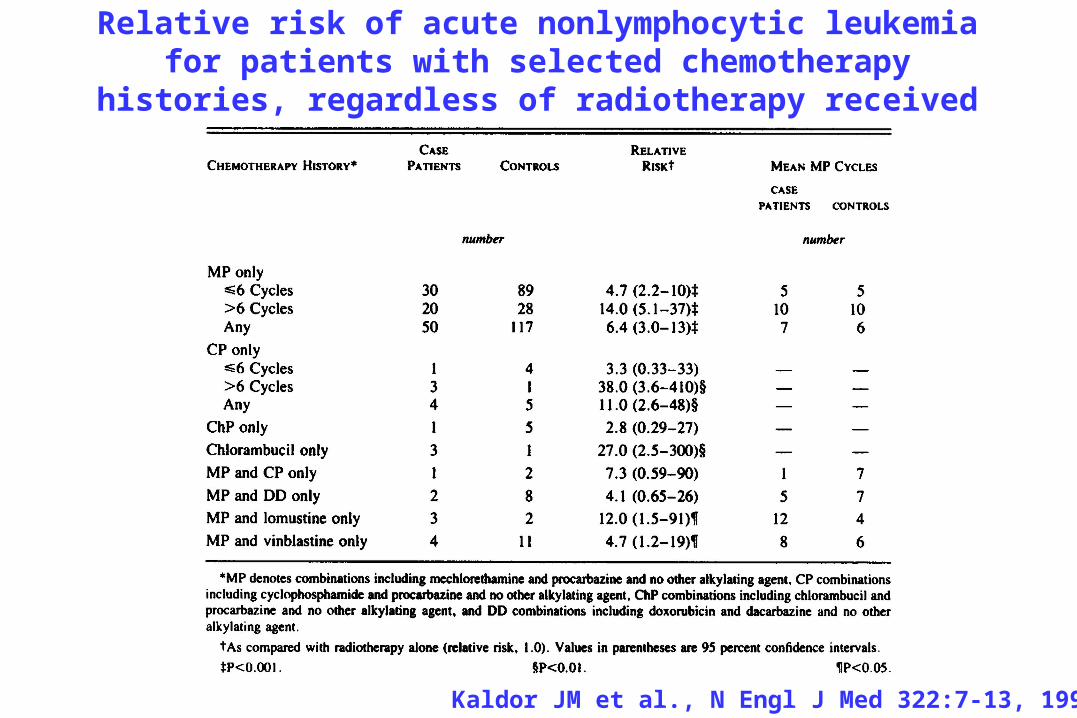
Relative risk of acute nonlymphocytic leukemia for patients with selected chemotherapy histories,
regardless of radiotherapy received
Kaldor JM et al., N Engl J Med 322:7-13, 1990

Risk factors for leukemia after Hodgkin’s disease
• Since the 1980s, MOPP-only chemotherapy has been gradually replaced by regimens containing doxorubicin, bleomycin, vinblastine, and dacarbazine (ABVD) in many centers.
• Patients treated with ABVD at the Milan Cancer Institute, where this regimen was designed, were shown to have a significantly lower risk of AML than MOPP-treated patients (15-year cumulative risks of 0.7% and 9.5%, respectively).
• Another study showed that HD patients treated with MOPP- and ABVD-containing regimens in the 1980s had substantially lower risk of AML and MDS than patients treated in the 1970s with MOPP alone (10-year cumulative risks of 2.1% and 6.4%, respectively; P = .07).
Valagussa P et al., 1982; Schellong G et al., 1997

Smith RE et al., J Clin Oncol 21:1195-1204, 2003

• There has been an increasing trend toward the use of dose-intensification strategies in chemotherapy protocols for breast cancer.
• Typically, these regimens contain high-dose cyclophosphamide in combination with one of the anthracyclines (doxorubicin or 4-epidoxorubicin) and other active drugs.
• The risk of AML associated with various AC regimens was quantified in six trials of the National Surgical Adjuvant Breast and Bowel Project (NSABP) (Smith RE et al, J Clin Oncol, 2003)
Secondary AML in breast cancer (II)

Cumulative incidence of acute myeloid leukemia/
myelodysplastic syndrome by cyclophosphamide intensity (mg/m2/cycle)
Smith RE et al., J Clin Oncol 21:1195-1204, 2003
AML/MDS, acute myeloid leukemia/myelodysplastic syndrome; TX, treatment

Secondary AML in breast cancer (I)• The low risk of AML after CMF-based chemotherapy was
confirmed by the Milan Cancer Institute and the Eastern Cooperative Oncology Group, who found cumulative risks of AML of 0.23% at 15 years and 0.18% at 7 years, respectively.
• The University of Texas M. D. Anderson Cancer Center reported a higher risk of leukemia after a standard dose-intensity FAC treatment.
• Fourteen cases of leukemia were observed among 1474 patients for an estimated cumulative risk of 1.5% (95% CI, 0.7 to 2.9) at 10 years.
• The risk of AML was significantly higher when chemotherapy was given in combination with radiotherapy (2.5% vs. 0.5%).
Valagussa P, et al, Ann Oncol 1994; Tallman MS et al., J Clin Oncol 1995; Diamandidou E et al., J Clin Oncol 1996

• The platinating agents cisplatin and carboplatin are among the most important cytotoxic drugs introduced in the last few decades and are widely used to treat many cancers.
• The platinum compounds, however, demonstrate carcinogenicity in vitro and in laboratory animals, forming intrastrand and interstrand DNA cross-links as do bifunctional alkylating agents.
• In a population-based study of women with ovarian cancer, cisplatin-based combination chemotherapy was linked to significantly increased risks of leukemia (P trend for cumulative dose, <.001) in a multivariate model adjusted for other treatment parameters.
• Future studies should evaluate whether other drug combinations that include platinum might also be linked to elevated risks of leukemia, because it is not clear whether cisplatin acts as a human leukemogen only in combination with selected cytotoxic agents
Platinating agent-induced AML

Risk of Leukemia According to the Cumulative Dose of Platinum, Duration of Therapy, and Specific Druga
Dose and Duration
No of Pts with Leukemia
No of Matched Control Pts
Median Value in Controlsb
Relative Risk (95% CI)c
All platinum drugs
Dosed <500 mg 4 30 418 mg 1.9 (0.5–7.9)500–749 mg 5 28 600 mg 2.1 (0.6–8.0)750–999 mg 7 25 896 mg 4.1 (1.1–14.8)>1000 mg 11 20 1230 mg 7.6 (2.3–
25.3)e Duration <6 mo 3 36 5.4 mo 1.2 (0.3–5.5)6–12 mo 16 49 8.5 mo 4.3 (1.4–12.9)>12 mo 8 18 14.2 mo 7.0 (1.8–
26.6)f Specific drug Cisplatin 19 85 600 mg 3.3 (1.1–9.4)Carboplatin 3 9 3300 mg 6.5 (1.2–36.6)Both 5 9 9.0 (2.2–37.6)Cisplatin 720 mg Carboplatin 2200 mg
aThe data are limited to 27 patients with leukemia and 103 controls who receive platinum-based chemotherapy without melphalan. bThe values shown are median cumulative doses of platinum and the median duration of therapy among controls. cThe reference group consisted of 6 patients with leukemia and 94 controls who were not exposed to platinum derivatives of other alkylating drugs. dCumulative amounts of carboplatin were divided by 4 to convert them to cisplatin-equivalent doses. e for trend <.001. f for trend = .001. (From Travis LB, et al. N Engl J Med 1999;340(5):351., with permission.)
From van Leeuwen FE & Travis LB, 2005

Plasma platinum concentrations of 61 cured testicular cancer patients 10–20 years after cisplatin combination chemotherapy
and 20 cured testicular cancer patients 10–20 years after orchidectomy
Gietema JA et al., Lancet 355:1075-6, 2000
Horizontal line=limit of quantification of platinum (6 pg/g plasma).

Concentration-time plot of plasma platinumconcentrations of 61 cured testicular-cancer
patients 10–20years after cisplatin combination chemotherapy
Gietema JA et al., Lancet 355:1075-6, 2000

Topoisomerase II inhibitors-related AML
• Ratain and coworkers (1987) were the first to recognize the potentially leukemogenic properties of etoposide-containing regimens in patients with non–small cell lung cancer, and this has also been documented for patients with other types of malignancies.

Acute leukemia related to epipodophillotoxins
• Use of etoposide and cisplatin to treat testicular cancer has been linked to increased risks of leukemia in relatively small studies, typically at large total amounts of etoposide (3000 mg/m2 or more).
• Considerably lower total doses of etoposide were administered in the case-control investigation reported by Travis et al., (2000) similar to the dose of less than 2000 mg/m2 used in current regimens.
• The IARC concluded that there is sufficient evidence that etoposide in combination with cisplatin and bleomycin is carcinogenic to humans.
• The overall level of risk, however, appears relatively low.
• Based on a review of selected U.S. clinical trials, Smith et al. (1999) estimated that the 6-year cumulative risk of secondary leukemia is 0.7% after cumulative etoposide doses of 1500 to 2999 mg/m2.
• Kollmannsberger et al. (1999) concluded that the cumulative incidence of leukemia among testicular cancer patients given etoposide at cumulative doses of 2000 mg/m2 or less and more than 2000 mg/m2 was 0.5% and 2.0%, respectively, at a median of 5 years of follow-up.

Secondary leukemias following chemotherapy of testicular cancer contaning cumulative etoposide
doses <2 g/m2
Number of secondary leukemias
No of pts Total Etoposide-related
Median follow-up (years)
References
636 4 3 5.7 Boshoff et al., 1995
538 2 2 4.9 Nichols et al., 1993
343 2 1 ≥5 Bajorin et al., 1993
221 1 1 5.5 Bokemeyer & Schmoll, 1993
130 0 0 5.4 Pedersen-Bejergaard et al., 1991
1868 9 (0.5%) 7 (0.4%) 5
Bokemeyer C & Kollmannsberger C, “Secondary Malignances” in Lipp HP ed, 1999

Secondary leukemias following chemotherapy for testicular cancer
contaning cumulative etoposide doses ≥2 g/m2
Number of secondary leukemias
No of patients Total Etoposide-related
Median follow-up (years)
References
82 5 4 5.4 Bokemeyer & Schmoll, 1993
25 2 2 5.7 Boshoff et al., 1995
128 1 1 4.5 Bokemeyer et al., 1995
302 6 4 5 Kollmannsberger et al., 1998
537 14 (2.6%) 11 (2.0%) 5
Bokemeyer C & Kollmannsberger C, “Secondary Malignances” in Lipp HP ed, 1999

AML-related to anthracyclines• Evidence has accumulated that the anthracyclines doxorubicin and
4-epidoxorubicin may induce a similar type of AML as the one related to epipodophyllotoxin treatment.
• According to the IARC, doxorobicin is probably carcinogenic to humans.
• An evaluation of the carcinogenic potential of doxorubicin is complicated, because it is typically given in combination with other chemotherapeutic agents, including alkylators.
• Curtis et al. (1992) found no increase in the risk of leukemia associated with doxorubicin therapy for breast cancer after adjustment for the effects of alkylating agents and radiotherapy.
• Although an increase in the dose of doxorubicin given to treat childhood cancer seemed weakly associated with an increased risk of leukemia after adjustment for use of alkylating agents, the investigators concluded that the excess risk was almost completely attributable to alkylators (Tucker MA, 1987).
• In a study of children with Wilms' tumor, the RR of leukemia (six cases) after doxorubicin-containing regimens was approximately 14; however, because a relatively constant dose of doxorubicin (300 mg/m2) was used and data on treatment of relapse were incomplete, evaluation of a dose-response relation was not possible (Breslow NE, 1995).

• The antimetabolites have generally not been regarded as carcinogenic.
• Cheson et al. (1999) observed that nucleoside analogue therapy (fludarabine, deoxycoformycin, cladribine) for chronic lymphocytic leukemia did not appear to confer a significantly increased risk of second cancer.
• However, in a report from St. Jude Children's Research Hospital (Relling et al., 1999), it was shown that children with ALL who received cranial irradiation and who had a wild-type thiopurine methyltransferase phenotype had an 8.3% cumulative risk of brain cancer, whereas children with ALL who received irradiation and had a defective phenotype had a 42% risk (P = .0077).
• Patients also received concurrent systemic chemotherapy with high-dose 6-mercaptopurine (75 mg/m2) plus high-dose methotrexate.
• It was hypothesized that the defective thiopurine methyltransferase activity resulted in higher exposures to thioguanine nucleotide metabolites of 6-mercaptopurine during the period of irradiation.
Antimetabolites and carcinogenic risk
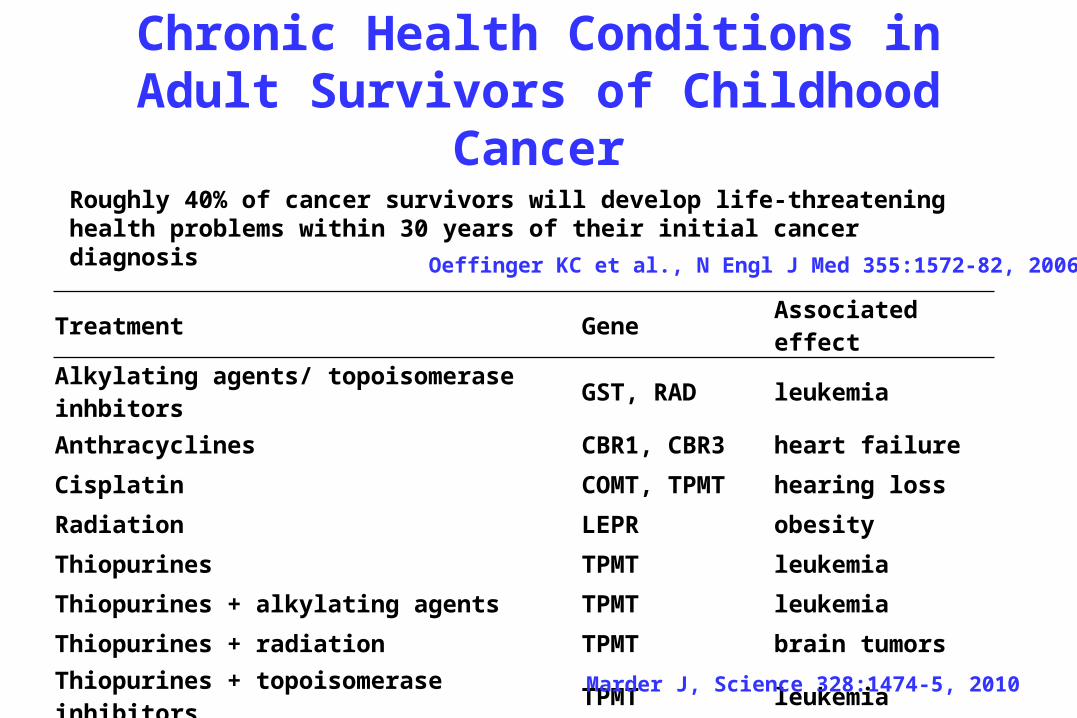
Chronic Health Conditions in Adult Survivors of Childhood Cancer
Treatment Gene Associated effect
Alkylating agents/ topoisomerase inhbitors GST, RAD leukemia
Anthracyclines CBR1, CBR3 heart failure
Cisplatin COMT, TPMT hearing loss
Radiation LEPR obesity
Thiopurines TPMT leukemia
Thiopurines + alkylating agents TPMT leukemia
Thiopurines + radiation TPMT brain tumors Thiopurines + topoisomerase inhibitors TPMT leukemia Marder J, Science 328:1474-5, 2010
Roughly 40% of cancer survivors will develop life-threatening health problems within 30 years of their initial cancer diagnosis
Oeffinger KC et al., N Engl J Med 355:1572-82, 2006

Risk of Bladder Cancer According to Cumulative Dose and Duration of Cyclophosphamide Therapy
Cyclophosphamide
Median Dose or
Durationa
Cases (n) Controls (n) Matched Relative
Riskb
95% CI
Cumulative dose
<20 gc 10.0 g 8 22 2.4 0.7–8.4
20–49 g 34.0 g 5 6 6.3d 1.3–29.0
50 g 87.7 g 5 2 14.5d,e 2.3–94.0
Duration of therapy
<1 y 6 mo 8 20 2.5 0.7–9.0
1–2 y 18 mo 3 6 3.7 0.6–22.0
>2 y 51 mo 7 4 11.8d,e 2.3–61.0aMedian cumulative dose of cyclophosphamide or median duration of therapy among all patients within the specified category. bThe referent group consists of 6 case subjects and 42 control subjects who were not treated with cyclophosphamide and who received a radiation dose to the bladder of 0.5 Gy or less. The multivariate model also included terms for patients who received radiotherapy without cyclophosphamide (6 case subjects and 16 control subjects). cThe minimum cumulative dose of cyclophosphamide in this group was 2.1 g. d <.05. e for trend <.005. (From Travis LB, et al. J Natl Cancer Inst 1995;87:524 , with permission.)
From van Leeuwen FE & Travis LB, 2005

Risk of bladder cancer according to cumulative dose and duration of
cyclophosphamide and administration of radiotherapy
Travis LB et al., J National Cancer Inst 87:524-530, 1995


Relative risk and absolute excess risk of second malignant disease in 32,591
patients treated for Hodgkin’s lymphoma
Lorigan P et al., Lancet Oncol 6: 773–79, 2005
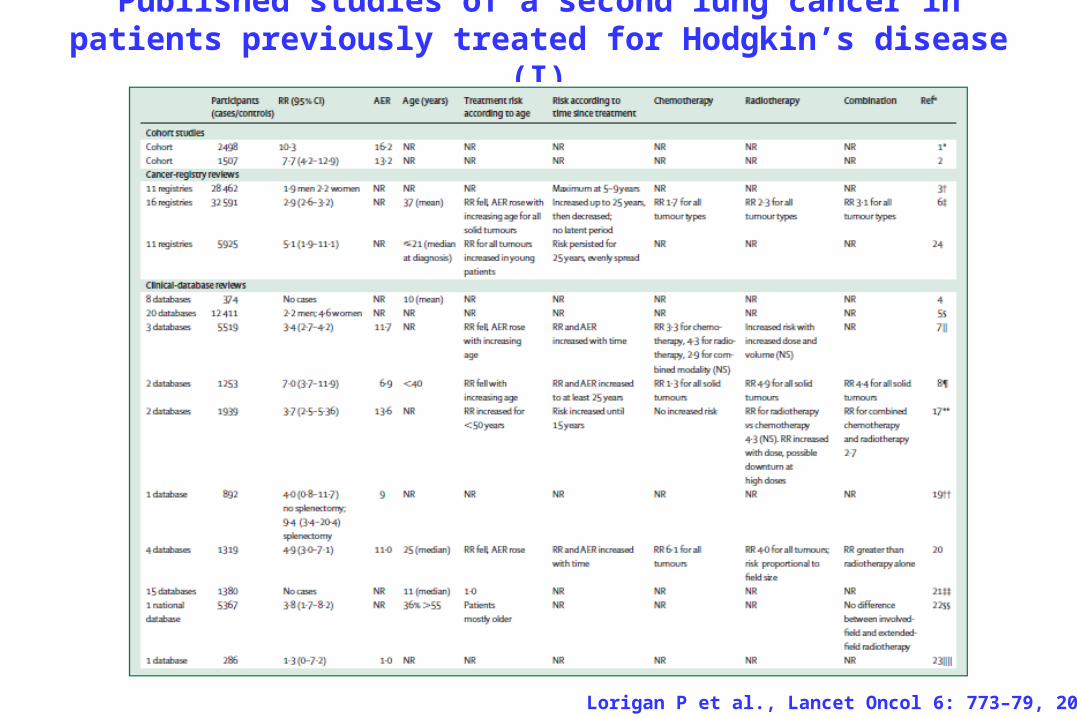
Published studies of a second lung cancer in patients previously treated for Hodgkin’s disease (I)
Lorigan P et al., Lancet Oncol 6: 773–79, 2005

Published studies of a second lung cancer in patients previously treated for Hodgkin’s disease
(II)
Lorigan P et al., Lancet Oncol 6: 773–79, 2005

Relative risk and absolute excess risk of a second lung cancer by age at first treatment
(years) in 5519 patients treated for Hodgkin’s lymphoma
Lorigan P et al., Lancet Oncol 6: 773–79, 2005

Relative risk and absolute excess risk of subsequent lung cancer by time since
treatment (years) in 5519 patients treated for Hodgkin’s lymphoma
Lorigan P et al., Lancet Oncol 6: 773–79, 2005

Relation between radiation dose, treatment with alkylating drugs, and cigarette smoking on relative risk of lung cancer in 222 patients with lung cancer
after treatment for Hodgkin’s disease
Lorigan P et al., Lancet Oncol 6: 773–79, 2005

Effects of SERMs and Aromatase Inhibitors on Nonbreast Tissue
Hayes DF, New Engl J Med, 2007
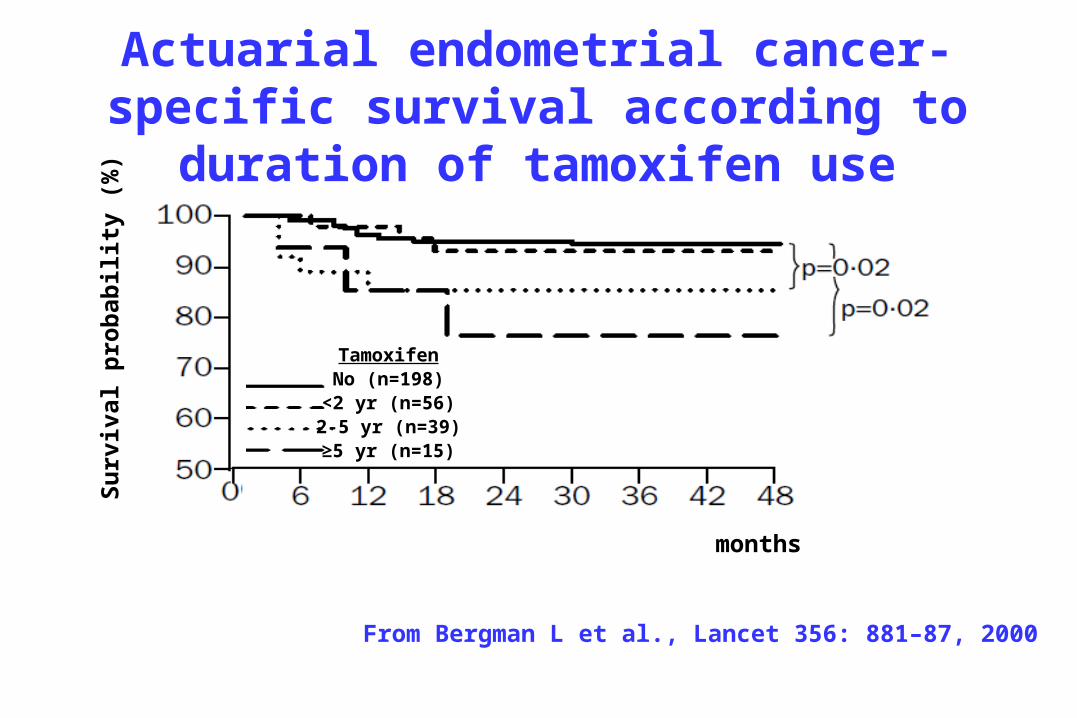
Actuarial endometrial cancer-specific survival according to
duration of tamoxifen use
months
Surv
ival
pro
babi
lity
(%)
TamoxifenNo (n=198)<2 yr (n=56)2-5 yr (n=39)≥5 yr (n=15)
From Bergman L et al., Lancet 356: 881–87, 2000

Risk of Endometrial Cancer after Tamoxifen Therapy in Women with Breast Cancer
Studya and Design No. of Breast Cancers
No. of Endometrial Cancers (No. in Tamoxifen Users)
Dose Evaluated
Duration of Tamoxifen Use
Relative Risk (95% of CIl)
Fisher et al., 1994; clinical trials
4063 24 (23) 20 mg Planned: 5 y Tamoxifen vs. control: 7.5 (1.7–32.7)
Tamoxifen vs. general population: 2.2b
Tamoxifen vs. control other trial: 2.3b
Rutqvist et al., 1995; clinical trial
4914 42 (34) 30–40 mg 48 wk–5 y Any: 4.1 (1.9–8.9)
EBCTCG, 1998; clinical trials
36,689 124 (92) Mostly 20 mg 1, 2, or 5 y Ever use: 2.6 (2.2–2.9)
Fisher et al., 1998; prevention trial
13,388 51 (36) 20 mg 1–5 y 5 Y: 4.2 (P <.001)
Any: 2.5 (1.4–5.0)Curtis et al., 1996; cohort (SEER based)
87,323 457 (73) Unknown Unknown Any tamoxifen vs. general population: 2.0 (1.6–2.6)
No tamoxifen vs. general population: 1.2 (1.1–1.4)
Mignotte et al., 1998; case control
NA 135 (91) 20–40 mg Varied Ever use: 3.1 (1.1–8.7)
5 Y: 10.7 (3.4–34.0) Trend with duration: P = .0001 Bernstein et al., 1999; case control
NA 324 (146) Mostly 20 mg Varied Ever use: 1.5 (1.1–2.2)
5 Y: 4.1 (1.7–9.5) Trend with duration: P = .0002 Bergman et al., 2000; case control
NA 299 (108) 20–40 mg Varied Ever use: 1.5 (1.1–2.0)
5 Y: 6.6 (2.2–19.7) Trend with duration: P <.001
EBCTCG, Early Breast Cancer Trialists' Collaborative Group; NA, not available; SEER, Surveillance, Epidemiology, and End Results program. aSeveral early reports are not presented because the dates are included in larger or updated studies presented here.bBecause the incidence of endometrial cancer appeared to be unexpectedly low among placebo-treated women, the investigators reestimated the risk associated with tamoxifen, using population-based rates and information from another trial. However, the resulting risk estimates of 2.2 and 2.3, respectively, are less valid than the estimate based on the endometrial cancer rate in placebo-allocated controls (relative risk, 7.5) because (a) regardless of treatment, a population of breast cancer patients entered into a clinical trial may have different endometrial cancer rates than the general population; and (b) the rates used were from a different geographic area, a different period, or both. 183 (Adapted from ref. 137.) From van Leeuwen FE & Travis LB, 2005

Forest plots of odds ratios for adverse events in endometrial carcinoma
Amir E et al., J Natl Cancer Inst 103:1299-1309, 2011
ATAC = Anastrozole, Tamoxifen alone or in combination (5); BIG 1-98 = Breast International Group 01-98 (3); ABCSG8 = Austrian Breast Cancer Study Group VIII (4); ITA = Italian Tamoxifen Anastrozole Trial (2); TEAM = Tamoxifen Exemestane Adjuvant Multinational Trial (15); AI = aromatase inhibitor; CI = confidence interval; OR = odds ratio.

Conclusions• Knowledge of risk factors for second malignancy has made it possible to identify
patient groups at high risk of developing second cancers due to treatments that they received in the past.
• Whenever effective screening methods are available, these should be implemented in the patients' follow-up program to improve their survival after diagnosis of second malignancy.
• The issue of treatment-induced second cancers must always be viewed in relation to the sometimes dramatic improvement in survival rates for patients with various malignancies.
• Clinical research should focus on the development of therapeutic regimens with less carcinogenic potential.
• It is of the utmost importance that changes in therapy to reduce the risk of late complications be made only in the context of carefully designed clinical trials that evaluate whether the overall efficacy of treatment is maintained.
• For many cancer treatments, the long-term effects on second malignancy risk are not yet known.
• In addition, new therapies are being introduced continuously, and the associated risks of late sequelae need to be evaluated.
• Results of investigations at the molecular level may clarify the influence of genetic susceptibility on treatment-related risk and contribute importantly to the elucidation of mechanisms underlying drug- and radiation-induced carcinogenesis.











![Enrico Fermi in Florence · Garbasso [Vercelli, Italy, April 16, 1871 – Florence, Italy, March 14, 1933] (Figure 3), renowned physicist, who studied with H. Hertz in Bonn and H](https://img.dokumen.tips/doc/110x75/5f7ba5c5e4a43003a247b4de/enrico-fermi-in-florence-garbasso-vercelli-italy-april-16-1871-a-florence.jpg)
















