Embed Size (px)
Citation preview

This article was downloaded by: [University of Glasgow]On: 19 December 2014, At: 07:23Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Reflective Practice: International andMultidisciplinary PerspectivesPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/crep20
Enhancing the empowerment agendain health promotion through reflectivepracticePaul Fleming aa University of Ulster , Northern IrelandPublished online: 12 Jul 2007.
To cite this article: Paul Fleming (2007) Enhancing the empowerment agenda in health promotionthrough reflective practice, Reflective Practice: International and Multidisciplinary Perspectives,8:3, 315-330, DOI: 10.1080/14623940701424827
To link to this article: http://dx.doi.org/10.1080/14623940701424827
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to orarising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Reflective PracticeVol. 8, No. 3, August 2007, pp. 315–330
ISSN 1462-3943 (print)/ISSN 1470-1103 (online)/07/030315–16© 2007 Taylor & FrancisDOI: 10.1080/14623940701424827
Enhancing the empowerment agenda in health promotion through reflective practicePaul Fleming*University of Ulster, Northern IrelandTaylor and Francis LtdCREP_A_242366.sgm10.1080/14623940701424827Reflective Practice1462-3943 (print)/1470-1103 (online)Original Article2007Taylor & Francis83000000August [email protected]
The formal practice of reflection is a relatively unknown concept in health promotion. A reflexiveapproach to health promotion practice normally resides in debates regarding the theory and practiceof health promotion; there have been few formal attempts to develop reflective practice. This paperdescribes a conceptual typology for reflective practice which focuses on three domains relating tothe role of self, the context of practice and the process of programme planning and delivery. Thesedomains are interrogated by a taxonomy of reflective questions tailored to the requirements andtiming of the reflection. An exemplar reflective application of the typology in this paper focused onthe evaluation of the smoking policy in a large university. Reflection centred on how the empower-ment of those working and studying in the institution was affected by the evaluation process.
Health promotion, the empowerment agenda and reflection
Reflective practice has become established in a range of professional areas in health,not least in nursing and the allied health professions (Glen et al., 1995; Tate & Sills,2004). The discipline of health promotion has, however, remained largely untouchedby the move towards embracing more formal reflective practice. A review of theliterature reveals that, apart from Issitt (2003), little had been written specificallyregarding reflective practice and health promotion, except in specialist areas such as‘community reflective action research’ (Boutilier et al., 1997).
The purpose of this paper is therefore to describe the development of a typology ofreflective practice in health promotion which takes account of both the individual andteam aspects of practice. It is recognised that reflection can be approached from arange of perspectives and contexts (Moon, 1999), so there is no suggestion that thismodel is definitive or exclusive. It is but one attempt to open health promotion
*Faculty of Life and Health Sciences, University of Ulster, Jordanstown, Newtownabbey, CoAntrim BT37 0QB, Northern Ireland. Email: [email protected]
Dow
nloa
ded
by [
Uni
vers
ity o
f G
lasg
ow]
at 0
7:23
19
Dec
embe
r 20
14

316 P. Fleming
planning to a reflective culture in an approach which is common to much healthpromotion practice—the application of a structured instrument which aids under-standing and analysis. This paper also explores how the typology has been used toreflect on how empowerment of individuals and populations (WHO, 1986) can beaffected by commonplace health promotion activity, in this case the evaluation of aworkplace smoking policy.
The term health promotion has a number of meanings and is, in some quarters, amatter of contestation (Fleming, 1999; Laverack, 2004). In its early stages ofdevelopment health promotion was defined as ‘the process of enabling people toincrease control over, and improve their health’ (WHO, 1986, p. 1). Several modelswhich derive from this early thinking use health promotion as an umbrella term whichincludes a range of interlinked activities such as heath education, prevention,development of healthy public policy and community development activity (Tanna-hill, 1985; French, 1990; Fleming, 1999). Health behavioural solutions, where avictim-blaming approach (Tones & Tilford, 2001) can be focused on individuals, areidentified as are population-focused interventions which are policy/legislatively-led.
Other theorists choose, rather than describing health promoting activity, to expli-cate the intention underpinning that activity. Thus health promotion can be viewedas rooted in, for example, medical or social models of health. It can primarily beprofessionally led, with compliance being expected from the target audience. Alter-natively, a more client-led model can be adopted whereby the target populations/communities/individuals are in control of the process, to varying degrees, from theneeds assessment phase onwards, creating a more partnership-oriented model(Beattie, 1991; Caplan & Holland, 1990). While this dichotomy of social andmedical/behavioural solutions, with their differing emphases on the balance ofpower between health promoters and their target/s, can seem clear-cut on paper, inreality the boundaries of approaches and practice can be much less clear (Laverack,2004).
The social-policy oriented models of health promotion (including health educa-tion), which eschew an emphasis being placed on individual health behaviour change,have been championed within the health promotion profession and literature formany years. Critical health education (Tones & Tilford, 2001) provides a keyexemplar within the wider paradigm of health promotion and has been described as‘creating social and political change in the interests of promoting public health’ (Tones &Green, 2004, p. 213). This concept, which is based on the extensive use of criticaltheory in its social theory iteration (Harvey, 1990; Calhoun, 1995), has a radicalagenda of social transformation as a key focus for the health gain of individuals,communities and wider populations. At the heart of the critical health educationmovement is the process of critical consciousness raising (Tones & Tilford, 2001), aconcept grounded in the beliefs and practices of liberation theologians (Friere, 1972).The educative act at the core of health education is the heightening of awarenesswithin society of the effects which socio-economic conditions have on the health ofthe public. The aim of critical consciousness raising is to galvanise society into takingradical action which will improve overall health status through addressing inequities
Dow
nloa
ded
by [
Uni
vers
ity o
f G
lasg
ow]
at 0
7:23
19
Dec
embe
r 20
14

Empowerment agenda in health promotion 317
in health, wealth and opportunity. The key to this process is empowered individuals,communities and populations.
Whichever iteration of health promotion is being practised, it has, however, beenobserved by Ziglio (1996) that, if enabling and empowerment (Rappaport, 1985;WHO, 1986) are not integral to the activity, then it is questionable if the activity ishealth promotion. Enabling improvement of socio-economic conditions, diseaseprevention or community development through education is primarily dependent onthe outworking of the principle of empowerment. It is therefore vital that the profes-sional engaging in health promotion is enabled to reflect on how a variety of factorscombine to enhance, or detract from, the empowerment agenda as a foundationalelement of any health promotion policy or programme. Further, it would seemappropriate that if reflection is to be employed in a meaningful manner, then someform of structure or intention must be engaged to render the reflective process bothaccessible and productive. It is for this reason that the research work of the author hasbeen employed to generate a model of reflective practice which is accessible to adiscipline which has hitherto not engaged in reflection in the formal sense.
Developing a reflective tool to enhance empowerment
When the absence of an appropriate tool for reflective practice in health promotionwas identified, it was decided that an incremental, experiential approach should beadopted which took account of the author’s role as a researcher, writer and theoristin health promotion. It was also essential that reflection should be firmly located in aclearly articulated health promotion discourse based on activity which was empower-ing and enabling (WHO, 1986; Ziglio, 1996; Fleming, 1999). To achieve this, severalpossibilities were explored.
In the first instance, there was the possibility of undertaking a simple, unstructuredform of ‘reflection’ which largely centred on considering themes such as ‘what I/wedid’, ‘how I/we could do it better’ and/or ‘where I/we went wrong’. This was,however, thought not to give enough assistance or focus to the potential reflectivepractitioner.
Another approach was through the issue of quality and its use of a ‘qualityassurance’ perspective. This did not, however, provide the desired solution as thisparticular type of tool required the setting of either an external standard through amechanism such as external standards inspection (ESI) or through the internal stan-dards typical of total quality management (TQI) (Øvretveit, 1996; Speller, 1998).This approach is used to good effect in core areas of health promotion practice,namely service provision and practice guidelines, professional development througheducation and training, recruitment and selection, principles of professional practiceand measurement and monitoring of standards of practice (Totten, 1992). However,when applying specific quality instruments, it must be remembered that a number ofthese are focused on single-organisation initiatives and are thus less applicable tomulti-agency collaborations; they are often focused on large scale initiatives and thusless useful to small scale projects; and health promotion projects tend to be unique in
Dow
nloa
ded
by [
Uni
vers
ity o
f G
lasg
ow]
at 0
7:23
19
Dec
embe
r 20
14

318 P. Fleming
their context and not often repeated (Haglund et al., 1998). In short, the developmentand application of a quality instrument is somewhat demanding in scale for theindividual practitioner or small team. Also, the setting of a standard against which aninitiative is measured may restrict the scope of the reflection.
A further approach considered was that of autoethnography where theresearcher would focus on his own experience as a health promotion planner andof facilitating research which would be used as a basis for health promotion plan-ning. This approach, which is recognised by some to be at the boundaries ofacademic research (Sparkes, 2000), is said to connect the personal to the cultural(Reed-Danahay, 1997). The underlying approach would be to produce a ‘highlypersonalised account where authors draw on their own experiences to extendunderstanding of a particular discipline or culture’ (Holt, 2003, p. 2). In this case‘the personal’ is the experience of the author in seeking to improve health promo-tion planning practice through a programme of research, and ‘the cultural’ is thecontext within which that programme would be undertaken. It was also recognisedthat autoethnography is both process and product (Tedlock, 2000) and in thiscase both of these entities would be generated less from a study of personal feelingsand reactions and more from a series of personal observations of the influences whichimpinge on key elements of planning. This paradigm, while offering possibilities,tends to focus primarily on individuals, their needs and reactions and does notnecessarily provide a framework within which the practitioner could operate tosystematically reflect on all the factors which contribute to create the totality oftheir practice.
Taking all the foregoing considerations into account, it was decided that a usefulreflective tool should structure reflective thought around a number of target areas inpractice and would permit a range of reflective activities to be employed. Theresearch and scholarship work of the author and, as appropriate, key partners, wastherefore developed over an extended period with a conscious, inbuilt reflectiveelement of self-discovery and critical examination of practice (Atkins & Murphy,1993; Scanlon & Chernonmas, 1997). The programme included a book chapter(Fleming, 1999) which sought to set out the author’s personal manifesto of under-standing, at that time, of foundational issues such as the nature of health and healthpromotion and the key issues in the planning process—clarification on knowledge,beliefs and values. This was followed by a series of empirical studies which sought toexplore the flexibility and applicability of a specific qualitative design, namely rapidappraisal (Harvey & Fleming, 2000; Harvey et al., 2001); and the creation of ahealth promoting environment in the workplace in the spirit of a settings approachto health promotion (Harvey et al., 2001, 2002a, b; Harvey & Fleming, 2002;Fleming & Harvey, 2002).
Over an extended period, a reflective worldview of practice was developed whichfocused on a process of self-awareness as a practitioner and researcher in both theindividual and team contexts. This worldview was, as it developed, factored into theprimary aim of each research or scholarship project. This permitted the developmentof a reflective tool which had four key aims, namely to:
Dow
nloa
ded
by [
Uni
vers
ity o
f G
lasg
ow]
at 0
7:23
19
Dec
embe
r 20
14

Empowerment agenda in health promotion 319
● Enable the ongoing development of a critical/reflective world view of key elementsof practice.
● Establish a flexible theoretical construct which would aid reflective practice bothin the self-reflective sense for individual practitioners and also for a range of plan-ning teams.
● Add to the body of knowledge regarding health promotion planning, particularlyin the workplace, through reflective practice.
● Develop any emergent reflective tool for use in teaching where those in educationand training contexts could reflect on their own practice and perspectives throughfocusing on the work of others.
The practice of reflection: theoretical underpinnings
Having established the rationale for the use of critical reflection in health promotion,it was then asked how this was to be operationalised in practice. In the first instance,it was considered that foundational elements of reflective practice should be about‘knowing’ the world of practice and ‘knowing’ the role of self within this world (VanManen, 1977). Further, critical reflection was perceived to involve issues such as in-depth questioning, considering alternative courses of action and affirming good prac-tice. To address these question categories, a range of evidence sources was consideredappropriate which included knowledge of self, personal observation, informedobservation of others and formal mechanisms such as research and audit.
In developing a theoretical perspective for reflective practice in health promotion itwas therefore necessary to underpin a reflective framework, which is useful for thehealth promotion practitioner, by defining the term ‘critical reflection’ to imply, in thecontext of health promotion …
… the ability of the health promotion practitioner to focus on specific issues in theirexperience and practice and, in the personal and organisational contexts, to contextualise,observe, analyse and learn, thus generating knowledge which will affirm good practice and,where appropriate, enable the practitioner to take enhancing/consolidating/correctiveaction which will lead to increased excellence in health promotion practice …
This approach to reflective practice could thus enable the reflective practitioner:
… to gain insight which will help discover not only what is not known, but what is thoughtto be correct that is wrong: this will lead to necessary unlearning—the unlearning of previ-ous beliefs. (Grainger, 2001, p. 461)
This form of reflection can clearly map onto both reflection-before-action (Green-wood, 1993) which is closely aligned to ‘anticipatory reflection’ (Van Manen, 1991)and Schön’s reflection-on-action (Schön, 1983). The juxtaposition of these threeelements of reflective practice sits well with the reflective practitioner in health promo-tion. The ability to structure reflection on an in-progress or completed intervention,to anticipate key issues in light of previous experience and to bring both of theseprocesses to bear on elements of planning is likely to generate hermeneutically derivedknowledge (Habermas, 1971) which will give insight into factors which influence
Dow
nloa
ded
by [
Uni
vers
ity o
f G
lasg
ow]
at 0
7:23
19
Dec
embe
r 20
14

320 P. Fleming
planning. This interpretive knowledge can use as its basis an eclectic evidence basewhich may be, in the first instance, analytical (in the positivist sense) or hermeneuticand will, in the Habermasian economy of knowledge constitutive interests, lead to thegeneration of emancipatory interests—the reflective language which describesempowerment as understood in the health promotion arena (Tones & Green, 2004).
In the wider literature of theory development, the terms ‘theory’ and ‘model’,which are widely extant in the field of health promotion, have been observed to beused somewhat haphazardly and, on a number of occasions, interchangeably (Dies-ing, 1971; Warr, 1980). Theory, in the scientific sense, is seen as a linguistic devicewhich interlinks a series of axioms which enable explanation and prediction fromthese axioms (Suppe, 1977). Models are, according to Nagel (1979), indispensableto theory as heuristic and analogically connective devices which play no part in theformulation of theory but are key to its explanation. Rawson (2002) points out,however, that in health promotion various health promotion taxonomies have beendeveloped with insufficient support of a theoretical base. He observes that ‘as anormative [ideal] account the underlying theory receives only the crudest analysis’(Rawson, 2002, p. 256).
This alleged deficit in the development of health promotion theory does not,however, lessen the observation of Tones and Tilford (1994) in relation to evaluationof health promotion interventions. They state that a sound theoretical framework isfoundational to practice. Such frameworks are observed at both the macro and microlevels. With regard to the usefulness of theory, Seedhouse (1997) states that reasonsfor the use of theory are based on the fact that health promotion is not neutral butembraces human values and biases. Further, as health promotion is often populationfocused, explicit permission or consent is not a possibility, thus making it imperativethat practitioners are both accountable and willing to explain our actions. To addressthese factors, theory must play a part in analysing the politics and ethics of practicethrough comparison and assessment of effectiveness and efficiency.
Thus, taking these considerations into account, theory can be described as:
Systematically organised knowledge applicable in a relatively wide variety of circumstancesdevised to analyse, predict, or otherwise explain the nature or behaviour of a specified setof phenomena that could be used as the basis for action. (van Rhyn & Heany, 1992)
It was with this desire for systematic organisation that the reflective tool for healthpromotion was developed which, in the first instance, sought to establish the first aim(see above) which was to create a reflective tool grounded in a coherent critical/reflec-tive world view. In this case, such a worldview was linked to the empowermentagenda which was, in turn, derived from the discourse of critical health education(Tones & Green, 2004).
The reflective typology
A series of structural attempts to reflect on the author’s research and scholarship hastherefore led, through an iterative process, to the formulation of a theoretical
Dow
nloa
ded
by [
Uni
vers
ity o
f G
lasg
ow]
at 0
7:23
19
Dec
embe
r 20
14

Empowerment agenda in health promotion 321
construct which enables the health promotion practitioner to reflect on her/hispractice. Termed ‘A typology for reflective practice in health promotion planning’,the construct is predicated on the understanding that the term ‘typology’ is under-stood as ‘a classification according to general type, especially in archaeology, psychol-ogy or the social sciences’ (The New Oxford Dictionary of English, 1998, p. 2003).
This understanding, as viewed by Rawson, accords with the Darwinian view oftaxonomic classification of species, and ‘may be regarded as embryonic formulationsnecessarily preceding the maturation of theory’ (Rawson, 2002, p. 258). Nutbeamand Harris (1999) also point out that many theories in frequent use in healthpromotion have not been rigorously tested, as they might be in the physical sciences.Therefore these theories should be more accurately referred to as theoretical frame-works or typologies. Further, according to Nutbeam and Harris, such frameworkshave, nonetheless, the capacity to make a substantial contribution to the planning ofhealth promotion interventions. Thus the range of planning influences is classifiedand systematised to produce a framework which enables insights into levels andphases of health promotion planning.
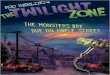
When viewed within the context of levels of theory an interesting issue arises. Whilethe typology itself sits in the domain of grand theory (models) it is used to deal withissues which are clearly at the level most used by those involved in health promotion,namely the practice theory domain (McKenna, 1997). Further, when reflecting onthe influences which impact on planning and delivery of health promotion interven-tions, it is observed that the determinants of health which are to be addressed and thehealth promotion efforts which form the intervention do not exist in a vacuum(Fleming, 1999; Barclay & Fleming, 2003). Planning is affected by a wide range ofissues which are not within the direct control of either clients, health promoters or,indeed, in many circumstances, policy-makers. The conceptual typology for reflectivepractice in health promotion planning is therefore derived from the second and thirdkey aims articulated above and is comprised of three interlinked components (seeFigure 1) which structure and systematise the reflection.Figure 1. A conceptual typology for reflective practice in health promotion planning
The reflective domains
The domains for reflection permit the practitioner to create what is described in thefirst aim as a world view which contextualises and explains the key elements ofpractice and permits a critical/reflective approach. These domains were identified atthe outset of the research through the use of a visual mapping exercise where all theperceived factors which might impinge on the inception, planning and delivery of ahealth promotion initiative were mapped around the term ‘health promotion plan-ning’. This range of factors was then categorised into a smaller number of conceptualgroups which were then further reduced to the three domains where:
● The self as programme planner seeks to examine personal attributes such as moti-vations, skills, values and beliefs of the programme planner/team including ethicaland professional issues as they impact on the individual/team. The actions and
Dow
nloa
ded
by [
Uni
vers
ity o
f G
lasg
ow]
at 0
7:23
19
Dec
embe
r 20
14

322 P. Fleming
reactions of the individual/team as participant in the process are also open toreflection.
● The programme planning context seeks to critically reflect on the contextual influ-ences within which the planning process is undertaken. This includes assumptions,values, principles, theories and models which underpin practice and are predomi-nant in the programme planning environment. Other contextual issues includepolicy issues, strategic approaches, finance and sociocultural factors.
● The programme planning process seeks to critically reflect on specific issues whichare key to elements of the planning process, its delivery and outcomes, bothintended and unintended. This includes a wide range of factors such as power andcontrol issues between those seeking to promote health and those whose health isthe subject of the intervention, the use and misuse of planning models, specificmodes of delivery of interventions, approaches to evaluation and unpredictedoutcomes.
The timing of reflection
This element of the typology is found at the base of Figure 1 and indicates thatreflection can take place at any point from pre-planning to post-intervention. This
The Context in Programme Planning
The Process of Programme Planning
The Self in Programme Planning
A T
axon
omy
ofK
ey R
efle
ctiv
e Q
uest
ions
Pre-implementation Implementation Post-implementation
Figure 1. A conceptual typology for reflective practice in health promotion planning
Dow
nloa
ded
by [
Uni
vers
ity o
f G
lasg
ow]
at 0
7:23
19
Dec
embe
r 20
14

Empowerment agenda in health promotion 323
time line indicates that reflective practice can either be engaged in before the planningand implementation of a programme through anticipatory reflection (Van Manen,1991), intermittently or continuously practised during a programme through reflec-tion-in-practice (Schön, 1983) or subsequent to the programme’s completionthrough reflection-on-action (Schön, 1983, 1991). Thus outcomes can be reflectedupon in anticipation, contemporaneously or retrospectively. The hatched linesreconnecting the domains indicate that reflection in any of the domains may lead toan initiation of further reflection in, or a revisiting of, any of the other domains forfurther reflection.
The taxonomy of reflective questions
The taxonomy of reflective questions is the primary vehicle for the fulfilment of thethird aim, which seeks to generate new knowledge to enhance and extend the bound-aries of practice. It also enables a coherent and planned approach to reflection in eachof the three reflective domains of the typology. The taxonomy is not, in fact, a fixedset of questions, but one which is created at the first stage of the reflective process andproduces a tailored framework of enquiry for each individual reflective exercise. Itshould be noted that while an initial taxonomy of questions is developed, this doesnot preclude development of further question areas; practice has shown that additionsand modifications are almost inevitable as the reflective process develops. Thus thereflective practitioner can engage in a questioning regime which ranges from arelatively extensive process of examining a wide range of factors which impinge onprogramme planning and delivery to, at its most minimal, one element of the processe.g. needs assessment, delivery methods or evaluation.
The method by which the questions are answered is varied, but involves a choiceof strategy which is ‘fit for purpose’. Thus anticipatory reflection which considers keyissues which may arise during the intervention; it may generate a series of questionswhich may be answered throughout the life of the project. In any of the reflectivemodes simple narrative may be appropriate in some cases while in others a two-column table may be created whereby key issues are listed and reflective responsesrecorded. In the case of reflection undertaken contemporaneously with delivery of aninitiative, a reflective diary may be maintained with the structure of entries beingeither predetermined or iterative. Further, any form of reflection may involve the useof peer observation and/or online techniques such as online blogging to test ideas andperspectives.
Reflection in practice: empowerment in the workplace
To illustrate the use of the typology in practice, an example is drawn from theauthor’s own reflective practice. The typology was applied to an evaluation of a work-place smoking policy which was undertaken in a large British university (Harvey et al.,2001). In the context of promoting health in the workplace, the university hadintroduced a smoking policy for the elimination of environmental tobacco smoke
Dow
nloa
ded
by [
Uni
vers
ity o
f G
lasg
ow]
at 0
7:23
19
Dec
embe
r 20
14

324 P. Fleming
(ETS) in all but two areas of its multi-campus buildings, these being the staffcommon room (a membership facility for a range of academic and non-academicstaff) and the students’ union. Designated smoking areas, equipped with appropriateair filtration systems, were also identified and provided as an interim measure in theimplementation of the policy; this provision was considered helpful in increasing thecommitment of smokers to adhere to the policy. Free smoking cessation programmeswere also provided on an ongoing basis to all staff and students. Subsequent to theintroduction of the policy, the health and safety committee of the university, whichhad overall responsibility for the formulation and implementation of the policy,decided to undertake a formal evaluation of its effectiveness. A primary motivator forthe evaluation was the proposed removal of the interim designated smoking areas.
The evaluation of the impact of the policy took the form of a rapid appraisal with astratified random sample of staff and students using a self-completed questionnairecontaining closed and open questions. The steering group for the project wasconsulted through a focus group format to formulate further action in light of theevaluation findings; this action resulted in the closure of designated smoking areas(Harvey et al., 2001). One specific area of learning which resulted from the applica-tion of the typology was a consideration of the ethical implications of introducing thecoercive measure of eliminating designated smoking areas with specific reference tothe impact on smokers (Harvey et al., 2002).
The typology was found capable of harnessing the critical powers of the reflectivepractitioner to develop insights into practice which generate new knowledge or rein-force pre-existing insights to enhance practice (Baumgartner, 2001). These powersemployed sentiency (Hullfish & Smith, 1961; Boud et al., 1985) and, from theauthor’s perspective, knowledge constitutive interests which are primarily hermeneu-tic in character (Habermas, 1971). A key goal was to increase the control which theworkforce has individually and collectively over their health—an emancipating inter-est (Habermas, 1971; Barnett, 1997). This increase in control came largely from anability to reflect on the involvement of the author (self) and his collaborators (others)(Van Manen, 1991) by learning from specific events, incidents and, notably,processes (Schön, 1983; Van Manen, 1991).
In the context of applying the typology, the substantive reflective exercise wasundertaken at the post-implementation stage of the smoking policy initiative. Thesmoking policy evaluation was ongoing in parallel with the development of thetypology. It was thus only after the completion of the full policy evaluation thatthe completed framework of the typology was available. It was therefore decidedthat the reflection on this initiative would focus on each of the three reflectivedomains in the typology. As this health promotion initiative was, as is common inhealth promotion, a team initiative, the reflection was applicable at a team level.However, individual team members could also reflect on their personal role in theevaluation process. In this case, a ‘mixed-mode’ exercise evolved whereby reflectionon the role of self was undertaken as a personal exercise while the contextualinfluences and process issues were reflected on at the team level.
The taxonomy of reflective questions was thus as follows:
Dow
nloa
ded
by [
Uni
vers
ity o
f G
lasg
ow]
at 0
7:23
19
Dec
embe
r 20
14

Empowerment agenda in health promotion 325
(a) Role of self ● What was my attitude to individuals, particularly smokers, who were the
subject of the evaluation?● How did I resolve the conflict between the findings of the evaluation and
my ‘gut reaction’ regarding the consequences of eliminating designatedsmoking areas?
● How did the role of self affect the empowerment of the population understudy?
(b) Contextual influences ● In how far was the timing of the evaluation an aid to the elimination of the
designated smoking areas?● What effect did the elimination of designated smoking areas have on the
use of areas not controlled by the university, i.e., staff common room andstudents’ union?
● What effects did the evaluation of a smoke-free environment have on theempowerment of the study population, both non-smokers and smokers?
(c) Process issues ● Was the qualitative element of the evaluation process sufficiently robust to
permit all the players in the ETS issue to have their voices heard?● Did the consultative process enhance empowerment levels of the study
population?
Outcomes of reflection
When reflecting on the role of self in the evaluation of smoking policy, an issue whichemerged was that of personal attitudes to smokers at the planning and implementa-tion stage of the evaluation. While the term ‘smoker’ was, unsurprisingly, the termused to describe the sub-population to be regulated by the smoking policy, onreflection this label represented a range of personal perceptions regarding smokers.These perceptions were seen as linked to a cadre of ambivalent attitudes.
In answering the reflective question regarding personal attitude, a brainstormingexercise was undertaken which identified that the term ‘smoker’ was representationalof other, stronger and often less positive descriptors/labels. These included termssuch as ‘users’, ‘addicts’, ‘victims’, ‘polluters’ and ‘litter louts’. Attribution ofperceived personal characteristics of smokers included lack of self-control, weak-will,inconsideration for others and subversive attitudes to workplace regulations. Interest-ingly, when the plight of the smoker was rank ordered with that of other forms ofaddiction, it was perceived to induce a less sympathetic reaction than would that ofthose addicted to, for example, alcohol or other drugs. Reasons for this were thoughtto link to the frequency with which smokers openly, and usually without negotiation,subjected others in their environment to environmental tobacco smoke.
Overall, these underlying, unspoken and hitherto unarticulated attitudes were seenas problematic when set in the context of two key principles of health promotion,
Dow
nloa
ded
by [
Uni
vers
ity o
f G
lasg
ow]
at 0
7:23
19
Dec
embe
r 20
14

326 P. Fleming
namely empowerment and enabling (Ziglio, 1996). Negative attitudes towards atarget population can have clear implications for the need for respect of all individualsand populations who are the targets of health promotion interventions. The desire togenuinely examine alternative outcomes which might be more facilitative to thesmoking population was perceived to be less evident than might be expected withother addictions.
A further consequence of self-reflection was a sense of crisis (Schön, 1992) inanalysing the disjunction between the evaluation findings and ‘gut reaction’ of theevaluator towards the consequences of the findings. This perception was identifiedwhen pairs of statements were created using the formula ‘I believe …’ and‘Conventional wisdom says …’; for example:
I believe that smokers should be able to choose to indulge their habit in an environmentwhich eliminates the risks from ETS (environmental tobacco smoke) for non-smokers.
Conventional wisdom says that total elimination of ETS, regardless of the consequencesfor smokers, is an imperative for the creation of a health promoting workplace.
In this case, the tension centred on needing to support the conventional wisdom ofa complete ban on smoking while balancing the human rights of all those in theuniversity environment (Harvey et al., 2002). However, self-reflection indicated thatthe need to maintain professional standing with motivated managers producedtension for the evaluator (a committed non-smoker) as he could also recognise theneed for smokers to have their addiction taken into account through the continuanceof designated smoking areas as well as through the planned provision of free smokingcessation programmes.
In terms of contextual issues, the role and timing of the evaluative exercise inproviding a formal justification for initiating the final change to a complete smokingban was examined. If the evaluation was used as a formal mechanism to support analready pre-determined course of action, then were the rights of the non-compliantsub-population (smokers) really given equal status to those of the compliant (non-smokers)? This coercive (in the non-pejorative sense) public health approach clearlyhad two outcomes regarding empowerment of the study population. Non-smokerssaw their control over their health increase as they were no longer in proximity to anETS—an increase in levels of empowerment. For non-smokers, however, the resultsof the evaluation diminished the possibilities for the empowered making of informedchoices regarding their health behaviour; their capacity to make autonomous deci-sions was reduced. Rather than choosing to smoke in a designated area where ETScould be controlled, they were given no choice but to leave the building or to makeheavier use of the two exempted areas—the staff common room and students union.There was therefore, arguably, a legitimate case to be made for the continuance ofdesignated smoking areas as these had a number of perceived benefits. First, theyprevented smokers being exposed to the often inclement weather with the consequenthealth risks. Secondly, hindsight revealed that they were key in controlling theconsiderable levels of tobacco detritus which accrued around building entrances afterthe complete ban was introduced. Finally, the designated areas prevented the
Dow
nloa
ded
by [
Uni
vers
ity o
f G
lasg
ow]
at 0
7:23
19
Dec
embe
r 20
14

Empowerment agenda in health promotion 327
congregation of smokers immediately in front of public entrances, thus forcing allentrants to proceed through a smoke-charged atmosphere.
The final element of reflective activity concerned process issues. The key elementwhich emerged was that while the evaluation process, which used both quantitativeand qualitative data, was robust for the purpose to which it was applied, the questionstill remained, did the qualitative element of the process permit the voices of all theplayers in the scenario to be heard and given equal credence? In this case, the contentof what was said was considered less important than whether or not all voices had hadan equal opportunity to be heard and taken seriously. Reflection revealed that thesmoking sub-population did indeed have an equal opportunity to have its voice heard.The use of a stratified random sample to identify the sub-populations of the universityensured equity in this regard. However, the limitations of the consultation tool itselfposed a question as to how effective the exercise was in terms of hearing what it waslike for smokers to manage their addiction during the working day in the context ofpolicy-imposed limitations on their smoking habit. A series of semi-structured inter-views might have further enhanced the understanding of the smokers’ perspective.
Conclusion
A number of learning points was derived from the use of the typology when theoutcomes were reviewed in light of the original aims for its creation. In the firstinstance the first aim, to enable the ongoing development of a critical/reflective world-view of key elements of practice, was clearly achieved particularly in relation to therole of self in the planning process. A somewhat uncomfortable but insight-producingoutcome was achieved through the ability to ask questions which would be difficultto pose in the context and conduct of a health promotion programme. Overall, thecapacity to challenge basic attitudes and assumptions was more feasible when theprompts of a formal taxomony of questions were available.
In terms of the second and third aims, the typology proved indeed to be a ‘flexibletheoretical construct which would aid reflective practice both in the self-reflectivesense for individual practitioners and also for a range of planning teams’. Its applica-tion to the exemplar programme proved its ability to add to the body of knowledgerelating to health promotion planning. The reasons for this assertion are derived fromthe fact that the typology:
1. Proved useful to experienced professionals who are accustomed to using suchtheoretical constructs for explaining and enhancing theory and practice.
2. Gave time, space and structure to self-evaluation which was not linked to anyrequirements by funders or managers; the findings were personal and could betaken account of without the need for exposure or publication of significant learn-ing points.
3. Permitted both individual and team-led approaches to reflection whereby thequestions in the taxonomy relating to context and process could be generated byan individual or in a collaborative manner—a key element for health promotion
Dow
nloa
ded
by [
Uni
vers
ity o
f G
lasg
ow]
at 0
7:23
19
Dec
embe
r 20
14

328 P. Fleming
and other public health activities where collaborative partnerships are a corner-stone of policy and practice both nationally and internationally.
4. Was applicable at a range of points in the timescale of any initiative.
The final aim sought to develop any emergent reflective tool for use in teachingwhere those in education and training contexts could reflect on their own practice andperspectives. Early use of the typology by students and practitioners has indicated itsvalue to lie in its ability to highlight the value of reflective practice as an integralelement of professional practice which lies entirely within the control of the healthpromotion specialist. Further, its flexibility in adapting to specific reflective needsfrom the superficial to the profound and detailed is recognized as is the accessibilityand simplicity of the typological design. Overall, it appears that the typology hasprovided one starting point for the development of a paradigm of reflective practicewhich will enhance the endeavours of all those involved in the delivery of healthpromotion which is both empowering and enabling.
Notes on contributor
Paul Fleming is Associate Dean of the University of Ulster’s Faculty of Life andHealth Sciences. As an academic Health Promotion Specialist, his teaching andresearch interests are in the areas of health promotion theory including reflectivepractice, health promoting settings (workplaces, schools and tertiary educationinstitutions) and adolescent mental and sexual health.
References
Atkins, S. & Murphy, K. (1993) Reflection: a review of the literature, Journal of Advanced Nursing,18, 1188–1192.
Barclay, L. & Fleming, P. (2003) The determinants of health—an overview, Promoting Health 18, 4–7.Barnett, R. (1997) Higher education, a critical business (Buckingham, Society for Research into
Higher Education).Baumgartner, L. M. (2001) An update on transformational learning, New Directions for Adult and
Continuing Education, 89, 15–22.Beattie, A. (1991) Knowledge and control in health promotion: a test case for social policy and
social theory, in: J. Gabe, M. Calnan and M. Bury (Eds) The sociology of the health service(London, Routledge), 162–202.
Boud, D., Keogh, R. & Walker, D. (Eds) (1985) Reflection: turning experience into learning (London,Kogan Page).
Boutilier, M., Mason, R. & Rootman, I. (1997) Community action and reflective practice in healthpromotion research, Health Promotion International, 12(1), 69–78.
Calhoun, C. (1995) Critical social theory. Culture, history and the challenge of difference (Oxford,Blackwell).
Caplan, R. & Holland, R. (1990) Rethinking health education theory, Health Education Journal,49(1), 10–12.
Diesing, P. (1971) Patterns of discovery in the social sciences (London, Routledge).Fleming, P. (1999) Health promotion for individuals, families and communities, in: A. Long (Ed.)
Interactions for practice in community nursing (Basingstoke, Macmillan), 228–259.
Dow
nloa
ded
by [
Uni
vers
ity o
f G
lasg
ow]
at 0
7:23
19
Dec
embe
r 20
14

Empowerment agenda in health promotion 329
Fleming, P. & Harvey, H. (2002) Strategy development in dealing with violence against employeesin the workplace, Journal of the Royal Society for the Promotion of Health, 122(4), 226–232.
French, J. (1990) Boundaries and horizons, the role of health education within health promotion,Health Education Journal, 49(1), 7–10.
Freire, P. (1972) Pedagogy of the oppressed (Harmondsworth, Penguin).Glen, S., Clark, A. & Nichol, M. (1995) Reflecting on reflection: a personal encounter, Nurse
Education Today, 15, 61–68.Grainger, C. (2001) Assessing and improving your own professional practice, in: D. Pencheon, C.
Guest, D. Melzer & J. A. Muir Gray (Eds) Oxford handbook of public health (Oxford, OxfordUniversity Press), 460–470.
Greenwood, J. (1993) Reflective practice: a critique of the work of Agyris and Schön, Journal ofAdvanced Nursing, 18, 1183–1187.
Habermas, J. (1971) Knowledge and human interests (London, Heineman).Haglund, B. J. A., Jansson, B., Petterson, B. & Tillgren, P. (1998) A quality assurance instrument
for practitioners. An example from Sweden, in: J. K. Davies & G. Macdonald (Eds)Quality, evidence and effectiveness in health promotion—striving for certainties (London, Rout-ledge), 93–116.
Harvey, H. D. & Fleming, P. (2000) A rapid appraisal method for the selection and pre-testing ofenvironmental health leaflets, Journal of the Royal Society of Health, 120(2), 112–116.
Harvey, H. D., Fleming, P. & Patterson, M. (2001) A rapid appraisal method for reviewing theeffectiveness of workplace smoking policies in large and medium sized organisations, Journalof the Royal Society of Health, 121(1), 50–55.
Harvey, H. D., Fleming, P. & Mooney, D. (2002a) Violence at work: an initial needs assessmentfor an environmental health department as health promoting workplace, Journal ofEnvironmental Health Research, 1(1), 41–49.
Harvey, H. D., Fleming, P. & Patterson, M. (2002b) Ethical dilemmas and human rightsconsiderations arising from the evaluation of a smoking policy in a health promoting setting,International Journal of Environmental Health Research, 12(3), 269–275.
Harvey, H. D. & Fleming, P. (2002) Strategy development in dealing with violence againstemployees in the workplace, Journal of the Royal Society of Health, 122(4), 226–232.
Harvey, L. (1990) Critical social research (London, Unwin-Hyman).Holt, N. L. (2003) Representation, legislation and autoethnography: an autoethnographic writing
story, International Journal of Qualitative Methods, 2(1), 1–22.Hullfish, H. & Smith, P. (1961) Reflective thinking: the method for education (New York, Dodd,
Mead & Co).Issitt, M. (2003) Reflecting on reflective practice for professional education and development in
health promotion, Health Education Journal, 62(2), 173–188.Laverack, G. (2004) Health promotion practice, power and empowerment (London, Sage Publications).McKenna, H. P. (1997) Nursing theories and models (London, Routledge).Moon, J. (1999) Reflection in learning and professional development: theory and practice (London,
Kogan Page).Nagel, E. (1979) The structure of science (Indianapolis, Hackett).Nutbeam, D. & Harris, E. (1999) Theory in a nutshell (Roseville, NSW, McGraw-Hill).Øvretveit, J. (1996) Quality in health promotion, Health Promotion International, 1, 55–62.Rappaport, J. (1985) Terms of empowerment/examples of prevention: toward a policy for commu-
nity psychology, American Journal of Psychology, 15(2), 121–147.Rawson, D. (2002) Health promotion theory and its rational construction, in: R. Bunton & G.
Macdonald (Eds) Health promotion disciplines, diversity and developments (London, Routledge),249–270.
Reed-Danahay, D. E. (1997) Auto-ethonography: re-writing of the self and the social (Oxford, Berg).Scanlon, J. M. & Chernonmas, W. M. (1997) Developing the reflective teacher, Journal of
Advanced Nursing, 25(6), 1138–1143.
Dow
nloa
ded
by [
Uni
vers
ity o
f G
lasg
ow]
at 0
7:23
19
Dec
embe
r 20
14

330 P. Fleming
Schön, D. (1983) The reflective practitioner (California, Josey-Bass).Schön, D. (1991) The reflective practitioner (California, Josey-Bass).Seedhouse, D. (1997) Health promotion. Philosophy, prejudice and practice (Chichester, John Wiley &
Sons).Sparkes, A. C. (2000) Autoethnography and narratives of self: reflections on criteria in action,
Sociology of Sport Journal, 17, 21–41.Speller, V. (1998) Quality assurance programmes: their development and contribution to
improving effectiveness in health promotion, in: D. Scott & R. Weston (Eds) Evaluating healthpromotion (Cheltenham, Stanley Thornes), 75–91.
Suppe, F. (1977) The search for philosophic understanding of scientific theories, in: F. Suppe(Ed.) The structure of scientific theories (Urbana, University of Illinois Press), 3–232.
Tannahill, A. (1985) What is health promotion?, Health Education Journal, 44, 167–168.Tate, S. & Sills, M. (2004) The development of critical reflection in the health professions (London,
Higher Education Academy LTSN Health Sciences and Practice Subject Centre).Tedlock, B. (2000) Ethonography and ethnographic representation, in: N. Denzin & Y. Lincoln
(Eds) Handbook of qualitative research (London, Sage Publications).Tones, K. & Tilford, S. (2001) Health education: effectiveness, efficiency and equity (London, Nelson
Thornes).Tones, K. & Green, J. (2004) Health promotion—planning and strategies (London, Sage
Publications).Totten, C. (1992) Developing quality in health education and health promotion (Society of Health
Education and Health Promotion Specialists).Van Manen, J. (1977) Linking ways of knowing with ways of being practical, Curriculum Inquiry, 6,
205–208.Van Manen, J. (1991) The tact of teaching (New York, The State of New York Press)Van Rhyn, M. & Heany, C. A. (1992) What’s the use of theory?, Health Education Quarterly, 19(3),
315–330.Warr, P. B. (1980) An introduction to models in psychological research, in: A. J. Chapman & D.
M. Jones (Eds) Models of man (Leicester, British Psychological Society), 291–310.World Health Organisation (1986) Ottawa charter on health promotion (Geneva, World Health
Organisation).Ziglio, E. (1996) How to move forward towards evidence-based health promotion interventions,
paper presented at Third European Conference on Effectiveness of Health Promotion and HealthEducation, Turin.
Dow
nloa
ded
by [
Uni
vers
ity o
f G
lasg
ow]
at 0
7:23
19
Dec
embe
r 20
14