-
8/6/2019 English 3 2
1/18
1
PREFACE
First of all, I would like to thank God for the blessing and
health so I could finish this
paper on time. I also want to thank my supervisor, Prof. Dr.
Widyasari K, Sp. MK. for his
guidance and help on this paper.
Thanks to my family that has supported me during this writing.
And thanks to my
friends for their helps. Without their helps and supports, I
wouldnt be able to finish this paper.
This paper is far from perfect. There are a lot of mistakes in
the writings, whether the
grammar or the theory. I hope after reading this paper, readers
could give me some advice and
critics. Hopefully, with the critics and advice, I will be able
to develop myself. I apologize for all
the mistakes Ive made in this paper.
I hope this paper could be useful to all the readers. Thank
you.
Jakarta, January 2011
Aji Patriajati
-
8/6/2019 English 3 2
2/18
2
CONTENTS
Preface .. 1
Contents .. 2
Abstract .. 3
CHAPTER I Introduction ...... 4
I. 1 Background ...... 4
I. 2 Problems ...... 4
I. 3 Limitation of the Problems.. 5
I. 4 Objectives ...... 5
I. 5 Methods of Writing ...... 5
I. 6 Frame of Writing ...... 6
CHAPTER II Dengue Virus ...... 7
II. 1 Morphology ...... 7
II. 2 Genome Organization .................. 7
II. 3
II. 4
Replication cycle
Antibody Responce
......................................................
..
8
10
CHAPTER III Comparison NS1 with IgM ELISA Capture ...... 13
CHAPTER IV Conclusion ......... 16
BIBLIOGRAFI ..... 18
-
8/6/2019 English 3 2
3/18
3
Abstract
Dengue is a viral infection of humans that is transmitted by
mosquitoes. Dengue is a very
important public health problem in many developing countries.
Recently, new tests to help
diagnose patients with dengue have been developed. Evaluating
these tests to see how well they
perform in different countries and in different health care
settings is an important process that
helps to guide health care policy on whether these assays are
likely to be useful in making a
diagnosis, and if so, when best to use them. Our hospital-based
results, using two different types
of NS1 tests for diagnosing dengue, indicates that these tests
are most sensitive when used during
the first 3 days of illness and are most likely to be positive
if the patient has primary dengue. Our
results also show that a positive NS1 test result is a
reflection of the amount of virus in the blood,
so that patients with high amounts of virus in the blood are
more likely to be NS1 positive.
Collectively, the results indicate these NS1 tests deserve
inclusion in the diagnostic approach to
dengue.
-
8/6/2019 English 3 2
4/18
4
CHAPTER I
Introduction
I. 1. Background
Dengue is a major public health problem in many parts of the
tropical developing world
[1,2]. Dengue is caused by infection with one of four serotypes
of dengue virus (DENV1-4),
which are arboviruses belonging to the Flaviviridae family.
Although most DENV infections are
asymptomatic, a proportion result in clinically apparent disease
that varies in severity from mild
undifferentiated fever through to more severe syndromes,
primarily dengue haemorrhagic fever
(DHF) and dengue shock syndrome (DSS). DHF is a vasculopathy
characterized by capillary
leakage and haematological dysregulation; in severe case
hypovolaemic shock (DSS) may
develop. There are no licensed vaccines or specific antiviral
therapies for dengue, and patient
management relies on good supportive care. Nowadays scientist
develop Detection of the dengue
NS1 antigen during the symptomatic phase of illness represents
an important advance in thediagnosis of dengue fever.
I.2. Problems
Dengue hemorrhagic fever, is an increasing cause of morbidity
and mortality throughout the
tropical world. There are an estimated 50 to 100 million cases
of dengue infection each year,
including about half a million cases of dengue hemorrhagic
fever. The number of cases of bothdengue fever and dengue
hemorrhagic fever has increased dramatically for the past few
decades,
and the geographic range has extended to involve most tropical
countries.
-
8/6/2019 English 3 2
5/18
5
I. 3. Limitation of the Problems
1. Early and accuratediagnosis can assist in patient management
by directing clinicalattention to the appearance of major warning
signs of severe or even life threatening
complications
2. Accurate dengue diagnosis prevents unnecessary and possibly
expensive antibiotic usage
3. Prompt diagnosis of index cases can facilitate vector control
activities in the community
so as to mitigate further transmission
4. Expanded use of accurate dengue diagnostics provides
important data on the
epidemiology and health burden of dengue
I. 4. Objectives
The objectives of writing this paper are to describe :
Comparison Non-Structural Protein NS1 sero-types specific Ig-G
with IgM dengue Blot
I. 5. Methods of Writing.
The writing of paper is carried out by a library research and
also via internet.
-
8/6/2019 English 3 2
6/18
6
I. 6. Frame of Writing
Preface .. 1
Contents .. 2
Abstract .. 3
CHAPTER I Introduction ...... 4
I. 1 Background ...... 4
I. 2 Problems ...... 4
I. 3 Limitation of the Problems.. 5
I. 4 Objectives ...... 5
I. 5 Methods of Writing ...... 5
I. 6 Frame of Writing ...... 5
CHAPTER II Dengue Virus ...... 6
II. 1 Morphology ...... 6
II. 2 Genome Organization .................. 7
II. 3
II. 4
Replication cycle
Antibody Responce
......................................................
..
7
7
CHAPTER III Comparison NS1 with IgM dengue blot .... 9
CHAPTER IV Conclusion .......... 14
BIBLIOGRAFI .. 16
-
8/6/2019 English 3 2
7/18
7
CHAPTER II
Dengue Virus
Dengue is caused by one of four closely related virus serotypes
of the genus Flavivirus, family
Flaviviridae, each serotype is sufficiently different that there
is no cross-protection and
epidemics caused by multiple serotypes (hyperendemicity) can
occur. The Dengue virus is a
member of the virus family Flaviviridae and is transmitted to
people through the bite of the
mosquitoesAedes aegypti andAedesalbopictus.
II. 1 Morphology of the Virus
Electron micrographs showed that dengue virions are
characterized by a relatively smooth
surface, with a diameter of approximately 500 , and an
electron-dense core surrounded by a
lipid bilayer. In addition to the plus-sense RNA genome of
10,700 nucleotides, there are three
structural proteins that occur in stoichiometric amounts in the
particle: core (C, 100 amino acids),
membrane (M, 75 amino acids), and envelope (E, 495 amino
acids).
II.2 Genome Organization of Dengue Virus
Dengue Virus (DV) belongs to the family Flaviviridae. The four
serotypes of dengue virus
(designated DEN-1, DEN-2, etc) can be distinguished by
serological methods. Infection in
humans by one serotype produces life-long immunity against
reinfection by that same serotype,
but only temporary and partial protection against the other
serotypes. Dengue viruses share many
characteristics with other flaviviruses, having a
single-stranded RNA genome surrounded by an
icosahedral nucleocapsid and covered by a lipid envelope. The
virion is approximately 50nm in
diameter. The flavivirus genome is approximately 11kb
(kilobases) in length, and the complete
genome sequence is known for isolates of all four serotypes of
dengue virus. The genome is
-
8/6/2019 English 3 2
8/18
8
composed of three structural protein genes, encoding the
nucleocapsid or core protein C, a
membrane-associated protein (M), an envelope protein (E) and
seven non-structural (NS) protein
genes. The domains responsible for neutralization, fusion and
interactions with virus receptors
are associated with the envelope protein. The order of proteins
encoded is 5-C-prM(M)-E-NS1-
NS2ANS2B- NS3-NS4A-NS4B-NS5-3. NS1, a glycoprotein is detected
in high titers in patients
with secondary dengue infections but its function is unknown.
NS2 region, is known to code for
2 proteins (NS2A and NS2B), which are assumed to play a role in
polyprotein processing. NS3,
the viral proteinase functions in the cytosol. NS4 region codes
for two small hydrophobic
proteins involved in the membrane bound RNA replication complex
establishment. NS5 codes
for a protein with a molecular weight of 105,000 and is the most
conserved flavivirus protein.
This protein is assumed to be the virus encoded RNA dependent
RNA polymerase. NS6 and NS7
function yet to be found.
A. Schematic of the single stranded RNA genome with highly
structured RNA elements in
the 5' and 3' NTRs.
B. DV genomic organization and functions of viral proteins. For
some proteins their
function in the viral life cycle is not yet established; they
are marked with a ?
C. Putative membrane topology of DV proteins and proteinases
involved in polyprotein
cleavage.
II.3 Dengue virus Replication cycle
Dengue virus (DV) particles bind to cells via interactions
between the surface glycoprotein and
one or several poorly defined cellular receptor(s). In addition,
particles may enter cells via Fc-
receptor upon opsonization. Virions are internalized by
receptor-mediated endocytosis resulting
in release of the viral genome from the nucleocapsid in a low pH
dependent manner. Soon after
infection, viral proteins induce rearrangments of intracellular
membranes forming distinct
structures that have designated vesicle packets and convoluted
membranes. It appears that
vesicle packets are sites of RNA replication that is probably
catalyzed by a multi-protein
-
8/6/2019 English 3 2
9/18
9
complex composed of viral proteins, cellular membranes and
presumably also cellular proteins.
DV RNA is replicated via a negative strand intermediate that
serves as a template for the
production of excess amounts of positive strand progeny. Virus
particles are thought to assemble
by budding into the ER and are transported through the host
secretory pathway.
Within the mosquito, the virus replicates during an extrinsic
incubation period of eight to twelve
days. The mosquito then bites a susceptible person and transmits
the virus to him or her, as well
as to every other susceptible person the mosquito bites for the
rest of its lifetime. The virus then
replicates in the second person and produces symptoms. The
symptoms begin to appear in an
average of four to seven days after the mosquito bite this is
the intrinsic incubation period, within
humans. While the intrinsic incubation period averages from four
to seven days, it can range
from three to 14 days also. The viremia begins slightly before
the onset of symptoms. Symptoms
caused by dengue infection may last for three to 10 days, with
an average of five days, after theonset of symptoms. So the illness
persists several days after the viremia has ended. Flaviviruses
vary widely in their pathogenic potential and mechanisms for
producing human disease.
However, it is useful to consider them in three major
categories: those associated primarily with
the encephalitis syndrome (prototype: St. Louis encephalitis),
with fever-arthralgia-rash
(prototype: dengue fever), or with hemorrhagic fever (prototype:
yellow fever). Human infection
with both mosquitoborne flaviviruses is initiated by deposition
of virus through the skin via the
saliva of an infected arthropod. Virus replicates locally and in
regional lymph nodes and results
in viremia.
Dengue viruses of all four serotypes cause three distinct
syndromes: classic dengue fever, dengue
hemorrhagic fever, and dengue shock syndrome. Although caused by
the same viruses, dengue
and dengue hemorrhagic fever are pathogenetically, clinically,
and epidemiologically distinct.
Dengue viruses appear to replicate in macrophages at the site of
the mosquito bite, in regional
lymph nodes, and then throughout the reticuloendothelial system.
Viremia is concurrent with
clinical illness. Virus is present in the serum and in
association with circulating monocytes.
Severe leukopenia is often present.
The mechanism by which flaviviruses enter the cells probably
involves an interaction between
the E protein and cellular receptors, followed by a
postattachment fusion event that occurs in
acidic intracytoplasmic vacuoles. Naked genomic RNA is
infectious if introduced into the
-
8/6/2019 English 3 2
10/18
10
cytoplasm. The genomic RNA is capped but not polyadenylated; it
serves as mRNA for all
proteins. Structural proteins are encoded at the 5' end of the
genome, and
nonstructural proteins (e.g., NS-1 and RNAdependent RNA
polymerase) are encoded in the
3'two-thirds. Complementary (negative-sense) RNA, made from
genomic RNA, serves as a
template to generate genomic RNA. Replication occurs in the
cytoplasm.
Virions are formed in perinuclear regions of the cytoplasm in
association with Golgi or smooth
membranes. Virions appear within cytoplasmic vacuoles and appear
to exit the cell as vacuoles
fuse with the plasma membrane. Unlike alpha viruses, no evidence
of budding has been seen in
flavivirus infected cells, and the mechanisms of virion assembly
and release remain obscure.
The 4 subtypes of dengue virus have 60-80% homology between each
other. The major
difference for humans lies in subtle differences in the surface
proteins of the different dengue
subtypes. After a person is infected with dengue, they develop
an immune response to thatdengue subtype. The immune response
produces specific antibodies to that subtypes surface
proteins that prevents the virus from binding to macrophage
cells (the target cell that dengue
viruses infect) and gaining entry. However, another type of
dengue virus infects the individual,
the virus will activate the immune system to attack the first
subtype. The immune system is
tricked because the 4 subtypes have very similar surface
antigens. The antibodies bind to the
surface proteins but do not inactivate the virus. The immune
response attracts numerous
macrophages, which the virus proceeds to infect because it has
not been inactivated. This
situation is referred to as Antibody-Dependent Enhancement (ADE)
of a viral infection. This
makes the viral infection much more acute. The body releases
cytokines that cause the
endothelial tissue to become permeable which results in
hemorrhagic fever and fluid loss from
the blood vessels.
II.4 Antibody Responce
Dengue infection will result in lifelong immunity to that
serotype, but only temporary immunity
to other serotypes.
-
8/6/2019 English 3 2
11/18
11
Primary Infection
1. IgM antibodies appear approximately 5 days after onset of
symptoms and rise for the next
1-3 weeks.
2. IgM antibodies detectable for up to 6 months.
3. IgG are detectable at approximately 14 days after onset of
symptoms and are maintained
for life.
Secondary Infection
Approximately 5% patients do not produce detectable levels of
specific IgM.
1. IgM titer can be slower to rise in secondary infection.2. IgG
appears approximately 2 days after symptoms appear.
3. IgG titre significantly higher in secondary infection.
The World Health Organization estimates that there may be 50 to
100 million cases of dengue
virus (DENV) infections worldwide every year, resulting in
250,000 to 500,000 cases of dengue
hemorrhagic fever (DHF) and approximately 25 000 deaths annually
(Guzman and Kouri, 2002;
Halstead, 2007; Kyle and Harris, 2008). Four serotypes of DENV
serotypes cause the disease in
humans (DENV-1 to DENV-4), producing a broad spectrum of
illnesses, which ranges from
asymptomatic infection, undifferentiated fever, and classic
dengue fever (DF) to the more severe
and sometimes fatal forms (DHF) and dengue shock syndrome (Deen
et al., 2006). In addition,
other nonclassic clinical forms has been described, such as
encephalitis and hepatitis (Deen et al.,
2006). One of the most challenging problems associated with
management of the infected patient
is to achieve a rapid and specific diagnosis of DENV infection
during the acute phase,
particularly in those countries where dengue coexists with other
acute tropical febrile illnesses,
presenting with similar symptoms and signs. Thus, a specific and
early diagnosis is determinant
to provide an adequate supportive and timely clinical treatment.
Currently virologic diagnostic
methodsare based on virus isolation or detection of viral RNA in
acute serum; however, both
methodologies are time consuming, expensive, and mainly
restricted to reference laboratories.
Serologic tests, which rely on the detection of DENV-specific
immunoglobulin M (IgM) and
-
8/6/2019 English 3 2
12/18
12
immunoglobulin G (IgG) antibodies by enzyme-linked immunosorbent
assay (ELISA), are more
commonly used for dengue diagnosis. During the acute phase, the
presence of IgM antibodies
alone suggests primary infection, whereas detection of both IgM
and IgG antibodies is
suggestive of secondary or later infection. Nevertheless,
detectable levels of IgM antibodies
appear approximately 4 to 6 days after the fever onset and
remains in serum for 90 days
afterward. This late and persistent IgM response, together with
the Flavivirus cross-reactivity,
restricts the efficacy of ELISA tests for the diagnosis of
dengue infections (WHO, 2000, 2007).
Several studies have shown that the DENV nonstructural 1 (NS1)
antigen, a highly conserved
glycoprotein, produced in both membrane-associated and secreted
forms, is abundant in the
serum of patients in the early stages of DENV infection. Because
of this, NS1 antigen constitutes
a suitable DENV biomarker, which can be detected before
seroconversion and, therefore,
represents a new approach for the diagnosis of acute dengue
infection (Alcon et al., 2002;Dussart et al., 2006; Libraty et al.,
2002; Xu et al., 2006; Young et al., 2000)
-
8/6/2019 English 3 2
13/18
-
8/6/2019 English 3 2
14/18
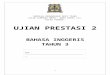
14
positive detection within the rst four days of illness. However,
the NS1 antigen-capture ELISA
has the added advantage of continuing to give good detection
rates up to seven days of the
illness. In this evaluation, the NS1 antigen-capture ELISA gave
a signi cantly higher detection
rate in acute primary dengue than in acute secondary dengue.
Despite the lower detection rate for
serum samples from patients with acute secondary dengue, the
Platelia NS1 antigen-capture
ELISA still gave a higher detection rate than the other dengue
diagnostic methods used in this
laboratory. Fig. 1 shows the positive detection rate of Platelia
NS1 antigen-capture ELISA,
which on the whole, gave a higher detection rate than the other
test methods at the various
sample ages. The sensitivity rate of IgM assay for early
diagnosis of dengue was poor in the rst
three days of the illness, notwithstanding the presence of
dengue speci c IgM was merely
indicative of recent dengue infection, and not con rmative of
acute dengue infection. The
nding of this evaluation shows that no dengue speci c IgM was
detected within the rst twodays of the fever and only 50% of
patients had detectable dengue IgM in their sera, even at the
fth post-fever day. Thus, the Platelia NS1 antigen-capture ELISA
should be considered as the
test of choice for patients suspected of acute dengue illness,
especially those with fever lasting
ve days or less. For those patients with a history of fever for
more than six days and are
suspected to have acute dengue infection, the test could also be
considered concurrently with an
assay of dengue specic IgM.
Fig. 1 Positive detection rate of each dengue test method with
respect to the sample age.
-
8/6/2019 English 3 2
15/18
15
The Platelia NS1 antigen-capture ELISA test has the prospect of
wide usage for early
diagnosis of acute dengue virus infection in dengue endemic
countries, since it uses the same
instruments as that of the dengue IgM-capture ELISA (MAC ELISA)
test, which is normally
carried out in the hospital diagnostic laboratories. This study
was limited by the lack of negative
controls to evaluate the speci city of the test kit. Further
work is ongoing to evaluate the speci
city of the Platelia NS1 antigen-capture ELISA kit and the
possibility of cross-reactivity with
NS1 antigens of other aviviruses. The possibility of a
correlation between a high level of
circulating dengue NS1 antigen with the occurrence of dengue
haemorrhagic fever, as
demonstrated by other studies, is also included in the ongoing
evaluation work.(18-20)
-
8/6/2019 English 3 2
16/18
16
Chapter IV
Conclusion
Early laboratory diagnosis of acute dengue virus infection still
remains a major problem
in many parts of the world especially in regions where dengue is
hyper-endemic but resources
are limited. Three basic methods used commonly by most
laboratories in resource rich countries
for the diagnosis of acute dengue virus infection are viral
isolation and identication, molecular
detection of viral genomic sequence by a nucleic acid
amplication assay, and detection of
dengue virus-specic IgM antibodies by IgM-capture enzyme-linked
immunosorbent assay
(MAC-ELISA) and/or rapid dengue immunochromatography test device
for detection of dengue
specic IgM. Although virus isolation and characterization are
considered the gold standard
for laboratory diagnosis of acute dengue virus infection, it is
expensive and at least 610 days are
required for the virus to replicate in tissue culture cells or
laboratory mosquitoes (adult or
larvae). Reverse transcriptase-polymerase chain reaction
(RT-PCR) is also an expensive method
and is not available widely, especially in hospital diagnostic
laboratories in developing countries.
The usefulness of anti-dengue specic IgM assays depends on the
time taken for the immuneresponse to produce IgM antibodies against
dengue virus antigens. Thus both rapid dengue
immunochromatography test device for detection of dengue specic
IgM (often considered as the
rapid test for the diagnosis of acute dengue infection) and
MAC-ELISA do not provide early
diagnosis of acute dengue infection, as in most cases the rst
detectable IgM only appears on
days 45 of the illness. A single serological detection of IgM is
merely indicative of a recent
exposure to dengue virus and should not be interpreted as a
diagnosis of acute infection without a
paired second serum sample for conrmation.
Recently, a highly sensitive and specic commercial dengue NS1
antigen-capture ELISA
kit has been evaluated and found to be better in comparison to
virus isolation and RT-PCR for
early laboratory conrmation of acute dengue virus infection
based on a single serum sample
(Kumarasamy et al., 2007). This NS1 antigen-capture ELISA has
the prospect of wide usage for
early diagnosis of acute dengue virus infection since it uses
the same instruments as for the
-
8/6/2019 English 3 2
17/18
17
dengue IgM-capture ELISA (MAC-ELISA). However, it is still
limited by the need for
sophisticated instrumentation and higher technical skill which
is normally only available in large
hospital diagnostic laboratories. A simple yet highly sensitive
and specic rapid dengue test that
does not require instrumentation will be highly desirable
for wide application to conrm acute dengue even in an outpatient
clinic setting or for
application in the eld. The nding of this study shows that the
rapid dengue NS1 antigen
immunochromatography test device meets the intended purpose.
With its high specicity
(99.5%) and positive predictive value (99.6%), this rapid
immunochromatography test device is
highly recommended for use in a dened population group with
clinical features suggestive of
acute dengue virus infection, but not as a routine screening
test for an asymptomatic population.
-
8/6/2019 English 3 2
18/18
18
Bibliografi
1. World Health Organization. Dengue haemorrhagic fever:
diagnosis,
treatment and control. Handbook of the World Health
Organization.
Geneva, 2000: 1-84.
2. Gubler DJ, Meltzer M. Impact of dengue/dengue hemorrhagic
fever
on the developing world. Adv Virus Res 1999; 53:35-70.
3. Gibbons RV, Vaughn DW. Dengue: an escalating problem. BMJ
2002;324:1563-6.
4. Monath TP, Heinz FX. Flaviviruses. In: Fields BW, Knipe DM,
Knipe
PM, Howley PM, eds. Fields Virology. Vol 1. 3rd ed.
Philadelphia:
Lippincott-Raven Press, 1996: 961-1034.
5. Henchal EA, Putnak JR. The dengue viruses. Clin Microbiol
Rev
1990; 3:376-96.
6. Schlesinger JJ, Brandriss MW, Putnak JR, Walsh EE. Cell
surface
expression of yellow fever virus non-structural glycoprotein
NS1:
consequences of interaction with antibody. J Gen Virol 1990;
71:593-9.
7. Mackenzie JM, Jones MK, Young PR. Immunolocalization of
the
dengue virus nonstructural glycoprotein NS1 suggests a role in
viral
RNA replication. Virology 1996; 220:232-40.