Embed Size (px)
Citation preview

Endothelial Effects of Hemostatic Devices for Continuous Cardioplegia or Minimally Invasive Operations L o u i s P. P e r r a u l t , M D , P h i l i p p e M e n a s c h 6 , M D , P h D , M i c h e l W a s s e f , M D ,
J e a n - P i e r r e B i d o u a r d , P h D , P h i l i p J a n i a k , D P h a r m , P h D , N i c o l e V i l l e n e u v e , P h D ,
C h r i s t i n e J a c q u e m i n , G 6 r a r d B l o c h , M D , J e a n - P a u l V i l a i n e , M D , a n d
P a u l M . V a n h o u t t e , M D , P h D
Cardiovascular Division, Institut de Recherches Servier, Suresnes; and Departments of Cardiovascular Surgery and Pathology, H6pital Lariboisi6re, Paris, France
Background. Improvements in myocardial protection may include the continuous delivery of normothermic blood cardioplegia. Technical aids are required for opti- mal visualization of the operative field during the per- formance of coronary anastomoses if cardioplegia is to be given continuously or during minimally invasive opera- tions. However, the effects of the different hemostatic devices on coronary endothelial function are unknown.
Methods. We compared the effects on endothelial func- tion of two commonly used hemostatic techniques, cor- onary clamping and gas jet insufflation, with those of a technique us ing extravascular bal loon occ lus ion to mimic systolic luminal closure by the surrounding myo- cardium. The three techniques were applied for 15 min- utes on porcine epicardial coronary arteries from ex- planted hearts. For coronary clamping, standard bulldog clamps were used. Gas jet insufflation was applied by blowing oxygen (12 L/min) tangentially at a 45-degree angle 1 cm away from a 3-mm arteriotomy. Extravascular balloon occlusion was achieved with a needle-tipped silicone loop, the midportion of which, once positioned beneath the coronary artery, was inflated to push a
myocardial "cushion" against the back of the vessel until its occlusion. Control rings were taken from the same coronary artery. The endothelial function of control and instrumented arterial rings was then studied in organ chambers filled with modified Krebs-Ringer bicarbonate solution.
Results. Contractions to potassium chloride and pros- t ag l and in F2c , and endothelium-independent relaxation to s in- l , a nitric oxide donor, were unaffected in all groups. Endothelium-dependent relaxation to serotonin was impaired after c lamping and preserved after gas jet insufflation and extravascular balloon occlusion. Maxi- mal endothelium-dependent relaxation to serotonin was as follows: for coronary clamping, 63% +-. 6% versus 87% - 3% in controls; for gas jet insufflation, 67% - 12% versus 88% --- 7%; and for extraluminal balloon occlu- sion, 79% + 6% versus 85% + 5%.
Conclusions. Whereas commonly used hemostatic de- vices may impair endothelial function, extravascular bal- loon occlusion appears to achieve effective hemostasis while preserving endothelial integrity.
(Ann Thorac Surg 1996;62:1158-63)
I mprovements in myocardial protection during cardiac operations include the continuous delivery of normo-
thermic blood cardioplegia through the antegrade route or the coronary sinus [1]. Technical aids are required for optimal visualization of the operative field during the performance of coronary anastomoses in the course of coronary artery bypass grafting without interrupting car- dioplegia delivery. Such aids are also required during the recently introduced minimally invasive operative revas- cularization techniques done without aortic cross- clamping when the operation is performed on the beat- ing heart with local isolation of the target blood vessel [2, 3]. The techniques in use include saline solution irriga- tion through a syringe, intraluminal occluders, gas jet
Accepted for publication May 18, 1996.
Address reprint requests to Dr Vanhnutte, lnstitut de Recherches [nter- nationales Servier, 6 place des Pl6iades 92415, Courbevnie, France.
insufflation [4], clamping of coronary arteries, and ex- travascular occlusion with silicone loops or polypro- pylene sutures. However, the effects of these hemostatic devices on coronary arterial endothelial function are unknown.
The purpose of this study was to compare the effects on endothelial integrity of two commonly used hemostatic techniques, coronary clamping and oxygen gas jet insuf- flation, with those of a system specifically designed for minimizing arterial injury using extravascular balloon occlusion.
Material and M e t h o d s
Operative Technique All experiments were performed using Large White swine of either sex, aged 8 _+ I weeks and weighing 23 _+ 2 kg. Animals were treated in compliance with the
© 1996 by The Society of Thoracic Surgeons 0003-4975/961515.00 Published by Elsevier Science Inc Pll S0003-4975(96)00536-X

Ann Thorac Surg PERRAULT ET AL 1159 1996;62:1158-63 ENDOTHELIAL EFFECTS OF HEMOSTATIC DEVICES
f J
Fiy, 1. Extraluminal balloon occluder ¢69% qf actual size).
"Guide for the Care and Use of Laboratory Animals" publ i shed by the National Insti tutes of Health (NIH publicat ion 85-23, revised 1985). After anesthesia with a mixture of t i le tamine and zo lazepam (15 mg/kg) injected i n t r amuscu l a r l y , the hea r t s were r e m o v e d r a p i d l y through a left thoracotomy and placed in modif ied Krebs-b ica rbona te solut ion (composi t ion in mmol/L: NaC1, 118.3; KC1, 4.7; MgSO4, 1.2; KH2PO4, 1.2; glucose, 11.1; CaC12, 2.5; NaHCO3, 25; and calcium ethylenedia- mine tetraacetic acid, 0.026 [control solution]). Oxygen- ation was ensured using a carbogen mixture (95% 0 2 and 5% CO2). For coronary c lamping and gas jet insufflation, the coronary arteries were dissected from the myocar- d ium and placed in a silicone dish before appl icat ion of the devices. Extraluminal bal loon occlusion was appl ied on the hear t immersed in physiologic solution before dissection of the coronary artery. The three hemostat ic devices were app l ied for 15 minutes to mimic a longer than average durat ion of coronary anastomosis . Proximal epicardial segments of the left anterior descending, cir- cumflex, and right coronary arteries were used randomly.
Experimental Groups
In the coronary, c lamping group (n = 9), a vascular b u l l d o g c l a m p (no. 19-8090; C o d m a n , C h a t e n a y - Malabray, France) was app l ied before the removal of epicardial fat to s imulate the per ivascular cushion seen in clinical practice. The force needed to displace the jaws of the clamp more than 1 m m was 80 g. In the gas jet insufflation group (n = 7), oxygen insufflation at a mean flow of 12 L/min was app l ied tangent ia l ly at a 45-degree angle 1 cm away from a 3-mm coronary ar ter io tomy using a Visuflo surgical site visualization wand (Research Medical Inc, Midvale, UT). Endothel ial function studies were per formed on segments 3 m m proximal and distal, but not contiguous, to the arter iotomy. In some rings (n - 6), gas insufflation was appl ied directly in the lumen to s tudy the effect of endolumina l gas delivery.
In the extravascular bal loon occlusion group (n = 8), the extraluminal bal loon occluder (Quest Medical, Allen, TX) consis ted of a silicone loop moun ted with a b lunt half-circle 1-cm long needle with a 3-cm long balloon, 3 ml in volume, in its midsect ion (Fig 1). The occluder was appl ied by passage of the needle with a needle holder through the myocard ium under the coronary ar tery at an approximate depth of 5 mm, and the silicone bal loon was pos i t ioned symmetr ica l ly on both sides of the vessel. The bal loon was initially inflated with 2.5 mL of air or saline, and coronary occlusion was confirmed using gentle irri- gation with physiologic solution through the coronary vessel under study. After the occlusion period, the coro- nary artery was dissected free from the myocard ium and divided into 4-mm rings, including the ins t rumented
rings (with devices). Control rings were taken from the same coronary artery.
Endothelial Function
The endothel ia l function of control and ins t rumented arterial r ings was s tudied in organ chambers filled with control solution (20 mL). Responses to potass ium chlo- ride, serotonin, and sin-1 (3-morpholino sydnonimine , a nitric oxide donor) were compared. All s tudies were per formed in the presence of indomethac in (10 5 mol/L, to exclude the product ion of endogenous prostanoids) , propranolol (10 7 mol/L, to prevent the activation of ]3-adrenergic receptors), and ketanser in (10 6 mol/L, to block serotonin 5HT-2 receptors). Each prepara t ion was s t re tched to the point of its active length curve (usually 4 g), as de te rmined by measur ing the contraction to potass ium chloride (30 mmol/L) at different levels of stretch, and then stabil ized for 90 minutes. The maximal contraction was de te rmined with potass ium chloride. After washing and a 30-minute stabil ization period, pros- t a g l a n d i n F2, ~ (range, 2 × 10 a to 10 ~ mol/L) was a d d e d to achieve a contraction averaging 50% to 70% of the maximal contract ion to KC1 (60 mmol/L). Ketanser in was incubated 40 minutes before the addi t ion of serotonin (10 10 to 10 ~ mol/L). Endo the l ium- independen t func- tion was s tudied using increasing concentrat ions of sin-1 (10 9 to 10 s mol/L). Before sin-1 was appl ied, the endothe l ium was gently removed by rubbing the luminal surface of the r ing with a small wooden stick.
Morphologic Studies
Silver nitrate staining was used to evaluate the endothe- lial cell coverage. Staining was pe r fo rmed immedia te ly after appl icat ion of the hemostat ic devices for 15 minutes. Coronary ar tery rings were opened longi tudinal ly and p inned down on a silicone dish under a small amount of tension to ensure a uniform surface. Silver ni trate stain- ing was per formed for each set of r ings (n = 6). Evalua- tion of endothel ia l coverage was pe r fo rmed by an inde- pe nde n t evaluator. The protocol was as follows. The rings were first fixed for 10 minutes with buffered paraformal- dehyde 4%. The rings were then washed for 1 minute with a HEPES sucrose buffer solution. Silver nitrate 0.25% was app l ied for I minute. Wash ing was pe r fo rmed for 1 minute before a second fixation for 2 minutes. The rings were exposed to light for 24 hours in a cacodylate buffer solution. En face endothel ia l p repara t ions of cor- onary artery segments were made and examined under the light microscope. Microphotographs of representa- tive areas were taken.
Light microscopic examinat ion with Masson t r ichrome staining was pe r fo rmed on the myocard ium sur rounding the coronary, artery, (left anter ior descending artery), under which the extravascular bal loon occlusion device

1160 PERRAULT ET AL Ann Thorac Surg ENDOTHELIAL EFFECTS OF HEMOSTATIC DEVICES 1996;62:1158-63
Table 1. Contraction and Relaxation Results in Coronary Arteries After Clamping, Gas Jet hlsufflation, and Extravascular Balloon Occlusion"
Clamp Clamp Gas Jet Balloon Result (n 9) Control (n 7) Gas Control (n = 8) Balloon Control
KC1 contraction (g) PGF2, ~ contraction (g) EDso serotonin (mol/L) Maximal relaxation to serotonin (%)
8.9 + 3.8 7.6 - 2.5 Z1 ~ 2.8 6 -+ 4 8.3 ~ 2 10 + 3 3.9 + 2 4.6 ~ 2.1 2.8 -+ 1.2 2.8 -+ 1.7 3 + 1.7 3.1 - 1.8
2.01 × 10 ~ 1.94× 10 ~ 2.22× 10 ~ 2.89× 10 9 9.16×10 9 1.44× 10 ~ 62.7 - 6 . 5 b 86.5 ÷ 3.2 66.6 _+ 12.5 ' 88 _+ 6.7 79.4 -+ 6 . 4 a 84.8 -- 4.5
~ Data are shown as mean + standard error ot the mean. control
EDs~ ~ --~ effective dose of serotonin for 50",, relaxation;
b p _~ 0.01 versus control.
PG prostaglandin.
p - 0.03 versus control. 3 p 0.3 (not significant) versus
was appl ied . The device was app l i ed in three dis t inct s i tuat ions: (1) af ter passage of the n e e d l e and loop wi thou t inf la t ion on an explan ted , n o n r e p e r f u s e d heart; (2) af ter 15 m i n u t e s of inf la t ion on an explan ted , non- r e p e r f u s e d heart ; and (3) af ter 15 minu t e s of inf la t ion on a bea t i ng hear t and 30 minu t e s of r epe r fus ion after def la t ion of the occluder .
Drugs All solutions were p repa red daily. F ive-hydroxyt ryptamine c rea t in ine sulfate (serotonin) , p ros t ag land in F2,~, ke tan- serin, i ndome thac in , and p r o p r a n o l o l w e r e p u r c h a s e d f rom Sigma C h e m i c a l Co (St. Q u e n t i n Falavier , France). Sin-1 was syn thes i zed at the Serv ie r Research Insti tute.
Statistical Analysis Rings w e r e exc luded if they failed to contract to potas- s ium chlor ide (exclusion rate less than 10%). Relaxat ion was ca lcu la ted as a p e r c e n t a g e of max ima l cont rac t ion for each g roup and was exp re s sed as m e a n ÷ s t anda rd e r ror of the mean; n refers to the n u m b e r of an ima l s s tudied. S t u d e n t ' s t test for pa i r ed or u n p a i r e d obse rva t ions was used for statist ical analysis . A p va lue of less than 0.05 was cons ide r ed significant . Analys is of va r i ance was p e r f o r m e d to c o m p a r e d o s e - r e s p o n s e curves. The N e w - m a n - K e u l s test was used as the post hoc test.
Results
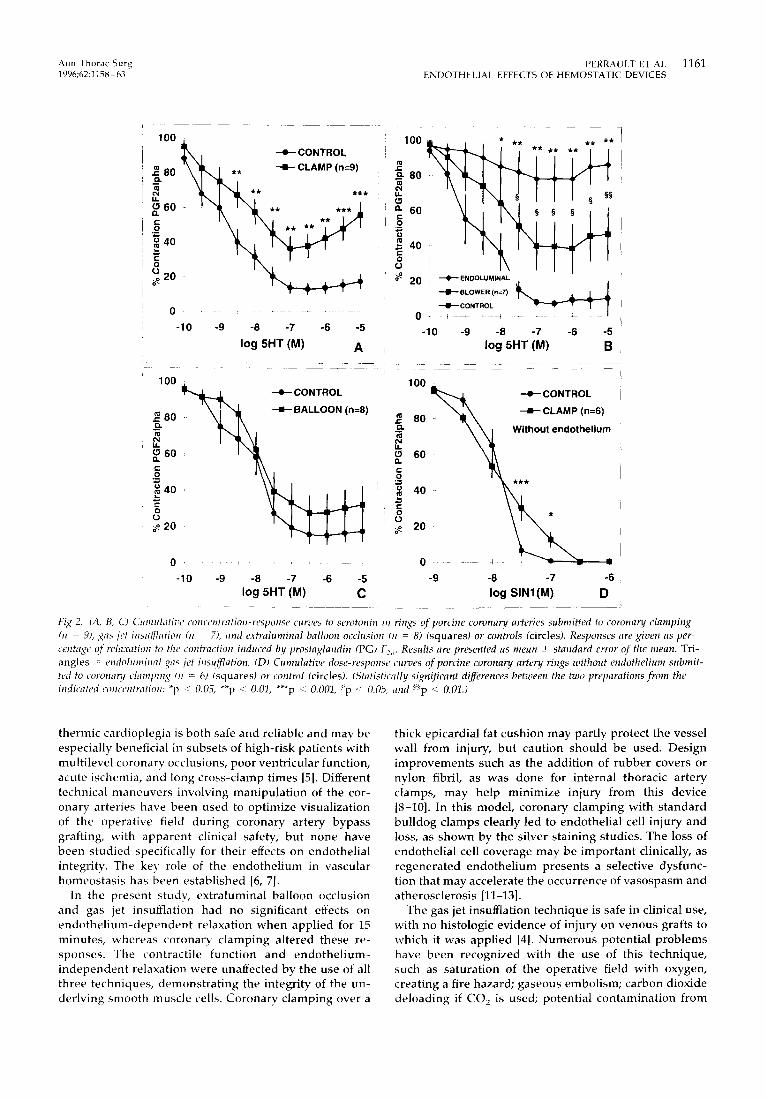
Endothelial Function There w e r e no dif ferences in the a m p l i t u d e of contrac- t ions to p o t a s s i u m chlor ide and p ros t ag l and in F 2 , ~ be- t w e e n the i n s t r u m e n t e d r ings or the cont ro l g roup (Table 1). Max ima l re laxat ion to se ro ton in was s ignif icant ly lower in the co ronary c l a m p i n g g roup than in controls . Max ima l re laxat ion was s ignif icant ly l ower in the gas jet insufflat ion g roup c o m p a r e d wi th controls . The re was no di f ference in m a x i m a l re laxat ion b e t w e e n the ex t ravascu- lar ba l loon occ lus ion g roup and controls (see Table 1).
C o r o n a r y r ings s u b m i t t e d to c l a m p i n g s h o w e d a sig- nif icant r educ t ion in re laxat ion to se ro ton in c o m p a r e d wi th controls (Fig 2A). C o r o n a r y r ings s u b m i t t e d to gas jet insufflat ion s h o w e d no s ignif icant r educ t ion of the re laxat ion to se ro ton in overal l c o m p a r e d wi th control rings. E n d o l u m i n a l appl ica t ion of the gas jet insufflator caused a s ignif icant r educ t ion in the re laxat ion to sero-
ton in c o m p a r e d wi th i n s t r u m e n t e d r ings and control r ings (Fig 2B). The re w e r e no dif ferences in the re laxa t ion to se ro ton in b e t w e e n r ings s u b m i t t e d to the ex t ravascu- lar ba l loon occ lus ion and controls (Fig 2C).
Co rona ry a r te ry r ings w i thou t e n d o t h e l i u m s u b m i t t e d to c l a m p i n g s h o w e d a s ignif icant r educ t ion of re laxat ion to sin-1 at two concentrations. There was no difference in maximal e n d o t h e l i u m - i n d e p e n d e n t relaxation to sin-1 be- tween the coronary c lamping group and controls (Fig 2D).
Histologic Findings C o r o n a r y r ings s u b m i t t e d to co ronary c l a m p i n g s h o w e d m a r k e d endo the l i a l cell loss, wi th noncon f luen t is lands of endo the l i a l cells s e p a r a t e d by d e n u d e d areas (Fig 3A). C o r o n a r y ar tery r ings exposed to gas jet insuff iat ion and to ex t ravascu la r ba l loon occlus ion s h o w e d m i n i m a l d a m - age, wi th p re se rva t ion of endo the l i a l con t inu i ty and a rch i tec tu re (Figs 3B, 3C).
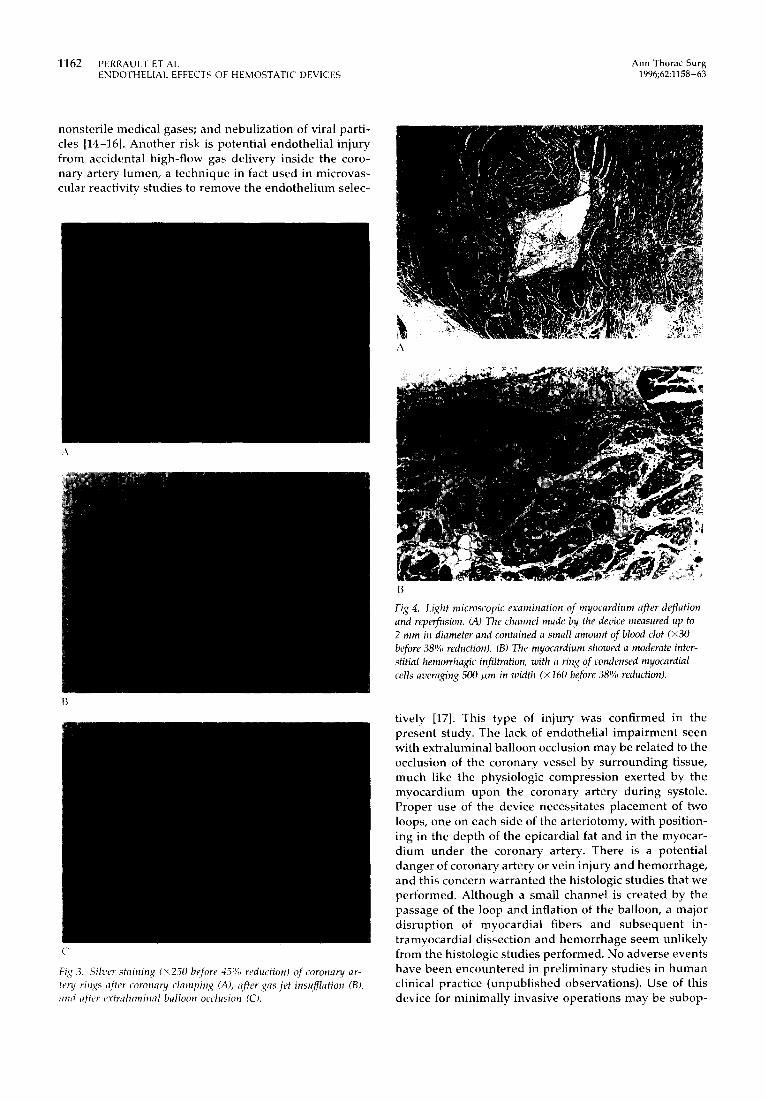
In the first expe r imen t , the channe l c rea ted by the non in f l a t ed dev ice m e a s u r e d 0.5 to 1.5 m m in he igh t and 50 to 100/zm in width; the over ly ing a r te ry and ve in were intact and the re was m i n i m a l d i s rup t ion of the myoca r - d ium. In the second expe r imen t , af ter inf la t ion of the bal loon, the channe l m e a s u r e d 2.7 to 4 m m in he igh t and up to 0.5 m m in wid th and was s u r r o u n d e d by an a rea of c o n d e n s e d m y o c a r d i u m up to 0.8 m m thick. The a r te ry was intact, and there was d i s rup t ion of a smal l ep icard ia l vein. In the th i rd expe r imen t , af ter def la t ion and repe r - fusion, the channe l m a d e by the device m e a s u r e d up to 2 m m in d i a m e t e r and was fi l led wi th a smal l a m o u n t of b lood clot (Fig 4A). The m y o c a r d i u m s h o w e d a m o d e r a t e interst i t ia l h e m o r r h a g i c infi l trat ion, wi th a r ing of con- d e n s e d myocard ia l cells a v e r a g i n g 500 ~ m in w id th (Fig 4B). An in t r amyoca rd i a l ve in s h o w e d a recen t t h r o m b o - sis, bu t ep icard ia l vessels were free of les ions (see Fig 4B).
C o m m e n t
Obs t ruc t ion of the opera t ive field d u r i n g p e r f o r m a n c e of co ronary a n a s t o m o s e s for co ronary a r te ry bypass graft- ing may occur wi th the use of any ca rd iopro tec t ive t e c h n i q u e because of med ia s t i na l col lateral flow. It is m o r e of ten e n c o u n t e r e d wi th the use of n o r m o t h e r m i c con t i nuous ca rd iop leg ia de l ive ry t h r o u g h e i the r the an- t eg rade or r e t r og rade route. A l t h o u g h its super io r i ty is not c lear ly e s t ab l i shed in all clinical s i tuat ions, n o r m o -
A n n T h o r a c S u r g P E R R A U L T E T A L 1161 1 9 9 6 ; 6 2 : 1 1 5 8 - 6 3 E N D O T H E L I A L E F F E C T S O F H E M O S T A T I C D E V I C E S
100 - ~ l -e--CONTROL
\TW; n ~ 60 - * *
~ 40
0 ~ 20
-10 -9 -8 -7 -6 -5
log 5HT (M) A ,
1 O0 , --e--CONTROL
~ 8 0 = )
~ 40
(.1 g 20
0 " • , . . . . . . .
-10 -9 -8 -7 -6 -5 log 5HT (M) C
100 * * * * * * * * * * * * *
e- "°
4o O
0
o~ 20 * • ENDOLUMINAL d I
BLOWER (n=7) ~ JL . L ~ L
~ CONTROL ~ ~ ' I I 0 i ~ ~ ~ F - - ~ ~
!
-10 -9 -8 -7 -6 -5 log 5HT (M) B
1 O0 -=e-- CONTROL
80" ~ . ~ Without endothelium U .
~ so
,~ 40
~ 20
0 - ~ ~ . . . . -
-9 -8 -7 -6 log SINI(M) D
Fig 2. (,4, B, (_=~ Cumulative concentration-response curves to serotonin m rings of porcine coronary arteries submitted to coronary clamping (n 9), gas/et insl(~ation (n - 7), and extraluminal balloon occlusion (n = 8) (squares) or controls (circles). Responses are given as per- centage of relaxation to the contraction induced by prostaglandin (PG) F2,. Results are presented as mean ++_ standard error of the mean. Tri- angles - endohmlinal gas jet inst(~ation. (D) Cumulative dose-response curves qf porcine coronary artery rings without endothelium submit- ted to coronar~t clamping ¢n = 6) (squaresJ or control (circles). (Sh#istically significant differences between the two preparations from the indicated concentration: *p --~ 0.05, **p <: 0.01, ***p ~ 0.001, ~p < 0.05, and ~p < 0.01.)
thermic cardioplegia is both safe and reliable and may be especially beneficial in subsets of high-risk patients with multilevel coronary occlusions, poor ventricular function, acute ischemia, and long cross-clamp times [5]. Different technical maneuvers involving manipulation of the cor- onary arteries have been used to optimize visualization of the operative field during coronary artery bypass grafting, with apparent clinical safety,, but none have been studied specifically for their effects on endothelial integrity. The key role of the endothelium in vascular homeostasis has been established [6, 7].
In the present study, extraluminal balloon occlusion and gas jet insufflation had no significant effects on endothel ium-dependent relaxation when applied for 15 minutes, whereas coronary clamping altered these re- sponses. The contractile function and endothel ium- independent relaxation were unaffected by the use of all three techniques, demonstrat ing the integrity, of the un- derlying smooth muscle cells. Coronary clamping over a
thick epicardial fat cushion may partly protect the vessel wall from injury, but caution should be used. Design improvements such as the addition of rubber covers or nylon fibril, as was done for internal thoracic artery clamps, may help minimize injury from this device [8-10]. In this model, coronary clamping with standard bulldog clamps clearly led to endothelial cell injury and loss, as shown by the silver staining studies. The loss of endothelial cell coverage may be important clinically, as regenerated endothel ium presents a selective dysfunc- tion that may accelerate the occurrence of vasospasm and atherosclerosis [11-13].
The gas jet insufflation technique is safe in clinical use, with no histologic evidence of injury on venous grafts to which it was applied [4]. Numerous potential problems have been recognized with the use of this technique, such as saturation of the operative field with oxygen, creating a fire hazard; gaseous embolism; carbon dioxide deloading if CO2 is used; potential contamination from
1162 PERRAULT ET AL Ann Thorac Surg ENDOTHELIAL EFFECTS OF HEMOSTATIC DEVICES 1996;62:1158-63
nonsterile medical gases; and nebulization of viral parti- cles [14-16]. Another risk is potential endothelial injury from accidental high-flow gas delivery inside the coro- nary artery lumen, a technique in fact used in microvas- cular reactivity studies to remove the endothelium selec-
A
C
Fig .3. Silver staining (>;250 before 45% reduction) of coronary, ar- tery rings ~flter coronary clamping (A), after gas jet insu~lation (BL and ~fter extraluminal balloon occlusion (C).
t
B
Fig 4. Light microscopic examination qf myocardium after deflation and reperfusion. (A) The channel made by the device measured up to 2 mm in diameter and contained a small amount of blood clot (×30 before 38% reduction). (B) The myocardium showed a moderate inter- stitial hemorrhagic infiltration, with a ring q]: condensed myocardial cells averaging 500 ttm in width (× 160 before 38% reduction).
tively [17]. This type of injury, was confirmed in the present study. The lack of endothelial impairment seen with extraluminal balloon occlusion may be related to the occlusion of the coronary vessel by surrounding tissue, much like the physiologic compression exerted by the myocardium upon the coronary, artery during systole. Proper use of the device necessitates placement of two loops, one on each side of the arteriotomy, with position- ing in the depth of the epicardial fat and in the myocar- dium under the coronary artery. There is a potential danger of coronary artery or vein injury and hemorrhage, and this concern warranted the histologic studies that we performed. Although a small channel is created by the passage of the loop and inflation of the balloon, a major disruption of myocardial fibers and subsequent in- tramyocardial dissection and hemorrhage seem unlikely from the histologic studies performed. No adverse events have been encountered in preliminary studies in human clinical practice (unpublished observations). Use of this device for minimally invasive operations may be subop-

Ann Thorac Surg PERRAULT ET AL 1163 1996;62:1158-63 ENDOTHELIAL EFFECTS OF HEMOSTATIC DEVICES
timal because the beat ing heart creates progressive dis- lodgment of the balloon and, subsequently, incomplete hemostasis.
Other techniques are used to ensure hemostasis dur- ing the performance of anastomosis. Among them, the traditional endoluminal balloon occluder placed inside the lumen has the potential for causing endothelial denudat ion because of the unavoidable contact with the vessel lumen. Other disadvantages include encroach- ment in the operative field and the potential for incom- plete occlusion and easy dislodgment. Techniques such as looping and snar ing of the coronary artery with a polypropylene suture and interposition of a pledget or a small piece of silicone tubing are currently in use in minimal ly invasive operations. Saline irrigation can be effective for improving visualization, although it requires constant application and carries the risk of hemodilut ion if large volumes are used.
Obvious limitations exist in this model. First, the use of an explanted, nonperfused heart may not provide the same tissue turgor as the heart under cont inuous car- dioplegic arrest and perfusion. However, the use of the explanted heart model has the advantage of ensur ing gentle application of the device and precise identification of the coronary segment to which it was applied. Al- though placement of the devices upon dissected, ex- planted coronary arteries may cause injury because of the additional manipula t ion required, this was controlled for by using control rings from the same coronary artery near the site where the device was applied. In addition, the young swine heart has minimal epicardial fat com- pared with the human adult heart, which may offer more protection from application of the coronary clamp. In the case of gas jet insufflation, because the study technique necessitated complete coronary artery rings, the ring bearing the arteriotorny could not be studied. However, nearby rings did show signs of endothelial dysfunction, as evidenced by lower maximal endo the l ium-dependen t relaxation. This finding was surprising considering that the gas stream was applied at a distance from the endothelial surface. Small amounts of gas may reach the lumen of the artery through the arteriotomy and alter endothelial function. Blood flowing through the arteriot- omy may prevent this, although a sufficiently forceful gas flow may still permit gas to reach the arterial lumen. Different gases and different flow rates applied for shorter periods may produce less injury. Finally, the inflation volumes used to fill the balloon of the extravas- cular occluding device and thus, the compressive forces exerted upon the coronary artery to produce complete occlusion in a nonperfused heart, may be smaller than those needed during cont inuous cardioplegia delivery or normal coronary perfusion. We did, however, confirm complete occlusion of the artery by testing saline injec- tion dur ing inflation of the balloon.
In conclusion, different hemostatic techniques are used for optimal visualization of the coronary artery in the course of coronary artery bypass grafting during contin- uous deliver), of cardioplegia or when the operation is performed on the beating heart with local isolation of the
target vessel. Potential complications may be avoided through knowledge of the effects of the devices on coronary endothelial function. The results of the present study suggest that coronary clamping and gas jet insuf- flation techniques may impair endothel ial function, whereas extravascular balloon occlusion, which mimics the physiologic systolic compression, may achieve effec- tive hemostasis while preserving endothelial integrity.
We are thankful to Catherine Gitton-Canovi and Isabelle Deles- cluse for technical assistance, to Corinne Thomas-Haimez and Lisa Maiofiss for the statistical work and to Roselyne Prioux for aid in preparation of the manuscript.
Doctor Perrault is supported by the Clinician-Scientist program from the Medical Research Council of Canada.
References
1. Lichtenstein SV, Ashe KA, El Dalati H, Cusimano RJ, Panos A, Slutski AS. Warm heart surgery. J Thorac Cardiovasc Surg 1991;101:269-74.
2. Subramanian VA, Sani G, Benetti FJ, Calafiore AM. Mini- mally invasive coronary bypass surgery: a multi-center re- port of preliminary clinical experience IAbstract]. Circula- tion 1995;92(Suppl 1):645.
3. Pirk J, Kellovsky P. An alternative to cardioplegia. Ann Thorac Surg 1995;60:464-5.
4. Teoh KHT, Panos AL, Harmantas AA, Lichtenstein SV, Salerno TA. Optimal visualization of coronary artery, anas- tomoses by gas jet. Ann Thorac Surg 1991;52:564.
5. Lichtenstein SV, Abel JG, Panos A, Slutsky AS, Salerno TA. Warm heart surgery: experience with long cross-clamp times. Ann Thorac Surg 1991;52:1009-13.
6. Furchgott RF, Vanhoutte PM. Endothelium-derived relaxing and contracting factors. FASEB J 1989;3:2007-18.
7. Vanhoutte PM. The endothelium--modulator of vascular smooth-muscle tone. N Engl J Med 1988;319:412-3.
8. Fonger JD, Yang XM, Cohen RA, Haudenschild CC, Shernin RJ. Human mammary artery endothelial sparing with fi- brous jaw clamping. Ann Thorac Surg 1995;60:551-5.
9. Fonger JD, Yang XM, Cohen RA, Haudenschild CC, Shemin RJ. Impaired relaxation of the human mammary artery after temporary clamping. J Thorac Cardiovasc Surg 1992;104: 966-71.
10. Kuo J, Ramstead K, Coumbe A, Graham TR, Lewis CT. Effect of vascular clamp on endothelial integrity of the internal mammary artery. Ann Thorac Surg 1993;55:923-6.
11. Shimokawa H, Aarhus L, Vanhoutte PM. Porcine coronary arteries with regenerated endothelium have a reduced en- dothelium-dependent responsiveness to aggregating plate- lets and serotonin. Circ Res 1987;61:256-70.
12. Lin PJ, Pearson PJ, Cartier R, Schaff HV. Superoxide anion mediates the endothelium-dependent contractions to sero- tonin by regenerated endothelium, J Thorac Cardiovasc Surg 1991;102:378-85.
13. Cartier R, Pearson PJ, Lin PJ, Schaff HV. Time course and extent of recovery of endothelium-dependent contractions and relaxations after direct arterial injury. J Thorac Cardio- vasc Surg 1991;102:371-7.
14. Pulton TJ. Optimal visualization of coronary artery anasto- moses by gas jet [Letter]. Ann Thorac Surg 1992;54:598-9.
15. Bognolo G, Bognolo DA, Chiariello L. Use of CO 2 blower for internal mammary artery harvesting. Ann Thorac Surg 1995; 59:1025.
16. Sasaguri S, Hosoda Y, Yamamoto S. Carbon dioxide gas blow for the safe visualization of coronary artery anastomo- sis [Letter]. Ann Thorac Surg 1995;60:1861.
17. Bjorling DE, Saban R, Tengowski MW, Gruel SM, Rao VK. Removal of venous endothelium with air. J Pharmacol Toxi- col Methods 1992;28:149-57.





























