Embed Size (px)
Citation preview

Istituto Clinico HUMANITAS Milano
Endotelio Corneale
Dott. Pietro Rosetta
www.o
opi.it

EDEMA CORNEALE
ENDOTELIOPATIE SECONDARIE SHOCK CHIRURGICO
DISTROFIE PRIMARIE
TERAPIA:
Farmacologica
DSAEK DMEK
Endotelio corneale
www.o
opi.it

VALUTAZIONE QUANTITATIVA Popolazione normale 350.000/500.000
Densità cell/mm2 > 2000 cell/mm2 Perdita annuale 100-500 cell/mm2
Endothelial Cell Density by Age
Age
Average Endothelial Cell Density (cells/mm2)
10 - 19 2,900 - 3,500
20 - 29 2,600 - 3,400
30 - 39 2,400 - 3,200
40 - 49 2,300 - 3,100
50 - 59 2,100 - 2,900
60 - 69 2,000 - 2,800
70 - 79 1,800 - 2,600
80 - 89 1,500 - 2,300
Amann J, et al. Increased endothelial cell density in the paracentral and peripheral regions of the human cornea. Am J Ophthalmol 135:584, 2003 ww
w.oopi.it

DENSITA’ ATTENDIBILE ?
CD 2700 cell/mm2
CD 1600 cell/mm2
CD 1100 cell/mm2
CD non eseguibile
CD non eseguibile
CD ≥ 300 and 500 cells/mm2 ? Spesso conta non è eseguibile ww
w.oopi.it

Konan Specular Microscope Photographic field 0.1 mm2
CD=2437 CV=31
A B
C
= central A = 0.5mm (1mm dia.) B = 1mm (2mm dia.) C = 2mm (4mm dia.)
Center image
A
B
C
www.o
opi.it
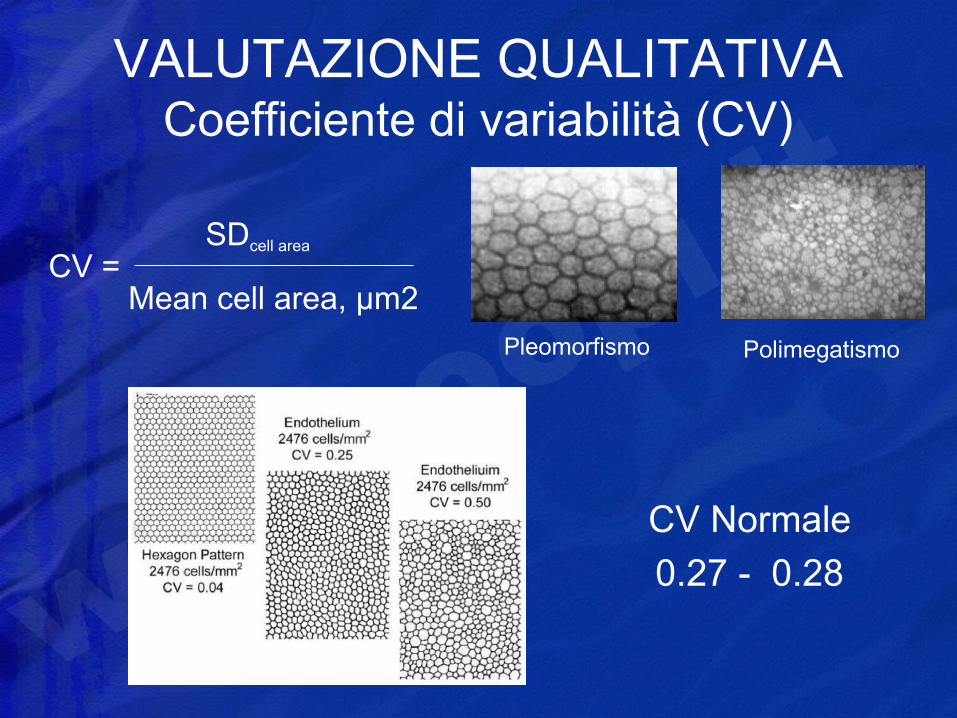
VALUTAZIONE QUALITATIVA Coefficiente di variabilità (CV)
Pleomorfismo Polimegatismo
CV = Mean cell area, µm2
SDcell area
CV Normale 0.27 - 0.28 ww
w.oopi.it

Polimegatismo
CV=45 CD=3268 CV=76 CD=2967 CV=58 CD=3121
Endothelial Cell Changes Caused by Contact Lenses Schoessler; J Am Opto Assoc. 58(10):804-810, 1987
LAC polimegatismo scarsamente reversibile www.o
opi.it
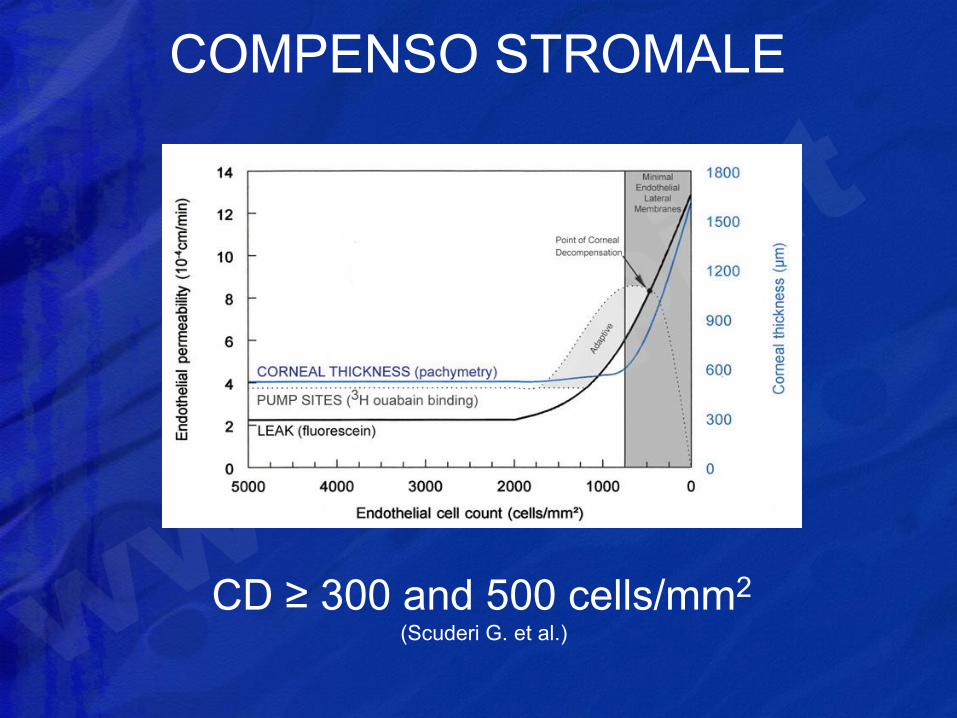
COMPENSO STROMALE
CD ≥ 300 and 500 cells/mm2 (Scuderi G. et al.)
www.o
opi.it

Trofismo vs Compenso
CD 637 cell/mm2 CD 988 cell/mm2 www.o
opi.it

• CORNEA GUTTATA
• DISTROFIA ENDOTELIALE DI FUCHS
EZIOLOGIA: ENDOTELIOPATIE PRIMARIE
ERNST FUCHS 1910 • ICE: IRIDOCORNEAL ENDOTHELIAL SYNDROME www.o
opi.it

DISTROFIA ENDOTELIALE DI FUCHS
Bergmanson et al.40 examined histopathologic sections of FECD corneas and detected that aberrant deposition of extracellular matrix caused stretching and thinning of CE cells positioned on top of guttae. ww
w.oopi.it

• POST-CHIRURGICHE chirurgia refrattiva e CXL chirurgia vitreoretinica estrazione di cataratta trapianto di cornea
• CHERATITI STROMALI da agenti fisici (traumi) da agenti chimici (farmaci) da agenti biologici (infezioni, cheratite disciforme)
• GLAUCOMA ACUTO
EZIOLOGIA: ENDOTELIOPATIE SECONDARIE
www.o
opi.it

EDEMA POST-CHIRURGICO
• Fisico Turbolenza in c.a. Trauma diretto circoscritto IOP elevata – Ipossia Ustione Ipotermia Danno epiteliale • Chimico Inibizione Na/K-ATPase da farmaci Ph PDMS
•Danno diretto perdita endoteliale
•Localizzazione del danno
• Biologico Facoanafilassi Sepsi Uveite Vitreo in c.a.
www.o
opi.it

Strategia terapeutica
• Intolleranza alle LAC: rimuovere LAC
• Flogosi: uso di steroidi antinfiammatori topici
• IOP elevata: farmaci antiglaucomatosi
• Vitreo in c.a.: vitrectomia
• Lacuna endoteliale circoscritta: attendere flusso migratorio
Terapia farmacologica iperosmolare
Vicaria la ridotta funzione di pompa
www.o
opi.it

TERAPIA CHIRURGICA
• DSAEK • DMEK Price FW Jr, Price MO. Descemet's stripping with endothelial
keratoplasty in 200 eyes: Early challenges and techniques to enhance donor adherence. J Refract Surg. 2006;32:411–8.
Terry MA. Endothelial keratoplasty: history, current state, and future directions. Cornea. 2006;25:873–8.
• CXL Ghanem RC, Santhiago MR, Berti TB, Thomaz S, Netto MV. Collagen crosslinking with riboflavin and ultraviolet-A in eyes with pseudophakic bullous keratopathy. J Cataract Refract Surg. 2010;36:273–6. Wollensak G, Aurich H, Wirbelauer C, Pham DT. Potential use of riboflavin/UVA cross-linking in bullous keratopathy. Ophthalmic Res. 2009;41:114–7. Krueger RR, Ramos-Esteban JC, Kanellopoulos AJ. Staged intrastromal delivery of riboflavin with UVA cross-linking in advanced bullous keratopathy: laboratory investigation and first clinical case. J Refract Surg. 2008;24:S730–6. Hafezi F, Dejica P, Majo F. Modified corneal collagen crosslinking reduces corneal oedema and
diurnal visual fluctuations in Fuchs dystrophy. Br J Ophthalmol. 2010 May;94(5):660-1.
• PK (Fachico) Rate and risk factors for cataract formation and extraction after
Descemet stripping endothelial keratoplasty. Price MO, Price DA, Fairchild KM, Price FW Jr. Br JOphthalmol. 2010
Nov;94(11):1468-71. Cataract progression and treatment following posterior lamellar
keratoplasty.
Price MO, Price J Cataract Refract Surg. 2004 Jun;30(6):1310-5.
• PTK Combined phototherapeutic keratectomy and amniotic
membrane grafts for symptomatic bullous keratopathy. Mannan R, Pruthi A, Rampal U. Cornea. 2010 Oct;29(10):1207-8; author reply 1208-9. Comparative evaluation of phototherapeutic keratectomy and
amniotic membrane transplantation for management of symptomatic chronic bullous keratopathy.
Chawla B, Sharma N, Tandon R, Kalaivani M, Titiyal JS, Vajpayee RB.
Cornea. 2010 Sep;29(9):976-9. Combined phototherapeutic keratectomy and amniotic
membrane grafts for symptomatic bullous keratopathy. Vyas S, Rathi V. Cornea. 2009 Oct;28(9):1028-31.
www.o
opi.it

Edema corneale: Terapia farmacologica o chirurgica ?
Diagnostica oggettiva e linee guida definite Pachimetria, Conta endoteliale, OCT SA, Pentacam
•Irreversiblità edema •Terapia farmacologica inefficace •Residuo visivo scadente ww
w.oopi.it

TERAPIA CHIRURGICA Criteri di inclusione (W. Stark)
TERAPIA FARMACOLOGICA CHIRURGICA (DSAEK)
PACHIMETRIA
< 600μ
600 - 640μ
600 – 640μ
> 640μ
EDEMA
EPITELIALE
NO
NO
SI
SI
www.o
opi.it

TERAPIA CHIRURGICA Criteri di inclusione
• Mappa pachimetrica differenziale
Acutezza visiva residua • Studio topoaberrometrico e OCT SA della ZO(escludere
leucomi, disomogeneità refrattiva) • Prospettive di recupero (patologie retiniche concomitanti )
www.o
opi.it

ZO 620µ Periferia 700µ
TERAPIA FARMACOLOGICA CHIRURGICA (DSAEK)
PACHIMETRIA
< 600μ
600 - 640μ
600 – 640μ
> 640μ
EDEMA
EPITELIALE
NO
NO
SI
SI
BSCVA 6/10
ZO a:609µ b:620µ +11µ
www.o
opi.it

ZO 765
BSCVA 1/20
TERAPIA FARMACOLOGICA CHIRURGICA (DSAEK)
PACHIMETRIA
< 600μ
600 - 640μ
600 – 640μ
> 640μ
EDEMA
EPITELIALE
NO
NO
SI
SI
www.o
opi.it

ZO 620-650µ Edema epiteliale BSCVA 1/10
TERAPIA FARMACOLOGICA CHIRURGICA (DSAEK)
PACHIMETRI
A
< 600μ
600 - 640μ
600 – 640μ
> 640μ
EDEMA
EPITELIALE
NO
NO
SI
SI
www.o
opi.it

Prevedere sempre doppia indicazione chirurgica PHACO + IOL + DSAEK
Il paziente firma Consenso informato per entrambi gli interventi a prescindere dalla pianificazione combinata o in due tempi chirurgici separati
DSAEK (ipermetropizzazione 1 D)
TERAPIA FARMACOLOGICA CHIRURGICA (DSAEK)
PACHIMETRIA
< 600μ
600 - 640μ
600 – 640μ
> 640μ
EDEMA
EPITELIALE
NO
NO
SI
SI
TERAPIA CHIRURGICA Cataratta + Scompenso Corneale
www.o
opi.it

IDROPE CORNEALE (CHERATOCONO ACUTO) • Rottura della membrana di Descemet • Possibile risoluzione spontanea per migrazione cellule endoteliali
adiacenti • CONTROINDICATO Trapianto corneale a caldo
Terapia • Ipotonizzante • Iperosmolare • Antibiotica (profilassi)
Attendere RISOLUZIONE DELL’EDEMA, prima di pianificare CHERATOPLASTICA PERFORANTE
Edema corneale: deficit endoteliale ?
www.o
opi.it

Edema corneale: deficit endoteliale ?
• 20aa fa KR refrattiva • BCSVA 0.3 -3.00sf -4.50cil @90 • Edema corneale inferiore e in ZO • Assenza di diastasi delle KR
Pachimetria 844μ www.o
opi.it

New therapeutic modality for corneal endothelial disease using Rho-associated kinase inhibitor eye drops. Cornea. 2014 Nov;33 Suppl 11:S25-31. Koizumi N1, Okumura N, Ueno M, Kinoshita S.
A ROCK Inhibitor Converts Corneal Endothelial Cells into a Phenotype Capable of Regenerating In Vivo Endothelial Tissue. The American Journal of Pathology, 2012 DOI: 10.1016/j.ajpath.2012.03.033 N. Okumura, N. Koizumi, M. Ueno, Y. Sakamoto, H. Takahashi, H. Tsuchiya, J. Hamuro, and S. Kinoshita. ww
w.oopi.it

La chirurgia può acutizzare o indurre scompenso
La chirurgia può curare e risolvere lo scompenso
•Lo studio dell’endotelio corneale rappresente un cardine imprescindibile nella diagnostica pre e post chirurgica
•Nella gestione dell’edema corneale è necessario affidarsi a linee guida basate su criteri oggettivi ww
w.oopi.it






























