Embed Size (px)
Citation preview

REFERENCES
1. O'Brien WM, Bagby GF. Rare adverse reactions to nonsteroidalantiinflammatory drugs. J RheumatoI1985;12:562-7.
2. Madhok R, MacKenzie JA, Lee FD, Bruckner FE, Terry TR,Sturrock RD. Small bowel ulceration in patients receiving nonsteroidal anti-inflammatory drugs for rheumatoid arthritis. Q JMed 1986;255:53-8.
3. Neoptolemos JP, Locke TJ. Recurrent small bowel obstructionassociated with phenylbutazone. Br J Surg 1983;70:244-5.
4. Tanner AR, Raghunath AS. Colonic inflammation and nonsteroidal anti-inflammatory drug administration. Digestion1988;41:116-20.
5. Hall RI, Petty AH, Cobden I, Lendrum R. Enteritis and colitisassociated with mefenamic acid. Br Med J [Clin Res]1983;287:1182.
6. Uribe A, Johansson C, Slezak P, Rubio C. Ulcerations of thecolon associated with naproxen and acetylsalicylic acid treatment [Letter]. Gastrointest Endosc 1986;32:242-3.
7. Bjarnason I, Price AB, Zanelli G, et al. Clinico-pathologicalfeatures of non-steroidal anti-inflammatory drug (NSAID)induced small intestinal strictures. Gastroenterology 1988;94:1070-4.
8. Bjarnason I, Peters TJ. Intestinal permeability, non-steroidalanti-inflammatory drug enteropathy and inflammatory boweldisease: an overview. Gut 1989;30:22-8.
Endoscopic demonstration of nonsteroidal anti-inflammatory drug-inducedsmall intestinal strictures
Noel B. Hershfield, MD
There is increasing evidence that non-steroidalanti-inflammatory drugs (NSAIDs) can cause damageto the small intestine. Lang et a1./ Bjarnason et a1.,2and others3
•4 have demonstrated lesions at surgery
and also claim that many patients on treatment withthese agents may develop small bowel inflammation,increased permeability, blood and protein loss andstrictures. Theyl-4 employed indium scanning of thesmall intestine, permeability studies, and laparotomyto determine these abnormalities.
We recently had the opportunity to study a patientwith such lesions at endoscopy. As far as we are aware,this is the first endoscopic description of ileal "diaphragm disease" induced by non-steroidal anti-inflammatory drugs.
CASE REPORTA 64-year-old woman presented with a small intestinal
obstruction. She had longstanding rheumatoid arthritis andhad used NSAIDs of various types for 15 years on a continuing basis. In 1960, a diagnosis of polyposis coli was established. She underwent a subtotal colectomy, with ileorectalanastomosis. Subsequently, she was followed with annual
Reprint requests: Noel B. Hershfield, MD, 711 South Tower, 3031Hospital Drive N. W., Calgary, Alberta T2N 2T9, Canada.
388
9. Sturges HF, Krone CL. Ulceration and stricture of the jejunumin a patient on long-term indomethacin therapy. Am J Gastroenterol 1973;59:162-9.
10. Huber T, Ruchti C, Halter F. Nonsteroidal antiinflammatorydrug-induced colonic strictures: a case report. Gastroenterology1991;100:1119-22.
11. Mair WSJ, McMahon MJ, Goligher JC. Stenosis of the colonin acute pancreatitis. Gut 1976;17:692-5.
12. O'Connell TX, Kadell B, Tompkins RK. Ischemia of the colon.Surg Gynecol Obstet 1976;142:337-42.
13. West BR, Ray JE, Gathright JB Jr. Comparison of transientischemic colitis with that requiring surgical treatment. SurgGynecol Obstet 1980;151:366-8.
14. Kaufmann HJ, Taubin HL. Nonsteroidal anti-inflammatorydrugs activate quiescent inflammatory bowel disease. Ann Intern Med 1987;107:513-6.
15. Lang J, Price AB, Levi AJ, Burke M, Gumpel JM, BjarnasonI. Diaphragm disease: pathology of disease of the small intestineinduced by non-steroidal anti-inflammatory drugs. J Clin PathoI1988;41:516-26.
16. Bjarnason I, Zanelli G, Smith T, et al. Nonsteroidal antiinflammatory drug-induced intestinal inflammation in humans. Gastroenterology 1987;93:480-9.
17. Kendall MJ, Nutter S, Hawkins CF. Xylose test: effect ofaspirin and indomethacin. Br Med J [Clin Res] 1971;1:533-6.
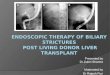
Figure 1. Sigmoidoscopic appearance of lowest diaphragm.
sigmoidoscopic examinations, and no further polyps werediscovered nor was there any evidence of malignancy.
On examination she was distressed, complaining of abdominal pain, distension, and vomiting foul-smelling material. Vital signs were normal. The abdomen was distended,visible peristalsis was seen, and high-pitched bowel soundswere heard. Rectal examination was negative. Evidence ofsevere rheumatoid arthritis in the upper and lower extremities was noted. Hematological investigation revealed a normocytic, normochromic anemia. White blood cell count was7500, platelet count was 450,000. Multichannel analysis wasnormal except for an albumin level of 20 g/liter (normal, 30to 50 g/liter). Abdominal x-rays demonstrated dilated loops
~SrnillN~STINALEND~C~Y

of small intestine. Sigmoidoscopic examination verified thepresence of pinhole strictures proximal to the ileal-sigmoidanastomosis in the ileum at 25, 35, and 45 cm from the analverge (Fig. 1). The lower stricture was easily fractured withthe instrument, but the lesions at 35 and 45 cm had to beforcibly dilated with a balloon passed through the sigmoidoscope. On completion of these maneuvers, a large gush ofbile-stained fluid poured out of the gut.
Biopsy of the areas revealed hyperplasia, villous blunting,and increased Paneth cell production, plus a chronic inflammatory infiltrate and gastric antral metaplasia (Figs. 2 to4).
The patient was reinvestigated at 6 months and 1 yearlater. She had discontinued all NSAIDs and was beingtreated with gold. No further lesions were detected on sigmoidoscopic examination.
DISCUSSION
The evolution of these lesions is unknown. Bjarnason et al.2
,5 demonstrated increased permeability ofthe small intestine in 70% of patients taking NSAIDswithin hours of ingestion. They suggest that intestinaldamage may result from toxin and macromoleculartransmigration across the wall of the gut, with invasion of the damaged mucosa by bacteria, leading toinflammatory changes with blood and protein loss.
Lang et al. l have noted these "diaphragms" at surgical operations for intestinal obstruction. These lesions are notoriously difficult to detect at surgery andradiological investigation. They reported seven casesof this unusual lesion, demonstrated at surgery.l
Bjarnason et al.6 suggested that NSAIDs appear tointerfere with intestinal barrier function and that thesite of the damage may be at the level of the intracellular junctions. They have found that two-thirds ofpatients on NSAIDs have evidence of subclinical inflammation in the small intestine and believe that thisleads to ulceration and subsequent stricture formation. They also noted similar lesions in rats treated
Figure 2. One biopsy shows flat mucosa, increased mononuclear cells in the lamina propria, and mild crypt irregularity(low power, H&E).
VOLUME 38, NO.3, 1992
Figure 3. Higher magnification of Figure 2. Neutrophils infiltrate surface epithelium and there is active chronic inflammation in the lamina propria.
Figure 4. The central cluster of glands, which are lined bysimple mucin-secreting epithelium, represent metaplasia togastric antral glands associated with regeneration (highpower, H&E).
389

with indomethacin. These lesions can be preventedwith prostaglandins and antibiotics.7
Our report represents a unique endoscopic description of so-called diaphragm disease of the ileum believed to be due to the effects of NSAIDs. One previousreport exists8 of intestinal inflammation. Patients whoare ingesting NSAIDs on a chronic basis and whocomplain of intestinal symptoms or are found to beanemic or hypoalbuminic should undergo indiumscanning and endoscopy in an attempt to demonstrateintestinal inflammation, or intestinal diaphragms.
REFERENCES1. Lang J, Price AB, Levi AJ, Gumpel JM, Bjarnason 1. Diaphragm
disease: pathology of the small intestine induced by nonsteroidal antiinflammatory drugs. J Clin PathoI1988;41:516-26.
390
2. Bjarnason I, ZaneIIi G, Smith T, et al. Nonsteroidal antiinflammatory drug-induced intestinal inflammation in humans. Gastroenterology 1987;93:480-9.
3. Sturgess HF, Krone CL. Ulceration and strictures of the jejunumin a patient on long term indomethacin. Am J Gastroenterol1973;59:162-9.
4. Bjarnason I, Zanelli G, Prouse P, et al. Blood and protein lossvia small intestinal inflammation induced by nonsteroidal antiinflammatory drugs. Lancet 1987;2:711-4.
5. Bjarnason I, So A, Levi AJ, et al. Intestinal permeability andinflammation in rheumatoid arthritis: effects of nonsteroidalantiinflammatory drugs. Lancet 1984;2:1171-4.
6. Bjarnason I, Williams P, Smethurst P, Peters TJ, Levi AJ. Theeffect of nonsteroidal drugs and prostaglandins on the permeability of the human small intestine. Gut 1986;27:1292-7.
7. Bjarnason I, Macpherson A. The changing side effect profile ofnonsteroidal drugs. A new approach for the prevention of a newproblems. Scand J GastroenteroI1989;163:56-64.
8. Morris AJ, Madhok R, Sturrock RD, Capell HA, MacKenzie JF.Enteroscopic diagnosis of small bowel ulceration in patientsreceiving nonsteroidal antiinflammatory drugs. Lancet1991;1:337-40.
GASTROINTESTINAL ENDOSCOPY

![Endoscopic incisional therapy for benign esophageal ... · caustic strictures and radiation strictures are known to be complex strictures[2]. Dilatation by bougie or balloon dilators](https://img.dokumen.tips/doc/110x75/5f80c75354e157596f1a7ef6/endoscopic-incisional-therapy-for-benign-esophageal-caustic-strictures-and-radiation.jpg)