Embed Size (px)
Citation preview

388
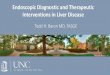
Proportion of children difficult to review and Griffiths total
quotient.
Numbers at top of columns refer to total in that quotient group.
The disability rate amongst those "easy to review" was only 4%but amongst the "difficult" group it was 35% (table). Failure toinclude follow-up details from the difficult to review group wouldbe serious: the frequency of severe disability rises from 4% to almost8% (18/230) when children difficult to review are included and toover 10% when known details of all neonatal survivors are included.When the children are ranked by their general quotient (Griffiths
assessment) the lower scoring groups contain higher proportions ofchildren who are difficult to review (p<0001; Armitage’s chi-squared test for trend) (figure).
It seems that parents who have not yet come to terms with theirchild’s disability may tend to avoid situations where that disability ishighlighted. This could be a source of ascertainment bias.
Unfortunately 100% follow-up is both difficult and expensive toachieve. Our results suggest that trying to persuade those parentswho seem to be reluctant for their children to be examined is a better
way of reducing bias than the tracing of families who are merelyhighly mobile.
U. W. held a research registrar post funded by the Northern RegionalHealth Authority.
We thank our obstetrician and paediatrician colleagues; the parents; andMrs Brenda Gibson whose persistence and skill was primarily responsible forfinding the children and winning the confidence of the families.
Department of Paediatrics,Sunderland District General Hospital,Sunderland, Tyne and Wear SR4 7TP
UNNI K. WARIYARSAM RICHMOND
1. Wariyar U, Richmond S, Hey E. Pregnancy outcome at 24-31 weeks’ gestation:neonatal survivors. Arch Dis Child (in press).
2. Griffiths R. The abilities of young children. London; Child Development ResearchCentre, 1970
3. Griffiths R. The abilities of babies Eden House, Amersham Association of Researchin Infant and Child Development, 1976.
TEACHERS, STRESS, AND MORTALITY
SIR,-Dr Herloffand Dr Jarvholm’s data (Jan 21, p 159) could beinterpreted as not supporting either of their two assumptions thatteachers are exceptionally stressed and that stress leads to increasedmortality, especially from cardiovascular disease. However, I
suggest an alternative hypothesis.Compared with other stressed professionals, teachers have the
advantage of holidays in which, generally, their professional workstands still and they have a chance to catch up with any backlog andthose aspects of their domestic and social life that have suffered
during termtime. I do not suggest that teachers do not work in theholidays, for many do; but it is regenerative work which gives them afresh start at the beginning of the next term. Some teachers do haveduties such as time-tabling, university entrance work, and field tripsin the holidays, but in general the more robust teachers progress to
these jobs. It is also true in the UK that many teachers may have totake jobs or mark examination papers in the holidays for economicreasons. But teachers do not usually suffer from the relentlesspressure that characterises many other jobs, where a holiday resultsin an additional backlog of work.A problem in such studies is that we do not have an adequate
model of the different types of stress. We do not understand howmuch intermittent resting counteracts the negative impact of stresson health. In the UK at least, the frustrations of teachers have risenand their morale and self-esteem have fallen in recent years. Itwould be interesting to see a study repeated regularly in the UK thatmeasured stress and the effect of holidays between terms.
Frankrijklaan 5,1900-Overijse, Belgium JOHN R. JACKSON
ENDOSCOPIC BIOPSY FORCEPS AND TRANSFEROF TISSUE BETWEEN CASES
SIR,-Endoscopy clinics and histopathology laboratories usuallyoperate systems to ensure that biopsy specimens and patients arematched correctly. Considerable attention is also given to thecleaning and disinfection of endoscopic equipment,’ but littleattention has been given to the risks of the carry over of tissue. Thatproblem first came to our attention in 1983 when a 50-year-old manunderwent oesophagogastrectomy after an endoscopic biopsydiagnosis of poorly differentiated squamous carcinoma of theoesophagus. A barium meal was reported as showing a strictureconsistent with carcinoma of the oesophagus-but the radiologistalready knew the biopsy diagnosis. The oesophagogastrectomyspecimen, after detailed examination, contained no evidence ofmalignancy. The patient recovered well and his delight at thesymptom relief and the reversal of the diagnosis of cancer was notmarred by the knowledge that the surgery had been much moreradical than it need have been. Clearly, however, this patient hadbeen subjected to unnecessary risk.Review of the biopsy material confirmed that there had been no
interpretational error; one of four mucosal fragments did indeedcontain poorly differentiated squamous carcinoma and the waxblock from which the sections had been cut also contained a
fragment of carcinoma. The endoscopy clinic records indicated thatanother patient with a histologically identical squamous carcinomaof the oesophagus had been seen earlier in the same gastroscopysession. Histopathology department records revealed that the twocases were handled non-consecutively, virtually ruling out transferof tissue in the laboratory. The two endoscopies had beennon-consecutive and different endoscopes had been used. Thebiopsy forceps had been immersed in glutaraldehyde solution for 20min but we do not know that the same forceps were used.
Following this incident the endoscopy clinic staff were instructedto pay closer attention to the mechanical cleaning of biopsy forceps.Subsequently no similar incident was identified. Recently,however, a gastric biopsy sample contained a small fragment of whatmight have been interpreted as gastric mucosa showing intestinalmetaplasia or as a fragment of small-bowel mucosa. There was,however, evidence of Whipple’s disease in the lamina propria of thisfragment. The day before, a histological diagnosis of Whipple’sdisease had been made on endoscopic biopsy tissue of small bowelfrom a different patient. The samples had been received andhandled by the laboratory on different days, making laboratoryerror impossible. The endoscopies, however, had been on the sameday but in different sessions, in different locations, and withdifferent endoscopes. The biopsy forceps used at the second
procedure had, however, been carried by the surgeon from thelocation of the earlier small bowel biopsy to a separate theatre. Theforceps had undergone the routine cleansing and disinfection
procedure.The transfer of tissue by biopsy forceps seems to have occurred in
both these cases. The current regimen of manual mechanicalcleansing followed by a 20 min soak in glutaraldehyde withultrasonification only at the end of each day, although standardpractice, may be inadequate. Glutaraldehyde, besides being aneffective disinfectant, is also an excellent tissue fixative and is very

389
often used as such in the preparation of tissues for electron
microscopy. Thus rather than helping to destroy or removeadherent tissue it may well preserve the tissue and cause it to stick tothe metal of the forceps. We have exposed tissue to disinfectantsolutions of 2% glutaraldehyde and fmd that the tissues are virtuallyindistinguishable from those fixed directly in formalin. There maybe some blurring of the nuclear chromatin pattern but this is aninconsistent and subtle feature and is unlikely to be noticed by thehistopathologist. We therefore strongly recommend that all theatresand endoscopy clinics are equipped with sufficient biopsy forceps topermit ultrasonification of the instruments after every case. Thisshould be done before immersion in glutaraldehyde.
Northampton General Hospital,Northampton NN1 5BD
S. B. COGHILLC. H. MASON
J. G. N. STUDLEY
1 Anon. Cleaning and disinfection of equipment for gastrointestinal flexible endoscopy:interim recommendations of a working party of the British Society of
Gastroenterology Gut 1988; 29: 1134-51.2. Hanson PJV, Jeffries DJ, Batten JC, Collins JV Infection control revisited: dilemma
facing today’s bronchoscopists. Br Med J 1988; 297: 185-87.
EPILEPTIC SEIZURES AND SMOTHER-PROOFPILLOWS
SiR,—Eighteen years ago H. J. A. Longmore and I reportedthree patients with grand mal epilepsy who suffocated during sleepA further seven cases have since become known to me.2--4 Weadvocated the use of a smother-proof pillow by all sufferers of grandmal epilepsy, a suggestion taken up by the Epileptic Assocation.
I retired from general practice three years ago, so judge myastonishment when a distraught mother telephoned to inform methat her daughter, a 14-year-old with epilepsy, had died ofsuffocation during a seizure in the night. The daughter had been apupil in a large residential school for epileptic children. Sodistressed was the mother that she had searched the literature andtracked me down. She was especially upset because she had used asafety pillow at home and had assumed the school would do thesame-the school had not, although it does now.The death of yet another epileptic patient poses the question:
what more can be done to publicise this danger? Some doctors mayrequire further proof of the benefit of smother-proof pillows, eventhough no epileptic patient using such a pillow has been reported tosuffocate during a seizure. Recently the manufacturer has ensuredconformity to government fire regulations.The Whins,Kinnel Banks,Lochmaben,Lockerbie DG11 1TD J. B. WILSON
1 Longmore HJA, Wilson JB. Epileptic death due to suffocation during sleep Lancet1970, ii: 782
2 Wilson JB Suffocation in epilepsy Br Med J 1973; iv. 173.3 Wilson JB Hazards of epilepsy. Br Med J 1978; ii: 200.4 Wilson JB. Epilepsy. Br Med J 1979; i. 1218.
HISTIOCYTIC MEDULLARY RETICULOSIS:A LETHAL FORM OF PRIMARY EBV INFECTION IN
YOUNG CHILDREN IN TAIWAN
SiR,-Histiocytic medullary reticulosis (HMR) remainscontroversial in respect of aetiology and the nature of the atypical"histiocytes". The clinical features and geographical distribution ofHMR have led to the suggestion that it is a fatal form of infectiousmononucleosis.12We have observed a high frequency of HMR in Taiwan, as
reported from mainland China and Uganda.Z3 The disease affectedpreviously healthy young children who presented with fever,jaundice, hepatosplenomegaly, and pancytopenia; the illness lasted2-3 weeks. The seasonal clustering of cases in Taiwan in July,August, and September made us question whether NMR is aneoplastic disease. We have studied fresh lymphoid tissue from ayoung patient with HMR looking for Epstein-Barr virus (EBV) bySouthern blot and in situ DNA hybridisation and investigated the
lineage of these atypical large cells. We found a high copy number ofEBV genomes (more than 100 per cell) in the extracted tissue DNA.In situ hybridisation demonstrated that the EBV-positive granuleswere present in the cytoplasm of the atypical histiocytes.Immunohistochemical study revealed that these atypical histiocytesrepresented polyclonal B-immunoblastic lymphoproliferation. Wereviewed our necropsy material and found that these childhoodcases of HMR shared the following features: lymphoid organs,liver, spleen, lungs, and bone marrow showed diffuse sinusoidinfiltration with variable numbers of large atypical cells,plasmacytoid cells, lymphocytes, and mature histiocytes with activehaemophagocytosis.
Since the age prevalence of primary EBV infection in Taiwancorrelates quite well with the age distribution of our HMR patients,’we hypothesise that cases of HMR in young children in Taiwanmay be a consequence of primary EBV infection or a fatal form ofinfectious mononucleosis.A fatal form of EBV-induced lymphoproliferative disorder, with
clinical and haematological features of HMR, has been reported inpatients with acquired immunodeficiency and in organ transplantrecipients.5-8 We do not know whether our young patients had anunderlying immunodeficiency, however, they had been well beforethe onset of disease. We are now studying the immune status andEBV serology of HMR patients to clarify this point.
Departments of Pathologyand Paediatrics,
College of Medicine,National Taiwan University Hospital,Taipei, Taiwan, Republic of China
IH-JEN SUHONG-JONG HSIEHCHIN-YING LEE
1. Mallick NP, Davson J. Is histiocytic medullary reticulosis a fatal form of infectiousmononucleosis? Lancet 1981; ii: 43.
2. Martelli MF, Tabilio A, Aversa F, Falini B, Rocchi G. Is histiocytic medullaryreticulosis an infectious disease? Lancet 1982; ii: 446-47.
3. Amsel S, Bijlsma F. Histiocytic medullary reticulosis: clinical and pathological studiesin Uganda. Trop Geogr Med 1974; 26: 31-38.
4 Lm KH, Chiang CH, Yang CS. Age distribution and Epstem-Barr virus,cytomegalovirus, and rubella virus antibodies. J Formosan Med Assoc 1987; 86:1316-19.
5. Mroczek EC, Weisenburger DD, Grierson HL, Markm R, Purtilo DT. Fatalinfectious mononucleosis and virus-associated hemophagocytic syndrome. ArchPathol Lab Med 1987; 111: 530-35.
6. Beissner RS, Rappaport ES, Diaz JA Fatal case of Epstein-Barr virus-inducedlymphoproliferative disorder associated with a human immunodeficiency virusinfection. Arch Pathol Lab Med 1987; 111: 250-53
7. Zutter MM, Martin PJ, Sale GE, et al. Epstein-Barr virus lymphoproliferation afterbone marrow transplantation. Blood 1988; 72: 520-29.
8. Nalesnik MA, Jaffe R, Starzl TE, et al. The pathology of post-transplantlymphoproliferative disorders occurring in the setting of cyclosporineA-prednisone immunosuppression. Am J Pathol 1988; 133: 173-92.
POSTICTAL SPET IN EPILEPSY
SiR,—Your Jan 21 editorial discusses the value of metabolic
imaging with positron emission tomography (PET) and singlephoton emission tomography (SPET) in the localisation of theepileptic focus. Accurate localisation is essential in the surgicaltreatment of intractable temporal lobe epilepsy (TLE), a valuableand underused procedure.’ As you say, interictal PET is useful forthis purpose but is not widely used because of its very high cost.SPET is widely available and preliminary reports, which youreview, suggest that peri-ictal studies may be especially valuable.Over the past eighteen months we have done postictal SPET with99n’-technetium hexamethylpropyleneamine oxime (99IDTc-HMPAO) in 45 patients with unilateral temporal lobe epilepsydiagnosed by ictal electroencephalogram (EEG) recordings.z°3 Thisstudy confirmed the value of postictal SPET and revealed hithertounknown features of postictal cerebral blood flow.
Whilst interictal SPET with lz3l_iodoamphetamines or 99IDTc-HMPAO shows hypoperfusion in a significant proportion ofpatients with temporal lobe epilepsy, our data with HMPAOdemonstrate that interictal abnormalities are not sufficiently specificto localise the epileptic focus confidently (table). In contrast,characteristic patterns of postictal perfusion2 gave correct
localisation in 33 of 45 cases (73%) and incorrect localisation in only1 patient. Our preliminary quantitative SPET analyses agree withthe quantitative interpretation.