Embed Size (px)
Citation preview

Case Reports
Endophthalmitis: A rare complication ofarteriovenous fistula infection
Madhav DESAI,1 Ram RAPOOR,1 Swarna Latha GUDITHI,1 Ravi KUMAR,2
Neela PRASAD,1 Kaligotla Venkata DAKSHINAMURTY1
1Department of Nephrology, Nizam’s Institute of Medical Sciences, Hyderabad, Andhra Pradesh, India;2Hyderabad Opthalmology Institute, Hyderabad, Andhra Pradesh, India
AbstractVascular access infection is a frequent problem in patients undergoing maintenance hemodialysis.
Infection of arteriovenous fistula (AVF) is less common than dialysis catheter-associated infection.
Previous case reports described endophthalmitis secondary to hemodialysis catheter-related infec-
tion, but not secondary to native AVF infection. We report a rare patient of endophthalmitis as a
metastatic infection of AVF cannulation site abscess. A 19-year-old girl on maintenance hemodialysis
for the past 2 years has presented with a history of fever, chills, and rigor of 3-days duration and
painful dimness of vision in the left eye of 1-night duration. It was followed by redness of the eye,
photophobia, and ocular discharge. On examination, the patient was febrile with an abscess near
cannulation site of AVF. There was no perception of light in the left eye, conjunctiva was congested,
cornea was clear, hypopyon present, and pupil was mid-dilated, not reacting to light. Lens was clear.
Vitreitis and exudative retinal detachment was present. Methicillin sensitive Staphylococcus aureus
was isolated from blood, pus from AVF abscess and vitreous fluid. Diagnosis of endophthalmitis was
confirmed by B-scan ultrasound. She was treated with both intravenous and intraocular antibiotics
and drainage of pus from AVF abscess and therapeutic vitrectomy. Though arteriovenous abscess
responded to sensitive antibiotics and drainage, vision has not improved much. Strict aseptic pre-
cautions during regular AVF cannulation are required. Lapses may lead to loss of vision apart from
described complications like access closure, endocarditis, and osteomyelitis.
Key words: Arteriovenous fistula infection, endophthalmitis, hemodialysis
INTRODUCTION
An ideal permanent access delivers a flow adequate for
the dialysis prescription, lasts for a long time and has a
low complication rate. The autologous arteriovenous
fistula (AVF) comes closest to satisfying these criteria.1
Infection is the most common reason for access failure
when cuffed silicone catheters are used for long-term
access, and is the second most common cause of graftfailure when poly tetra fluoro ethylene (PTFE) grafts are
used. Infection rates of an AVF continue to be acceptable
(o1%).2 The infections are potentially lethal due to
impaired immunological status of long-term dialysis
patients. Infection may be at the arteriovenous anasto-
mosis, which requires immediate resection of infected
tissue and securing a new AVF. Infection at cannulation
sites requires cessation of cannulation at that site. Access-
related bacteremia leading onto metastatic complicationshas been described with intravenous catheters.3 We
report a rare patient case of acute endophthalmitis as a
metastatic infection of AVF cannulation site abscess.
CASE REPORT
A 19-year-old girl has been on maintenance hemodialysis
since February 2005. She was diagnosed with focal seg-
Correspondence to: Prof. K.V. Dakshinamurty, Departmentof Nephrology, Nizam’s Institute of Medical Sciences,Punjagutta, Hyderabad – 500082, Andhra Pradesh, India.E-mail: [email protected]
Hemodialysis International 2008; 12:227–229
r 2008 The Authors. Journal compilation r 2008 International Society for Hemodialysis 227
mental glomerulosclerosis in 1999. An AVF was securedin October 2004. She has been on regular thrice-weekly
bicarbonate hemodialysis and erythropoietin. Her Kt/V
in December 2006 was 1.4.
She has presented with history of fever, chills, and rigor
of 3-days duration and painful dimness of vision in left
eye of 1-night duration. It was followed by redness of eye,
photophobia, and ocular discharge. On examination,
patient was febrile with an abscess near cannulation siteof AVF (Figure 1). There was no perception of light in the
left eye, conjunctiva was congested, cornea was clear,
hypopyon present, and pupil was mid-dilated, not react-
ing to light. Lens was clear. Vitreitis and exudative retinal
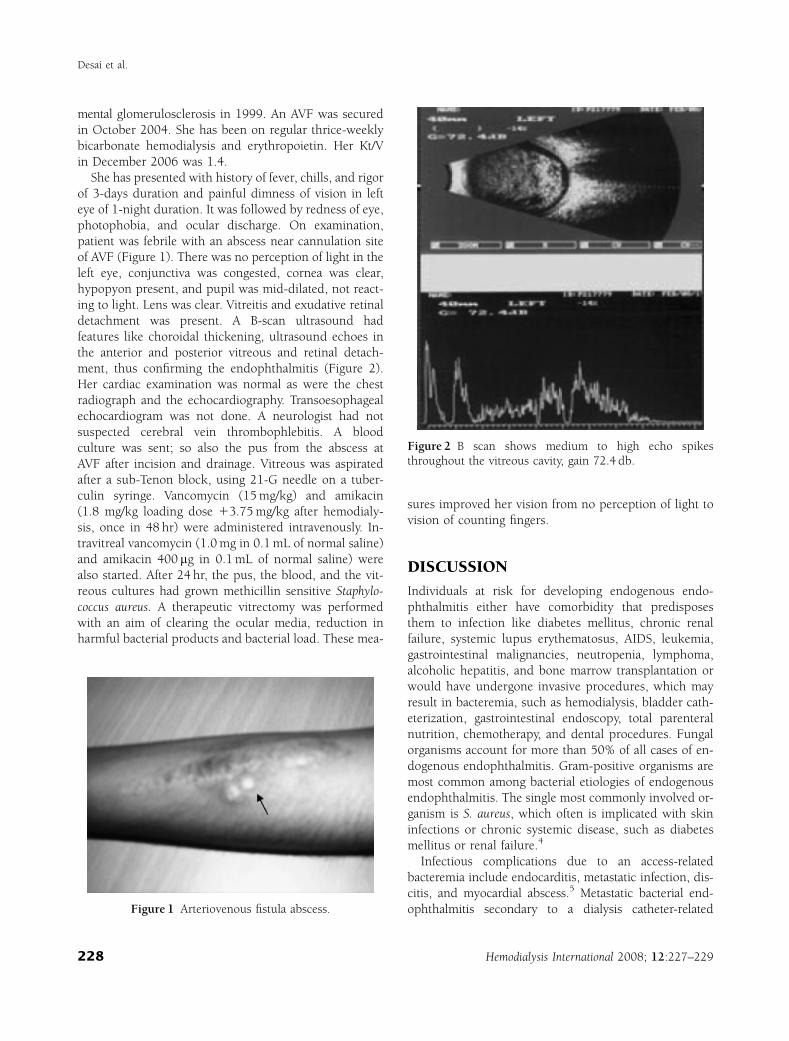
detachment was present. A B-scan ultrasound had
features like choroidal thickening, ultrasound echoes in
the anterior and posterior vitreous and retinal detach-
ment, thus confirming the endophthalmitis (Figure 2).Her cardiac examination was normal as were the chest
radiograph and the echocardiography. Transoesophageal
echocardiogram was not done. A neurologist had not
suspected cerebral vein thrombophlebitis. A blood
culture was sent; so also the pus from the abscess at
AVF after incision and drainage. Vitreous was aspirated
after a sub-Tenon block, using 21-G needle on a tuber-
culin syringe. Vancomycin (15 mg/kg) and amikacin(1.8 mg/kg loading dose 13.75 mg/kg after hemodialy-
sis, once in 48 hr) were administered intravenously. In-
travitreal vancomycin (1.0 mg in 0.1 mL of normal saline)
and amikacin 400 mg in 0.1 mL of normal saline) were
also started. After 24 hr, the pus, the blood, and the vit-
reous cultures had grown methicillin sensitive Staphylo-
coccus aureus. A therapeutic vitrectomy was performed
with an aim of clearing the ocular media, reduction inharmful bacterial products and bacterial load. These mea-
sures improved her vision from no perception of light to
vision of counting fingers.
DISCUSSION
Individuals at risk for developing endogenous endo-
phthalmitis either have comorbidity that predisposes
them to infection like diabetes mellitus, chronic renal
failure, systemic lupus erythematosus, AIDS, leukemia,
gastrointestinal malignancies, neutropenia, lymphoma,alcoholic hepatitis, and bone marrow transplantation or
would have undergone invasive procedures, which may
result in bacteremia, such as hemodialysis, bladder cath-
eterization, gastrointestinal endoscopy, total parenteral
nutrition, chemotherapy, and dental procedures. Fungal
organisms account for more than 50% of all cases of en-
dogenous endophthalmitis. Gram-positive organisms are
most common among bacterial etiologies of endogenousendophthalmitis. The single most commonly involved or-
ganism is S. aureus, which often is implicated with skin
infections or chronic systemic disease, such as diabetes
mellitus or renal failure.4
Infectious complications due to an access-related
bacteremia include endocarditis, metastatic infection, dis-
citis, and myocardial abscess.5 Metastatic bacterial end-
ophthalmitis secondary to a dialysis catheter-relatedFigure 1 Arteriovenous fistula abscess.
Figure 2 B scan shows medium to high echo spikesthroughout the vitreous cavity, gain 72.4 db.
Desai et al.
Hemodialysis International 2008; 12:227–229228

septicemia has been described in the past.3,6,7 But therewere few reports of endophthalmitis due to AVF infection.
Marr et al.8 in a retrospective study of staphylococcal
bacteremia in hemodialysis patients in 5431.8 patient-
months have identified 58 (89%) episodes of bacteremia
considered to have originated in a vascular access device
of which 31 (53%) patients with device-related bacter-
emia were dialyzed through dual lumen, tunneled, cuffed
catheters; 8 (14%) were dialyzed through temporary cath-eters; 10 (17%) were dialyzed through AVFs; and 9 (16%)
were dialyzed through PTFE grafts. Not a single patient
of endophthalmitis has been described though infective
endocarditis, osteomyelitis, and septic arthritis were
reported. There was a report of simultaneous bacterial
endocarditis and endophthalmitis due to Pseudomonas
aeruginosa in a patient who had both the AVF and arte-
riovenous graft (AVG).9 The report was not explicit aboutthe source of infection—AVF or AVG.
At our Institute, ‘‘universal precautions’’ are strictly
implemented. Entry into the hemodialysis center, other
than for patients, was forbidden. The nurses were all
trained in aseptic handling of the vascular access.
Surgical mask, aseptic gloves, and dressing were donned
by the nurses before vascular access manipulation. The
skin before needle puncture was prepared with povi-done-iodine, followed by spirit. The needle puncture site
was enclosed prior by a drape.
Prevention can be done with obsessional requirement
of correct preparation of skin before needle puncture,
which should be no less rigorous than during a surgery.
Staff and patients alike should understand the importance
of such a care and should be ever vigilant for the signs of
infection. Other preventive measures include periopera-tive antibiotics, treatment of active infection at other sites
before implantation of a vascular prostheses and elimi-
nation of nasal carriage, particularly in patients in whom
recurrent staphylococcal infection was associated withwell-documented nasal staphylococcal carriage.
Manuscript received September 2007; revised January
2008.
REFERENCES
1 Allen M, Work J. Venous catheter access for haemodial-ysis. In: Daugirdas JT, Blake PG, Ing TS eds. Handbook ofDialysis. Philadelphia, PA: Wolter Kluwer and LippincottWilliams and Wilkins; 2007; 87–104.
2 Escobar FS III, Morris DE. Vascular access for haemodi-alysis. In: Nissenson AR, Fine RN eds. Dialysis Therapy.Philadelphia, PA: Hanley and Belfus Inc.; 2002; 16–31.
3 Saleem MR, Mustafa S, Drew PTJ, et al. Endophthalmitis,a rare metastatic bacterial complication of haemodialysiscatheter-related sepsis. Nephrol Dial Transplant. 2007;22:939–941.
4 Jakobiec FA. Endogenous endophthalmitis. In: AlbertDM ed. Principles and Practice of Ophthalmology, Vol. 5.London: W B Saunders Co; 1994; 3120–3125.
5 Troidle L, Eisen T, Pacelli L, Finkelstein F. Complicationsassociated with the development of bacteremia withStaphylococcus aureus. Hemodial Int. 2007; 11:72–75.
6 Smith KG, Ihle BU, Heriot WJ, Becker GJ. Metastaticendophthalmitis in dialysis patients. Am J Nephrol. 1995;15:78–81.
7 Bloomfield SE, David DS, Cheigh JS, et al. End-ophthalmitis following staphylococcal sepsis in renal fail-ure patients. Arch Intern Med. 1978; 138:706–708.
8 Marr KA, Kong L, Fowler VG, et al. Incidence and out-come of Staphylococcus aureus bacteremia in hemodialysispatients. Kidney Int. 1998; 54:1684–1689.
9 Hsu KH, Ben RJ, Shiang JC, Feng NH. Pseudomonasaeruginosa endocarditis associated with endophthalmitiscaused by arteriovenous fistula and graft infection. J ChinMed Assoc. 2003; 66:617–620.
AV fistula related endophthalmitis
Hemodialysis International 2008; 12:227–229 229





























