Embed Size (px)
Citation preview

Oman Medical Specialty Board
Endometriosis After Surgical Menopause Mimicking Pelvic Malignancy: Surgeons’ Predicament
Rani A. Bhat, Melissa Teo and Akhil Krishnanand Bhat
Rani A. Bhat Consultant Gynaecological Oncologist HCG Oncology No. 8, P Kalinga Rao Road Sampangi Ramnagar Bangalore - 560027. India.E-mail: [email protected]
Melissa TeoSenior Consultant, Department of Surgical Oncology, National Cancer Centre Singapore, Singapore.
Akhil Krishnanand BhatSenior Consultant-General Surgery, St. Philomena's Hospital, No. 4 Cambell Road, Viveknagar, Bangalore-560047, India.
Abstract
Prevalence of persistent endometriosis in women after menopause without any hormonal replacement therapy is very rare. This is a case of a woman with previous history of total hysterectomy and bilateral salpingo-oophorectomy for endometriosis who presented with hemoperitoneum, vaginal bleeding, pelvic mass, and pulmonary thromboembolism mimicking as rectovaginal septum carcinoma. This is the first case report with a unique mode of presentation wherein the patient presented with hemoperitoneum requiring emergency embolization of the vessel to stabilize the patient. She underwent en bloc resection of the tumor with high anterior resection of the rectum. Histopathology confirmed endometriosis.
Keywords: Endometriosis; Ovarian cancer; Menopause.
Introduction
The incidence of endometriosis in post-menopausal women is 2% to 5%1,2 and is commonly seen in those who have received hormonal replacement therapy after menopause.3 This report is about a rare case of a patient with post-menopausal endometriosis, who presented with intra-abdominal bleeding, pelvic mass, vaginal bleeding and pulmonary thromboembolism. With clinical and radiological findings and past history of endometriosis, the disease was considered as rectovaginal septum carcinoma of clear cell type resulting from malignant transformation of endometriosis.
Received: 10 Feb 2014 / Accepted: 12 Apr 2014© OMSB, 2014
Case Report
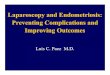
A 50-year-old para 2 was referred to our hospital in view of pelvic mass, bilateral hydronephrosis and pulmonary embolism. She had initially presented to a private hospital with a history of acute abdomen due to hemoperitoneum and bleeding per-vagina. A contrast enhanced CT scan of the abdomen and pelvis showed large hemoperitoneum with solid dense areas in the caudal portion of the pelvis with a blush of increasing contrast enhancement in the central part of the pelvis indicating active bleeding likely from a branch of inferior mesenteric artery (Figs. 1A and B). She underwent emergency embolization of the feeding vessels with gelfoam to stop the active bleeding. Following the embolization, CT showed a lobulated soft tissue density mass in the pelvis measuring about 15 × 6.6 × 6.5 cm which was compressing the rectum and the bladder and with bilateral hydronephrosis (Figs. 2A and B). Serum CA-125 was 595.8 and CA-19.9 was 26.9.
Figures 1A and B: Computed tomography (CT) of abdomen, pelvic and chest. A: Large amount of dense free fluid within the pelvis and moderate amount of more hypodense free fluid is also visualized in the abdomen. B: There is a blush of increasing contrast enhancement in the central and right hemipelvis in keeping with active hemorrhage.
Her past surgical history suggested that she had undergone total hysterectomy for fibroid uterus and after two years she had bilateral salpingo-oophorectomy and partial vaginectomy for deeply infiltrating endometriosis. Post-operatively, she was neither treated
Oman Medical Journal (2014) Vol. 29, No. 3:226-231DOI 10.5001/omj.2014.56

227
Oman Medical Specialty Board
for her endometriosis nor was she on any hormonal replacement therapy. With this mode of clinical presentation, the differential diagnosis considered were carcinoma of the peritoneum or recto-vaginal septum due to malignant transformation of the remnant endometriosis mainly of clear cell type due to the typical features of pelvic mass, pulmonary embolism and past history of endometriosis.
Figures 2A and B: CT of abdomen, pelvis and chest after embolization of inferior mesenteric artery: Lobulated soft tissue density mass seen in the pelvis measuring about 15 × 6.6 × 6.5 cm, compressing the rectum and bladder and displacing the small bowel loops laterally.
She underwent laparotomy revealing a 5 × 3 × 2.5 cm mass which was densely adherent to the rectosigmoid colon, to the pelvic side walls involving bilateral ureters, and eroding into the vagina causing ulceration of the vaginal vault. There was neither free intraperitoneal fluid nor any signs of pelvic or abdominal endometriosis. Preoperative CT showed a 15 × 6.6 × 6.5 cm mass in the pelvis, but intraoperatively, only a 5 × 3 × 2.5 cm mass was noted in the pelvis giving rise to a possibility that the intraperitoneal bleeding had undergone resorption. She underwent uretrolysis, en bloc resection of the tumor, and high anterior resection of the rectum. Postoperatively, the patient made uneventful recovery and was discharged home on the 9th postoperative day. Final histopathological findings showed features consistent with so-called necrotic pseudoxanthomatous nodule, associated with longstanding endometriosis and no features of malignancy.
Discussion
It has been hypothesized that endometriosis is estrogen-dependent and that progesterone inhibits the cellular proliferation, therefore endometriosis is commonly seen in women of reproductive age group and very rarely seen after menopause. Different theories have been postulated for recurrence of endometriosis in women
who have undergone surgical menopause, such as ovarian remnant syndrome (ORS), wherein part of the ovarian tissue has been left behind after bilateral oophorectomy which continues to produce hormone and stimulate the ectopic endometrial implant. The endometrial implants can also be reactivated by exogenous estrogen in the form of hormonal replacement therapy,3,4 or endogenous estrogen which comes from peripheral conversion of androgen and androstenedione from adrenal glands. Evidence also shows that endometrial implants harbor aromatase expression which is stimulated by PGE2 leading to local production of estrodiol. These implants also lack hydroxysteroid dehydrogenase (17β-HSD) type 2 expression thus impairing conversion of estradiol to estrone which results in local accumulation of potent estrodiol. Another possible hypothesis of endometriosis after menopause is due to spontaneous coelomic metaplasia and vascular endometrial cell transportation. It is possible that our patient had ovarian remnant syndrome because her BMI was normal, had no history of HRT but had past history of deep endometriosis making it possible that part of ovarian tissue must have been left in-situ during laparotomy done for bilateral salpingo-oophorectomy and vaginectomy. Since we did not have preoperative serum estradiol and FSH levels, it was difficult to demonstrate her true menopausal status.
Table 1 shows a summary of studies on endometriosis in women who have undergone surgical menopause. Presentation of endometriosis in post-menopausal patients can be unpredictable and mainly depends on the location of the endometriotic implants. Since endometriosis is usually associated with surrounding inflammation and fibrosis, symptoms can sometimes be very severe. Since the time of Sampson in 1925,5 numerous case reports and review of the literature have shown that endometriosis can be a precursor of ovarian, primary peritoneal or recto-vaginal septum cancer mainly of clear cell, endometroid type.6,7 Literature has also shown that endometriosis can act as a precursor for both cystic and adenofibromatous types of clear cell carcinoma of the ovary.8 Endometriosis can sometimes present with ascites, pelvic mass and pleural effusion mimicking as advanced ovarian cancer,9 thus making preoperative diagnosis of endometriosis, especially in women who have undergone total hysterectomy and bilateral salpingo-oophorectomy, very challenging to the treating physician. Clear cell carcinoma demonstrates unique clinical features such as large pelvic mass, thromboembolic complications and hypercalcemia.
In this case report, the patient had clinical features of pelvic mass, hemoperitoneum and pulmonary embolism and our diagnosis was carcinoma of the recto-vaginal septum of clear cell type associated with endometriosis. Surgical resection of all endometriotic implants and restoring normal anatomy is the treatment of choice. Hence, in patients with deeply infiltrating endometriosis, radical surgery involving bowel resection becomes inevitable. Following surgery postoperative hormonal treatment to suppress endometriosis has not yet been established.10
Oman Medical Journal (2014) Vol. 29, No. 3:226-231

228
Oman Medical Specialty Board
Tab
le 1
: Sum
mar
y of
stud
ies o
f end
omet
rios
is in
wom
en a
fter
tota
l hys
tere
ctom
y w
ith b
ilate
ral s
alpi
ngo-
ooph
orec
tom
y (T
HB
SO).
Cas
e no
Ref
eren
ceA
geM
eno-
paus
e st
atus
Mod
e of
pr
esen
tati
onC
linic
al
feat
ures
Past
his
tory
of
en
dom
etri
osis
Past
his
tory
of
surg
ery
His
tory
of
horm
onal
tr
eatm
ent f
or
endo
met
rios
is
Past
his
tory
of
HR
T**
*P
re-o
pera
tive
diag
nosi
s mad
eT
reat
men
tH
isto
logy
1T
akay
ama
K, Z
eito
un K
, G
unby
RT
, Sas
ano
H, C
arr
BR, B
ulun
SE
. Tre
atm
ent
of se
vere
pos
tmen
opau
sal
endo
met
rios
is w
ith a
n ar
omat
ase
inhi
bito
r.Fe
rtil
Ster
il. 1
998
Apr
;69(
4):7
09-1
3
53Ye
sPe
lvic
pai
nB
ilate
ral
dist
al u
rete
ral
obst
ruct
ion
Yes
TH
BSO
*N
oYe
s (or
al
conj
ugat
ed
estr
ogen
)
End
omet
rios
isE
xcis
ion
of th
e en
dom
etri
osis
and
re
impl
anta
tion
of b
ilate
ral u
rete
r in
to th
e bl
adde
r. R
ecur
renc
e of
en
dom
etri
osis
aft
er 3
ye
ars w
as tr
eate
d w
ith
arom
atas
e in
hibi
tor.
End
omet
rios
is
2G
iare
nis I
, Gia
mou
gian
nis
P, S
peak
man
CT
, Nie
to
JJ, C
rock
er S
G. R
ecur
rent
en
dom
etri
osis
follo
win
g to
tal h
yste
rect
omy
with
oo
phor
ecto
mym
imic
king
a
mal
igna
nt n
eopl
astic
lesi
on:
a di
agno
stic
and
ther
apeu
tic
chal
leng
e.A
rch
Gyn
ecol
Obs
tet.
2009
M
ar;2
79(3
):419
-21.
44Ye
sPa
inle
ss v
agin
al
blee
ding
Pelv
ic m
ass
Yes
TH
BSO
*N
oYe
s (c
onju
gate
d es
trog
en)
Mal
igna
nt
neop
last
ic
lesi
on, p
ossi
bly
a sa
rcom
a
Exc
isio
n of
the
pelv
ic
mas
s with
ant
erio
r re
sect
ion
of th
e si
gmoi
d co
lon.
End
omet
rios
is
3B
aile
y A
P, S
chut
t AK
, M
odes
itt S
C. F
lori
d en
dom
etri
osis
in
post
men
opau
sal w
oman
. Fer
til
Ster
il. 2
010
Dec
;94(
7):2
769.
e1-4
. Epu
b 20
10 M
ay 2
6.
53Ye
sG
ross
he
mat
uria
Rig
ht si
ded
retr
oper
itone
al
mas
s cau
sing
se
ver h
ydro
-ur
eter
o-ne
phro
sis
Yes
TH
BSO
*N
oN
oN
ot m
entio
ned
Rig
ht si
mpl
e ne
phre
ctom
y, ra
dica
lre
sect
ion
of th
e re
trop
erito
neal
mas
s in
clud
ing
diss
ectio
n of
par
tof
the
psoa
s mus
cle
and
the
infe
rior
ven
a ca
va, r
esec
tion
of th
e di
stal
ileum
plu
s cec
um
and
appe
ndix
due
to
mes
ente
ric
inva
sion
, an
d pr
imar
yile
oasc
endi
ng c
olon
re
anas
tom
osis
End
omet
rios
is
Oman Medical Journal (2014) Vol. 29, No. 3:226-231

229
Oman Medical Specialty Board
Oman Medical Journal (2014) Vol. 29, No. 3:226-231
Cas
e no
Ref
eren
ceA
geM
eno-
paus
e st
atus
Mod
e of
pr
esen
tati
onC
linic
al
feat
ures
Past
his
tory
of
en
dom
etri
osis
Past
his
tory
of
surg
ery
His
tory
of
horm
onal
tr
eatm
ent f
or
endo
met
rios
is
Past
his
tory
of
HR
T**
*P
re-o
pera
tive
diag
nosi
s mad
eT
reat
men
tH
isto
logy
4In
drac
colo
U, B
arbi
eri F
. Sile
nt
onse
t of p
ostm
enop
ausa
l en
dom
etri
osis
ina
wom
an w
ith re
nal f
ailu
re in
ho
rmon
e re
plac
emen
t the
rapy
: a
case
repo
rt. J
Med
Cas
e R
epor
ts. 2
010
Aug
4;4
:248
.
54Ye
sR
enal
failu
reB
ilate
ral
hydr
onep
hros
is
indu
ced
byex
trin
sic
com
pres
sion
of
both
ure
ters
(at
supr
aves
ical
foss
a) b
y no
dule
s co
mpa
tible
Yes
TH
BSO
*N
oYe
s (es
trog
en
base
d on
ly)f
or
seve
n ye
ars
End
omet
rios
isla
paro
scop
ic e
xcis
ion
of th
e en
dom
etri
otic
no
dule
s
End
omet
rios
is
5K
hong
SY,
Lam
A, C
oom
bes
G, F
ord
S. S
urgi
cal
man
agem
ent o
f rec
urre
nt
uret
eric
end
omet
rios
is c
ausi
ng
recu
rren
t hyp
erte
nsio
n in
a
post
men
opau
sal w
oman
.J M
inim
Inva
sive
Gyn
ecol
. 20
10 Ja
n-Fe
b;17
(1):1
00-3
.
62Ye
sR
ecur
rent
ur
inar
y tr
act
infe
ctio
n an
d pa
in in
left
ilia
c fo
ssa
Obs
truc
ted
left
ure
ter a
nd
hydr
onep
hros
is
Yes
TH
BSO
*N
oYe
s (es
trog
en
patc
h)E
ndom
etri
osis
Exc
isio
n of
en
dom
etri
otic
nod
ule
End
omet
rios
is
6Po
pout
chi P
, dos
Rei
s Lem
os
CR
, Silv
a JC
, Nog
ueir
a A
A,
Fere
s O, R
ibei
ro d
aR
ocha
JJ: P
ostm
enop
ausa
l in
test
inal
obs
truc
tive
endo
met
rios
is: c
ase
repo
rt a
nd re
view
of t
he
liter
atur
e. Sa
o Pa
olo
Med
J 20
08, 1
26:1
90-1
93.
74Ye
sH
emat
oche
zia,
te
nesm
us a
nd
pelv
ic p
ain
Col
onos
copy
re
veal
ed a
fr
iabl
e an
d st
enos
ing
tum
or
form
atio
n in
the
uppe
r rec
tum
.
Yes
TH
BSO
*N
oN
oA
bio
psy
reve
aled
m
ucos
al
frag
men
ts o
f en
dom
etri
al
type
Abd
omin
al
rect
osig
moi
dect
omy
with
a lo
w m
echa
nica
l co
lore
ctal
ana
stom
os
and
tran
sver
sost
omy
in a
pro
tect
ive
loop
pe
rfor
med
.
End
omet
rios
is
7R
. Fly
ckt,
S. L
yden
, A. R
oma
and
T. F
alco
ne*
Post
-men
opau
sal
endo
met
rios
is w
ith in
feri
or
vena
cav
a in
vasi
on re
quir
ing
surg
ical
man
agem
ent
Hum
Rep
rod.
201
1, 2
6 (1
0):2
709-
2712
.doi
: 10.
1093
/hu
mre
p/de
r260
59Ye
sLe
ft lo
wer
ab
dom
inal
pai
nPe
ri-a
ortic
mas
s w
ith u
rete
ral
obst
ruct
ion
YE
ST
HB
SO*
No
Yes
(Con
juga
ted
equi
ne
estr
ogen
)
CT
** g
uide
d bi
opsy
reve
aled
en
dom
etri
osis
Exc
isio
n of
the
tum
or
with
rese
ctio
n an
d lig
atio
n of
infe
rior
ve
na c
ava
End
omet
rios
is
Tab
le 1
: Sum
mar
y of
stud
ies o
f end
omet
rios
is in
wom
en a
fter
tota
l hys
tere
ctom
y w
ith b
ilate
ral s
alpi
ngo-
ooph
orec
tom
y (T
HB
SO).
-cont
inue
d

230
Oman Medical Specialty Board
Cas
e no
Ref
eren
ceA
geM
eno-
paus
e st
atus
Mod
e of
pr
esen
tati
onC
linic
al
feat
ures
Past
his
tory
of
en
dom
etri
osis
Past
his
tory
of
surg
ery
His
tory
of
horm
onal
tr
eatm
ent f
or
endo
met
rios
is
Past
his
tory
of
HR
T**
*P
re-o
pera
tive
diag
nosi
s mad
eT
reat
men
tH
isto
logy
8Jo
seph
J, R
eed
CE
, Sa
hn S
A. Th
orac
ic
endo
met
rios
is. R
ecur
renc
e fo
llow
ing
hyst
erec
tom
y w
ith b
ilate
rals
alpi
ngo-
ooph
orec
tom
y an
d su
cces
sful
tr
eatm
ent w
ith ta
lc
pleu
rode
sis.
Che
st. 1
994
Dec
;106
(6):1
894-
6.
30Ye
sIn
term
itten
tri
ght-
and
left
-si
ded
pleu
ritic
ch
est p
ain,
he
mop
tysi
s of
6-ye
ars'
dura
tion,
and
re
cent
ple
ural
eff
usio
n.
Dec
reas
ed v
ocal
fr
emitu
s and
di
min
ishe
d br
eath
soun
ds in
th
e le
ft b
ase,
Thor
acen
tesi
s re
veal
eda
hem
orrh
agic
flu
id
Yes
TH
BSO
* +
pa
st h
isto
ry o
f th
orac
otom
y an
d ex
cisi
on o
f ri
ght l
ung
bleb
san
d pl
eura
l ab
rasi
on
wer
e do
ne
for r
ecur
rent
pn
eum
otho
rax
for r
ecur
rent
en
dom
etri
osis
.
Yes (
dana
zol)
Yes (
estr
ogen
an
d pr
oges
tero
ne)
End
omet
rios
isT
alc
Ple
urod
esis
for
recu
rren
t tho
raci
c en
dom
etri
osis
End
omet
rios
is
9R
ana
N, R
otm
an C
, H
asso
n H
M, R
edw
ine
DB
, D
mow
ski W
P. O
vari
an
rem
nant
synd
rom
e af
ter
lapa
rosc
opic
hys
tere
ctom
y an
d bi
late
rals
alpi
ngo-
ooph
orec
tom
y fo
r sev
ere
pelv
ic
endo
met
rios
is.
J Am
Ass
oc G
ynec
ol L
apar
osc.
1996
May
;3(3
):423
-6.
33Ye
sV
agin
al
blee
ding
and
pe
lvic
pai
n
Cys
tic le
sion
in
the
pelv
isYe
sH
ad
Supr
acer
vica
l hy
ster
ecto
my
and
BSO
fo
llow
ing
faile
d m
edic
al
man
agem
ent
for
endo
met
rios
is,
but h
ad
recu
rren
ce in
sp
ite o
f med
ical
m
anag
emen
t of
endo
met
rios
is
Yes
(cyc
lic-
nore
thin
o-dr
one
acet
ate)
Yes (
ethi
nyl
estr
adio
l)E
ndom
etri
osis
Vag
inal
rese
ctio
n of
th
ece
rvic
al st
ump
and
lapa
rosc
opic
rese
ctio
n of
the
ovar
ian
rem
nant
.
End
omet
rios
is
*TH
BSO
: Tot
al h
yste
recto
my
with
bila
tera
l sal
ping
o-oo
phor
ecto
my,
**C
T: C
ompu
ted to
mog
raph
y, **
*HRT
: Hor
mon
al re
plac
emen
t the
rapy
Tab
le 1
: Sum
mar
y of
stud
ies o
f end
omet
rios
is in
wom
en a
fter
tota
l hys
tere
ctom
y w
ith b
ilate
ral s
alpi
ngo-
ooph
orec
tom
y (T
HB
SO).
-cont
inue
d
Oman Medical Journal (2014) Vol. 29, No. 3:226-231

231
Oman Medical Specialty Board
Oman Medical Journal (2014) Vol. 29, No. 3:226-231
Conclusion
Endometriosis after surgical menopause is rare and symptoms can vary based on the site of endometriotic implants. Sometimes endometriosis can present with symptoms which can mimic pelvic malignancies and also since endometriosis confers the risk of malignant transformation, this makes it difficult for a treating physician to make appropriate pre-operative diagnosis. Although endometriosis after surgical menopausal is rare, it should be considered in the differential diagnosis of abdominal or pelvic mass, especially in women with past history of endometriosis.
Acknowledgements
We would like to thank Professor Soo Khee Chee and A / Prof Koong Heng Nung for their help with the design of the study protocol. No conflict of interests or funding to declare.
References
1. Manero MG, Royo P, Olartecoechea B, Alcázar JL. Endometriosis in a postmenopausal woman without previous hormonal therapy: a case report. J Med Case Rep 2009;3:135.
2. Punnonen R, Klemi PJ, Nikkanen V. Postmenopausal endometriosis. Eur J Obstet Gynecol Reprod Biol 1980 Dec;11(3):195-200.
3. Matorras R, Elorriaga MA, Pijoan JI, Ramón O, Rodríguez-Escudero FJ. Recurrence of endometriosis in women with bilateral adnexectomy (with or without total hysterectomy) who received hormone replacement therapy. Fertil Steril 2002 Feb;77(2):303-308.
4. Fedele L, Bianchi S, Raffaelli R, Zanconato G. Comparison of transdermal estradiol and tibolone for the treatment of oophorectomized women with deep residual endometriosis. Maturitas 1999 Aug;32(3):189-193. .
5. Munksgaard PS, Blaakaer J. The association between endometriosis and ovarian cancer: a review of histological, genetic and molecular alterations. Gynecol Oncol 2012 Jan;124(1):164-169. Published online 26 Oct 2011.
6. Munksgaard PS, Blaakaer J. The association between endometriosis and ovarian cancer: a review of histological, genetic and molecular alterations. Gynecol Oncol 2012 Jan;124(1):164-169. Published online 26 Oct 2011.
7. Mabrouk M, Vicenzi C, Ferrini G, Geraci E, Forno SD, Caprara G, et al. Mixed adenocarcinoma of the rectovaginal septum associated with endometriosis and endometrial carcinoma: a case report. Case Rep Oncol 2011 Jan;4(1):149-154. Published online 18 Mar 2011.
8. Cakir E, Aydin E, Durmus NI, Samdanci E, Sahin N, Nurkabul Z. Prımary Ovarıan Clear Cell Adenofıbroma of Borderlıne Malıgnancy. Oman Med J 2012;27(1) online publication.
9. Goumenou A, Matalliotakis I, Mahutte N, Koumantakis E. Endometriosis mimicking advanced ovarian cancer. Fertil Steril. 2006 Jul;86(1):219.e23-5.
10. Yap C, Furness S, Farquhar C. Pre and post operative medical therapy for endometriosis surgery. Cochrane Database Syst Rev 2004;(3):CD003678. doi:10.1002/14651858.CD003678.pub2.
“Submit Proceedings of Conferences or Workshops As Supplements To OMJ”
• Proceedings of conferences or workshops will be considered as a supplement to the Oman Medical Journal.
• Original work or abstracts will be accepted.
• Material in supplements will be included with the regular issue of the journal or will be distributed separately as supplement.
• Supplements will also be available on the Oman Medical Journal website.