Embed Size (px)
Citation preview

Endogenous antibody interference inimmunoassays
Ellen Anckaert, M.D., Ph.D.Dienst Klinische Chemie en Radio-immunologieUZ Brussel

To help protect your privacy, PowerPoint has blocked automatic download of this picture.
False positive serum hCG values have lead to cancermisdiagnosis
Jury awards $15.5 million to woman misdiagnosed with cancerUniversity of Washington and diagnostic company share blame
Photo: Grant M. Haller/Seattle Post-IntelligencerPublished June 29, 2001

Interference by endogenous antibodies inimmunoassays: an ongoing story
J Clin Endocrinol Metab 2016
J Clin Endocrinol Metab 2015
RARE CAUSES
J Clin Endocrinol Metab 2014
FREQUENT CAUSES

Immunoassay interference by endogenousantibodies
Antibodies againstassay antibodies
Antibodiesagainstanalyte
Antibodies againstsignal molecules

Endogenous antibodies against assay antibodies
Possible clinical consequences:• Misclassification of monitoring results• Unnecessary follow-up examinations• False therapy decisions• Unfavorable patient prognosis

Mechanisms of interference by heterophilicantibodies
Bridging of capture anddetector antibodies=> Falsely elevated result
Exclusive binding of capture or detector antibodyonly=> Falsely lowered result

Endogenous antibodies against assay antibodies
Heterophilic
antibodies
Human anti-mouseantibodies (HAMA)
Rheumatoid factor
Etiology Poorly defined,
no clear immunogen
Known antigenicstimulus
Auto-antibody
Specificity Low:
bind different species Ig
High Low: bind Fcregion of differentspecies Ig
Affinity Low High Low
Titer Low High High in activerheumatic disease
Ig class IgG, IgM IgG, IgA, IgM Usually IgM
Prevalence 40% In 40-70% ofpatients treatedwith mouse Mabs
Up to 10% gen. pop
5-10% gen. pop
70% autoimmunerheumatic disease

1. Addition of a combination of blocking agents
Addition of a “blocking agent” of the same species as the assayantibodies:- animal normal serum- animal nonimmune immunoglobulin- aggregated mouse monoclonal IgG1 (MAK33) to eliminate strong HAMAinterferences, usually therapy induced

2. Fragmentation of antibodies
Use of Fab orF(ab’)2 fragments
Single chainfragments scFv

Variable region from mouse
IgG
C1 constant region from
human IgG
Fc-fragment cleaved off
3. Chimeric antibody fragments
Constructed from 2 different species (mouse / human )

Prevalence of interference
l Prevalence of interference depends on the immunoassay (IA) method
l Bjerner, Clin Chem 2002 (CEA, 11.261 patient samples)g unblocked IA 4%g Fc removal 0.1%g Heat-treated MAK33 0.06%

Assay design: measures against heterophilicantibody interference
No protection
Use of blocking proteins
Fragmentation of Antibodies
Use of chimeric MABs
Interference level:High: <5-15% Low: <= 0,05%
Interference is not completely eleminated

What can the lab do to detect immunoassayinterference?
1. Repeat the analysis with an alternative immunoassay,preferably using assay antibodies from a different species
2. Treat the sample with an additional blocking agent(Heterophilic Blocking Tubes, Scantibodies)
3. Serial dilution: non linearity indicates assay interference
Use several measures: a single negative interference test doesnot exclude interferenceMarks (Clin Chem 2002): blood from 10 donors with interference in one immunoassay
• 8.7% of 3445 immunoassay results were ‘falsely increased’
• half of these were not corrected by HBT

Immunoassay interference by endogenousantibodies
Antibodies againstassay antibodies
Antibodiesagainstanalyte
Antibodies againstsignal molecules

Interference in immunoassays by autoantibodiesagainst analytes
l Antibodies leading to macrohormones:
l Anti-prolactin (macro-prolactin)
l Anti-TSH (macro-TSH)
l Anti-calcitonin (macro-calcitonine)
l Anti-thyroglobulin antibodies
l Anti-insulin antibodies
l ...

Circulating forms of prolactin
MACROPROLACTINEMIA: hyperprolactinemia with an elevated % ofcirculating PRL consisting of BIOLOGICALLY INACTIVE macroprolactin
• 1-4% of general population• 4-40% in patients with hyperPRL• > 90% of cases: macroPRL = PRL-IgG complex• macroPRL accumulates in circulation due to decreased renal clearance

titel17 27-10-2016
Causes of hyperprolactinaemia
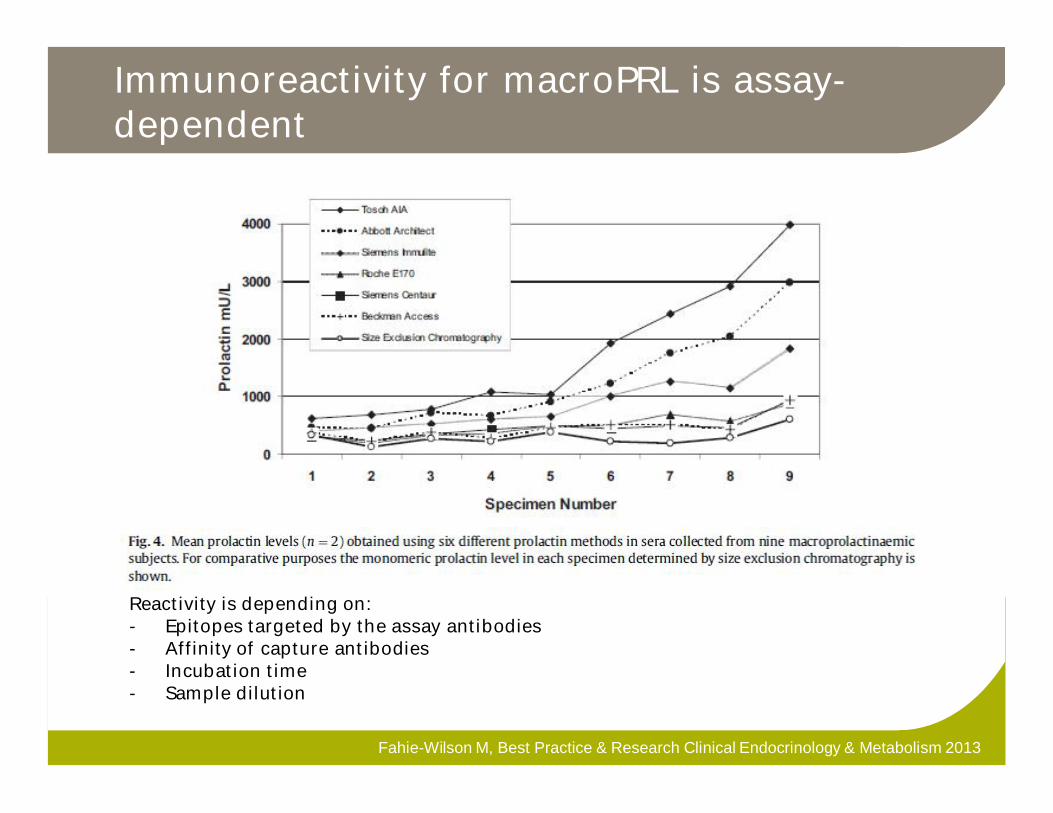
Immunoreactivity for macroPRL is assay-dependent
Fahie-Wilson M, Best Practice & Research Clinical Endocrinology & Metabolism 2013
Reactivity is depending on:- Epitopes targeted by the assay antibodies- Affinity of capture antibodies- Incubation time- Sample dilution

PEG-precipitation for detection ofmacroprolactin
• 200 µL serum + 200 µL PEG 6000 25% (g/v) in PBS buffer in conical tube(room temperature)
• vortex , centrifuge and measure PRL in supernatant• % recovery = (PRL supernatant * 2)/PRL serum *100
³ 60% = absence of macroPRL (method-dependent!)• Monomeric PRL after PEG

Macro-TSH
l Macro-molecule composed of TSH and anti-TSHimmunoglobulin
l Reduced renal clearance leads to accumulation ofmacro-TSH
l Macro-TSH is biologically INACTIVEg Patients are typically clinically EUTHYROID
g Typically: (grossly) elevated TSH with normal FT4

Variable detection of macro TSH bycommercial immunoassays
Hattori, 2016

What can the lab do to detect macro-TSH?
1. REPEAT ANALYSIS WITH ALTERNATIVE IMMUNOASSAY:results VARY depending on immunoreactivity with macro-TSH
2. TREAT SAMPLE WITH BLOCKING AGENT: NO EFFECT
3. SERIAL DILUTION:
gMacro-TSH: dissociation ↑ or nl TSH recovery
g Heterophilic antibody interference: ↓ TSH recovery
4. PEG-PRECIPITATION of high molecular weight proteins:
gMacro-TSH: ↓ TSH recovery
g Heterophilic antibody interference ↓ TSH recovery
5. Mix with hypothyroid serum (= high TSH) sample:
gMacro-TSH: free anti-TSH binds TSH ↓ TSH recovery

Confirmation of macro-TSH by gel filtrationchromatography
Patient serum: TSH peak fraction thatapproximates the molecular size of IgG (dots).
Patient serum incubated with hypothyroidserum: HMW fraction, confirming excessTSH binding capacity and macro-TSH(trangles).
Loh T P, JCEM 2012

Clinical characteristics of macro-TSH patients
Case Sex Age Thyroidantibodypositive
Clinicalsigns/symptoms
TSH (mIU/l) Immunoassay
1 F 56 Anti-Tg No 274 Elecsys
2
3
F
-
mother
newborn
-
-
No
No
308
828
Elecsys
Elecsys
4
5
6
F
-
F
28
45
23
Neg
Neg
TRAb
No
No
Graves HT
5.1
22
9.7
Elecsys
Elecsys
Elecsys
7
8
F
F
mother
newborn
-
Neg
No
No
55
103
Elecsys
Delfia
9 F 46 Neg No 24.5 Elecsys
10 M 60 Anti-TPO No 232 Vitros
11 M 29 -
-
No 40-115 RIA
12
13
F
F
53
6
Neg
Neg
No
No
1.4 ->100
2.7 ->100
Immunoassay
Immunoassay
Reviewed by Loh, JCEM 2013

Vertical transmission of anti-TSH antibody
Rix, Acta Paediatr 2011

Prevalence of macro-TSH
Method: systematic screening of samples with elevated TSH by PEGprecipitation and confirmation by GFC
• Mills 2013: TSH > 10 mIU/l (Roche Elecsys)• 3/495 (0,6%)
• Hattori 2015: elevated TSH, normal FT4 (Vitros)• 10/681 (1,5%)
• Hattori 2016: TSH > 4 mIU/L, normal FT4 (EIA)• 15/1901 (0,8%)

Other macro-hormones
J Clin Endocrinol Metab 2016
Other case reports: macro-LH, macro-FSH, ...

Tg antibody interference in Tg immunoassays
l Sensitive Thyroglobulin (Tg) measurement is important forfollow-up of differentiated thyroid carcinoma (DTC)
l No Tg method is completely free from anti-Tg interference
g Frequent underestimation in non-competitive assay
g Rare false elevation is possible in competitive assay
l Anti-Tg antibody prevalence
g 10% general population
g 25% in DTC
g 60% in autoimmune thyroid diseaseDifferent epitope recognition patterns

Tg antibody interference in Tg immunoassays
Anti-Tg interference in Tg IMA is a common problem

Tg antibody interference in Tg immunoassays
l What can the lab do:g Comment on Tg value ‘not reliable in case of anti-Tg’g Confirm by an alternative method (RIA, LC-MSMS)g Exogenous Tg recovery test
l low recovery indicates interferencel normal recovery does not exclude interference
l TgAbs can be used as a surrogate tumour marker
l Guidelines: measurement of Tg in follow-up of DTC shouldalways be accompanied by anti-Tg measurement using asensitive anti-Tg immunoassay

TgAb immunoassay
J Clin Endocrinol Metab 2011
Even when cut-off is based on analyticalsensitivity: failure to detect interferencein 20-30% of cases
Analytical sensitivityCut-off provided by manufacturer

Immunoassay interference by endogenousantibodies
Antibodies againstassay antibodies
Antibodiesagainstanalyte
Antibodies againstsignal molecules

Interference by anti-ruthenium antibodies inFT4 – FT3 immunoassays
Anti-Ru antibodies
l Mainly in areas with textile industryg Use of Ru in dying process of clothing
g Ru in environment, clothing or food chain
l Estimated frequency of interference in first generationelectrochemiluminescence FT3 assay: 0.2% (Sapin, Clin ChemLab Med 2007)

Anti-RU interference in FT4 – FT3immunoassay

Protection against anti-Ru antibodies in nextgeneration immunoassay
The sulfo-RU label is less recognized by anti-RU
Current generationOlder generation

Case report
Visit Normal values4 3 2 1
TSH (mIU/l) 0.552 0.344 0.569 0.515 0.27-4.2
FT3 (ng/l) 3.2 5.9 7.0 6.2 2.6-4.4
FT4 (ng/l) 12.6 20.8 21.2 19.5 9.3-17.0
Inappropriate TSH secretion:- Thyrotropinoma (1/1.000.000)- Thyroid hormone resistance (1/50.000)
Switch to current generation FT3 and FT4assays

Biotin
Streptavidin
Antibodies against other assay components
Biotin IgM antibodies present in 3%of Finish population interfere in EIA(Chen, PlosOne 2012)
Case report: interference by anti-streptavidin in ECLIA (Johnson Rulander, ArchPatol Lab Med 2013)

Immunoassay interference
l Frequent causes of interference (macro-PRL, anti-Tg)require a systematic approach
l No method is completely free from interference
g be aware of the susceptibility of a particular commercialimmunoassay to interference
g clinician should be actively encouraged to contact the laboratoryin case of any doubt
l In case of confirmed interference:
g Patient medical record should contain information about thepresence of interfering substances in serum
g Manufacturer should be noticed


Interference by endogenous antibodies inFT4 – FT3 assays
Anti-T4 and anti-T3 antibodies
l Prevalence depends on the selected population and themethod of detection
l £20% in autoimmune thyroid disease
l 6% in non-thyroidal autoimmune disease
l 0-2% in healthy individuals
l women > men
l Mostly IgG subclass, mostly polyclonal
l Most patients also have anti-Tg and/or anti-microsomalantibodies
l Impact on immunoassay (interference) depends onl the assay format
l titer, affinity and specificity of the antibody

One step method - Labeled Analog
SerumBindingProtein
T4
FT4+ + *
Anti - T4 AntibodyBound to Particle
+
*SeparateandCount
X*
ConjugatedAnalog


Clinically inconsistent TSH result
Perform serial dilution of the sample and measure TSH
Repeat the measurement of TSH on an alternative platform
Screen for macro-TSH if unexplainedassay interference
Likely heterophile antibodies interference
Heterophile blocking tube studies
Likely interference by rheumatoid factors
Measure rheumatoid factors
Linear recovery
Non-discrepantresult
Normal recoveryNegative
Assay interference unlikely
Low recovery
Positive
Non-linearrecovery
Discrepantresult
Mix with hypothyroid patient serum
GFC

Heterophilic antibody / HAMA interference
l Prevalence of interference depends on the immunoassay (IA)method
l Bjerner 2002 (CEA, 11.261 patient samples)g unblocked IA 4%g blocked IA (Fc removal) 0.1%g blocked IA (Fc removal – MAK33) 0.06%
l Boscato 1986 (hCG IRMA, 668 healthy subject samples)g unblocked IA 15%g blocked IA 0.6%
l Ward 1997 (TSH, 21.000 patient samples)g blocked IA 0.03%
Þ addition of “blocking reagent” reduces interference, but isno garantee for complete elimination of interference
Þ estimated prevalence: 0.03 – 3%

titel45 27-10-2016
Major forms of PRL in serum
Variant MW %
Monomeric hPRL 23 kDa 85
BigPRL 60 kDa 10
BigBig PRL= MacroPRL
>150 kDa 1 - 5
Macroprolactinemia:• Hyperprolactinemia where an elevated fraction of circulating PRL
consists of biologically inactive macroprolactin• Prevalence: 1-4% of general population, 4-40% in patients with
hyperPRL• > 90% of cases: macroPRL = PRL-IgG complex

Case report macro-TSH (1)
l 60 year old man, clinically euthyroidg TSH1 232 mIU/l (0.45-5 mIU/l)
g FT4 10 pmol/l (10-23 pmol/l)
g TPO Ab 496 IU/ml (0-50 IU/ml)
g Tg Ab Neg
g anti-TSH receptor Abs Neg
l Test with an alternative immunoassay methodg TSH2 122mIU/l
1 Vitros 5600, Ortho Clinical Diagnostics; 2 Advia Centaur, Siemens Healthcare Diagnostics
l Test dilution linearity3:l TSH 1:1 122mIU/l
l TSH 1:10 165 mIU/l (135% recovery)
3 TSH assay diluent and immunoassay: Advia Centaur
l Test for antibodies against assay antibodiesl RF Negative
l Heterophilic blocking tubes No interference detected
Loh T P, JCEM 2012





























