Embed Size (px)
Citation preview

Endocrine Treatment of Early Breast Cancer
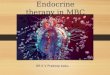
Sites of oestrogen synthesis
Miller WR. Best Pract Res Clin Endocrinol Metab 2004; 18(1): 1–32
Premenopausal women
• Oestrogen produced in the ovaries
• At some stages of the menstrual cycle,
up to 50% may be produced elsewhere
Postmenopausal women
• Ovaries no longer produce oestrogens
• Synthesis takes place in adipose tissue,
skin, liver, muscle and breast tissue

Hormonal therapy
• Hormonal treatments are only effective in HR+ve tumours1
• Two thirds of postmenopausal breast cancers are oestrogen dependent2
• Two major strategies for affecting oestrogen deprivation:
1. ER blockade
2. inhibition of oestrogen synthesis
1. Miller WR. Best Pract Res Clin Endocrinol Metab 2004; 18(1): 1–32
2. Brueggemeier R. Breast Cancer Res Treat 2002; 74(2): 177–185

The role of tamoxifen
• The benchmark for newer treatments
• 5 years of tamoxifen therapy was the current gold standard for adjuvant hormonal therapy in postmenopausal ER+ve breast cancer1
• Early Breast Cancer Trialists’ Collaborative Group (EBCTCG)
meta-analyses (15 year follow-up): – Annual recurrence rate almost halved (recurrence rate ratio
0.590.03)2
– Breast cancer mortality rate reduced by one third (death rate ratio 0.66 0.04)2
• The efficacy of tamoxifen can be improved upon
1. Ravdin PM. Medscape Hematology-Oncology 2004: 7(2)
2. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Lancet 2005; 365(9472): 1687–1717

Current Endocrine Therapy Protocol for Early Breast Cancer
• Premenopausal
– Tamoxifen
– Ovarian ablation • Intolerant of Tam or
??high risk patients

Current Endocrine Therapy Protocol for Early Breast Cancer
• Post-menopausal – PATIENTS AT FIRST PRESENTATION: – There are no clear data to guide management in this group – International guidlines support the use of either an initial aromatase
inhibitor, or the initiation of tamoxifen with a subsequent switch to an aromatase inhibitor after 2-3 years. (NCCN, St. Gallen)
– It is suggested that the majority of patients are treated with TAMOXIFEN FOR 2-3YRS FOLLOWED BY EXEMESTANE OR ANASTRAZOLE OR FOR 2-3YRS FOR A TOTAL TREATMENT DURATION OF 5YRS.
– Patients with contraindications to TAMOXIFEN should continue to be treated with ANASTRAZOLE for 5years.
– Given the current uncertainties regarding the optimal use of aromatase inhibitors in the adjuvant setting, the choice of treatment should be made after discussion between the responsible clinician and the woman about the risks and benefits of each option
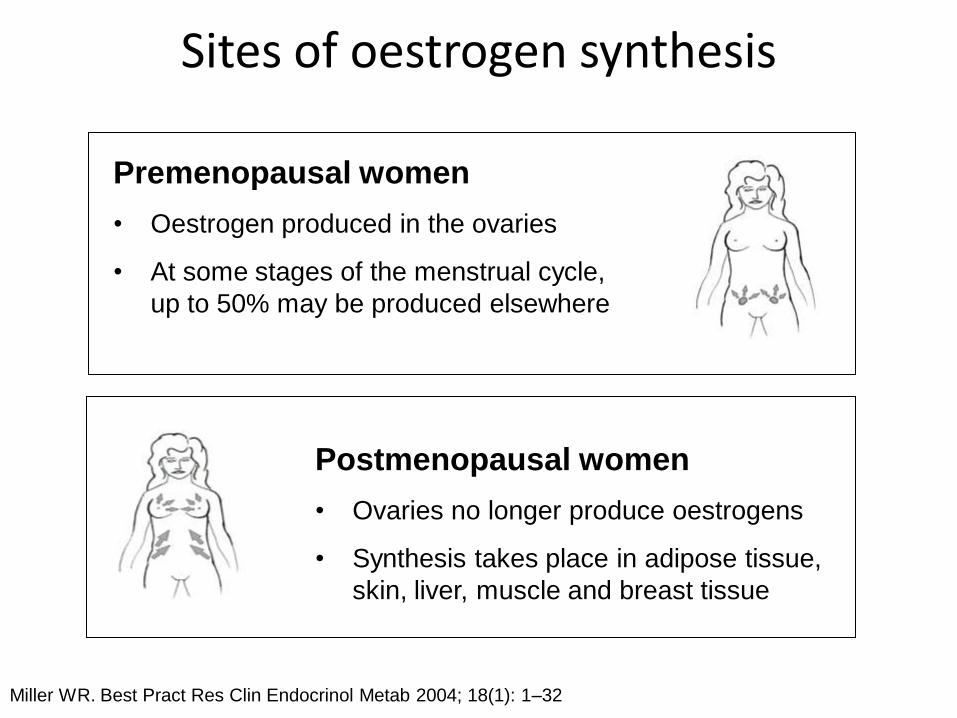
Adjuvant Hormonal Therapy Trial Designs
SUPPORTING TRIALS
• ATAC
• BIG 1-98 straight arm
• TEAM (not yet reported)
EARLY ADJUVANT (START)
Randomization
SUPPORTING TRIALS
• IES
• ITA
• ARNO/ABCSG combined analysis *
SWITCHING
Randomization
*
EXTENDED ADJUVANT SUPPORTING TRIALS
• MA-17
• ABCSG 6a
Randomization
* Note that some patients from the original newly diagnosed population
are lost due to recurrence or adverse events prior to randomization
SUPPORTING TRIALS
• ABCSG 8 alone (arms A & C)
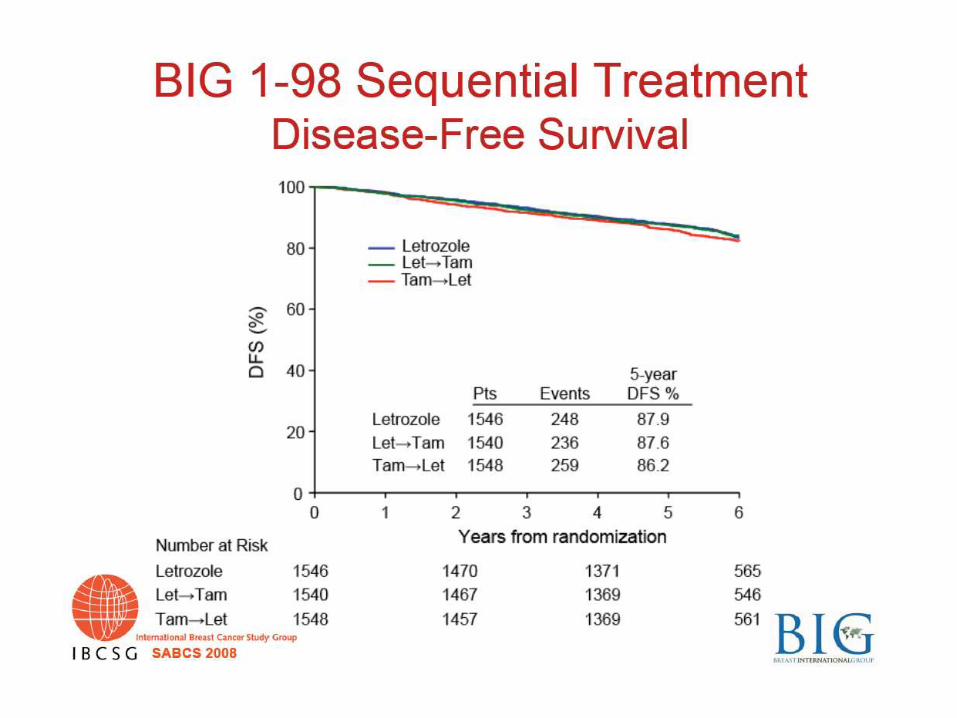
• BIG 1-98 sequencing arms (arms C&D)
Randomization
SEQUENCING
A B
C D

ATAC trial design
Tamoxifen
(n = 3116)
ITT population
n = 3125
Safety population
n = 3092
HR+ subpopulation
n = 2618
ITT population
n = 3116
Safety population
n = 3094
HR+ subpopulation
n = 2598
ITT, intent-to-treat; HR+, hormone receptor-positive
Anastrozole
(n = 3125) Combination
n=3125
Discontinued following
initial analysis as no
efficacy or tolerability
benefit compared with
tamoxifen arm
Postmenopausal women with invasive breast cancer
(n = 9366)
Surgery radiotherapy chemotherapy
Randomisation 1:1:1 for 5 years

Time to recurrence HR+ patients
2618
2598
2541
2516
2453
2400
2361
2306
2278
2196
2159
2075
1995
1896
1801
1711
1492
1396
608
547
At risk:
A
T
Patients
(%)
30
25
20
15
10
5
0
0 1 2 3 4 5 6 7 8 9
30
25
20
15
10
5
0
12.5% 17.0%
21.8%
Follow-up time (years)
9.7%
2.8% 4.8%
Absolute
difference
HR+
HR
0.76
95% CI
(0.67, 0.87)
p-value
0.0001
Tamoxifen (T)
Anastrozole (A)
The ATAC Trialists’ Group. Lancet Oncol 2008; 9: 45-53

†included as a non-predefined adverse event of interest
Predefined adverse events at any time on treatment or any severity
Hot flushes
Nausea and vomiting
Fatigue / tiredness (asthenia)
Mood disturbances
Musculo-skeletal disorders
Vaginal bleeding
Vaginal discharge
Ischaemic cardiovascular disease
Ischaemic cerebrovascular event
Venous thromboembolic events
Deep venous thromboembolic events
Cataracts
Carpal tunnel syndrome†
1102 (35.6)
394 (12.7)
578 (18.7)
599 (19.4)
1104 (35.7)
167 (5.4)
110 (3.6)
130 (4.2)
64 (2.1)
87 (2.8)
48 (1.6)
189 (6.1)
79 (2.5)
1263 (40.8)
358 (12.4)
544 (17.6)
555 (17.9)
915 (29.6)
319 (10.3)
409 (13.2)
106 (3.4)
91 (2.9)
141 (4.6)
75 (2.4)
218 (7.0)
22 (0.7)
Anastrozole
(N = 3092)
Tamoxifen
(N = 3094)



The Intergroup Exemestane Study
Coombes RC, Hall E, Gibson LJ et al
N Engl J Med 2004; 350(11): 1081–1092
Coombes RC, Hall E, Snowdon CF et al. Updated survival analysis. Data presented at the 27th San Antonio Breast Cancer Symposium, December
2004

Disease-free survival
Coombes RC, Hall E, Snowdon CF et al. Data presented at the 27th San Antonio Breast Cancer
Symposium, December 2004
* Events occurring more than 4 years after randomisation
Women surviving
event free (%)
Years from randomisation
0 1 2 3 4
0
25
50
75
100
Number of events/at risk
Hazard ratio = 0.73 (95% CI: 0.62–0.86)
Log-rank test: p=0.0001
Exemestane
Tamoxifen
0/2,352 57/2,233 65/2,081 75/1,413 41+24*/661 0/2,372 82/2,243 105/2,062 96/1,359 47+23*/650 Tamoxifen
Exemestane
(262 events)
(353 events)

Overall survival
Coombes RC, Hall E, Snowdon CF et al. Data presented at the 27th San Antonio Breast Cancer
Symposium, December 2004
0 1 2 3 4
0
25
50
75
100
Hazard ratio: 0.83
95% CI: 0.67–1.02
Log-rank test: p=0.08
Exemestane (152 deaths)
Tamoxifen (187 deaths)
Pati
en
ts a
live (
%)
18/2,270 41/2,137 41/1,469 37+15*/690
23/2,300 53/2,165 49/1,465 41+21*/701 Tamoxifen
Exemestane
* Events occurring more than 4 years after randomisation
0/2,352
0/2,372
Years from randomisation Number of events/at risk

Switching to Arimidex
• ABCSG trial 8 and ARNO 95
• Reported in The Lancet 6th August 05
• Similar results
– Median follow up 30.1 months
– 40% reduction in risk of an event (local or distant metastases or contralateral breast primary)
– Similar survival benefit to that seen in IES for switch
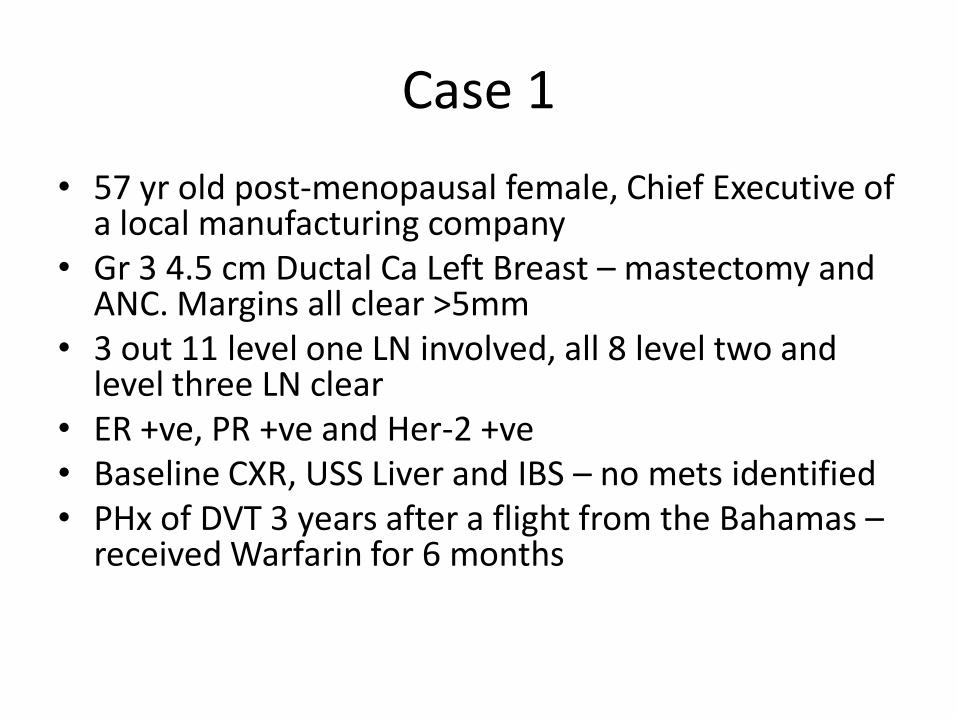
Case 1
• 57 yr old post-menopausal female, Chief Executive of a local manufacturing company
• Gr 3 4.5 cm Ductal Ca Left Breast – mastectomy and ANC. Margins all clear >5mm
• 3 out 11 level one LN involved, all 8 level two and level three LN clear
• ER +ve, PR +ve and Her-2 +ve • Baseline CXR, USS Liver and IBS – no mets identified • PHx of DVT 3 years after a flight from the Bahamas –
received Warfarin for 6 months

Q1. What is the most appropriate standard management of this lady?
1. Adjuvant Chemotherapy followed by radiotherapy followed by Herceptin, followed by hormone therapy
2. Adjuvant Chemotherapy followed by hormone therapy followed by Herceptin therapy
3. Adjuvant Chemotherapy and Radiotherapy concurrently followed by Herceptin and Hormone therapy
4. Adjuvant Chemotherapy followed by Radiotherapy followed by Herceptin together followed by Hormone therapy
5. Adjuvant Chemotherapy followed by Herceptin and Hormone therapy
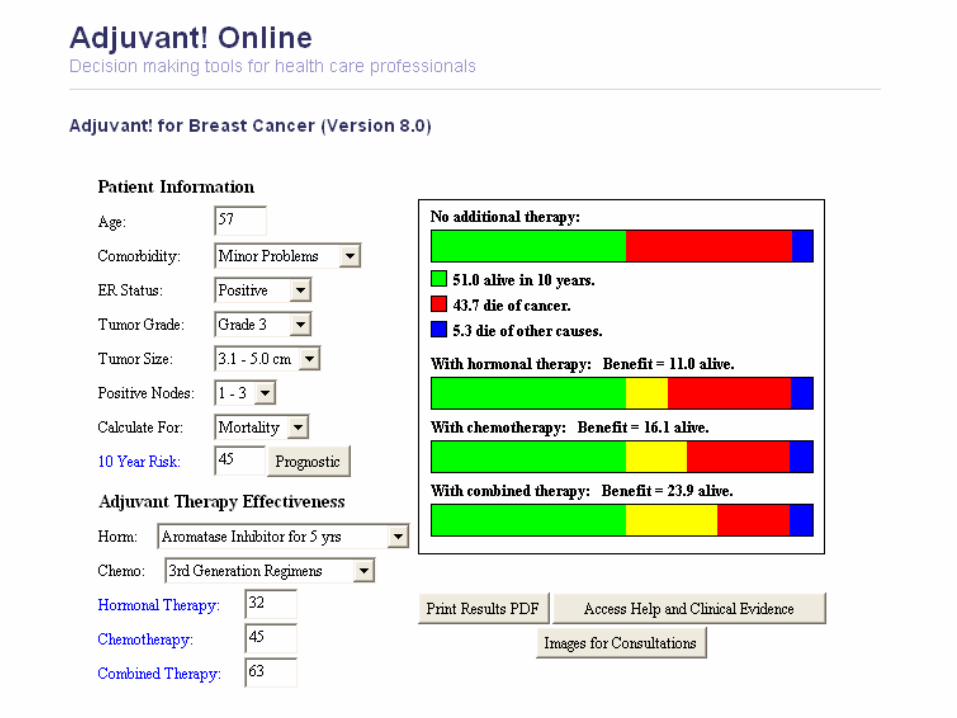

Combined Benefit is 23.9%,
Net chemo benefit is: 23.9-11.0 = 12.9%

Q1. Answer
Adjuvant Chemotherapy followed by Herceptin and Hormone therapy
Radiotherapy not routinely indicated in 1 to 3 nodes positive group. However could offer entry into the Supremo trial.
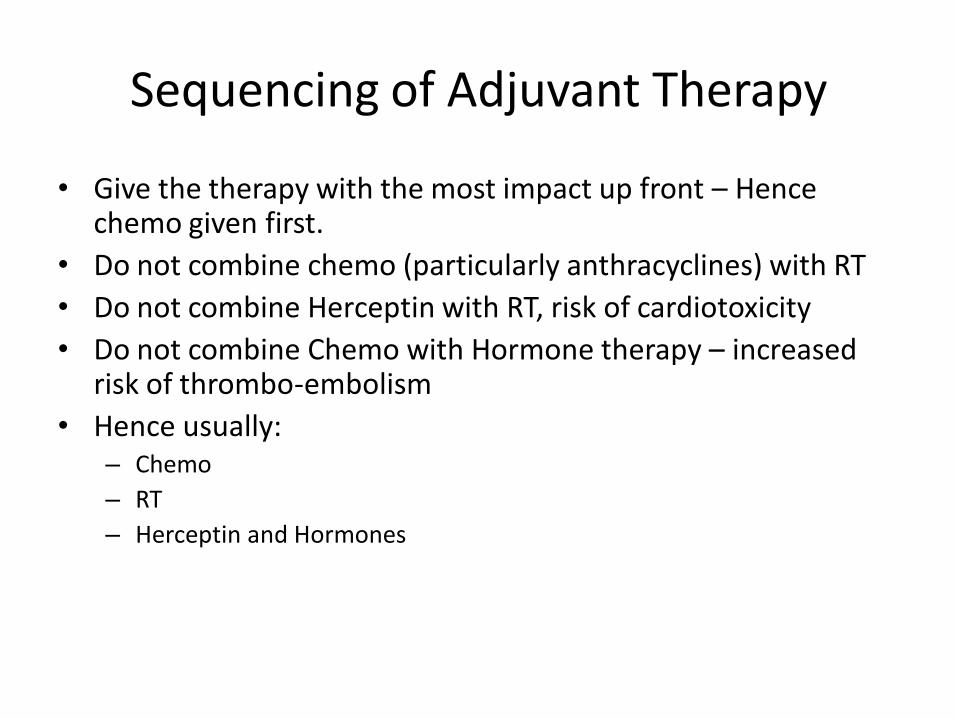
Sequencing of Adjuvant Therapy
• Give the therapy with the most impact up front – Hence chemo given first.
• Do not combine chemo (particularly anthracyclines) with RT
• Do not combine Herceptin with RT, risk of cardiotoxicity
• Do not combine Chemo with Hormone therapy – increased risk of thrombo-embolism
• Hence usually: – Chemo
– RT
– Herceptin and Hormones

Q2. What Adjuvant Chemotherapy Would you chose?
1. FEC 60 for 6 cycles
2. FEC 100 for 6 cycles
3. FEC 100 for 4 cycles followed by Docetaxol for 4 cycles
4. FEC 100 for 3 cycles followed by Docetaxol for 3 cycles
5. Cyclophosamide and Docetaxol for 6 cycles

Q2 Answer
FEC 100 for 3 cycles followed by Docetaxol for 3 cycles
In node positive breast cancer the optimal therapy is a Taxane and Anthracycline based
regimen

EBTCG - Chemotherapy Survival benefit – absolute %
Under 50 yrs
50-69 years
Node positive 12% 3% Node negative 7% 2%

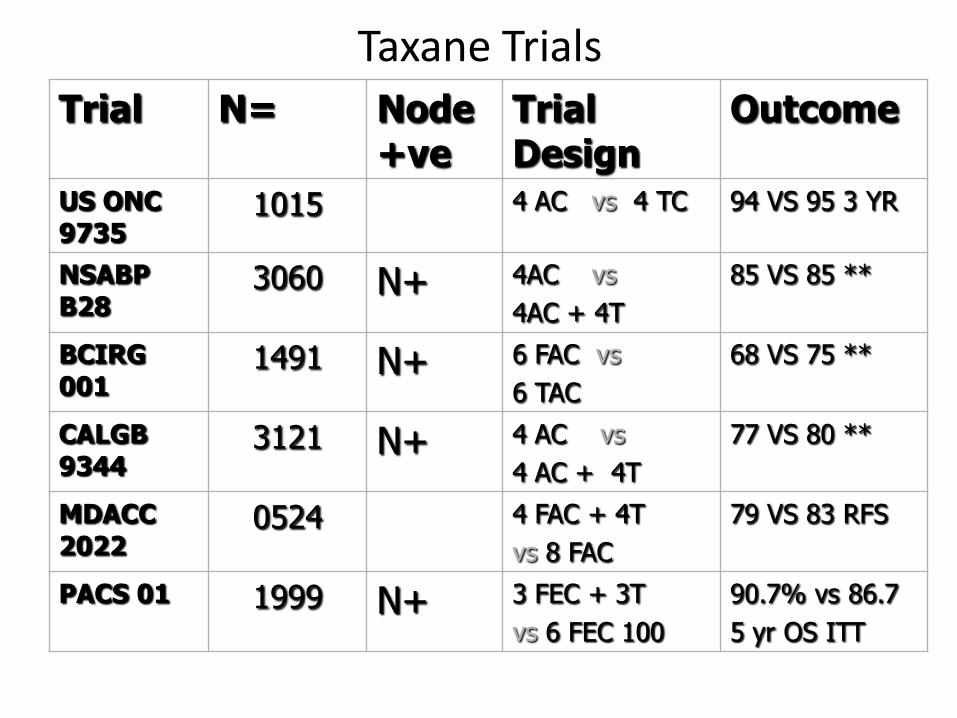
Taxane Trials
Trial N= Node +ve
Trial Design
Outcome
US ONC 9735
1015 4 AC vs 4 TC 94 VS 95 3 YR
NSABP B28
3060 N+ 4AC vs
4AC + 4T
85 VS 85 **
BCIRG 001
1491 N+ 6 FAC vs
6 TAC
68 VS 75 **
CALGB 9344
3121 N+ 4 AC vs
4 AC + 4T
77 VS 80 **
MDACC 2022
0524 4 FAC + 4T
vs 8 FAC
79 VS 83 RFS
PACS 01 1999 N+ 3 FEC + 3T
vs 6 FEC 100
90.7% vs 86.7
5 yr OS ITT
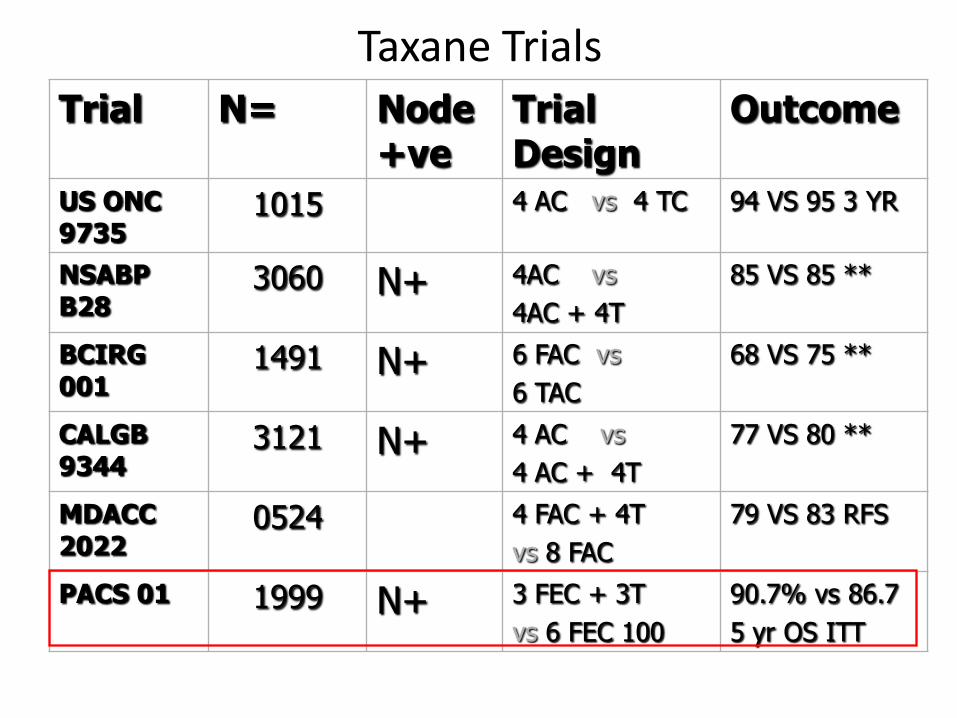
Taxane Trials
Trial N= Node +ve
Trial Design
Outcome
US ONC 9735
1015 4 AC vs 4 TC 94 VS 95 3 YR
NSABP B28
3060 N+ 4AC vs
4AC + 4T
85 VS 85 **
BCIRG 001
1491 N+ 6 FAC vs
6 TAC
68 VS 75 **
CALGB 9344
3121 N+ 4 AC vs
4 AC + 4T
77 VS 80 **
MDACC 2022
0524 4 FAC + 4T
vs 8 FAC
79 VS 83 RFS
PACS 01 1999 N+ 3 FEC + 3T
vs 6 FEC 100
90.7% vs 86.7
5 yr OS ITT

PACS 01 Overall Survival (ITT)
J Clin Oncol 2006;24(36):5664-71
Pro
ba
bil
ity
0.00
0.25
0.50
0.75
1.00
0 1 2 3 4 5 6 7 8
FEC → T: 90.7%
FEC: 86.7%
Log-rank unadjusted p=0.013
Log-rank adjusted p=0.017
HR (Cox model)=0.73 [0.56-0,94], p=0.050
Time (years)
0 2 116 397 835 913 958 987 996 FEC
0 1 106 427 876 936 966 997 1 003 FEC-T
N° at risk
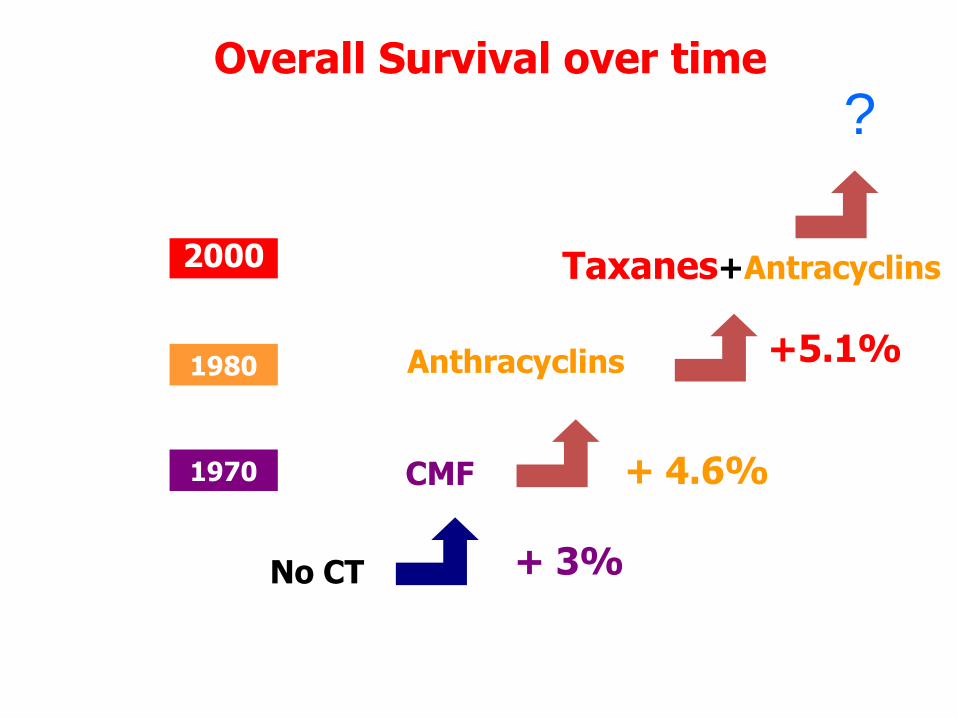
Overall Survival over time
No CT
CMF 1970
+ 3%
Anthracyclins
+ 4.6%
1980
Taxanes+Antracyclins 2000
+5.1%
?

Which hormone therapy would you offer?
1. Adjuvant Exemestane for 5 years
2. Adjuvant Anastrozole/Letrozole for 5 years
3. Adjuvant Tamoxifen for 2 years followed by Exemestane for 3 years
4. Adjuvant Tamoxifen for 2 years followed by adjuvant Anastrozole for 3 years
5. Adjuvant Tamoxifen for 5 years followed by adjuvant Letrozole for 5 years
Q3. Answer
Adjuvant Anastrozole/Letrozole for 5 years
In the setting of a prior personal history of venous thrombo-embolism, tamoxifen is
contra-indicated
Exemestane is not licensed for up-front usage
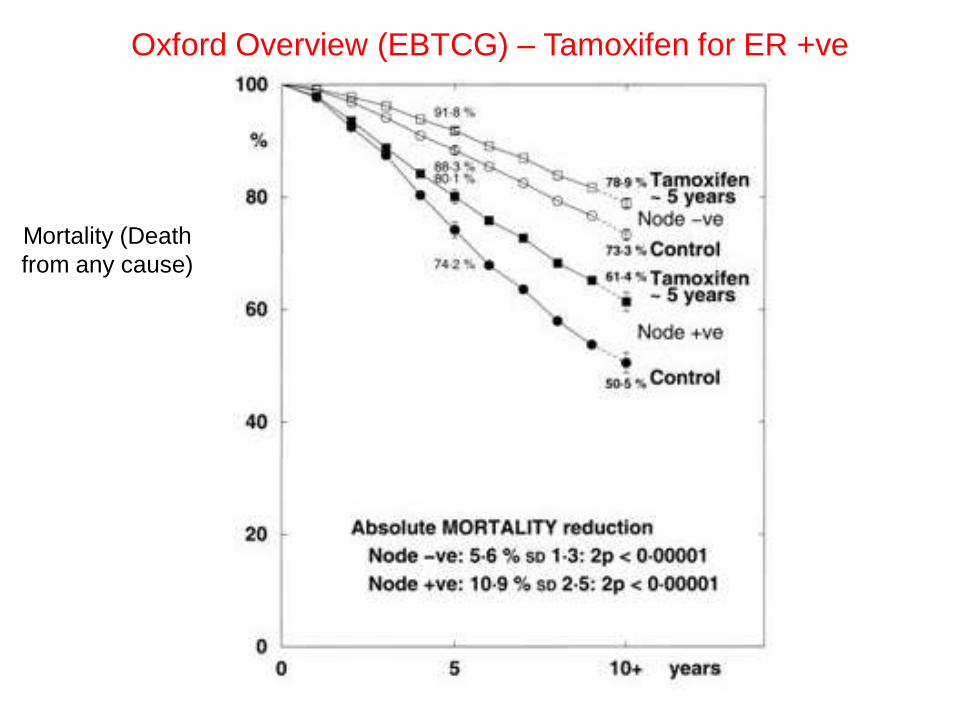
Mortality (Death
from any cause)
Oxford Overview (EBTCG) – Tamoxifen for ER +ve

When to use an upfront AI in place of Tamoxifen
• For those with contra-indications or increased risk with Tamoxifen (DVT, Endometrial Ca)
• Previous separate breast primary treated with Tamoxifen
• ? Those with high risk features (Her-2 +ve, GrIII, Node Positive)
• ? All adjuvant Patients
Case 2
• 49 year old female, post-menopausal, optician
• Gr II 1.8cm ER positive, Her negative, ductal ca – Right Partial Mastectomy
• Node negative, CXR, LFTs and Bone Profile normal
• No significant PHx
Q4. What is the most appropriate subsequent management?
1. FEC 60 followed by RT and Hormone therapy
2. FEC 100 followed by RT and Hormone therapy
3. FEC-D followed by RT and Hormone therapy
4. RT and Hormone therapy
5. Cyclosphosphamide and Docetaxol followed by Hormone therapy

Combined Benefit is 4.7%,
Net chemo benefit is: 4.7-2.4 = 2.3%

An Answer
FEC 100 followed by RT and Hormone therapy
Although benefit of chemo very small, it is above the 2% threshold and as such would discuss chemo in this setting

Q5. Which hormone therapy would you chose?
1. Tamoxifen for 5 years
2. Adjuvant Anastrozole for 5 years
3. Adjuvant Tamoxifen for 2 years followed by Exemestane for 3 years
4. Adjuvant Tamoxifen for 5 years followed by adjuvant Letrozole for 5 years

Options
• Adjuvant Tamoxifen switched to an AI (Anastrozole or Exemestane) at 2 years
• AI for 5 years

Current Endocrine Therapy Protocol for Early Breast Cancer
• Post-menopausal – PATIENTS AT FIRST PRESENTATION: – There are no clear data to guide management in this group – International guidlines support the use of either an initial
aromatase inhibitor, or the initiation of tamoxifen with a subsequent switch to an aromatase inhibitor after 2-3 years. (NCCN, St. Gallen)
– It is suggested that the majority of patients are treated with TAMOXIFEN FOR 2-3YRS FOLLOWED BY EXEMESTANE OR ANASTRAZOLE OR FOR 2-3YRS FOR A TOTAL TREATMENT DURATION OF 5YRS.
– Patients with contraindications to TAMOXIFEN should continue to be treated with ANASTRAZOLE for 5years.
Given the current uncertainties regarding the
optimal use of aromatase inhibitors in the adjuvant setting, the choice of treatment should
be made after discussion between the responsible clinician and the woman about the risks and
benefits of each option