Embed Size (px)
Citation preview

Endocrinology Review

Review Outline
• Adrenal
• Pituitary
• Thyroid
• Calcium
• Diabetes

Adrenal
Disorders

Adrenal Insufficiency
Primary
• autoimmune
• hemorrhage
• tuberculosis (TB)
Secondary
• steroid treatment*
• pituitary disease

CRH

Cortisol ACTH
Primary Low High
Secondary Low Low or
(central) normal

Primary AI Secondary AI
ACTH high low or normal
Hyperpigmentation yes no
Aldosterone low normal
Symptoms +++ +
Na low low or normal
K high normal

Adrenal Insufficiency
Suspected
ACTH Stimulation Test:
Cortisol >20 ug/dl
Normal HPA axis
Cortisol < 20 ug/dl
Adrenal Insufficiency
Plasma ACTH
Elevated Normal or Low
Primary Adrenal
Insufficiency
Secondary Adrenal
Insufficiency

Adrenal Insufficiency Imaging
• Primary: get adrenal CT of abdomen
• Secondary: pitutiary MRI (if not on steroids)

1o AI 2o AI Stress HC 100 q 8 HC 100 q 8
Maint. HC 20/10 HC 20/10
fludrocortisone
Treatment with hydrocortisone (HC):

Cushing’s Syndrome: Etiology
• Pituitary tumor 70%
• Adrenal tumor 15%
• Ectopic tumor 15%

Cushing’s Syndrome
• Do one of the three. If positive then do a second one.
• Establish hypercortisolism: 24 hr. Urine Free Cortisol
1 mg ODST
• Biochemical localization: ACTH, 8 mg ODST
– Remember, ectopic will not supress with dex.
• Radiographic localization: MRI, CT, octreotide
+/- petrosal sinus sampling
• Treatment: surgically resect tumor

Cushing’s Syndrome Suspected
24 hour urine-free cortisol
Overnight dexamethasone (1 mg) suppression test
Abnormal
ODST: serum cortisol > 2 ug/dl
urine free cortisol > 100 mcg/24
Plasma ACTH
Normal
ODST: serum cortisol < 2 ug/dl
urine free cortisol < 100 mcg/24
ACTH < 10
Adrenal
(Adrenal CT scan)
ACTH normal or high
8 mg ODST
Suppression
Pituitary
(Sella MRI)
Non-suppression
Ectopic ACTH
(CXR, CT chest, ? octreoscan)

Cushing’s syndrome
• pituitary MRI
• inferior petrosal venous sampling

Primary Aldosteronism
• clinical: hypertension, low K, metabolic alkalosis
• screening: aldosterone/renin ratio > 20 and
absolute aldosterone >15
• confirmation: saline suppression test
• localization: CT scan, +/- adrenal vein sampling
• treatment: adenoma-surgery
hyperplasia-spironolactone
eplerenone

Multiple Endocrine Neoplasia Syndromes
MEN 1 MEN 2a MEN 2b
Pancreas MTC MTC
Pituitary Pheo Pheo
1o HPT 1o HPT mucosal neuromas,
marfanoid habitus

MEN Syndromes
• MEN1 looks like a kite, pituitary,
parathyroid and pancreas.
• MEN 2 A looks like a square. Pheo and
parathyroid.
• MEN 2 B looks like a triangle.
Oral/intestinal ganglioneuromatosis (think
of the top of the triangle as the mouth/GI
tract) and also pheo.
• Both MEN 2 are ret mutation and
medullary thyroid

Pituitary
Disorders

Pituitary Gland Hormones
• FSH
• LH
• TSH
• ACTH
• Prolactin
• Growth Hormone

Pituitary Gland Tumors
• Prolactinoma 50%
• Non-secreting 30%
• GH-secreting 10%
• ACTH-secreting 10%

Provided by: Eric Tay, MD
Microadenoma vs. Macroadenoma: 1.0 cm


Hyperprolactinemia: the “4 P’s”
• Pregnancy
• Primary Hypothyroidism
– TRH is a prolactin release hormone!
• Prescription Drugs
• Prolactinoma*

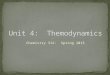
7’ 2”

Prolactinomas
Women
• microadenomas
• amenorrhea
• galactorrhea
Men
• macroadenomas
• headache
• visual complaints
• hypogonadal


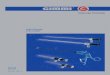
after one year of
bromocriptine therapy before treatment
Macroprolactinoma

Hyperprolactinemia
• diagnosis: 4 P’s
• macroprolactinoma if PRL > 200
• MRI to confirm
• treatment: MEDICAL!
bromocriptine or cabergoline

Acromegaly
• diagnosis: GH, IGF-1, + Oral Glucose
Tolerance test
– Ideally GH should suppress with ORGTT
(but if it doesn’t)
• localization: MRI

Radiation
Surgery Somatostatin
receptor ligands:
octreotide,
lantreotide
GH receptor
antagonists:
pegvisomant


Diabetes Insipidus
• polyuria, polydipsia
• high serum Na
• high serum osmolality
• low urine osmolality < 200
• therapy: DDAVP
– The urine should concentrate with DDAVP which is a
ADH analog

DI
• Two types
• Central DI
– There is a central deficit in the production of
ADH. The way to treat this is to give them
DDAVP.
• Nephrogenic DI
– The kidneys do not respond to ADH
– The kidney does not respond to the
desmopresin test

Thyroid
Disorders

Hypothyroidism: Symptoms
Fatigue
Weight gain
Depression
Constipation
Menstrual irreg.
Cold intolerance
Dry skin
Hair loss

Free T4 TSH
*Primary Low High
Secondary Low Low/normal

Hypothyroidism
• Hashimoto’s is most common cause
– antiTPO
• Dx.: TSH and FT4 and exam (no nodules)
• Imaging rarely needed
• Treatment: levothyroxine
– Follow the TSH. If they still have symptoms with nl
TSH then refer them out and give them to social work
(cause were super awesome surgeons)

Hyperthyroidism: Causes
Common:
a. Graves’ disease
Anti-TSH Ab
b. Toxic MNG
c. Solitary toxic nodule
d. Subacute thyroiditis
e. Iodine-induced
f. Iatrogenic

Hyperthyroidism: Symptoms & Signs
• Nervousness/Anxiety
• Palpitations
• Weight loss
• Increase appetite
• Diaphoresis
• Muscle Weakness
• Dry bulging eyes
• Diarrhea
• Heat intolerance
• Menstrual irregularity
• Tremor
• Tachycardia (60%)
• Warm, moist skin
• Heart failure (HO)
• Proximal myopathy
• Lid retraction/lag (Graves)
• Proptosis* (Graves)
• Thyroid bruit*
• Goiter

Differential Dx: 24 hour RAIU
High RAIU (>30%)*
• Graves’ disease
• toxic MNG
• solitary toxic nodule
Low RAIU (<5%)**
• subacute thyroiditis
– hyper->hypo->eu
– Generally viral etiology
• iodine-induced
• factitious/iatrogenic
**self-limited conditions
*require “definitive therapy”

Definitive Treatments:
Hyperthyroidism

Hyperthyroidism: Treatment
High uptake hyperthyroid
• I-131
• anti-thyroid drugs
– Agranulocytosis
– Hepatic Damage c PTU
• Black box warning!!!!!!!
• thyroidectomy
Low uptake hyperthyroid
• treat symptoms
-B blockers
(also blocks some
peripheral conversion
like PTU)
-NSAID’s for SAT

TSH & FT4
Normal Hyperthyroid Hypothyroid
“Idiopathic”
radioactive
iodine
replace LT4
and follow
Goiter
1. follow
2. suppress
3. surgery
Graves’ or toxic MNG Hashimotos’s thyroiditis

Thyroid Nodules
• 5% of adult population has palpable nodule
• < 10% of palpable nodules are malignant
• > 95% are euthyroid
• After obtaining serum TSH, the best initial test:
FNA thyroid biopsy
• Incidentalomas: U/S guided bx. if > 10 mm

TSH
Normal
Low High FNA
biopsy
24 hr. RAIU Replace LT4
and follow
Thyroid Nodule
Benign Malignant
Surgery Follow

Thyroid Cancers:
• Papillary thyroglobulin
– Major complication of neck radiation
• Follicular thyroglobulin
• Anaplastic no marker
– Comes on in old people the most. Refractory to Tx
• Medullary calcitonin
– C cell derived. ALWAYS THINK MEN2!!! Concurrent PHEO

Thyroid Cancers: Treatment
• Papillary - surgery, I-131, LT4
• Follicular - same as PTC
• Anaplastic - palliative
• Medullary – surgery

Thyroid Cancer Treatment
Surgery I-131 LT4
suppression
Papillary + + +
Follicular + + +
Medullary + -- --
Anaplastic -- -- --

Calcium
Disorders

Pathophisiology of
Hypercalcemia:
• 1. Increased bone resorption
• 2. Increased renal resorption of calcium
• 3. Increased gut absorption of calcium

Causes of Hypercalcemia
Common
1. Primary HPT
2. Malignancy
Uncommon
1. Lithium, HCTZ
2. Vitamin D or A toxicity
toxicity
3. Hyperthyroidism
4. Granulomatous disease
5. Immobilization
6. FHH
7. Milk-alkali

Diagnosis: PTH Level
High PTH
• Primary HPT
• FHH*
* Check 24 hr. urine calcium
Low PTH
• Malignancy
– He says this is “low
yield” but this also
comes from the guy who
said peritibial myxedema
is low yield
• Everything else

Primary HPT Malignancy
Serum calcium < 12 > 12
Symptoms +/- +++
Duration > 6 mos. < 6 mos.
PTH high low
PTHrP low high

Hypocalcemia: Causes
• Vitamin D deficiency
– Low calcium and phos
• Hypoparathyroidism
-post-surgical (most common)
-autoimmune (very rare)
• Low magnesium (primes the Ca sensitive sensor to
sense Ca)
• Pseudohypoparathyroidism
– PTH levels are actually elevated but dysfunctional G proteins
make it so PTH can’t work on the receptor. The pt has other
problems besides just hypocalcemia

Vitamin D deficiency: Common
• low serum calcium
• low serum phosphate
• high PTH – secondary hyperparathyroidism
– The body tries to restore Vit D balance. Recall that PTH
increases 1ahydrolyase activity in the kidney. 1,25OH is the
main active form.
– Low Ca with Low PTH is Primary hyperpara
• low 25-OH vitamin D
• low 24 hour urine calcium

Osteoporosis

Primary Osteoporosis
Women
• postmenopausal
• senile
Men
• senile

Secondary Osteoporosis
• vitamin D deficiency
• primary HPT
• hypercalciuria
• glucocorticoid excess
• hyperthyroidism
• multiple myeloma
• hypogonadism in both women and men

Secondary Osteoporosis
• Women: up to 40% have 2o cause
• Men: 60% have 2o
cause
1. testicular failure
2. glucocorticoid excess
3. ETOH

Osteoporosis Treatment: Non-pharmacologic
• calcium and vitamin D supplements
• exercise
• fall precautions

Osteoporosis Treatment: Pharmacologic
Antiresorptive
decrease formation and resorption
• Bisphosphonates
• SERMS: raloxifene
• Calcitonin
• Estrogen therapy
Bone Formation Stim
increase formation and resorption
• Teriparatide (PTH)
– Intermittent exposure
to PTH will activate
blasts more than
clasts.

Osteoporosis
• Diagnosis: T-score < -2.5 or fragility fracture
• R/O secondary causes
• Treatment (if no secondary cause)
-calcium and vit D, exercise, fall precautions
-bisphosphonates, raloxifene or PTH

Diabetes

Diabetes: Pathogenesis
Type 1
• absolute insulin
deficiency
Type 2
• partial insulin deficiency
• defect in insulin secretion
• insulin resistance
• increase hepatic glucose
production

Fuel Metabolism: Normal “Balance”
Anabolic
• Insulin
Catabolic (“counteregulatory”)
• catecholamines
• glucagon
• cortisol
• growth hormone

DKA:
• Insulin
• (no insulin is around so
ketones can be made…)
• catecholamines
• glucagon
• cortisol
• growth hormone

DKA Treatment
• I.V. Insulin
• Replace fluids
• Replace K
– The patient might look eukalemic on labs but they are
actually at a deficet. Insulin will drive K+ back into
cells!!! And then the patient will be hypokalemic on
labs
• Treat precipitating cause (infection or MI)
(until anion gap resolves)

Diabetes: Diagnosis
• Fasting glucose > 126 mg/dL X 2 or
• Random glucose > 200 mg/dL with classic
symptoms of hyperglycemia

Diabetes: Complications
Microvascular
Prevented by glucose control
• nephropathy
• retinopathy
• neuropathy
Macrovascular
Not prevented by glucose control
• Myocardial infarction MI)
• Stroke (CVA)
• Peripheral vascular
disease (PVD)

Diabetes: Treatment Type 1
• insulin
• diet
Type 2
• weight loss: diet/exercise
• oral agents
– Metformin
– Thiazolidinediones
– Sulfonylureas
• exenatide
• insulin

DM-2: Oral agents
Type 2
• partial insulin deficiency.…. Sulfonylurea
• insulin resistance….. Thiazolidinediones
• increase hepatic glucose production… metformin

Insulin Therapy:
• DM-1: need 24 hour insulin coverage
NPH X 2 or glargine X 1
• DM-2: 24 hr. coverage not always necessary
add bedtime NPH to oral agent

Lipid Disorders • High cholesterol
– Familial Hypercholesterolemia
• High LDL. Likely a deficiet in LRL-R (to remove LDL from the circulation). Cholesterol may be deposited around
the body (eg eye xanthelasma palpbrarum), iris arcus senilis corneae, tendons around the body such as the
Achilles or hand)
– Familial defective B-100
• High LDL. Presents like LDL-R. apoB-100 binds to LRL-R to get the LDL out of the system
– Polygenic Hypercholesterolemia
• Presence of Xanthomata can confirm the diagnosis of FH. Only moderate LDL increase (140-300) with TG in
normal range.
• High triglycerides and cholesterol
– Familial Combined Hyperlipidemia
– Dysbetalipoproteinemia
• Increase in LDL, cholesterol, and TG levels with decreased HDL levels. Presents with xanthoma triatum
palmara which is orange or yellow discoloration on the hands. Also with eruptive xanthomas on the elbows and
knees. There is a deficit in ApoE which allows for LDL/IDL/VLDL/chylomicros to be absorbedd into the liver.
• High triglycerides
– Familial hypertriglyceridemia
• Pancreatitis, hepatomegaly, spelanomegaly, xanthomas
– LDL deficiency
– Apo-CII deficiency
• ApoC2 is needed for LPL to hydrolyze TGs. Presents with xanthomas, pancreatitis, and hepatoplenomegaly.
Not at risk for atherosnclerosis
– Sporadic Hypertriglyceridemia

Lipid Disorders: Etiology
• genetic
• obesity
• diabetes
• medications: estrogen, thiazides
• smoking
• hypothyroidism
• chronic renal failure; nephrotic syndrome
• obstructive liver disease

Typical Lipid Pattern: DM-2
• High triglycerides
– No insulin to upregulate LPL
• Low HDL
• Normal or high LDL cholesterol

Lipid Disorders: Treatment
High cholesterol
• statins*
• ezetimibe
• bile acid resins
High triglycerides
• gemfibrozil, fenofibrate*
• niacin
*risk of myositis when used in combination

The “Insulin Resistance Syndrome”
aka The “Metabolic Syndrome”
• obesity
• insulin resistance: high insulin levels
• hyperglycemia/diabetes
• hypertension
• lipid abnormalities
• coronary artery disease

Hypoglycemic Disorders
72 hour fast:
• glucose
• insulin
• C-peptide
• sulfonylurea screen

Hypoglycemic Disorders
72 hour fast:
• insulinoma:
– low glucose
– high insulin
– high C-peptide
• sulfonylureas: same except + sulfonylurea screen
• surreptitious insulin injection:
– low Glucose
– high insulin
– low C-peptide