Embed Size (px)
Citation preview
DOI: 10.1111/j.1610-0387.2011.07731.x Academy 705
© The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2011/0909 JDDG | 9˙2011 (Band 9)
Section EditorProf. Dr. Jan C. Simon,
Leipzig
Keywords• coccidioidomycosis• histoplasmosis• paracoccidioidomycosis• blastomycosis• systemic mycoses• treatment
JDDG; 2011 • 9:705–715 Submitted: 24. 2. 2011 | Accepted: 18. 5. 2011
CME
Endemic systemic mycoses: coccidioidomycosis,histoplasmosis, paracoccidioidomycosis andblastomycosisAlexandro Bonifaz1, Denisse Vázquez-González1, Ana María Perusquía-Ortiz2
(1) Departamento de Micología, Servicio de Dermatología, Hospital General de México, Ciudad de México(2) Department of Dermatology, University of Münster, Germany
SummaryEndemic deep or systemic mycoses are common in specific geographical areasof the world. Coccidioidomycosis is present in semi-desert areas, histoplasmo-sis and paracoccidioidomycosis in tropical regions and blastomycosis belongsto temperate climates. The two former are widely distributed in the Americancontinent and some tropical regions of the world; the third is limited to Centraland South America, and the last to North America and Central and East Africa.These mycoses all have a similar pathogenesis, as the inoculum enters the hostthrough the respiratory tract. Cutaneous manifestations are secondary to lym-phatic and hematogenous dissemination. These deep mycoses are exceptionalin Europe. Most cases are observed in returning travelers from endemic areas,aid workers, archaeologists, speleologist and immigrants. However, there have been some autochthonous cases of histoplasmosis due to Histoplasmacapsulatum var. capsulatum reported in European countries such as Italy andGermany. In this article, we provide up-to-date epidemiological, clinical, diag-nostic and therapeutic data on the four most important imported systemicmycoses in Europe.
Endemic systemic mycosesIntroduction The most common endemic systemic mycoses – coccidioidomycosis, histoplasmosis,paracoccidioidomycosis and blastomycosis – occur predominantly in specific climatezones. Common to all is the entry via the respiratory tract, from here there can behematogenous and lymphatic spread to the skin and other organs. All pathogens aredimorphic fungi. They differ in epidemiology, symptoms and prognosis [1, 2].
CoccidioidomycosisEtiology and pathogenesis Coccidioidomycosis is elicited by two dimorphic fungus species, Coccidioides immitis,(almost only in the San Joaquin Valley, California, USA) and Coccidioides posadasii(in other regions of the USA, along the Mexican border and in endemic areas ofMiddle and South America) [1–3]. They belong to the order Onygenales and theyflourish in desert regions with semiarid and clayey conditions with very low precipi-tation, extreme temperature variations (0 °C to 45 °C) and predominantly xerophyticflora (Cactaceas) [1]. The infection is via the respiratory tract (98 %), in someextremely rare cases through the skin. All age groups can be affected, usually malemigrant workers in the border region between Mexico and the USA [1, 2].
Common to all is the entry via the res-piratory tract, from here there can behematogenous and lymphatic spreadto the skin and other organs.
Coccidioidomycosis is elicited by twodimorphic fungus species, Coccid-ioides immitis, (almost only in the SanJoaquin Valley, California, USA) andCoccidioides posadasii (in other re-gions of the USA, along the Mexicanborder and in endemic areas of Mid-dle and South America).
Arthroconidia of both pathogens enter via the respiratory tract. In both, dependingon the immune status of the host, the infection can take an asymptomatic course (in75 % of cases) or lead to fungal pneumonia, sometimes with dissemination into theskin or lymph nodes [4, 5].
Clinical coursePrimary pulmonary coccidioidomycosis can take a insidious course; severe coursesresemble pulmonary tuberculosis. The skin can be involved by two routes. More frequent is secondary spread via blood or lymphatic vessels form a pulmonary lesion,usually in the vicinity of peripheral lymph nodes with nodular infiltration, gumma-ta, abscesses, ulcers and retracting scars [1, 6] (Figure 1). Primary cutaneous involve-ment is quite rare and manifests at the site of inoculation (by injury). Initially thefirst lesion is a “change” with lymphadenitis and lymphangitis; later, in chronic casesnodular-gummatous, verrucous and even ulcerative lesions can be developed [6].Very rare is meningeal involvement with neurological manifestations such asheadaches, memory disturbances or loss of orientation. These clinical features aremore common in latin-americans, blacks as well as immunosuppressed patients, e. g.in HIV/AIDS (acquired immunodeficiency syndrome) [1].Differential diagnoses for coccidioidomycosis, histoplasmosis, paracoccidioidomyco-sis and blastomycosis are listed in Table 1.
706 Academy
JDDG | 9˙2011 (Band 9) © The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2011/0909
In both pathogens, depending on theimmune status of the host, the infec-tion can take an asymptomatic courseor lead to fungal pneumonia, some-times with dissemination into the skinor lymph nodes.
The skin can be involved by tworoutes: More frequent is secondaryspread via blood or lymphatic vesselsfrom a pulmonary lesion, usually inthe vicinity of peripheral lymphnodes; primary cutaneous involve-ment is quite rare and manifests atthe site of inoculation (by injury).
Very rare is meningeal involvementwith neurological manifestations.
Table 1: Principal differential diagnoses of systemic mycoses.
Coccidioidomycosis• Lymph node tuberculosis
and tuberculosis cutis ver-rucosa
• Sporotrichosis• Blastomycosis• Leishmaniasis• Atypical mycobacterioses• Paracoccidioidomycosis
Histoplasmosis• Tuberculosis cutis
colliquativa and verrucosa• Leishmaniasis• Cryptococcosis• Molluscum contagiosum• Atypical mycobacterioses• Paracoccidioidomycosis
Paracoccidioidomycosis • Tuberculosis cutis
colliquativa and verrucosa• Histoplasmosis• Coccidioidomycosis• Lymphoma• Leishmaniasis• Blastomycosis• Lupus vulgaris• Syphilis
Blastomycosis• Tuberculosis cutis
colliquativa and verrucosa• Leishmaniasis• Sporotrichosis• Coccidioidomycosis• Paracoccidioidomycosis • Lymphoma• Atypical mycobacterioses• Squamous cell carcinoma• Syphilis
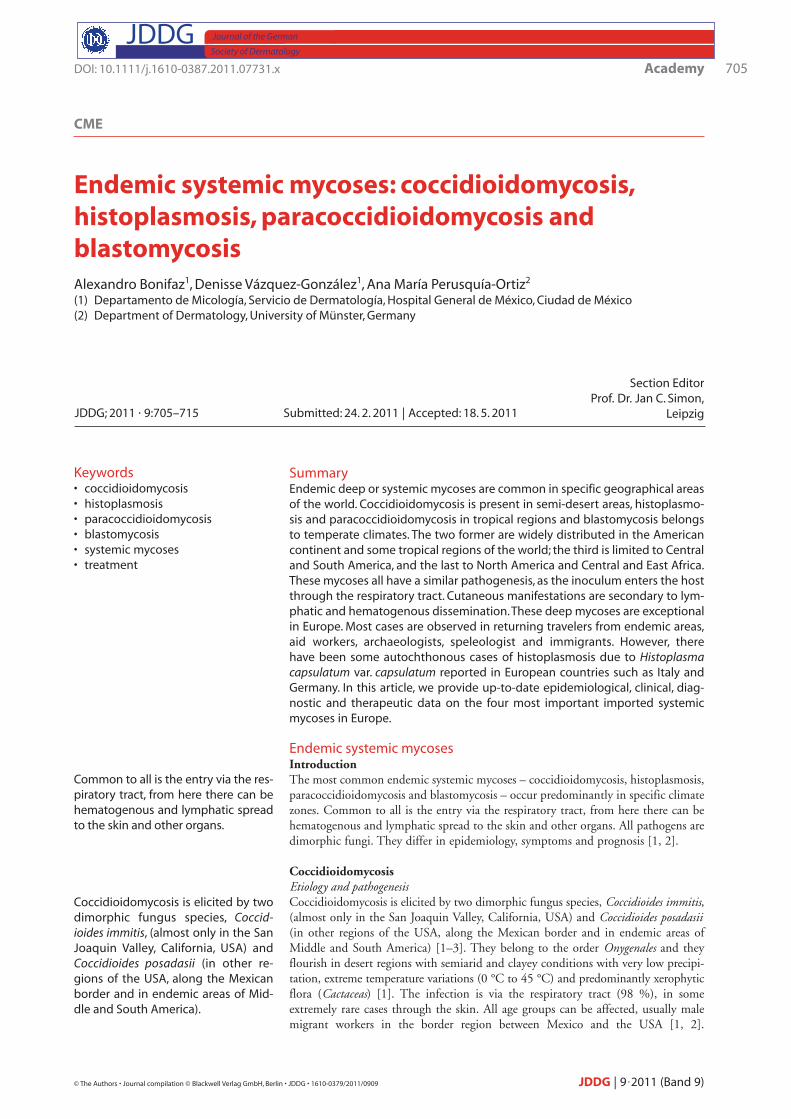
Figure 1: (a) Coccidioidomycosis with lymph node involvement; (b) nodules and ulcers in secondarycutaneous coccidioidomycosis; (c) micromorphology: Coccidioides immitis hyphae with arthroconidia(Cotton blue stain, 60�); (d) direct microscopy: spherules with endospores (KOH, 60�).

Diagnostic approachLaboratory diagnostics: In direct microscopy using potassium hydroxide (KOH,10–20 %) of pus from abscesses, sputum or bronchial lavage material the typical par-asitic form of the pathogen can be recognized: spherules 20 to 70 µm in diameterwith a double membrane containing masses of endospores (2–5 µm). Culturing thepathogens is dangerous and reserved for highly specialized S3 laboratories with highsecurity standards. The cultures of both fungi are similar; they form white, downyand dry colonies. Micromorphology reveals hyphae and arthroconidia separated by afine membrane called article [1–5] (Figure 1). Histology: tuberculoid granulomas with spherules of different sizes that can easily bestained with PAS (periodic acid-Schiff ) and Grocott [6]. Immunological methods: Diagnostically useful is the intradermal reaction to coccid-ioidin (coccidioidin skin test) as well as the analysis of specific antibodies by comple-ment fixation. Both tests allow for conclusions on the prognosis of the disease [1].Radioimmunoassay (RIA), enzyme-linked immunosorbent assay (ELISA), immuno-fluorescence assay (IFA) and particularly in Germany the immunoblot (Western-blot) are valuable diagnostic techniques today. The reference laboratory in Germany,where culture and differentiation of suspected isolates as well as serological methodscan be performed is the Consulting Laboratory for Pathogens of non-EuropeanSystemic Mycoses, Robert Koch Institute, FG 16 – Mycology, Nordufer 20, 13353Berlin, Germany.Molecular biologic methods: The fungus can be detected by the polymerase chain reac-tion (PCR) and in-situ hybridization (ISH) [1].In endemic regions of the two Mexican states Sonora and California a positive reac-tion to coccidioidin (coccidioidin skin test) was found in 80 % of the population. Inthe endemic regions of the middle valley of California, in the USA a serological con-version was found in almost 100 % of the population [1, 7].
TherapyIn severe and disseminated cases treatment with amphotericin B desoxycholate isindicated in doses between 0.25 and 0.75 mg/kg up to a cumulative total dose of 30to 50 mg. At present amphotericin B can be administered as lipid, liposomal and col-loidal-disperse preparations in doses from 3 to 6 mg/kg/d. Additionally, a triazolesuch as itraconazole (300–400 mg/d) or fluconazole (200–400 mg/d) can be admin-istered orally; the former brings the best results, the latter is indicated particularly formeningeal dissemination, as fluconazole penetrates the blood-brain barrier [1–3].The use of itraconazole as monotherapy is largely reserved for limited or cutaneousinitial involvement; it is nonetheless valuable for maintenance therapy [1, 2]. Good results have also been reported for newer triazoles such as voriconazole andposaconazole at a dose of 800 mg/d each [8]. Criteria for healing are: clinical, myco-logical and immunological recovery, being the latter the most important parameterfor prognosis, when titration of complement-fixing antibodies (with use of therespective antigen) is lower than 1 : 8. Therefore, treatment duration differs frompatient to patient [1, 6].
HistoplasmosisEtiology and pathogenesisAmerican histoplasmosis or Darling’s disease is a systemic mycosis caused by thedimorphic fungus Histoplasma capsulatum var. capsulatum, which particularly affectsthe reticulohistiocytic system [1]. The pathogen belongs to the order Onygenales andpossesses a teleomorphic phase: Ajellomyces capsulatus [1, 2]. The lung is the usual siteof initial infection. Later the fungus can spread to various organs, even the skin.Worldwide, histoplasmosis is the most common fungal lung infection, occurringalmost everywhere; reports exist from over 60 countries. The pathogen flourishes par-ticularly in tropical climate zones such as Middle or South America, in the easternUSA, in the Ohio and Mississippi River valleys, but also in southern Mexico [9]. Thefungus is found in soil, in decaying plant materials, but especially in droppings ofbats and some birds such as chicken, turkeys or geese. Particularly favorable growthconditions are found at temperatures between 20 °C and 30 °C at relatively highhumidity and chalky soil [9, 10]. The incubation period varies between 1–3 days to
Academy 707
© The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2011/0909 JDDG | 9˙2011 (Band 9)
In direct microscopy with KOH 10–20 % the typical parasitic form ofthe pathogen can be recognized:spherules with a double membranecontaining masses of endospores.
Histology: tuberculoid granulomaswith spherules of different sizes thatcan easily be stained with periodicacid-Schiff (PAS) and Grocott.
The intradermal reaction to coccid-ioidin (coccidioidin skin test) as wellas the analysis of specific antibodiesby complement fixation allow for conclusions on the prognosis of thedisease.
In severe and disseminated cases treat-ment with amphotericin B is indicated;additionally, a triazole such as itracona-zole or fluconazole can be adminis-tered orally.
Criteria for healing are: clinical, myco-logical and immunological freedomfrom disease. The latter is most impor-tant prognostically; therefore treat-ment duration differs from patient topatient.
Worldwide, histoplasmosis is the mostcommon fungal lung infection, occur-ring almost everywhere.
American histoplasmosis is caused bythe dimorphic fungus Histoplasmacapsulatum var. capsulatum, whichflourishes particularly in Middle andSouth America, in the eastern USA, inthe Ohio and Mississippi River valleys,but also in southern Mexico.
708 Academy
JDDG | 9˙2011 (Band 9) © The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2011/0909
1–5 months. All age groups are affected, especially people in the 3rd and 4th decadeof life, men somewhat more frequently than women. Histoplasmosis occurs fre-quently in miners, cave explorers, guano workers, farmers, beekeepers and archeolo-gists [1, 9]. The pathogens enter the body in the form of spores or conidia via therespiratory tract. Occasionally, they also enter through the skin. Inhaled spores canreach the alveoli via the bronchioles. There they can produce a primary complex sim-ilar to tuberculosis with lymphangitis and hilar lymphadenopathy [1, 10, 11]. Mostcases are asymptomatic. Skin involvement is more frequent in HIV-positive patients.Three factors are important for the development of the disease: amount and viru-lence of the pathogen as well as the immunological status of the host [9–11].Some cases of autochthonous infections by Histoplasma capsulatum var. capsulatumhave, nevertheless, been detected in European countries such as Italy (in the valley ofthe Po River) and Germany, where the fungus has been found in soil [12].
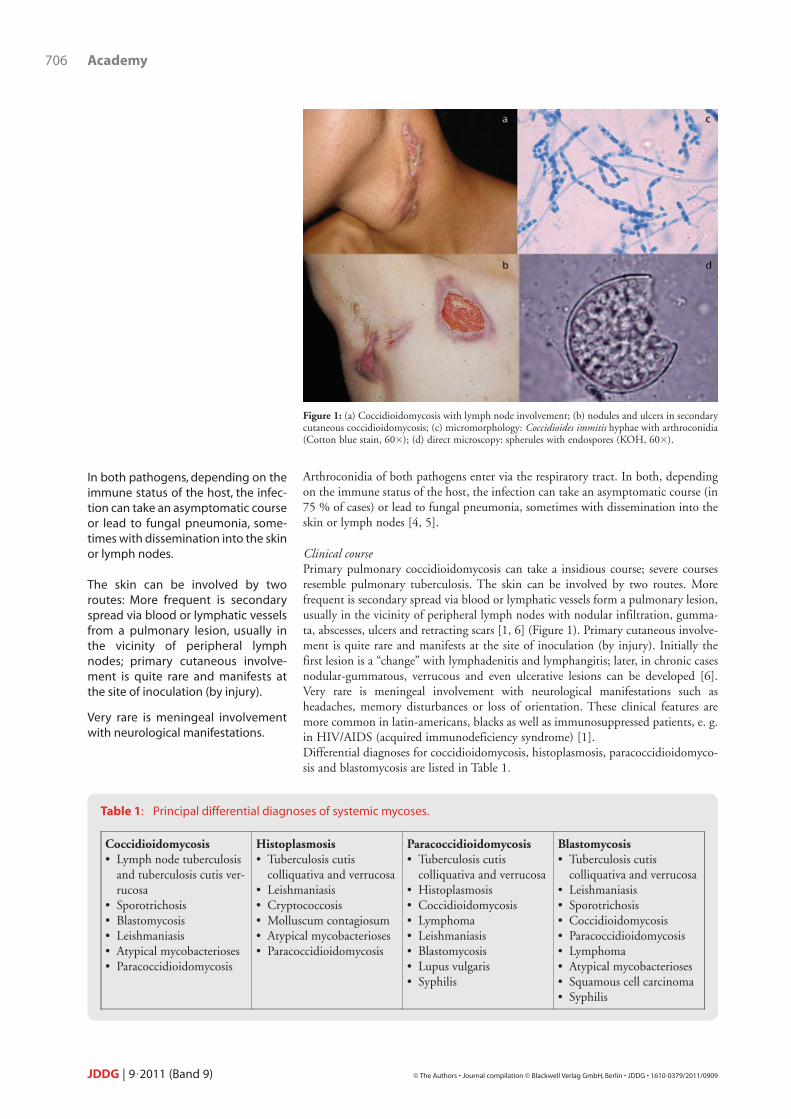
Clinical coursePulmonary histoplasmosis is the most important form. It can take a mild course, butcan lead to an acute or chronic severe pneumonia similar to tuberculosis.Dissemination is usually into visceral organs such as pancreas, liver, spleen and intes-tines. Occasionally, the meninges are affected [9]. The primary cutaneous form is veryrare. It usually results from injury during risky activities such as guano production,cleaning of chicken coops and similar activities. Cutaneous histoplasmosis manifestsinitially as a “chancre” with lymphangitis and lymphadenitis, later with nodular gum-matous lesions, cellulitis, ulcers, panniculitis or verrucous lesions [9]. In progressivechronic cases dissemination can extend to the nasal and oral mucous membranes, thelarynx and pharynx as well as the genitals and lead to sharply delineated erythematousulcerative lesions there. In HIV/AIDS patients lesions usually develop on the head andneck; occasionally the entire skin is affected including palms, soles, oral, anal and genital mucous membranes [9–11] (Figure 2). The lesions are then often molluscumcontagiosum-like papules as well as confluent nodular and gummatous lesions withvegetating plaques. In addition, abscesses, ulcers, purpuric lesions and panniculitismay be present [9, 11]. Cutaneous cryptococcosis is an important differential diagno-sis because the lesions are clinically quite similar, especially in HIV/AIDS patients [1].
Diagnostic approachLaboratory diagnostics: The pathogen can be detected in PAS, Giemsa, Grocott orPapanicolaou stains of wound exudate, sputum or bronchial lavage fluid.
Pathogen detection (intracellularyeast cells in macrophages and neu-trophilic granulocytes with a refrac-tive edge) succeeds in PAS, Giemsa,Grocott or Papanicolaou stains.
Histoplasmosis occurs frequently inminers, cave explorers, guano work-ers, farmers, beekeepers and archeol-ogists.
Three factors are important for thedevelopment of the disease: amountand virulence of the pathogen as wellas the immunological status.
Pulmonary histoplasmosis is the most important form. Disseminationis usually into visceral organs such aspancreas, liver, spleen and intestines;occasionally the meninges are af-fected.
In HIV/AIDS patients lesions usuallydevelop on the head and neck, often,however, the entire skin is affected bymolluscum contagiosum-like papulesincluding palms, soles, oral, anal andgenital mucous membranes.
Figure 2: (a) Disseminated histoplasmosis in an HIV/AIDS-infected patient (courtesy of GriseldaMontes de Oca, M.D., Mexico); (b) Dermatopathology: numerous intracellular yeast cells (H&E,100�); (c) Histoplasma capsulatum, echinulate conidia (Cotton blue stain, 60�).

Intracellular yeast cells 1 to 3 µm in diameter can be observed in macrophages andneutrophilic granulocytes with a refractive edge simulating a capsule. Culture is per-formed in standard Sabouraud agar with or without antibiotics at 28 °C in an aver-age time of 1 to 2 weeks. Two types of colonies are differentiated: A (albina) and B(brown); both are downy, sharply delineated and dry [1]. Their micromorphology issomewhat different: B strains demonstrate typical needle-like or echinulate macro-conidia with a double membrane in a larger number (resembling washers for clocks)and microconidia attached to hyphae. When the fungus H. capsulatum is incubatedin nutrient-rich culture media and at 37 °C, the yeast phase develops (dimorphism)[1, 10]. Histology: tuberculoid granuloma with many polymorphonuclear leukocytes and histiocytes with numerous intracellular yeast cells. To make the structures visible PASor Grocott stains are performed [10] (Figure 2). Immunological methods: Histoplasmin skin test and analysis of specific antibodies bycomplement fixation. Both tests determine the prognosis of the disease. RIA, IFA, gelimmunodiffusion test and immunoblot are further helpful techniques today [10, 11].Molecular biological methods: The fungus can be detected by “Random Amplificationof Polymorphic DNA“-PCR (RAPD-PCR) and nested PCR [10, 11].
TherapyEssentially three approaches are common practice depending on the clinical variant ofhistoplasmosis and the general condition of the patient. In chronic progressive cases useof trimethoprim-sulfamethoxazole in a dose of 80/400 mg/d is indicated; mean treat-ment duration is one to two years [1]. The azoles offer a second therapeutic option.Among the most frequently recommended are itraconazole and fluconazole. Both areadministered in a dose of 200–400 mg/d with gradual tapering. Fluconazole can beadministered intravenously in a dose of 6 mg/kg/d. In the event of meningeal involve-ment it has the advantage of penetrating the blood-brain barrier. Good results are alsoachieved with voriconazole and posaconazole at doses of 800 mg/d [1, 9, 13]. In severeand disseminated cases or in patients with HIV/AIDS amphotericin B desoxycholatein doses between 0.25 and 1 mg/kg/d and for the lipid, liposomal and colloidal-dis-perse preparations between 3 and 5 mg/kg/d must be administered [13]. In asympto-matic courses with a positive histoplasmin skin test and suspicious radiological findingspreventive therapy with itraconazole in a dose of 200 mg/d over two to three monthsis recommended, as immunosuppression can reactivate the disease [1].As a preventive measure the use of protective masks is recommended for anthropol-ogists, cave explorers, guano workers and miners [1].A further type of histoplasmosis exists: African histoplasmosis, a subcutaneous myco-sis or systemic mycosis caused by the dimorphic fungus Histoplasma capsulatum var.duboisii, which primarily affects skin, lymph nodes and bone. The disease is limitedto equatorial Africa. It is treated the way as Histoplasma capsulatum [1].
Paracoccidioidomycosis Etiology and pathogenesis This systemic mycosis with an acute course is caused by a dimorphic fungus,Paracoccidioides brasiliensis, which is classified in the order Onygenales. It is character-ized by almost always asymptomatic primary lesions of the lung. From there it canspread to the oropharyngeal mucosa, lymph nodes, skin and various organs [1, 2,14]. Paracoccidioidomycosis is limited to the American continent, especially toSouth America (Brazil, Columbia, Venezuela, Paraguay) as well as some regions ofCentral America and Mexico [14]. The fungus has been isolated from soil and decay-ing plant tissue, especially in acid soil (area of cultivation of coffee and sugar cane),in tropical and very humid regions. Men are affected preferentially, perhaps on hor-monal grounds, most frequently in the 3rd and 4th decade of life, while children arerarely affected. It is a typical occupational infection of farmers and outdoor workers[14, 15]. The pathogen generally enters via the respiratory tract or injuries of the skinand mucous membranes. Inhalation of conidia leads to a primary infection of thelung, which almost always remains asymptomatic. The clinical course depends on theimmune status of the host; dissemination from the lung lesion into skin, mucousmembranes and other organs is possible [15].
Academy 709
© The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2011/0909 JDDG | 9˙2011 (Band 9)
Histology: tuberculoid granuloma withmany polymorphonuclear leukocytesand histiocytes with numerous intra-cellular yeast cells.
In chronic progressive cases use oftrimethoprim-sulfamethoxazole is in-dicated; mean treatment duration isone to two years.
In severe and disseminated cases or inpatients with HIV/AIDS amphotericinB must be administered.
A further type of histoplasmosis:African histoplasmosis caused by thedimorphic fungus Histoplasma capsu-latum var. duboisii, which primarily affects skin, lymph nodes and bone.
Paracoccidioidomycosis is caused bythe dimorphic fungus, Paracoccidioidesbrasiliensis, which is limited to theAmerican continent, especially to SouthAmerica (Brazil, Columbia, Venezuela,Paraguay) as well as some regions ofCentral America and Mexico.
It is a typical occupational infection offarmers and outdoor workers; thepathogen enters via the respiratorytract and injuries of the skin and mu-cous membranes.

Clinical courseSymptomatic cases develop an acute or chronic pneumonia with features of the respiratory tract resembling tuberculosis [1]. By mucous membrane manifestation,is primarily the oropharynx involved (80 %), followed for the nasal mucosa in sec-ond place. In chronic cases the larynx and trachea may also be involved. Oralinvolvement by paracoccidioidomycosis, also termed “moriform stomatitis” or“Aguiar-Pupo stomatitis”, initially takes an insidious course and manifests as smallsuperficial ulcerations in the palate with irregular edges resembling reddish-violetgranulation tissue. The lesions can extend to the gums, palate and tongue [1–6,9–11, 13–15] (Figure 3). Symptoms include odontalgia, facial pain and tooth lossresulting in a tapir-like appearance of the mouth [1]. The lesions are found mainlybetween the lips and nose: nodular-gummatous and verrucous or vegetating lesionsand ulcers. Symptomatology is variable with some patients complaining of pruritusand pain, while others are asymptomatic. Purely cutaneous lesions have no site ofpredilection and consist of erythematous violet nodes that tend to melt down andulcerate (gummata) [1, 14]. The disease affects particularly the supraclavicular, cer-vical, axillary and inguinal lymph nodes. In chronic cases or in immunosuppressedpatients dissemination into the digestive tract, liver, spleen, pancreas and adrenalglands is possible [15, 16].
Diagnostic approachLaboratory diagnostics: Direct microscopy with 10 % KOH or Lugol solution ofwound secretion, sputum or bronchial lavage fluid reveals yeast cells with multipolarbudding with a mother cell of 10–40 µm diameter, refractive double membrane, surrounded by numerous 2–6 µm large buds [1, 2]. Wright, Giemsa or Pas stain canbe used to increase contrast.. Culture is performed on standard Sabouraud agar withor without antibiotics at 28 °C; colonies develop in between 3–4 weeks and up to2 months. Histology: Usually tuberculoid granulomas with yeast cells with multipolar budding(“steering-wheel” form) that can be seen well in the PAS and particularly in theGrocott stain [1, 14] (Figure 3).Immunological methods: Paracoccidioidin skin test as well as analysis of specific anti-bodies measured with various techniques such as gel immunodiffusion test, comple-ment fixation, counterimmunoelectrophoresis [1].Molecular biological methods: At present PCR methods are also employed [1].
710 Academy
JDDG | 9˙2011 (Band 9) © The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2011/0909
By mucous membrane manifestation,is primarily the oropharynx (80 %) in-volved, nasal mucosa in second place.Symptoms include odontalgia, facialpain and tooth loss resulting in a tapir-like appearance of the mouth.
Direct microscopy using 10 % KOH orLugol’s solution reveals yeast cellswith multipolar budding.
Histology: Usually tuberculoid granu-lomas with yeast cells with multipolarbudding (“steering-wheel” form) thatcan be seen well in the PAS and partic-ularly in the Grocott stain.
Figure 3: (a) Facial paracoccidioidomycosis; (b) ulcers of the nasal and oral mucous membranes insecondary cutaneous paracoccidioidomycosis; (c) direct microscopy: Paracoccidioides brasiliensis, mul-tiple budding cells (KOH, 80�); (d) dermatopathology: multiple yeast cells (Grocott, 60�) (courtesyof Mary Ann Robledo, M.D., Colombia).
TherapyAs in histoplasmosis three different principles can be employed. Slowly metabolizedsulfonamides such as trimethoprim-sulfamethoxazole in doses of 160/800 mg twicedaily can be given until clinical and mycological healing occurs. A further extensionof treatment over one or two years is recommended. Azole derivatives are the besttherapeutic option. Particularly effective are ketoconazole (less desirable due to theside effects) and itraconazole (most often recommend) in doses from 200 to300 mg/d over 2 to 3 months with subsequent reduction to 100 mg/d over a timeperiod of at least 6–8 months [1, 16]. Further azoles that have shown good resultsare fluconazole (200–400 mg/d) and, since recently, voriconazole in doses of800 mg/d. Lastly, amphotericin B is the indicated treatment in severe and dissemi-nated cases, with the desoxycholate variant in doses of 0.25–0.75 mg/kg/d and insome cases up to 1 mg/kg/d; the lipid and liposomal preparations as well as the col-loidal dispersion are administered in doses of 3–5 mg/kg/d [1, 17].
BlastomycosisEtiology and pathogenesis This subacute and chronic fungal infection is caused by the dimorphic fungusBlastomyces dermatitidis (teleomorphic form Ajellomyces dermatitidis). It affects lungs,skin and bone. The most significant endemic epicenter is North America (Canadaand particularly the Eastern USA between the Ohio and Mississippi River valleys).In second place comes Middle and East Africa. Infection occurs via the respiratorytact, exceptionally through the skin, and affects primarily adult men, especially agri-cultural workers and farmers [1, 2].
Clinical courseThe most important form is primary pulmonary blastomycosis. Most cases areasymptomatic, the rest displays mild to severe respiratory findings similar to tuber-culosis or other systemic mycoses. Two types of cutaneous forms are differentiated.The more common is the secondary form resulting from dissemination from a lung lesion which manifests as nodules, gummata, abscesses and ulcers in variousregions of the body (Figure 4). Primary skin involvement is rarer and is seen at theinoculation or injury site and starts with lymphangitis and lymphadenitis. Laternodular, verrucous and ulcerous lesions develop [1, 18].
Academy 711
© The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2011/0909 JDDG | 9˙2011 (Band 9)
Three different principles can be em-ployed for therapy: sulfonamides suchas trimethoprim-sulfamethoxazole,azole derivatives such as itraconazoleand finally amphotericin B for indi-cated for severe and disseminatedcases.
Blastomycosis is caused by the dimor-phic fungus Blastomyces dermatitidis.It affects lungs, skin and bone.
The most significant endemic epicen-ter is North America (Canada and theEastern USA between the Ohio andMississippi River valleys); in secondplace comes Middle and East Africa.
The most important form is primarypulmonary blastomycosis.
Two types of cutaneous forms are dif-ferentiated: More commonly is thesecondary form resulting from dis-semination from a lung lesion; primaryskin involvement is rarer.
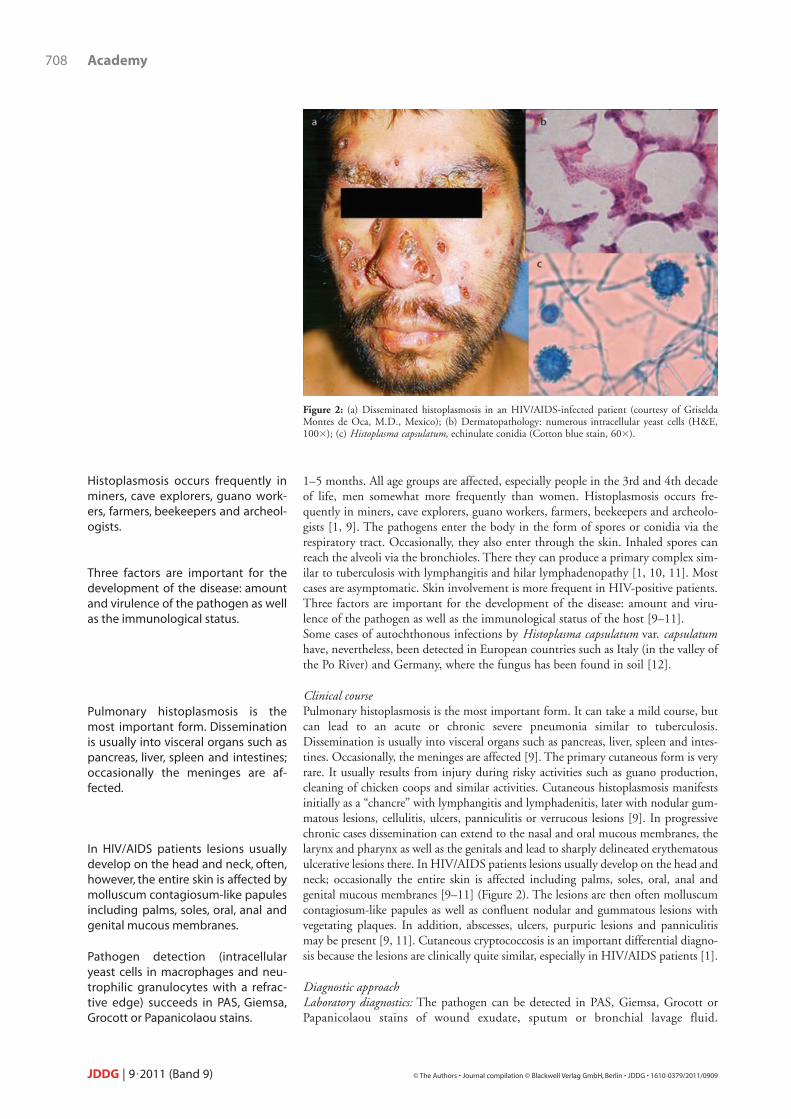
Figure 4: (a) Blastomycosis with lymph node involvement; (b) direct microscopy: single buddingcells (KOH, 80�); (c) macromorphology: Blastomyces dermatitidis with the typical Coremium (groupof hyphae) (Sabouraud agar); (d) micromorphology: filaments and piriform conidia (Cotton bluestain, 40�).

Diagnostic approach Laboratory diagnostics: In direct microscopy of wound secretion, sputum or bronchiallavage fluid with 10–20 % KOH 8–10 µm large yeast cells with unipolar budding aswell as thick and highly refractive cell walls can be seen. Culture is performed onstandard Sabouraud and Mycosel agar. The fungi form white, downy, dry colonieswith Coremium (groups of hyphae). Microscopically, small piriform (pear-shaped)conidia can be observed [1].Histology: Tuberculoid granulomas contain unipolar budding yeasts. With the helpof PAS or Grocott stains the pathogens are better contrasted from tissue [1]. Immunological methods: Blastomycin skin test as well as analysis of special antibodiesby complement fixation [1].Molecular biological methods: PCR identification [1].
TherapyTreatment is similar to that of coccidioidomycosis. In severe cases amphotericin B, inmild cases or those exclusively affecting the skin as well as in maintenance therapiesazole derivatives such as itraconazole are recommended.
ConclusionsThe primary lesions of coccidioidomycosis, histoplasmosis, paracoccidioidomycosisand blastomycosis in the lungs are usually hardly recognizable clinically in immuno-competent patients. They are therefore difficult to diagnose and treat early. Normallycutaneous lesions are a consequence of dissemination from a lung lesion. Mostpathogens respond to itraconazole and amphotericin B. Protective measures such asmasks for work in possibly contaminated environments might reduce the danger ofinfection for anthropologists, cave explorers, guano workers and miners. The featuresof the major deep fungal infections are summarized in Table 2.
712 Academy
JDDG | 9˙2011 (Band 9) © The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2011/0909
Table 2: Principal features of systemic mycoses.
Coccidioidomycosis Histoplasmosis Paracoccidioidomycosis Blastomycosis
Most common pathogens
Coccidioides immitisCoccidioides posadasii
Histoplasmacapsulatum
Paracoccidioides brasiliensis
Blastomyces dermatitidis
Pathogen types Dimorphic fungi Dimorphic fungi Dimorphic fungi Dimorphic fungi
Clinical features
Primary: gummatous,nodular lesions andverruciform plaquesSecondary: Nodules,ulcers, abscesses andfistulas
Molluscum-like papules, nodules,ulcers, cellulitis, purpuric lesions andpanniculitis
„Moriform stomatitis“,gummatous, nodular lesions, ulcers and vegetating plaques
Gummatous, nodularlesions andverruciform plaques,ulcers and abscesses
Affected body sitesPrimary: Inoculationsite Secondary: Lymphnodes
Face, trunk, nasal andoral mucosa
Face, mucous membranes(oral, nasal and ocular),trunk and limbs
Face (nose), lymphnodes, trunk andlimbs
Parasitic form Spherules Intracellular yeast cellsMultipolar budding yeast cells
Unipolar buddingyeast cells
DermatopathologyTuberculoidgranuloma with spherules
Tuberculoid granulomawith intracellular yeastcells (histiocytes)
Tuberculoid granulomawith multipolar buddingyeast cells
Tuberculoid granulomawith unipolar buddingyeast cells
Treatment• Amphotericin B• Itraconazole
• Amphotericin B• Itraconazole
• Amphotericin B• Itraconazole• Trimethoprim-
sulfamethoxazole
• Amphotericin B• Itraconazole
Response to treatment
Satisfactory Satisfactory Good Satisfactory
In direct microscopy with 10–20 %KOH yeast cells with unipolar buddingas well as thick and highly refractivecell walls can be seen.
Histology: Tuberculoid granulomascontain unipolar budding yeasts. Withthe help of PAS or Grocott stains thepathogens are better contrasted fromtissue.
The treatment is similar to that of coc-cidioidomycosis.
The primary lesions of systemic my-coses in the lungs are usually hardlyrecognizable clinically in immuno-competent patients.
Most pathogens respond to itracona-zole and amphotericin B.
AcknowledgmentsThe authors thank Thomas Bicsan for assistance in translation and Prof. Dr. MaxHundeiker for linguistic review of the text.
Conflicts of interestNone.
Alexandro Bonifaz
Correspondence toAna María Perusquía Ortiz, M.D.Central Study Coordination for Innovative Dermatology (ZiD)Department of DermatologyUniversity of MünsterVon-Esmarch-Straße 58D-48149 Münster, GermanyTel.: +49-251-83-56558Fax: +49-251-83-57296E-mail: [email protected]
References 1 Bonifaz A. Micología médica básica. 3ª edición, McGraw-Hill, México D.F., 2009.2 Lupi O, Tyring SK, McGinnis MR. Tropical dermatology: fungal tropical diseases.
J Am Acad Dermatol 2005; 53: 931–51.3 DiCaudo DJ. Coccidioidomycosis: a review and update. J Am Acad Dermatol 2006;
55: 929–42.4 Parish JM, Blair JE. Coccidioidomycosis. Mayo Clin Proc 2008; 83: 343–8.5 Laniado-Laborín N. Coccidiodomycosis and other endemic mycoses in Mexico. Rev
Iberoam Micol 2007; 24: 249–58.6 Carpenter JB, Feldman JS, Leyva WH, DiCaudo DJ. Clinical and pathologic characte-
ristics of disseminated cutaneous coccidiodomycosis. J Am Acad Dermatol 2010; 62:831–7.
7 Borchers AT and Gershwin ME. The immune response in coccidioidomycosis. Au-toimmunity Reviews 2010; 10: 94–102.
8 Wollina U, Hansel G, Vennewald I, Schönlebe J, Tintelnot K, Seibold M, Kittner T.Successful treatment of relapsing disseminated coccidioidomycosis with cutaneous in-volvement with posaconazole. J Dtsch Dermatol Ges 2009; 7: 46–9.
9 Bonifaz A, Cansela R, Novales J, Montes de Oca G, Navarrete G, Romo J. Cutaneoushistoplasmosis associated with acquired immunodeficiency syndrome (AIDS). Int JDermatol 2000; 39: 35–9.
10 Kauffman CA. Diagnosis of histoplasmosis in immunosuppressed patients. Curr OpinInfect Dis 2008; 21: 421–5.
11 Rosenberg JD, Scheinfield NS. Cutaneous histoplasmosis in patients with acquired im-munodeficiency syndrome. Cutis 2003; 72: 439–45.
12 Ashbee HR, Evans EG, Viviana MA, Dupont B, Chryssanthou E, Surmont I, Tomsi-kova A, Vachkov P, Enero B, Zala J, Tintelnot K. Histoplasmosis in Europe report onan epidemiological survey from the European Confederation of Medical MycologyWorking Gropu. Med Mycol 2008; 46: 57–65.
Academy 713
© The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2011/0909 JDDG | 9˙2011 (Band 9)

13 Wheat J, Sarosi G, McKinsey D, Hamill R, Bradsher R, Johnson PH, et al. PracticeGuidelines for the Management of Patients with histoplasmosis. Clin Infect Dis 2000;30: 688–95.
14 Brummer E, Castaneda E, Restrepo A. Paracoccidioidomycosis: an update. ClinMicrobiol Rev 1993; 6: 89–117.
15 Ameen M, Talhari C, Talhari S. Advances in paracoccidioidomycosis. Clin Exp Derma-tol 2010; 35: 576–80.
16 Shikanai-Yasuda MA, Telles Filho Fde Q, Mendes RP. Guidelines in paracoccidioi-domycosis. Rev Soc Bras Med Trop 2006; 39: 297–310.
17 Yasuda MA. Pharmacological management of paracoccidioidomycosis. Expert OpinPharmacother 2005; 6: 385–97.
18 Saccente M, Woods GL. Clinical and laboratory update on blastomycosis. Clin Micro-biol Rev 2010; 23: 367–81.
714 Academy
JDDG | 9˙2011 (Band 9) © The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2011/0909

Academy 715
© The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2011/0909 JDDG | 9˙2011 (Band 9)
1. Die beiden ätiologischen Erreger der Kokzidioidomykosesind:a) Cryptococcus neoformans und
Cryptococcus gattiib) Paracoccidioides brasiliensis und
Pseudallescheria boydiic) Coccidioides immitis und
Coccidioides posadasiid) Ajellomyces capsulatus und
Sporothrix globosae) Histoplasma capsulatum und
Blastomyces dermatitidis
2. Was beobachten Sie bei der Kokzidioidomykose in demNativpräparat mit KOH?a) muriforme Zellenb) doppelmembranige Spherulen mit
Endosporenc) multipolar sprossende Hefezellend) „asteroid bodies“ und elongierte
Hefene) intrazelluläre Hefen
3. Eines der bevorzugten chemo-therapeutischen Schemata bei einer disseminiertenKokzidioidomykose ist:a) Itraconazol 200–400 mg/d über
4 Monateb) Amphotericin-B-Desoxycholat
0,75 mg/kg/d + Itraconazol 300–400 mg/d
c) Ketoconazol 200 mg/d über 8 Monate
d) Trimethoprim-Sulfamethoxazol800/160 mg/d über 1 Jahr
e) Fluconazol 200 mg/d über 6–8 Wochen
4. Die wichtigsten Träger des Erre-gers und das Habitat des Histoplasmacapsulatum, des ätiologischenErregers der Histoplasmose, sind:a) Mangroven und stagnierende
Gewässerb) kalkhaltige Böden und Kot von
Fledermäusen und Vögelnc) Rinderkot und verseuchte Weidend) aride Regionen und abgestorbenes
pflanzliches Gewebee) Kaffeeanbaugebiete und Stacheln
5. In der Labordiagnostik der Histo-plasmose beobachten Sie:a) doppelmembranige Spherulen mit
Endosporenb) unipolar sprossende Hefezellenc) multipolar sprossende Hefezellend) zweisprossige kapsulierte Hefene) intrazelluläre Hefen mit lichtbre-
chenden Rand
6. Markieren Sie die häufigsten Differenzialdiagnosen der dissemi-nierten kutanen Histoplasmose inPatienten mit HIV/AIDS:a) Blastomykose und Myzetomb) Sporotrichose und
Chromoblastomykosec) disseminierte kutane Kryptokokkose
und Molluscum contagiosumd) Syphilis III und Aktinomykosee) Phaeohyphomykose und
Leishmaniose
7. Die klinische Hauptlokalisationder Parakokzidioidomykose ist:a) Rumpf und untere Extremitätenb) Rumpf und obere Extremitäten
c) Kopfhaut und Nackend) Lippen, Nase und buccopharyn-
geale Höhlene) anogenitaler Bereich und untere
Extremitäten
8. Welche Struktur findet man imNativpräparat einer Parakokzidioi-domykose?a) intrazelluläre Hefen mit doppel-
brechenden Randb) muriforme Zellenc) multipolar sprossende Hefezellend) elongierte unipolar sprossende
Hefezellene) kapsulierte Hefen
9. Welche sind die Behandlungsop-tionen bei der Parakokzidioidomy-kose?a) Amphotericin B/Kaliumjodid/
Equinocandine (Neumokandyne)b) Sulfonamide/Azolderivate/
Amphotericin Bc) Equinocandine/Azolderivate/
Penicillind) Sulfonamide/Benzylamine/
Kaliumjodide) Aminoglykoside/Makrolide/
Amphotericin B
10. Welche Struktur findet man imNativpräparat einer Blastomykose?a) intrazelluläre Hefen mit doppel-
brechendem Randb) mikrosiphonierte Drusenc) muriforme Zellend) einsprossige Hefen mit refringenter
Zellwande) multipolar sprossende Hefezellen
Fragen zur Zertifizierung durch die DDA
Liebe Leserinnen und Leser,der Einsendeschluss an die DDA für diese Ausgabe ist der 21. Oktober 2011.Die richtige Lösung zum Thema „Aktuelle Standards zur Diagnostik und Therapie von Haarerkrankungen – Haarsprechstunde“in Heft 5 (Mai 2011) ist: 1b, 2d, 3b, 4e, 5c, 6c, 7d, 8b, 9c, 10c.Bitte verwenden Sie für Ihre Einsendung das aktuelle Formblatt auf der folgenden Seite oder aber geben Sie Ihre Lösung onlineunter http://jddg.akademie-dda.de ein.












![Blastomycosis - A Northwoods Nuisance · Blastomycosis - A Northwoods Nuisance Lake Tides ... Photo courtesy of John Archer Photo courtesy of John Archer [Blastomycosis] is treatable,](https://img.dokumen.tips/doc/110x75/5b8fe87009d3f27a6d8d0c4a/blastomycosis-a-northwoods-nuisance-blastomycosis-a-northwoods-nuisance.jpg)















