Embed Size (px)
Citation preview

Kidney International, Vol. 64 (2003), pp. 1808–1816
End-stage renal disease in Scotland: Outcomes and standardsof care
WENDY METCALFE, IZHAR H. KHAN, GORDON J. PRESCOTT, KEITH SIMPSON,and ALISON M. MACLEOD, ON BEHALF OF THE SCOTTISH RENAL REGISTRY
Department of Medicine and Therapeutics, University of Aberdeen, Aberdeen, Scotland, United Kingdom; Renal Unit,Aberdeen Royal Infirmary, Aberdeen, Scotland, United Kingdom; Department of Public Health, University of Aberdeen,Aberdeen, Scotland, United Kingdom; and Scottish Renal Registry, Walton Building, Glasgow Royal Infirmary, Glasgow,Scotland, United Kingdom
End-stage renal disease in Scotland: Outcomes and standardsof care.
Background. The number of patients starting renal replace-ment therapy (RRT) for end-stage renal disease (ESRD) inthe United Kingdom rises annually. Patients are increasinglyelderly with a greater prevalence of comorbid illness. Unad-justed survival, from the time of starting RRT, is not improving.The United Kingdom Renal Association has published recom-mended standards of treatment, which all United Kingdomnephrologists strive to attain. This study was devised to definethe impact of attaining recommended treatment standards, ad-justing for patient age and comorbid illnesses, upon survivalon RRT in the United Kingdom population.
Methods. A prospective, registry based, observational studyof all patients starting RRT in Scotland over a 1-year period,followed for the first 2 years of RRT.
Results. Of the 523 patients who were studied, 217 (41.5%)had died by 2 years of follow-up, 32% excluding deaths withinthe first 90 days. Age, comorbidity, weight when starting RRT,and attaining the recommended standards for albumin andhemoglobin had a significant impact upon survival.
Conclusion. This study has emphasized the very high mortal-ity of patients starting RRT in Scotland. By paying close atten-tion to the attainment of recommended standards of care forpatients with ESRD, it may be possible to improve upon cur-rent mortality figures. The monitoring of such success is onlypossible if correction is made for age and comorbidity.
The number of patients starting renal replacementtherapy (RRT) for end-stage renal disease (ESRD) con-tinues to rise annually. There is evidence that this islargely due to increased access to RRT for older patientswith greater comorbidity, treatment that previously maynot have been available to them. The reported crude sur-vival of patients treated by RRT is not improving, proba-bly because of this increasing age and infirmity of the
Key words: Scottish Renal Registry, comorbidity, standards of care.
Received for publication September 16, 2002and in revised form February 10, 2003, and May 1, 2003Accepted for publication June 26, 2003
2003 by the International Society of Nephrology
1808
RRT population. When survival is adjusted for age andprimary renal diagnosis (PRD), however, improvementsare seen in survival across Europe [1] and the UnitedStates [2].
One of the challenges currently facing nephrologistsis to improve the survival of an infirm RRT populationby optimizing their treatment.
In 1995, the Renal Association of the United Kingdom(UKRA) published a consensus document of recom-mended standards for the treatment of adult patientswith ESRD [3], an expanded second edition was pub-lished in 1997 [4]. The purpose of this document wasto provide recommended standards for optimal clinicalpractices to guide nephrologists and thereby improvepatient outcomes. Similarly, in the United States, theNational Kidney Foundation established the DialysisOutcomes Quality Initiative (DOQI) in 1995 [5].
The frequency of comorbid illness amongst the inci-dent RRT population is rising [6, 7]. The presence ofillnesses such as diabetes, atherosclerotic cardiac andcerebral disease, or malignancy have long been recog-nized to confer an increased mortality risk in the ESRDpopulation [8, 9]. The effect of comorbidity upon at-taining recommended treatment standards is not welldescribed.
Large registries report the survival of patients treatedby RRT. In the United States, the United States RenalData System (USRDS) reports no statistics relating tothe first 90 days of treatment but reports details of theeffects of standards of care. European registries whilenot systematically excluding the first 90 days of treatmentcannot claim with certainty to have registered all patientsdying within this period. Such patients are difficult toidentify particularly using retrospective methods and soactual mortality probably exceeds those estimates avail-able. The Scottish Renal Registry (SRR), while reportingupon all patients receiving RRT for ESRD in Scotland,does not yet routinely take into account comorbid ill-nesses.

Metcalfe et al: End-stage renal disease in Scotland 1809
Table 1. Mode of presentationfor renal replacement therapy (RRT)
Presentation
Planned Permanent vascular or peritoneal accessready for use for first RRT
Unplanned Follow-up by nephrologist for �1 month,steady progression to end-stage, nopermanent access
Acute renal failure Presentation with presumed acute renalfailure but failure to recover function
Acute on chronic Follow-up by nephrologist for �1 month,unexpected acute deterioration infunction to reach end-stage
End-stage Require RRT within 1 month ofpresentation to a nephrologist
The purpose of this study was to prospectively inves-tigate all patients starting RRT in a defined UnitedKingdom population, to assess the impact of attainingrecommended treatment standards for hemoglobin con-centration, serum albumin and hemodialysis adequacyupon mortality, and to adjust this assessment for age,burden of comorbid illnesses, and other factors, whichmight influence survival and standard attainment.
METHODS
Between October 1, 1997 and September 30, 1998, alladult patients starting RRT for ESRD in Scotland’s 11adult renal units were registered when they started RRTand their treatment was assessed over the next 2 years.Data relating to attainment of treatment standards werecollected for each patient after 3, 6, 9, 12, and 18 months’duration of treatment.
Patients were identified weekly by one of us contactinga liaison person in each unit. A monthly checklist wascirculated to each unit to ensure no patients had beenmissed. The data routinely collected by the SRR wereaugmented by data collected at each site by a singlemedically qualified observer (W.M.) from patients, casenotes, and, where available, renal unit computer systems,and entered directly on to the Registry via a securemodem. Baseline and follow-up information were col-lected in the same way. The same single observer scoredpatients’ comorbidity and allocated them to groups ac-cording to presentation and diagnosis, at the time ofstarting RRT. The data collected at baseline were age,gender, race, primary renal diagnosis, comorbidity, modeand access for RRT, mode of presentation, duration ofcare by a nephrologist prior to starting RRT, weight,hemoglobin, and albumin. The SRR does not routinelycollect data pertaining to duration of care by a nephrolo-gist prior to the initiation of RRT, comorbidity, weight,or serum albumin. The patients were registered on theday they started RRT, except those failing to recoverfrom presumed acute renal failure, who were registered
Table 2. Charlson comorbidity score
Weight Condition
1 Myocardial InfarctCCFPeripheral vascular diseaseCerebrovascular diseaseDementiaChronic pulmonary diseaseConnective tissue diseasePeptic ulcer diseaseMild liver diseaseDiabetes
2 HemiplegiaModerate or severe renal diseaseDiabetes with end-organ damageAny tumour (solid tumour without metastases
diagnosed in past 5 years)Leukemia (acute and chronic and polycythemia vera)Lymphoma (includes Hodgkins, Waldenstroms,
myeloma, lymphosarcoma)3 Moderate or severe liver disease (cirrhosis, portal
hypertension, varices)6 Metastatic solid tumor
HIV
when the physician caring for them considered theywould require permanent RRT. Patients were prospec-tively entered into five groups according to their modeof presentation for RRT (Table 1) as previously de-scribed [10]. Follow-up was measured in months fromthe time the patient was first seen by a nephrologist tothe time of their first RRT; thus, follow-up is the periodunder the care of a nephrologist prior to starting RRT.
Patients were grouped according to comorbid condi-tions present when starting RRT using the Charlson in-dex of comorbidity (Table 2) [11, 12]. The Charlsonindex was used excluding age, which was entered intothe analyses as a separate variable. All patients had se-vere renal disease by definition and therefore the twopoints usually accorded for this diagnosis were disre-garded. Angina is not included within the Charlson scor-ing system and was analyzed separately.
A primary renal diagnosis code was chosen from thelist issued by the European Renal Association-EuropeanDialysis and Transplant Association (ERA-EDTA). Di-agnoses in the ERA-EDTA list have previously beenplaced into seven categories: (1) primary glomerulo-nephritis, (2) interstitial disease, (3) diabetes, (4) hyper-tensive nephropathy, (5) atherosclerotic renal disease, (6)other multisystem diseases, and (7) unknown cause [10].
Serum albumin was analyzed using bromocresol greenin all but 17 (3.2%) patients in whom bromocresol purplewas employed. Urea reduction ratio was calculated inall renal units using the “stop dialysate flow method”[13]. The attained serum albumin, hemoglobin and ureareduction ratio for each individual were recorded at eachof 3, 6, 9, 12, and 18 months’ duration of RRT or untildeath. Examination of the mean values at each time

Metcalfe et al: End-stage renal disease in Scotland1810
Table 3. Number and % of patients dying in the first 2 years ofrenal replacement therapy (RRT)
Overall mortality Excluding 90 dayDuration of RRT N � 523 deaths N � 450
90 days 14% 73 — —6 months 19.9% 104 6.9% 311 year 27.5% 144 15.8% 7118 months 35% 183 24.4% 1102 years 41.5% 217 32% 144
point, both for patients who survived and those whodied, showed that there was no long-term decline inthose patients who died.
For univariate analyses chi square, Kruskal Wallis ort tests were used where appropriate to identify factorsassociated with death within 2 years of starting RRT.Cox regression analysis was employed for multivariateanalyses of factors associated with length of survival.Serum albumin, hemoglobin, and urea reduction ratioswere analyzed as time-related covariates in the Cox re-gression analysis. Thus, each patient was analyzed ac-cording to whether the recommended standards hadbeen attained at each time point. A 5% significance levelwas employed throughout. All statistical analyses wereperformed using SPSS for windows version 9.0.
RESULTS
A total of 542 patients entered the study. After 2 years2 (0.4%) patients had been lost to follow-up and 17(3.1%) patients had unexpectedly recovered indepen-dent native renal function. These patients are excludedfrom the analyses discussed here. Fifty-four patients hadfunctioning renal transplants by the end of 2 years oftreatment; these patients are excluded from the survivalanalysis but included in the descriptive statistics.
Of the 523 patients studied, 217 (41.5%) were deadby the end of 2 years of follow-up. Excluding deathswithin the first 90 days of RRT, mortality after 1 yearwas 15.8% and 2-year mortality was 32% (Table 3). Theunadjusted mortality in the first year of RRT was 27.5%and in the second year 19.3% (73 of the 379 patientswho survived the first year of RRT) (see Fig. 1).
Cardiovascular or vascular disease elsewhere was re-sponsible for the death of 43.3% (94 patients) of allpatients dying within the first 2 years of starting RRT.Infection was the primary cause of death for 13.8% (30patients). Death followed withdrawal of RRT in 15.7%(34 patients) either through patient choice, medical deci-sion, or a combination of the two. The withdrawal oftreatment was always in the face of intractable comorbiddisease or disability. Malignant disease was the primarycause of death for 11.5% (25 patients) and of these 11(5% of the total cohort) died as a consequence of multi-ple myeloma which had been their primary renal disease.
Fig. 1. Survival from time of starting renal replacement therapy (RRT).Excludes those patients receiving a renal transplant.
Univariate analysis revealed that increasing age, co-morbidity, including angina, mode of presentation, initialmode of RRT, primary renal diagnosis group, short dura-tion of follow-up by a nephrologist prior to RRT, andinitial serum albumin were all significantly associatedwith death within 2 years of starting RRT. Low bodyweight when starting RRT was also associated with in-creased mortality, the average weight of those survivingfor 2 years or more after starting RRT was 70.7 kg (SD16.0), compared with 67.3 kg (SD 14.2) (P � 0.01, t test)for those dying within 2 years. Gender and hemoglobinconcentration at the time of starting RRT did not havea significant influence on survival in the univariate analy-sis. A diagnosis of diabetes per se, irrespective of PRD,did not influence 2-year survival; diabetes was only asso-ciated with reduced survival when it was the cause ofrenal failure (Table 4).
Mean attained hemoglobin, albumin and urea reduc-tion ratio values over the first 2 years of treatment werecalculated from blood results at 3, 6, 9, 12, and 18 monthsor until death. By necessity, patients dying within 90days were excluded. The average attained levels over 18months were divided into two groups, those on averageattaining the UKRA standards and those not. This wastaken as serum albumin �35g/L, hemoglobin �10 g/dL,and urea reduction ratio �65% (Table 5).
A higher attained albumin and hemoglobin were asso-ciated with survival in the univariate analysis both whenanalyzed as continuous variables and when grouped intoaverage values falling above and below the recommendedstandards of care. When the attained urea reduction ratioof patients treated throughout their RRT career onlyby hemodialysis were analyzed, a higher attained ureareduction ratio was again associated with survival but

Metcalfe et al: End-stage renal disease in Scotland 1811
Table 4. Patient characteristics when starting renal replacement therapy (RRT) and 2-year survival: Univariate analysis
Cohort 2-year mortality P value and(N � 523) number statistical test
Age group15–49 years 119 15 (12.6%) P � 0.00150–64 years 150 48 (32.0%) �2
65–75 years 168 98 (57.7%)�75 years 86 57 (66.3%)
GenderMales 311 126 (40.5%) P � 0.6Females 212 91 (42.9%) Fisher exact
Follow-up prior to RRT0 to 1 month 133 77 (57.9%) P � 0.0012 to 3 months 51 29 (56.9%) �2
4 to 6 months 28 11 (39.3%)7 to 12 months 53 17 (32.1%)�12 months 257 83 (32.3%)
PresentationPlanned 225 58 (25.8%) P � 0.001Unplanned 129 54 (41.9%) �2
Acute renal failure (no recovery) 53 36 (67.9%)Acute on chronic 62 42 (67.7%)End-stage renal disease 54 27 (50.0%)
First mode of RRTHemodialysis 400 187 (46.8%) P � 0.001Peritoneal dialysis 122 30 (24.6%) Fisher exact
Primary renal diagnosisGlomerulonephritis 69 19 (27.5%) P � 0.001Interstitial disease 119 33 (27.7%) �2
Multisystem disease 78 57 (73.1%)Hypertensive nephropathy 21 5 (23.8%)Secondary glomerulonephritis 27 9 (33.3%)Diabetic nephropathy 86 35 (40.7%)Unknown 123 59 (48.0%)
DiabetesPresent 124 58 (46.8%) P � 0.2No 399 159 (39.8%) Fisher exact
Charlson score0 194 34 (17.5%) P � 0.0011 102 53 (52.0%) �2
2 122 67 (54.9%)�2 105 63 (60.0%)
Angina grade0 372 129 (34.7%) P � 0.0011–2 128 73 (57.0%) �2
3–4 23 15 (65.2%)Serum albumin day 0
�35 g/L 192 110 (57.3%) P � 0.001�35 g/L 330 106 (32.1%) Fisher exact
Hemoglobin day 0�10 g/dL 329 142 (43.2%) P � 0.3�10 g/dL 192 74 (38.5%) Fisher exact
this effect was not seen when grouped according to therecommended standard of care.
Cox regression analysis was performed to identifythose factors significantly associated with death withinthe first 2 years of RRT when all influences were takeninto account. Patients who died within the first 90 daysof treatment were excluded from the analysis, as werethose lost to follow up, those who received a transplant,and those who recovered independent renal function.A further 15 patients were excluded from the analysisbecause they had incomplete records of albumin and/or
hemoglobin values over time precluding analysis as atime related variable. Therefore, 381 patients were en-tered into the analysis.
Age, Charlson grouping, body weight when startingRRT, and attaining the recommended standards for al-bumin and hemoglobin over the first 18 months of RRTall had a significant impact upon survival over the first2 years of RRT. The analysis was repeated with initialvalues of hemoglobin and albumin (those at the time ofstarting RRT) being retained within the Cox regressionmodel, in order to exclude the possibility that attained
Metcalfe et al: End-stage renal disease in Scotland1812
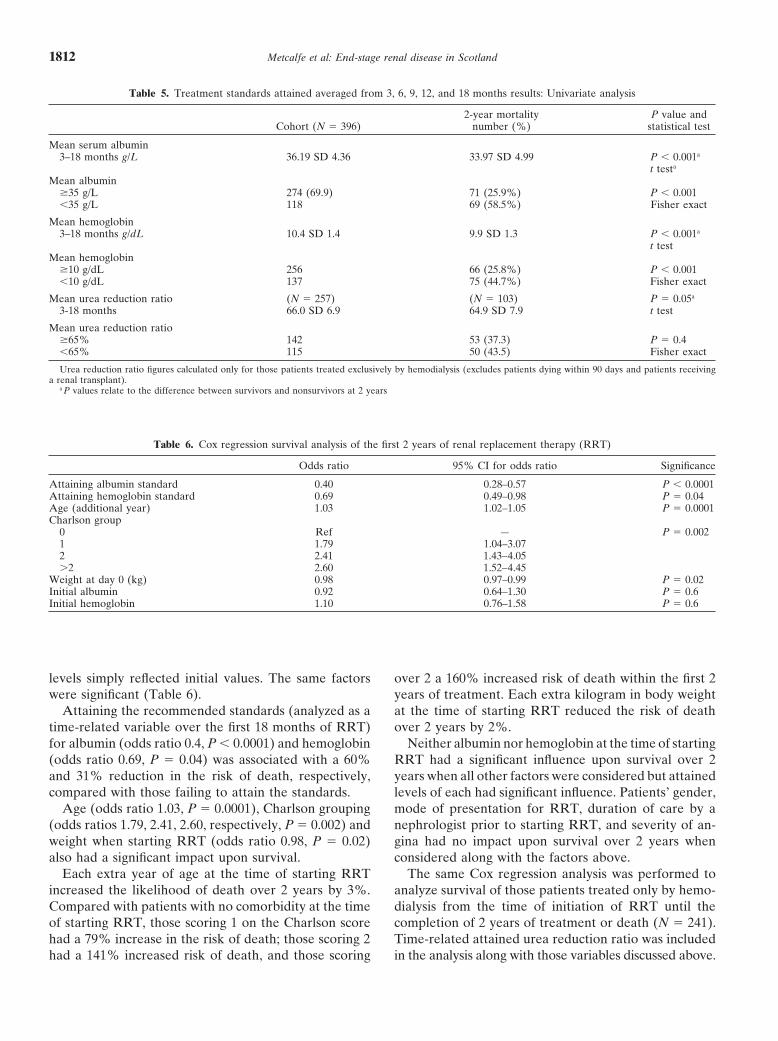
Table 5. Treatment standards attained averaged from 3, 6, 9, 12, and 18 months results: Univariate analysis
2-year mortality P value andCohort (N � 396) number (%) statistical test
Mean serum albumin3–18 months g/L 36.19 SD 4.36 33.97 SD 4.99 P � 0.001a
t testa
Mean albumin�35 g/L 274 (69.9) 71 (25.9%) P � 0.001�35 g/L 118 69 (58.5%) Fisher exact
Mean hemoglobin3–18 months g/dL 10.4 SD 1.4 9.9 SD 1.3 P � 0.001a
t testMean hemoglobin
�10 g/dL 256 66 (25.8%) P � 0.001�10 g/dL 137 75 (44.7%) Fisher exact
Mean urea reduction ratio (N � 257) (N � 103) P � 0.05a
3-18 months 66.0 SD 6.9 64.9 SD 7.9 t test
Mean urea reduction ratio�65% 142 53 (37.3) P � 0.4�65% 115 50 (43.5) Fisher exact
Urea reduction ratio figures calculated only for those patients treated exclusively by hemodialysis (excludes patients dying within 90 days and patients receivinga renal transplant).
a P values relate to the difference between survivors and nonsurvivors at 2 years
Table 6. Cox regression survival analysis of the first 2 years of renal replacement therapy (RRT)
Odds ratio 95% CI for odds ratio Significance
Attaining albumin standard 0.40 0.28–0.57 P � 0.0001Attaining hemoglobin standard 0.69 0.49–0.98 P � 0.04Age (additional year) 1.03 1.02–1.05 P � 0.0001Charlson group
0 Ref — P � 0.0021 1.79 1.04–3.072 2.41 1.43–4.05�2 2.60 1.52–4.45
Weight at day 0 (kg) 0.98 0.97–0.99 P � 0.02Initial albumin 0.92 0.64–1.30 P � 0.6Initial hemoglobin 1.10 0.76–1.58 P � 0.6
levels simply reflected initial values. The same factorswere significant (Table 6).
Attaining the recommended standards (analyzed as atime-related variable over the first 18 months of RRT)for albumin (odds ratio 0.4, P � 0.0001) and hemoglobin(odds ratio 0.69, P � 0.04) was associated with a 60%and 31% reduction in the risk of death, respectively,compared with those failing to attain the standards.
Age (odds ratio 1.03, P � 0.0001), Charlson grouping(odds ratios 1.79, 2.41, 2.60, respectively, P � 0.002) andweight when starting RRT (odds ratio 0.98, P � 0.02)also had a significant impact upon survival.
Each extra year of age at the time of starting RRTincreased the likelihood of death over 2 years by 3%.Compared with patients with no comorbidity at the timeof starting RRT, those scoring 1 on the Charlson scorehad a 79% increase in the risk of death; those scoring 2had a 141% increased risk of death, and those scoring
over 2 a 160% increased risk of death within the first 2years of treatment. Each extra kilogram in body weightat the time of starting RRT reduced the risk of deathover 2 years by 2%.
Neither albumin nor hemoglobin at the time of startingRRT had a significant influence upon survival over 2years when all other factors were considered but attainedlevels of each had significant influence. Patients’ gender,mode of presentation for RRT, duration of care by anephrologist prior to starting RRT, and severity of an-gina had no impact upon survival over 2 years whenconsidered along with the factors above.
The same Cox regression analysis was performed toanalyze survival of those patients treated only by hemo-dialysis from the time of initiation of RRT until thecompletion of 2 years of treatment or death (N � 241).Time-related attained urea reduction ratio was includedin the analysis along with those variables discussed above.
Metcalfe et al: End-stage renal disease in Scotland 1813
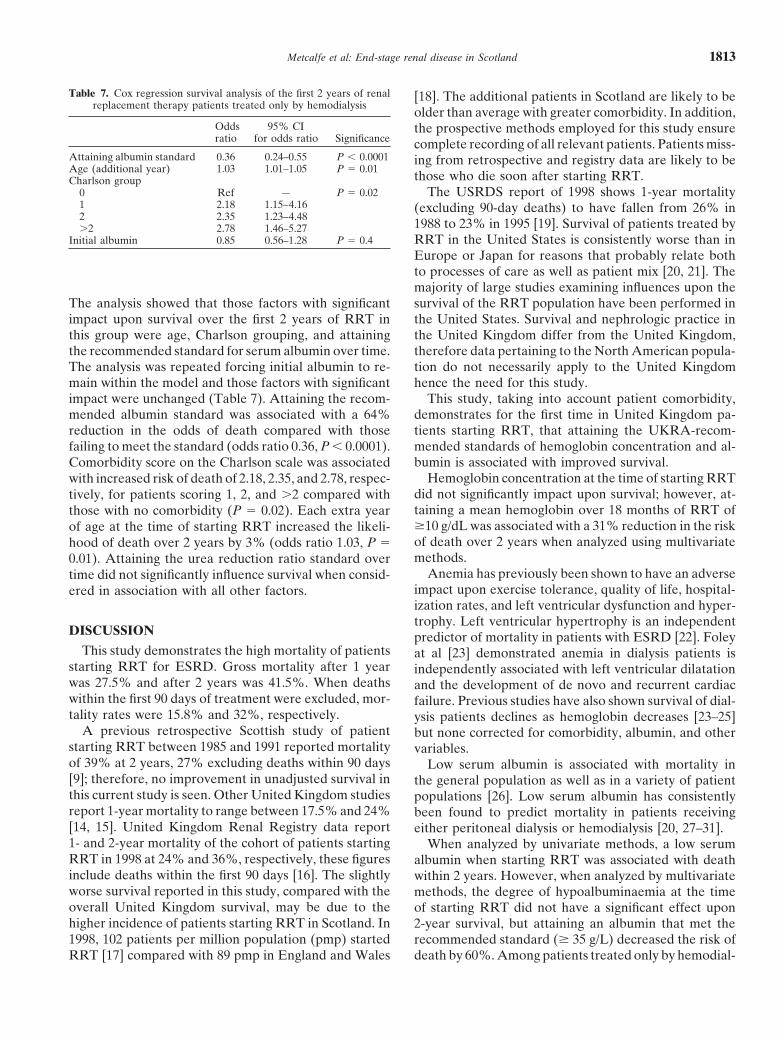
Table 7. Cox regression survival analysis of the first 2 years of renalreplacement therapy patients treated only by hemodialysis
Odds 95% CIratio for odds ratio Significance
Attaining albumin standard 0.36 0.24–0.55 P � 0.0001Age (additional year) 1.03 1.01–1.05 P � 0.01Charlson group
0 Ref — P � 0.021 2.18 1.15–4.162 2.35 1.23–4.48�2 2.78 1.46–5.27
Initial albumin 0.85 0.56–1.28 P � 0.4
The analysis showed that those factors with significantimpact upon survival over the first 2 years of RRT inthis group were age, Charlson grouping, and attainingthe recommended standard for serum albumin over time.The analysis was repeated forcing initial albumin to re-main within the model and those factors with significantimpact were unchanged (Table 7). Attaining the recom-mended albumin standard was associated with a 64%reduction in the odds of death compared with thosefailing to meet the standard (odds ratio 0.36, P � 0.0001).Comorbidity score on the Charlson scale was associatedwith increased risk of death of 2.18, 2.35, and 2.78, respec-tively, for patients scoring 1, 2, and �2 compared withthose with no comorbidity (P � 0.02). Each extra yearof age at the time of starting RRT increased the likeli-hood of death over 2 years by 3% (odds ratio 1.03, P �0.01). Attaining the urea reduction ratio standard overtime did not significantly influence survival when consid-ered in association with all other factors.
DISCUSSION
This study demonstrates the high mortality of patientsstarting RRT for ESRD. Gross mortality after 1 yearwas 27.5% and after 2 years was 41.5%. When deathswithin the first 90 days of treatment were excluded, mor-tality rates were 15.8% and 32%, respectively.
A previous retrospective Scottish study of patientstarting RRT between 1985 and 1991 reported mortalityof 39% at 2 years, 27% excluding deaths within 90 days[9]; therefore, no improvement in unadjusted survival inthis current study is seen. Other United Kingdom studiesreport 1-year mortality to range between 17.5% and 24%[14, 15]. United Kingdom Renal Registry data report1- and 2-year mortality of the cohort of patients startingRRT in 1998 at 24% and 36%, respectively, these figuresinclude deaths within the first 90 days [16]. The slightlyworse survival reported in this study, compared with theoverall United Kingdom survival, may be due to thehigher incidence of patients starting RRT in Scotland. In1998, 102 patients per million population (pmp) startedRRT [17] compared with 89 pmp in England and Wales
[18]. The additional patients in Scotland are likely to beolder than average with greater comorbidity. In addition,the prospective methods employed for this study ensurecomplete recording of all relevant patients. Patients miss-ing from retrospective and registry data are likely to bethose who die soon after starting RRT.
The USRDS report of 1998 shows 1-year mortality(excluding 90-day deaths) to have fallen from 26% in1988 to 23% in 1995 [19]. Survival of patients treated byRRT in the United States is consistently worse than inEurope or Japan for reasons that probably relate bothto processes of care as well as patient mix [20, 21]. Themajority of large studies examining influences upon thesurvival of the RRT population have been performed inthe United States. Survival and nephrologic practice inthe United Kingdom differ from the United Kingdom,therefore data pertaining to the North American popula-tion do not necessarily apply to the United Kingdomhence the need for this study.
This study, taking into account patient comorbidity,demonstrates for the first time in United Kingdom pa-tients starting RRT, that attaining the UKRA-recom-mended standards of hemoglobin concentration and al-bumin is associated with improved survival.
Hemoglobin concentration at the time of starting RRTdid not significantly impact upon survival; however, at-taining a mean hemoglobin over 18 months of RRT of�10 g/dL was associated with a 31% reduction in the riskof death over 2 years when analyzed using multivariatemethods.
Anemia has previously been shown to have an adverseimpact upon exercise tolerance, quality of life, hospital-ization rates, and left ventricular dysfunction and hyper-trophy. Left ventricular hypertrophy is an independentpredictor of mortality in patients with ESRD [22]. Foleyat al [23] demonstrated anemia in dialysis patients isindependently associated with left ventricular dilatationand the development of de novo and recurrent cardiacfailure. Previous studies have also shown survival of dial-ysis patients declines as hemoglobin decreases [23–25]but none corrected for comorbidity, albumin, and othervariables.
Low serum albumin is associated with mortality inthe general population as well as in a variety of patientpopulations [26]. Low serum albumin has consistentlybeen found to predict mortality in patients receivingeither peritoneal dialysis or hemodialysis [20, 27–31].
When analyzed by univariate methods, a low serumalbumin when starting RRT was associated with deathwithin 2 years. However, when analyzed by multivariatemethods, the degree of hypoalbuminaemia at the timeof starting RRT did not have a significant effect upon2-year survival, but attaining an albumin that met therecommended standard (� 35 g/L) decreased the risk ofdeath by 60%. Among patients treated only by hemodial-

Metcalfe et al: End-stage renal disease in Scotland1814
ysis, the decrease in the odds of death was 64% for thoseattaining the recommended standard.
We did not find that attaining recommended urea re-duction ratio standards conferred a survival benefit de-spite a benefit of higher urea reduction ratio when ana-lyzed by univariate methods. This may be because only257 patients had only been treated by hemodialysis andwere therefore eligible for analysis of the influence ofurea reduction ratio. However, in contrast to previousstudies that have demonstrated a survival benefit of in-creasing urea reduction ratio, it was the aim of treatmentfor all patients to have a urea reduction ratio of �65%;therefore, the mean urea reduction ratio of the cohortwas 66; SD 6.9. There was little variation in the attainedurea reduction ratio for the majority of patients and thusother influences upon survival, such as comorbidity, hadgreater impact.
There is evidence, again mainly from North America,that survival of patients on hemodialysis is positivelyassociated with high interdialytic removal of low-molecu-lar-weight toxins, of which urea is an easily measuredsurrogate [20, 28, 32–38]. The evidence that improvingsuch adequacy of dialysis in patients treated by perito-neal dialysis is less consistent, but the CANUSA studyreported this to be the case [30]. Differing survival ratesbetween American dialysis centers have also been shownto correlate with the average urea reduction ratios at-tained in each center [39].
The major impact of comorbid illness on survival ofpatients treated by RRT is demonstrated by this study.Both in the cohort as a whole and the subset treatedexclusively by hemodialysis, increased comorbidity was astrong predictor of poor outcome. Compared with thosewith no comorbid illnesses, patients scoring more than2 on the Charlson scale had 2.6 times the odds of deathover 2 years when all other factors had been taken intoaccount.
The adverse effect of comorbidity upon survival ofpatients on RRT is well documented [9, 40–42]. Thechallenge is to adopt a method of recording comorbidityuniformly in a straightforward manner so that survivalstatistics can be meaningfully compared between patientgroups and units providing RRT. The Charlson index ofcomorbidity is a widely used tool in areas other thanESRD. It has been used in previous studies of patientswith ESRD and found to predict survival in patientstreated both by peritoneal dialysis [43] and a cross-sec-tion of patients treated by hemodialysis [44]. The Charl-son index is unambiguous and straightforward to use,thereby providing a uniform, reproducible score of co-morbidity.
Patient’s primary renal diagnosis did not significantlyinfluence mortality when considered in association withall other factors however several primary renal diagnosesimply comorbid illnesses. The multisystem disease group
consisted largely of those with renal failure as a conse-quence of multiple myeloma or atherosclerotic renal ar-tery disease. Five percent of total deaths in this studywere due to myeloma. This poor prognosis is reflectedin a retrospective study of USRDS data, which reporteda 58% 2-year mortality for patients with myeloma com-pared with 31% in all other patients [45]. The proportionof patients starting RRT who have atherosclerotic reno-vascular disease causing their renal failure is increasing;anecdotally, they are also assumed to comprise a largeproportion of patients in whom a definitive diagnosis isnot possible. Such patients are also likely to have coro-nary heart disease, peripheral vascular disease, andcerebrovascular disease [46].
Greater body weight when starting RRT was demon-strated to confer a survival benefit, each extra kilogramin weight reducing the odds of death within 2 years by2%. We did not have any further information availablefrom which an estimation of body mass index or leanbody mass could be calculated and therefore the signifi-cance of this finding is difficult to qualify. It is possiblethat body weight is acting as a crude marker of nutrition.Poor nutritional status has been described to be a poorprognostic indicator for patients treated by RRT [29, 31,47]. Examination of the data suggested that body weightwas not simply a surrogate marker of either gender orserum albumin since there was no consistent relationshipbetween weight and these variables.
This study has emphasized the very high mortality ofpatients starting RRT in Scotland. Age, comorbidity,and attaining recommended standards of care for hemo-globin and serum albumin are the major factors affectingsurvival of patients receiving RRT. This information isimportant for nephrologists and generalists alike in orderto inform discussions with patients and their relatives,and thus prevent unrealistic expectations of outcomeson RRT. RRT is truthfully described as a life-savingtreatment, those with ESRD cannot survive without it;however, the effect of comorbid illnesses must be consid-ered.
In all observational studies of this type, causality can-not be deduced and hence we have been careful to reportassociations and not infer causality. The correlation be-tween attainment of standards and outcomes, however,remains significant after all efforts were made to adjustfor confounding factors. It is by refining the data ele-ments collected in observational studies, including co-horts of patients systematically reported by registries,that we can improve upon the information they provide.This study highlights not only the need for comorbidityto be taken into account but also the necessity of findinga practical method for routinely doing so, including thedefinition of a minimum data set for comorbidity thatwill reflect outcomes.
By paying close attention to the attainment of recom-
Metcalfe et al: End-stage renal disease in Scotland 1815
mended standards of care for patients with ESRD it maybe possible to improve upon current mortality figures.However, the monitoring of such success is only possibleif correction is made for age, comorbidity, and serumalbumin. A uniform method of adjusting for comorbidityshould be adopted in order to allow for direct compari-son of outcomes between patient groups, facilities pro-viding RRT, and internationally.
ACKNOWLEDGMENTS
We would like to thank the staff of Scotland’s adult renal units fortheir help in executing this study: Aberdeen Royal Infirmary; Cross-house Hospital, Kilmarnock; Dumfries and Galloway Royal Infirmary;Glasgow Royal Infirmary; Monklands Hospital, Airdrie; NinewellsHospital, Dundee; Queen Margaret’s Hospital, Dunfremline; Raig-more Hospital, Inverness; Royal Infirmary of Edinburgh; Stobhill Hos-pital, Glasgow; Western Infirmary, Glasgow. Funding was providedby a grant from the Scottish Office Department of Health ClinicalResource and Audit Group (CRAG). The views expressed are thoseof the authors and not necessarily those of either the Scottish OfficeDepartment of Health or CRAG. The Scottish Renal Registry wasfunded jointly by all the Scottish Health Boards. The funding sourcedid not contribute to either the study design, collection, analysis orinterpretation of the data.
Reprint requests to Dr. Wendy Metcalfe, The Renal Unit, GloucesterRoyal Hospital, Great Western Road, Gloucester, England, GL1 3NN.E-mail: [email protected]
REFERENCES
1. Elinder CG, Jones E, Briggs JD, et al: Improved survival in renalreplacement therapy in Europe between 1975 and 1992. NephrolDial Transplant 14:2351–2356, 1999
2. Agodoa LY, Eggers PW: Renal replacement therapy in the UnitedSates: Data from the United States Renal Data System. Am JKidney Dis 25:19–133, 1995
3. Renal Association Standards Subcommittee: Treatment of AdultPatients With Renal Failure: Recommended Standards and AuditMeasures, 1st ed., London, Royal College of Physicians, 1995
4. Renal Association Standards Subcommittee: Treatment of AdultPatients With Renal Failure: Recommended Standards and AuditMeasures, 2nd ed., London, Royal College of Physicians, 1997.
5. National Kidney Foundation: Dialysis Outcomes Quality Initia-tive: Clinical Practice Guidelines, New York, National KidneyFoundation, 1997
6. Collins AJ, Hanson G, Umen A, et al: Changing risk factordemographics in end-stage renal disease patients entering haemo-dialysis and the impact on long-term mortality. Am J Kidney DisXV:422–432, 1990
7. Mailloux LU, Napolitano B, Bellucci AG, et al: The impact ofco-morbid risk factors at the start of dialysis upon survival ofESRD patients. ASAIO 42:164–169, 1996
8. Shapiro FL, Umen A: Risk factors in hemodialysis patient survival.ASAIO 6:176–184, 1983
9. Khan IH, Catto GRD, Edward N, et al: Influence of coexistingdisease on survival on renal-replacement therapy. Lancet 341:415–418, 1993
10. Metcalfe W, Khan IH, Prescott G, et al: On behalf of the ScottishRenal Registry. Can we improve early mortality in patients receiv-ing renal replacement therapy? Kidney Int 57:2539–2545, 2000
11. Charlson ME, Pompei P, Ales KL, MacKenzie RC: A newmethod of classifying prognostic comorbidity in longitudinal stud-ies: Development and validation. J Chron Dis 40:373–383, 1987
12. Charlson ME, Szatrowski TP, Peterson J, Gold J: Validationof a combined comorbidity index. J Clin Epidemiol 47:1245–1251,1994
13. Geddes CC, Traynor J, Walbaum D, et al: A new method of
post-dialysis urea sampling: The “stop dialysate flow” method.Nephrol Dial Transplant 15:517–523, 2000
14. Chandna SM, Schulz J, Lawrence C, et al: Is there a rationalefor rationing chronic dialysis. A hospital based cohort study offactors affecting survival and morbidity. Br Med J 318:217–223,1999
15. Walters G, Warwick G, Walls J: Analysis of patients dyingwithin one year of starting RRT. Am J Nephrol 20:358–363, 2000
16. Renal Registry Report UK, Bristol, UK Renal Registry, 200117. Scottish Renal Registry Report, 1998; www.show.scot.nhs.uk/srr18. Renal Registry Report UK, Bristol, UK Renal Registry, 199919. USRDS 1998 Report: V. Patient mortality and survival. Am J
Kidney Dis 32(Suppl 1):S69–S80, 199820. Collins AJ, Ma JZ, Umen A, Keshaviah P: Urea index and
other predictors of hemodialysis patient survival. Am J KidneyDis 23:272–282, 1994
21. Held PJ, Brunner F, Odaka M, et al: Five-year survival for end-stage renal disease patients in the United States, Europe and Japan,1982 to 1987. Am J Kidney Dis XV:451–457, 1990
22. Silberberg JS, Barre PE, Prichard SS, Sniderman AD: Impact ofleft ventricular hypertrophy on survival in end-stage renal disease.Kidney Int 36:286–290, 1989
23. Foley RN, Parfrey PS, Harnett JD, et al: The impact of anemiaon cardiomyopathy, morbidity, and mortality in end-stage renaldisease. Am J Kidney Dis 28:53–61, 1996
24. Collins AJ, Ma JZ, Xia A, Ebben J: Trends in anaemia treatmentwith erythropoietin usage and patient outcomes. J Am Soc Nephrol32(Suppl 4)S133–S141, 1998
25. Locatelli F, Conte F, Marcelli D: The impact of haematocritlevels and erythropoietin treatment on overall and cardiovascularmortality and morbidity—The experience of the Lombardy dialysisregistry. Nephrol Dial Transplant 13:1642–1644, 1998
26. Goldwasser P, Feldman J: Association of serum albumin andmortality risk. J Clin Epidemiol 50:693–703, 1997
27. Lowrie EG, Lew NL: Death risk in hemodialysis patients: Thepredictive value of commonly measured variables and an evalua-tion of death rate differences between facilities. Am J Kidney DisXV:458–482, 1990
28. Owen WF, Lew NL, Liu Y, et al: The urea reduction ratio andserum albumin concentration as predictors of mortality in patientsundergoing hemodialysis. N Engl J Med 329:1001–1006, 1993
29. Goldwasser P, Kaldas AI, Barth RH: Rise in serum albuminand creatinine in the first half year on hemodialysis. Kidney Int56:2260–2268, 1999
30. CANUSA Peritoneal Dialysis Study Group: Adequacy of dial-ysis and nutrition in continuous peritoneal dialysis: association withclinical outcomes. J Am Soc Nephrol 7:198–207, 1996
31. Leavey SF, Strawderman RL, Jones CA, et al: Simple nutritionalindicators as independent predictors of mortality in hemodialysispatients. Am J Kidney Dis 31:997–1006, 1998
32. Goldwasser P, Mittman N, Antignani A, et al: Predictors ofmortality in hemodialysis patients. J Am Soc Nephrol 3:1613–1622,1993
33. Hakim RM, Breyer J, Ismail N, Schulman G: Effects of dose ofdialysis on morbidity and mortality. Am J Kidney Dis 23:661–669,1994
34. Lowrie EG: Chronic dialysis treatment: Clinical outcome and re-lated processes of care. Am J Kidney Dis 24:255–266, 1994
35. Held PJ, Port FK, Wolfe RA, et al: The dose of hemodialysisand patient mortality. Kidney Int 50:550–556, 1996
36. Wolfe RA, Ashby VB, Daugirdas JT, et al: Body size, dose ofdialysis and mortality. Am J Kidney Dis 35:80–88, 2000
37. Hornberger JC: The hemodialysis prescription and quality-adjusted life expectancy. J Am Soc Nephrol 4:1004–1020, 1993
38. Maiorca R, Brunori G, Zubani R, et al: Predictive value of dialysisadequacy and nutrional indices for mortality and morbidity inCAPD and HD patients. A longitudinal study. Nephrol Dial Trans-plant 10:2295–2305, 1995
39. McClellan WM, Soucie JM, Flanders WD: Mortality in end-stage renal disease is associated with facility-to-facility differencesin adequacy of dialysis. J Am Soc Nephrol 9:1940–1947, 1998
40. Davies SJ, Russell L, Bryan J, et al: Comorbidity, urea kineticsand appetite in continuous peritoneal dialysis patients: Their inter-

Metcalfe et al: End-stage renal disease in Scotland1816
relationship and prediction of survival. Am J Kidney Dis 26:353–361, 1995
41. Foley RN, Parfrey PS, Hefferton D, et al: Advance predictionof early death in patients starting maintenance dialysis. Am J Kid-ney Dis 23:836–845, 1994
42. Nicolucci A, Cubasso D, Labbrozzi D, et al: Effect of coexistentdiseases on survival of patients undergoing dialysis. ASAIO38:M291–M295, 1992
43. Fried L, Bernardini J, Piraino B: Charlson comorbidity index asa predictor of outcomes in incident peritoneal dialysis patients.Am J Kidney Dis 27:337–342, 2001
44. Beddhu S, Bruns FJ, Saul M, et al: A simple comorbidity scalepredicts clinical outcomes and costs in dialysis patients. Am J Med108:609–613, 2000
45. Abbott KC, Agodoa LY: Multiple myeloma and light chain associ-ated nephropathy at end-stage renal disease in the United States:Patient characteristics and survival. Clin Nephrol 56:207–210, 2001
46. Fatica RA, Port FK, Yound EW: Incidence trends and mortalityin end-stage renal disease attributed to renovascular disease in theUnited States. Am J Kidney Dis 37:1184–1190, 2001
47. Chauveau P, Combe C, Laville M, et al: Factors influencing sur-vival in haemodialysis patients aged older than 75 years: 2.5-yearoutcome study. Am J Kidney Dis 37:997–1003, 2001





























