Embed Size (px)
Citation preview

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline
V2.0
June 2020

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 2 of 28
Summary
Background
The ‘Caring for patients at the end of life document’ supports staff to deliver safe, effective, holistic care to patients in the last days and hours of life.
The document provides an evidence based aide memoire and a single multi-disciplinary communication tool. Having the information within a single care plan supports clinical audit, providing the opportunity to demonstrate measurable improvements in care and supporting governance processes.
The care plan was developed with reference to the ‘One chance to get it right’ document (Leadership Alliance for care of dying people 2014) and the NICE quality standards (NICE QS144).

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 3 of 28
1. Aim/Purpose of this Guideline
1.1. To provide a resource for all healthcare professionals working on adult hospital wards on the correct processes for recording the care delivered to patients in the last days or hours of life. The care plan aims to support the multi-disciplinary team (MDT) to deliver high quality, individualised care for dying patients and to support those identified as important to the patient. The emphasis is on the provision of dignity, comfort, sensitive communication and compassionate care. This includes the management of the common symptoms at end of life and the provision of psychological, social, spiritual and practical support. 1.2. This version supersedes any previous versions of this document.
2. The Guidance
2.1. When to start the care plan
2.1.1. The ’Caring for patients at the end of life’ care plan (appendix 3) is suitable for both patients with a known terminal illness where dying is recognized, and those having experienced a sudden catastrophic event for example a stroke. 2.1.2. Deterioration amongst those patients with an established terminal illness may present as:
Profound weakness, usually bedbound & requiring assistance with all care.
Gaunt physical appearance, particularly with cancer.
Drowsy or reduced cognition may be disorientated to time or place, extreme difficulty in concentrating.
Diminished intake of food and fluids.
Difficulty swallowing.
National Council for Palliative Care 1997
Data Protection Act 2018 (General Data Protection Regulation – GDPR) Legislation
The Trust has a duty under the DPA18 to ensure that there is a valid legal basis to process personal and sensitive data. The legal basis for processing must be identified and documented before the processing begins. In many cases we may need consent; this must be explicit, informed and documented. We cannot rely on opt out, it must be opt in.
DPA18 is applicable to all staff; this includes those working as contractors and providers of services.
For more information about your obligations under the DPA18 please see the Information Use Framework Policy or contact the Information Governance Team [email protected]

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 4 of 28
2.1.3. Generally potentially reversible causes of deterioration (e.g. Infection, hypercalcemia, acute kidney injury, toxicity) have been explored, assessed and treated. The patient continues to deteriorate despite optimal medical management or the patient may choose to have no further treatment. 2.1.4. Commencing the care plan should be an MDT decision. Any member of the MDT can raise the possibility that the patient may be approaching end of life. 2.1.5. End of life, in the context of commencing this care plan refers to an expectation that the patient in question has a few hours/ days to live.
2.1.6. If the patient makes an unexpected recovery e.g. it is thought they may survive beyond the period of a few weeks, this document can be discontinued.
2.1.7. Any document is only as good as the information provided/completed; MDT members should work together in a supportive manner, to ensure the document is as fully completed as possible.
2.2. Completion notes
2.2.1. The care plan reflects the ‘Five priorities of care’ identified in the ‘One chance to get it right’ document, these are printed on the cover page for reference and provide the guiding principles upon which care should be planned and delivered. A poster summary of the ‘Five priorities’ & a ‘Five priorities expanded guidance leaflet for staff’ are available to print as appendices 3 & 4.
2.2.2. Where possible tick boxes have been provided, where more detailed information is indicated it is important that this is recorded. Throughout the document designated medical and nursing responsibilities are identified though at times these may overlap.
2.3. Quick reference guidance
2.3.1. Guidance notes are located to the rear of the care plan on page 14 and page 15. Care plan users will find advice on completing the document, discontinuing interventions, specialist referral, care etc.
2.3.2. The Cornwall & Isles of Scilly anticipatory prescribing guidance and associated drug conversion chart are displayed on the back of the document
2.4. Additional resources
2.4.1. The care plan should always be used with the Symptom Assessment Chart CHA4214 (appendix 6) & the companion Symptom Assessment Guide CHA 4259 (appendix 5).
2.4.2. Continuation sheets (CHA3740) can be added to the care plan if required.

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 5 of 28
3. Monitoring compliance and effectiveness
Element to be monitored
The audit will take into account record keeping by health professionals working on RCHT adult wards.
Lead Clinical nurse specialist end of life care Joint lead practitioners for specialist palliative & end of life care.
Tool Adherence to guidelines will be monitored as part of the ongoing audit process on a Word or Excel template specific to the topic.
Frequency 20 care plans of patients that are approaching end of life on RCHT adult wards will be audited monthly.
A report will be completed quarterly.
The report will be shared quarterly.
Reporting arrangements
End of Life Care Group
During the process of the audit if deficiencies are identified,
This will be highlighted at the next End of Life Care Group and an action plan agreed.
Acting on recommendations and Lead(s)
Action leads will be identified and a time frame for the action to be completed.
The action plan will be monitored by the Joint lead practitioners for specialist palliative & end of life care.
Change in practice and lessons to be shared
Required changes to practice will be identified and actioned within a time frame agreed on the action plan.
A lead member of the group will be identified to take each change forward where appropriate.
4. Equality and Diversity
4.1. This document complies with the Royal Cornwall Hospitals NHS Trust
service Equality and Diversity statement which can be found in the 'Equality, Inclusion & Human Rights Policy' or the Equality and Diversity website.
4.2. Equality Impact Assessment
The Initial Equality Impact Assessment Screening Form is at Appendix 2.

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 6 of 28
Appendix 1. Governance Information
Document Title End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0
This document replaces (exact title of previous version):
Clinical Guideline For End Of Life Care Plan V1.0
Date Issued/Approved: 20th February 2020
Date Valid From: June 2020
Date Valid To: June 2023
Directorate / Department responsible (author/owner):
Suzanne Adams, Joint Lead Practitioner Specialist Palliative & End Of Life Care
Contact details: Mobile number via Switchboard – 01872 250000
Brief summary of contents To give guidance to all healthcare professionals working on RCHT adult wards on the correct process for end of life care planning and processes.
Suggested Keywords: Treatment - Palliative care - Patient care
Target Audience RCHT CFT KCCG
Executive Director responsible for Policy:
Director of Nursing, Midwifery and Allied Health Professionals
Approval route for consultation and ratification:
End of Life Care Group
General Manager confirming approval processes
Kim O'Keefe
Name of Governance Lead confirming approval by specialty and care group management meetings
Claire Martin
Links to key external standards Ambitions for Palliative and End of Life Care: a national framework for local action 2015-2020
Related Documents: End of Life Care Strategy
Training Need Identified? Yes. Ward based training. Learning and development department informed.
Publication Location (refer to Policy on Policies – Approvals and Ratification):
Internet & Intranet Intranet Only
Document Library Folder/Sub Folder
Clinical / Palliative

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 7 of 28
Version Control Table
Date Version
No Summary of Changes
Changes Made by (Name and Job Title)
10/11/2016 V1.0 Initial version
Allison May End of Life Care Training Facilitator Palliative Care Team
20/02/2020 V2.0 Full update and transposed to latest Trust document – updated all areas.
Suzanne Adams, Joint Lead Practitioner Specialist Palliative & End Of Life Care
All or part of this document can be released under the Freedom of Information
Act 2000
This document is to be retained for 10 years from the date of expiry. This document is only valid on the day of printing
Controlled Document
This document has been created following the Royal Cornwall Hospitals NHS Trust Policy for the Development and Management of Knowledge, Procedural and Web
Documents (The Policy on Policies). It should not be altered in any way without the express permission of the author or their Line Manager.

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 8 of 28
Appendix 2. Equality Impact Assessment
Section 1: Equality Impact Assessment Form
Name of the strategy / policy /proposal / service function to be assessed End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0
Directorate and service area: Palliative & End Of Life Care
Is this a new or existing Policy? Existing
Name of individual/group completing EIA Suzanne Adams, Joint Lead Practitioner Specialist
Contact details: Mobile number via Switchboard – 01872 250000
1. Policy Aim Who is the strategy / policy / proposal / service function aimed at?
To give guidance to all healthcare professionals working on RCHT adult wards regarding completion of the end of life care plan.
2. Policy Objectives To ensure all staff communicate and document effectively when caring for patients who are approaching end of life and to promote excellence in care of the dying patient.
3. Policy Intended Outcomes
Good communication, good standards of documentation and improved patient experience.
4. How will you measure the outcome?
Compliance Monitoring Tool
5. Who is intended to benefit from the policy?
RCHT adult patients approaching end of life.
6a). Who did you consult with?
b). Please list any groups who have been consulted about this procedure.
Workforce Patients Local groups
External organisations
Other
X
Please record specific names of groups: Specialist palliative 7 end of life care team, ward managers and their teams,
Specialist Palliative Care Consultants, Medical Consultants.
c). What was the outcome of the consultation?
Agreed

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 9 of 28
Are there concerns that the policy could have a positive/negative impact on:
Protected Characteristic
Yes No Unsure Rationale for Assessment / Existing Evidence
Age
X
Sex (male, female non-binary, asexual etc)
X
Gender reassignment
X
Race/ethnic communities /groups
X
Disability (learning disability, physical disability, sensory impairment, mental health problems and some long term health conditions)
X
Religion/ other beliefs
X
Marriage and civil partnership
X
Pregnancy and maternity
X
Sexual orientation (bisexual, gay,
heterosexual, lesbian)
X
If all characteristics are ticked ‘no’, and this is not a major working or service change, you can end the assessment here as long as you have a robust rationale in place.
I am confident that section 2 of this EIA does not need completing as there are no highlighted risks of negative impact occurring because of this policy.
Name of person confirming result of initial impact assessment:
Suzanne Adams, Joint Lead Practitioner Specialist
If you have ticked ‘yes’ to any characteristic above OR this is a major working or service change, you will need to complete section 2 of the EIA form available here: Section 2. Full Equality Analysis For guidance please refer to the Equality Impact Assessments Policy (available from the document library) or contact the Human Rights, Equality and Inclusion Lead [email protected]
A summary of the results will be published on the Trust’s web site.
7. The Impact Please complete the following table. If you are unsure/don’t know if there is a negative impact you need to repeat the consultation step.

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 10 of 28
This Page Is Intentionally Blank
–
Please see Appendix 3 on following pages.

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 11 of 28
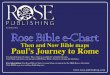
Appendix 3. Caring For Patients at the End of Life Form
This document should be viewed across two pages
Acknowledging uncertainty
Five priorities of
care
Who & when to
call
Copy LPA (legal) file in
the notes
When time is short
Plan with the patient
Review the plan daily & discontinue
if the patient
improves

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 12 of 28
Title page ‘Caring for patients at the end of life’: The care plan itself should be developed collaboratively with the patient and those important to them where possible. The patient’s mental capacity status and ability to engage in care planning should be recorded. Patients should always be addressed according to their preference. This should be identified and recorded. The details of family members and the preferences for contact in event of the patient’s deterioration should be documented, alongside any individuals having lasting power of attorney (LPA) for health and welfare. Copy documents of any LPA should be obtained, filed in the paper notes and sent to the Health records team for scanning and uploading to Maxims. For patients presenting at End of life in the emergency department, priority actions have been highlighted in red. For this patient group the care plan should be immediately revisited on transfer to the ward area where any outstanding actions should be completed.

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 13 of 28
Jonathan Atkins J. Atkins F1

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 14 of 28
Butterfly scheme-Nursing actions (page 2): Butterfly Cornwall is a scheme developed to enhance the immediate environment and experience of care for patients and their families at End of life. It incorporates a range of interventions including good practice measures such as communicating with ward based Mitie staff, practical assistance such as parking permits and comfort measures such as meal vouchers. The components of the scheme should be explained to the patient and/or family and consent to participate obtained. Patients with specific End of life wishes that can be facilitated by the ward team may be eligible for rapid financial support from the rainbow day fund. For more information contact the Specialist palliative & End of life care team. Preference for a sideroom should be established and sourced where possible to promote privacy. The patient and/or family should routinely be offered the ‘Caring for patients at the end of life’ leaflet. All care plan users (page 2): A signature sheet is provided on which all staff completing the care plan should record their details. If required this will support care after death or any investigations that may be indicated.

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 15 of 28
Any plan for consultation
or treatment
Document the discussion
Record MDT involvement
Support for certification
Start to
plan

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 16 of 28
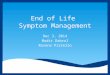
Initial medical review/plan (page 3): The decision to commence the care plan should preferably be taken during daytime hours by the senior doctor overseeing the patients care. In the absence of the senior doctor a delay in commencing EOL care should be avoided by seeking advice from the most senior doctor available. Any plan for consultation at the earliest opportunity should be documented; similarly where there is any prognostic uncertainty this should not delay commencing end of life care where this be to the detriment of the patient or family. Any plan to continue with a trial of treatment (ie antibiotics) alongside EOL care planning should be clearly documented. The decision to commence EOL care may be informed by the patient or family should include other members of the multi-disciplinary team. This should be recorded in the care plan. The recognition that the patient is likely to be dying and the reasons for this should be communicated swiftly and compassionately to patients and their loved ones. The content and participants in these discussions or any barriers to achieving this should be recorded. The treatment escalation plan (TEP) should be reviewed and updated if necessary. For those patients having a CRT-D or ICD the risk of burdensome device therapies should be mitigated. The clinician responsible for the current episode of care should contact the on-call Consultant Cardiologist (via RCHT switchboard) to arrange device deactivation at the earliest opportunity. Any Advance care plan or Advance decision to refuse treatment should be consulted in consultation with the patient/family. For patients lacking capacity any expressed wishes and preferences should inform the plan of care and form the basis for best interest decision making. Attempts should be made to establish and document the patient’s preferred place of death. Where possible and feasible every effort should be made to fulfil this and barriers to achieving this should be recorded. For those patients with a previously expressed wish for organ donation consideration should be given as to whether this is appropriate. Where this may be achievable, record and prepare for this ahead of time. For advice on organ donation ring the helpline on 03000 20 30 40. It is important to recognise that this is usually limited to patients who are ventilated in a critical care environment and that this can cause disappointment for some patients/families. Patients may be eligible for tissue/corneal donation -call the National Referral Centre on 0800 432 0559 for advice. Where able senior doctors should identify if a referral to the coroner or post mortem is anticipated, or document the suggested cause of death where known. The medical examiner can be contacted via the bereavement office 01872 252713.

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 17 of 28
Weigh the benefits &
the burdens
Discuss ahead of
time where possible

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 18 of 28
Initial medical review/plan (page 4): The benefits and burdens of all interventions and treatments should be weighed carefully at EOL with the recognition that comfort should be prioritised and over-treatment avoided. A review of routine monitoring should be recorded and should include the appropriateness of eobs, blood tests etc. Decisions should be individualised with exceptions made for those interventions which promote comfort and enhance symptom control for example:
Oxygen therapy: this may be continued if desaturation contributes to a patient’s confusion. This should be administered at the lowest flow rate required via nasal specs for patient comfort without routine monitoring of oxygen saturations.
Non-invasive ventilation (NIV): discuss a plan for weaning off and discontinuation with the patient and family/carer (specialist discussion).
Diabetes: in the last days of life poorly managed blood glucose can cause unpleasant symptoms. Keep tests to a minimum. If observed symptoms indicate hypo or hyperglycaemia, occasional blood or urine testing may be needed. More detailed guidance for managing diabetes at end of life is located separately on the end of life care shelf on the intranet.
Nutrition and hydration (page 4): Patients must be supported to eat and drink for as long as they are able to do so. A patient’s ability to eat and drink should be subject to ongoing review. Most patients in the last days of life experience loss of appetite and a decreased interest in food and drink, this can be distressing for families and the plan or care should be sensitively discussed and clearly documented. It is normal for a percentage of patients to experience dysphagia in the last days of life therefore a speech & language assessment can be helpful. A patient who has previously been assessed as unsafe for oral intake should still be offered food and drink if they wish it; and it is not distressing for them. Some patients that display thirst may benefit from IV/SC fluids and this should be considered on an individual basis. The risks & benefits of CAHN should be sensitively discussed with patient +/- family and documented. It should be acknowledged that CAH may cause problems such as discomfort swelling at infusion site, oedema and that it is not known if CAH prolongs life or whether it will hasten or extend the dying process Some patients may have already commenced artificial nutrition and the question of whether to withdraw this may arise and need to be considered on an individual basis. This can be a source of distress and unease for the patient and family. The risks and benefits of discontinuing feeds should be assessed individually, discussed sensitively and the outcome documented. During this process it is important that patients are not being kept nil by mouth inappropriately.

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 19 of 28
Rationalise medication
Discuss ahead of
time where possible
Plan for comfort
Prescribing guidance

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 20 of 28
Medication review/anticipatory prescribing (page 4): Consider discontinuing routine medication that is not contributing to symptom control. For patients no longer able to swallow some essential medication may need to be converted to an alternative route eg subcutaneous. This may include diuretics for pulmonary oedema or steroids for raised intracranial pressure. Medication should be prescribed to address each of the common symptoms that patients may experience at EOL. This should be prescribed subcutaneously and documented ahead of time and should reflect the Cornwall and Isles of Scilly anticipatory prescribing guidance (see back cover). Prescribing should be individualised and should be adjusted to reflect the patient’s current regime (see back cover). For patients with an eGFR<30 prescribing should reflect the Cornwall and Isles of Scilly renal prescribing guidance located on the EOL shelf on the intranet. An end of life electronic prescribing bundle is located on the EPMA system for opioid naïve patients (search EOL on EPMA). Two options are available and the appropriate one should be selected based upon the patient’s renal function. Specialist palliative & end of life care team (Page 4): Please refer all patients with complex symptom management issues, psychological distress or complex social circumstances to the specialist palliative and EOL care service. For patients at RCHT Contact via bleep 3055 or refer via Maxims, daily from 8am to 4pm. For patient in a community Hospital setting refer to the Community Specialist Palliative Care Team on Bodmin 01208 251300 For out of the hours advice please ring Cornwall Hospice Care advice line on 01736 757707 Syringe driver (page 4):
Patients requiring ongoing symptom relief should be prescribed a continuous subcutaneous infusion via a syringe driver. This should enable improved symptom control by continuous delivery, mitigating the need for repeated injections & allowing for multiple drug delivery. The rationale for subcutaneous administration, possible side effects and the potential need for a syringe driver should be sensitively discussed with the family and documented accordingly.

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 21 of 28
Ensure holistic care
Baseline comfort
assessment & care
rounding

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 22 of 28
Initial nursing review (page 5): A baseline nursing assessment should be completed to identify immediate symptom control needs, this should be documented alongside any action taken. Symptom assessment chart (CHA 4214, appendix 6) should be commenced alongside symptom assessment guidance (CHA 4259, Appendix 5) Hourly mouth care should be commenced routinely in all patients no longer taking regular oral fluids. The need to balance the benefits and burdens of repositioning should be carefully considered. Though end of life patients are high risk pressure damage is not inevitable risks should be mitigated where possible. An air mattress should be sourced and implemented immediately according to the skin bundle. The patient’s skin should always be kept clean and dry. Gently discussing the risks and the need for monitoring or repositioning can help patients and families. Report any pressure damage found on the Datix system. For advice contact the tissue viability team 07909930765 The need for any additional comfort measures ie catheterisation should be documented. Psychological, social and spiritual support (page 5): To ensure that holistic care is delivered three fields within the care plan are devoted to what is important to the patient and their family, what worries them and what may bring them comfort. Example question designed to facilitate the patient’s wishes, priorities and concerns eg. ‘What’s important to you now?’. This will enable staff to identify opportunities to offer support and comfort to the patient and their family. By completing these fields with the patient and their family staff can be confident that care remains individualised and that specific care needs are identified and met. An attempt should be made to identify any spiritual care needs. All patients should routinely be offered pastoral support and the outcome recorded. The hospital pastoral care team are available to offer pastoral support at end of life to patients of any or no faith and are on call 24/7. They can be contacted by bleep via the RCHT switchboard. Continuation of care (pages 6-12): Patient’s receiving EOL care should receive a daily medical review to assess if the patient is still considered to be dying and to decide if the current plan for EOL care is still appropriate. The Symptom assessment chart and prescribing and the EOL care plan should be reviewed daily to identify any new concerns relating to the patient/family and any adjustments in the care plan necessary to maintain comfort or alleviate distress. Continuation sheets (CHA3740) are available to order via Unit 4.

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 23 of 28
Carefully invite
concerns
Ensure individualised care in death
Standards for care after
death checklist
support best practice

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 24 of 28
Care after death (page 13): Any specific religious or cultural wishes and preferences should be identified and recorded ahead of time. Where possible these should be accommodated according to the trusts bereavement policy. Who was present at the patient’s death and whether the family were contacted according to their wishes should be recorded. The family should be sensitively informed of the patient’s death according to the Trust protocol. This can be found at in the bereavement policy located in the documents library. It is important to identify at the earliest opportunity any concerns the family may have about the patient’s care or death. There may be some instances where these can be addressed by the ward team and documented. For any concerns that require further investigation or escalation these should be clearly documented and communicated to the nurse in charge where a plan for follow up should be documented. It should be recorded that the family has been supplied with the Trust’s bereavement booklet. For patients at RCHT families should be advised that they will be contacted by the bereavement office the next working day. The patient should receive personal care according to the Trust care after death checklist. The verification of death section should be completed and recorded by a suitably qualified member of staff. This may be the doctor overseeing the patient’s care or, according to location, one of the nursing or site coordination team.

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 25 of 28
Appendix 3. Priorities for Care of the Dying Person

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 26 of 28
Appendix 4. Priorities for Care of the Dying Person

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 27 of 28
Appendix 5. CHA4259: Symptom Assessment Guidance For CHA4214

End of Life Care Plan and Symptom Assessment Chart Clinical Guideline V2.0 Page 28 of 28
Appendix 6. Symptom Assessment Chart CHA4214- Available to order via unit 4