Embed Size (px)
Citation preview

End of Life Care-An Integrated approach to service delivery

Programme
• Delivering Choice Programme – Simon Gordon, Senior Project Manager, Marie Curie Cancer Care
• Palliative Care Coordination Centre – Karen Torley, Regional Manager, Marie Curie Cancer Care Nursing Service
• Community Palliative Care Services – Julie Newby, Palliative Care Manager, STFT
• GP palliative care register – Lesley Davie, Project Manager, NECN
• Deciding Right – Sarah Rushbrooke, Network Quality and Patient Safety Director, NECN
• Future priorities – Dr Henry Choi, End of Life Lead, Sunderland Clinical Commissioning Group
Sunderland population (2010/11) 281,500
• Sunderland population (2010/11) 281,500
Total deaths 2,667

1,644 Hospital deaths (61.6%)
531 Home deaths (19.9%)
142 Hospice deaths (5.3%)
310 Nursing/Residential home deaths (11.6%)
40 Other (1.5%)

Thank you

Marie Curie Delivering Choice ProgrammeNorthumberland Tyne and Wear

Choice in place of care and death• Major gap between preference and what actually
happens
• Given the choice, more than 60% of us would prefer to be cared for and to die at home if we were terminally ill, surrounded by family and friends
• Just 4% of us would choose to die in hospital
“If I could wave a magic wand, I would just go home.”

Marie Curie Delivering Choice Programme
Our visionTogether, we will develop and provide
the best possible services for palliative care patients,
allowing them to be cared for in the place of their choice.
Programme objectives
Working in partnership with the NHS, social services, and the voluntary sector, we aim to provide:
1) Patient-focused 24-hour service models that serve local needs and ensure:
– The best possible care for palliative care patients– Choice in place of care and death is available to all– Improved equity of access to services – Appropriate support services to palliative care patients and
their carers– Information on choice is available and known to all– Improved co-ordination of care among stakeholders

Programme objectives2) Independent evaluation of the economic impact to healthcare
services of more patients receiving palliative care at home as compared with hospitals
3) Dissemination of findings to other health and social care providers leading to the replication of solutions across the UK

Northumberland Tyne and WearPhase 1 - 2009
• Distributed 2,400 questionnaires to various professional groups • Set up 25 focus groups with carers and professionals including
community matrons, District Nurses and home care nurses• Interviewed over 140 staff across services in hospitals, hospices,
ambulance providers and social care • Shadowed Out of Hours District Nurses and hospital-based social
workers• Observed patient case studies through admission and discharge
audits• Reviewed demographic, epidemiological and service utilisation data • Reviewed operational documentation of services• Listened to the experiences of 43 patients who are using palliative
care services
Northumberland Tyne and WearPhase 2 - 2009 onwards
• Following the Phase I investigation, a series of workstreams were proposed to improve palliative care services in the project area. At the Project Executive Committee meeting of 8th October 2009, the following work streams were approved for progression to Phase II:
• Workstream 1• Primary Care and Community Services- The development of consistent 24 hour are accessible,
responsive and coordinated– Workstream to be taken forward with two separate working groups for North and South of Tyne
• Workstream 2• Acute Care- Managing palliative care pathways
• Workstream 3• Appropriate transportation for patients with palliative care needs
• Workstream 4• Carer Support
• Workstream 5• The development of appropriate systems that allow communication across all providers
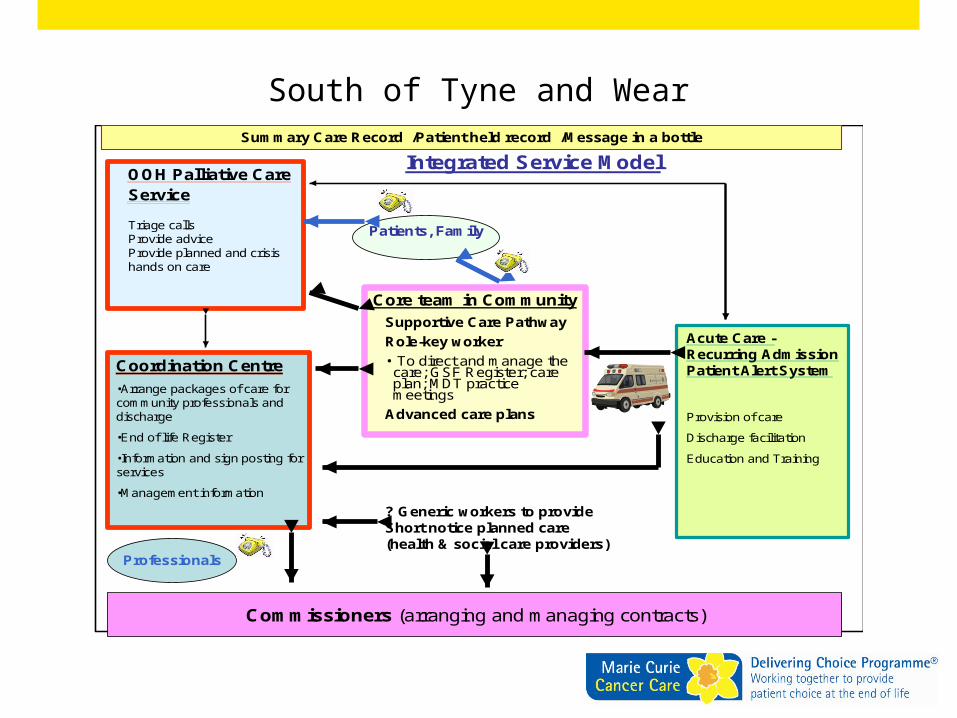
South of Tyne and Wear
Core team in Community
Patients, Family
Supportive Care Pathway
Role-key worker
• To direct and manage the care; GSF Register; care plan; MDT practice meetings
Advanced care plans
OOH Palliative Care Service
Triage callsProvide adviceProvide planned and crisis hands on care
Acute Care -Recurring Admission Patient Alert System
Provision of care
Discharge facilitation
Education and Training
Integrated Service Model
Professionals
? Generic workers to provideShort notice planned care(health & social care providers)
Coordination Centre
•Arrange packages of care for community professionals and discharge
•End of life Register
•Information and sign posting for services
•Management information
Commissioners (arranging and managing contracts)
Summary Care Record /Patient held record /Message in a bottle

Contact Details
Simon Gordon
Senior Project Manager
Marie Curie Cancer Care
Tel: 0191 219 1042
Mob: 0782 4837 384
Email: [email protected]
http://deliveringchoice.mariecurie.org.uk

Thank you

South of Tyne and Wear Palliative Care Coordination Centre

Aims• Improve the co-ordination and provision of packages of
care for patients at the end of life and their families.
• Enable people to be cared for and to die in the place of their choice.
• Facilitate effective use of resources and provide management information on service utilisation.
• Maintain a locality palliative care register.

Key Daily Tasks• Receive fax or telephone referrals from DN’s and other healthcare
professionals• Communicate patient care needs to appropriate care providers• Consult with care providers to co-ordinate packages of care.• Facilitate ordering of equipment.• Communicate care bookings to all appropriate healthcare
professionals and patients.• Modify care packages as necessary and communicate changes when
they are received.• Maintain and update palliative care register.• Signposting facility for “inappropriate calls”.

Overview of Centre• 1 Coordination Centre Manager supported by 5
Palliative Care Coordinator Administrators
• Based at Marie Curie Hospice, Newcastle
• Hours of service: 8am - 6pm Monday-Friday 10am - 3pm Saturday-
Sunday
• Bespoke telephony and IT systems
How will the centre benefit local users?• Reduce the amount of time spent by clinical staff
organising packages of care, allowing time to be reinvested into the delivery of clinical care
• Improve the organisation of care through a coordinated approach.
• Provide support in the booking of care packages to all professional groups
• Promote integrated working across health and social care professionals
• Holding and maintaining a palliative care register for South of Tyne and Wear

Outcomes for CommissionersFunction of PCCCResponse time and prioritisationKey patient data collectionUser feedback
Outcomes for patients Patient and carer preferred place of careSingle point of contact

Thank you

Gateshead and South Tyneside Out of Hours
Specialist Palliative care Team
Commencing April 2nd 2012
Julie Newby Feb 2012

The Sunderland ModelPopulation 297,00
“Legacy of our post Industrial and Mining Economy”High levels of: • CA• HF• Alcohol consumption• Smoking and obesity• Social depravation• Unemployment• Early Mortality
Gateshead210,000
South Tyneside150,000

Sunderland Overnight Palliative Care Team commenced 9th February 1998
Awarded Beacon Status 1999
Cited in the National Cancer Plan(2000) as a model of excellence for the development of overnight Palliative care services.
The Past

The Aim
‘To enable people to be cared for/die in the place of
their choice’

Drivers for Change
• Locally – The team struggling to meet demand
• NICE Palliative and Supportive Care Guidelines (2004)
• EOL Strategy(2008)• Palliative Care for all life limiting diseases• ACP/PPC• Demographics and Cost

The Present
October 2008 the OOH specialist palliative care team now worksfrom 4pm-9.15am every evening and night
Two trained nurses are on duty each evening and night providingdirect planned care in patients homes, residential/nursing homesand responding to crisis calls as well as telephone triage/advice/Support
Provide advice/support to staff and patients in hospital/hospice

Aims of the Service
Provide a service which enables patients with cancer or other life limiting conditions to be cared for/die in the place of their choice.
Facilitate rapid discharge from hospital/hospice both in and out of hours.
Offer a planned visit following discharge from hospice/hospital.
Provide a co-ordinated and flexible/seamless service to meet the patient/carers needs over the 24 hours period.

Referrals
• DN• GP• Primecare (OOH Deputising Service)• UCT/24/7• Community Matrons• Hospice• Paramedics
• Local acute trust.• A&E• Specialist PC nurses (community/hospital)• PC Consultants• Marie Curie• Telecare/wardens• Patient/carer

Source of Referrals
0
50
100
150
200
250
300
Apr-10 May-10 Jun-10 Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11
OtherGPPrimecare Hospice Consultant HospiceSRHSpecialist Nurse Marie CuriePatient / CarerDN

Current Activity
• Average - 43 new patients per month
• Average - 100 patients per month on caseload
• Average - 90% of patients on OOH team caseload die at home 93% achieve PPC (where hospice is nominated)
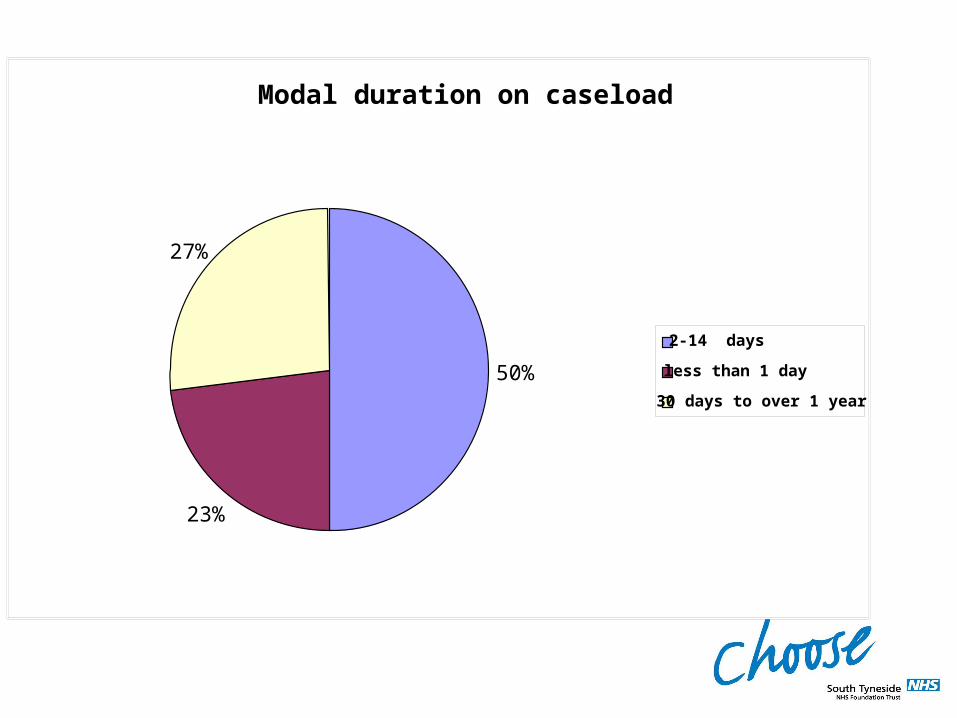
Modal duration on caseload
50%
23%
27%
2-14 days
less than 1 day
30 days to over 1 year

0
200
400
600
800
1000
1200
1400
1600
1800
2003-04 2004-05 2005-06 2006-07 2007-08 2008-09 2009-10
Crisis visits
Planned visits
TelephoneAdvice/ Support
Type of Visit

Reason For Referral(April 2010 - January 2011)
362
605
518
188
1563
185
276
186
Emotional support
Controlled Drugs
Other Medication
General Nursing Care
Enema
Catheter Care
Last Offices
LCP supportive visit
Other

0
50
100
150
200
250
300
350
400
450
2003-04
2004-05
2005-06
2006-07
2007-08
2008-09
2009-10
2010-11
Deaths athomeDeaths inhospitalDeaths inhospice
Place of Death

The QIPP Agenda

Quality99.3% of Crisis Visits enabled the patient to remain at home
(April 1st 2011-January 31st 2012)

90%
10%
QualityCrisis Visits Seen Within 1 hour
(April 2010-March2011)

94%
6%
QualityPlanned visits seen within 30 minutes of appointment
(April 2010-March 2011)

Quality• Patient and satisfaction survey reports• Compliment/ letters/ cards• Patient and carer stories (independently
audited)• Close MDT patient centred working
relationships• Team - low sickness rates
- low staff turnover- ease of recruitment
• 1 complaint in over 14 years• Excellent working relationships with deputising
doctor service• Excellent working relationships with GPs and
DNs

Innovation
• 1998-First dedicated OOH Palliative Care Service in UK• 1999-National Beacon Award• 2000-cited in National cancer Plan as model of excellence• 2001-Established small committed consortium of pharmacists to
access drugs OOH • 2003-commenced verification of death by nurse in the
community• 2004-developed and commenced use of PGDs for PC pts in
community• 2008-Marie Curie, Delivering Choice Programme• 2009-won Nursing Standard ‘Innovation in Palliative Care award’• 2011-outcome of Marie Curie Delivering Choice project and
workforce development• 2012-Won tender to develop OOH service for South Tyneside
and Gateshead.

Productivity
Continuously Increasing numbers of:• patient’s dying at home• averted admissions• referrals• rapid discharges• patients achieving PPC• patient’s dying on LCP• Increased utilisation of service for all life limiting
diseases

Prevention of:
• unnecessary futile admissions• re-admission• protracted length of stay in hospital• waste of NHS resources:
- reduced ambulance call out,- reduced deputising doctor call out
(use of PGD and verification of death)• Complaints

The Future
• Capacity issues and investment• Preventing avoidable admissions• Weekends and BH daytime• 24/7 model?• Offering patients/carers real
choice – PPC• The wider needs of the locality• Equity of access to services• Saving money for NHS
Win, Win!
The Future
‘Invest to Save’
Sunderland has 14 years experience to demonstrate that our model of OOH PC:
• keeps dying patients at home• vastly reduces stress for patients and carers• prevents avoidable and largely futile
hospital admissions.
In terms of prevention of admission and facilitation of rapid discharge for every
£1spent, £1.65 can be saved

JULIE NEWBY
Palliative Care Team MangerOut of Hours
St. Benedict’s HospiceSunderland
0191 541005507876654083
Thank you

North of England Cancer NetworkGP Palliative Care Register Project
Lesley Davie, Project Manager
Your register, their palliative care

Rationale• Wide variation in the use of palliative care registers
and in advance care planning• Poorer co-ordination of care for people at the end of
their life.• National Primary Care Audit in End of Life Care
(2009):• Patients on a palliative care register receive better
co-ordinated care• Earlier identification of patients (cancer and non
cancer) will lead to improved end of life care
Project Baseline Data Findings
• 59% of practices had 20 or less patients on their register
• 42% added patients to the register 12 months before death
• 62% of GPs and 18% of administrative staff were responsible for adding patients onto the register
• 64% discuss palliative care patients monthly

Resources
Help and guidance is now available:• The ‘How to’ Guide will give primary care
teams help to achieve a gold standard of palliative care planning
• The Palliative care template for EMIS LV and SystmOne practice systems

Finally,
• We need your support to implement the ‘How to’ Guide and templates in as many GP practices as possible
• And now ‘Deciding Right’

Deciding Right
Sarah RushbrookeNetwork Quality & Patient Safety Director
North of England Cancer NetworkMarch 2012

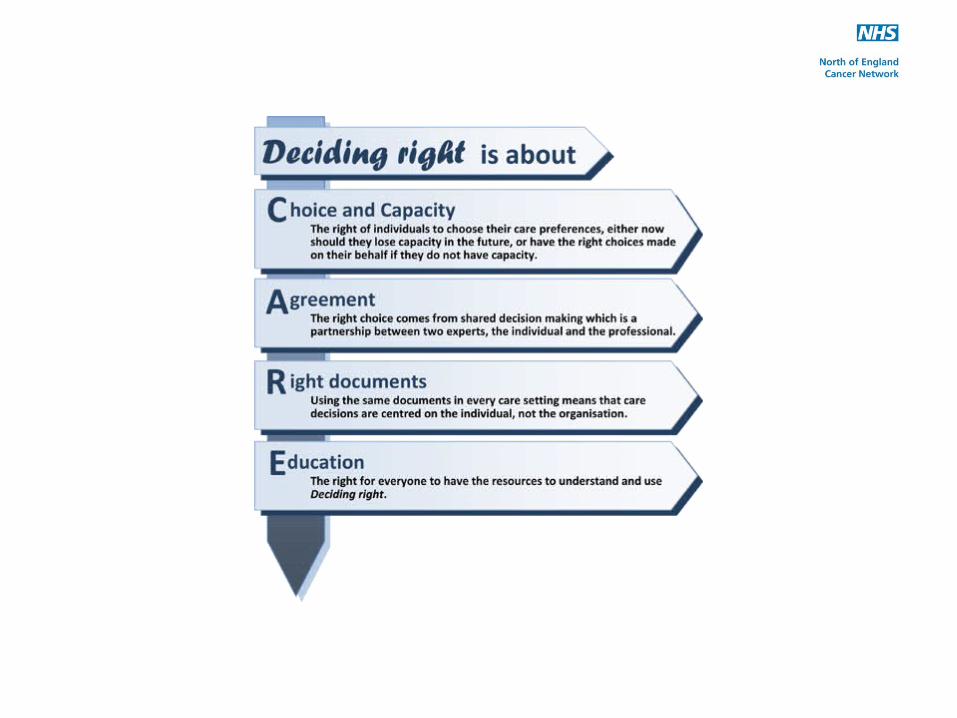
‘Deciding Right’
Deciding right - a new north east initiative integrated approach for making care decisions in advance with children, young people and adults

The challenges of planning future care
• Changing clinical decisions from organisational policy-driven decisions to patient-centred shared decisions
• Embedding existing legislation and guidelines into clinical practice, e.g. the Mental Capacity Act
• Creating region-wide documentation for use in any setting
• Ensuring clarity, flexibility and choice• Understanding the limitations of advance care planning• Enabling policy dissemination

Advance Care Planning
• Widespread confusion over definition• Now firmly linked to the Mental Capacity Act• Not the same as general care planning• Can only be made by people with capacity• Only applies to a future loss of capacity• Only three written outcomes:
- advance statement- Advance Decisions to Refuse Treatment (ADRT)- Lasting Power of Attorney
Advance Decision to Refuse Treatment (ADRT)Regional ADRT policy
• Governed by the Mental Capacity Act• Can only be made by someone with capacity for
that decision• Only active when capacity is lost• Can be verbal, but must be written if refusing life-
sustaining treatment• If valid and applicable, an ADRT is legally binding• Not the answer to immediate care decisions• A regional ADRT form now exists

Cardiopulmonary resuscitation (CPR) decisions
• Based on 2007 BMA/RC/RCN Joint Statement• Identifies the triggers for making CPR decisions• Creates a single DNACPR form for use in all
settings• Recognises the Liverpool Care Pathway for the
Dying Patient document as a DNACPR order• Introduces Emergency Health Care Plans as an
important adjunct in specialist care settings

The next steps• Chief Executive Sign up has been agreed by Trust & PCTs. All
other organisations endorse the principles.• Training issues and how do we overcome these – local
champions, agree a training strategy• Launch to the profession - Mid March• Launch to the public - Spring• How to make available to all providers of care – who will
host documentation/forms• What is the role of IT services & systems?• How do we ensure that all people on the LCP
are DNACPR?• Cit and Network SPC group to agree a way forward.
Thank You
Deciding right is now online on www.theclinicalnetwork.org
http://www.theclinicalnetwork.org/end-of-life-care---the-clinical-network/decidingright

End of Life CareFuture Priorities
ByDr. H. Choi
Vision Our vision is to achieve ‘better health for Sunderland’ and was agreed by the Executive Committee in November 2011. Our vision is supported by three high level goals which
describe the changes we aim to make in the medium to
longer term, which are to:
Improve the health and well being of all local
people; to live longer, with a better quality of life
and a reduction in health inequalities across the
locality;
Integrate services better across health and
social care;
Underpinned by more effective clinical decision
making.
We will do this by working closely with patients, the public, carers, providers and partners.
Core Values
We have identified a set of core values which will shape
and underpin all of the work we undertake to deliver our
vision, including all aspects of decision making and
governance, as illustrated on the following chart:
Open and
honest
Responsive
Empowering
Integrity Inclusive
Better Health for all the people in
Sunderland

Future Priorities
• Effective Communication• Empowering patients and carers• Integrate Health and Social Care• Effective Team Working• Reduced Clinical Variation• Reduced Unplanned Admission• Training and Education

How people died remains in the memory of those who live on
by Dame Cicely Saunders

Thank you








![INTEGRATED PROJECT DELIVERY AGREEMENT · 1816211.10 [PROJECT NAME] INTEGRATED PROJECT DELIVERY AGREEMENT [Profit Deferred Until Final Completion]](https://img.dokumen.tips/doc/110x75/5f7b1be6148ce06db6337b9f/integrated-project-delivery-agreement-181621110-project-name-integrated-project.jpg)




















