Embed Size (px)
Citation preview

Employee Benefits Summary - NY
INSURANCE & OTHER BENEFITS Dental Insurance: Eligible employees may enroll in a dental insurance plan. Individual and family coverage is available. A portion of the premium is paid by Human Technologies. Disability Insurance (Short Term – NYS): Employees receive New York State statutory temporary protection for a non-work related injury or illness. Disability (Supplemental): Eligible employees may enroll and purchase a disability plan for themselves in addition to the plan that Human Technologies pays. Flexible Spending Account (FSA): Eligible employees may participate in a flexible spending account. Health Insurance: Eligible employees may enroll in a health insurance plan. Individual, family and plus one coverage is available. A portion of the premium is paid by Human Technologies. Health Reimbursement Account (HRA): For employees who enroll in a high deductible health insurance plan Human Technologies will contribute into an HRA. Life Insurance (Group): Eligible employees receive group life insurance at a rate of 1 ½ times their salary. 100% paid by Human Technologies. Life Insurance (Supplemental): Eligible employees may enroll and purchase a life insurance plan for themselves and family members. Retirement Plan: Employees may participate in a retirement program within the first quarter of employment. Employees 20 years of age or older who work at least 1000 hours in their first year of employment and have completed one year of service are eligible for the corporation’s retirement plan. Human Technologies will contribute up to 4% of an individual’s annual salary. Employees working on a Service Contract have a plan that is structured different and will be discussed upon hire. Section 125 Plan: Flexible Benefits Plan: Employee premiums associated with Group Health Insurance and/or Dental Care Insurance and 401k contributions are deducted from wages before taxes are computed on earnings. Unemployment Compensation: Employees may be eligible to receive a portion of their income if the employee becomes unemployed. Benefit eligibility is determined by the Department of Labor. Vision Insurance: Eligible employees may enroll and purchase a vision insurance plan. Individual and family coverage is available. Workers’ Compensation: Employees that incur a work related injured or illness may have a portion of their income protected by the corporation’s Worker Compensation Insurance and medical bills covered.

Rev 2016-1
LEAVES OF ABSENCE Bereavement Leave: Employees are granted up to 3 paid days off. Family and Medical Leave Act (FMLA): Eligible employees may be granted up to 12 weeks of unpaid family leave during a 12 month period. Additionally, eligible employees may be granted up to 26 weeks of unpaid leave for specified reasons related to certain military deployments. Jury Duty: Employees are granted up to 10 days off annually with pay to serve as a juror. Military Leave: Eligible employees are granted leaves of absence in accordance with federal and state law and may be eligible for paid leave. Volunteer First Responders Leave: Employees who are volunteer emergency responders may be eligible for a leave of absence during a federal or NY State declared emergency in compliance with NYS Labor Law.
HOLIDAYS AND PAID TIME OFF (PTO) Holidays—11 paid holidays PTO*—FT Employees receive paid time off on an accrual based on tenure:
Employment: PTO
Date of hire – 12 months (0 – 1 year) 11 days
13-36 months (1 -3 years) 14 days 37-72 months (3 – 6 years) 19 days
73-179 months (6 – 15 years) 24 days
180 & more (15+ years) 30 days *Refer to the Employee Handbook for accrual chart for part time and PMG direct labor employees.
Leadership Team: PTO – 20 day accrual upon hire
Long Term Disability 100% paid.
Contact Human Resources for specific information on these benefits.

The information in this Benefits Overview is presented for illustrative purposes and is based on information provided by the employer. In case of discrepancy between the Benefits Overview and the actual plan documents, the actual plan documents will prevail.
HEALTH/MEDICAL Note: this is intended only as a general overview of health/medical insurance. See the “Understanding Your…” section for the specifics around the plan(s) offered to you.
Health/Medical Insurance
A contract that requires your health insurer to pay some or all of your health care costs in exchange for a premium.
Making a thoughtful decision and picking the best health plan for your situation is important for you and your family.
Following are some of the basic reasons you should consider obtaining health coverage.
FINANCIAL PROTECTION
You don’t usually plan for medical care; if you or a family member gets sick or hurt, you likely didn’t see it coming. Big
expenses—such as treatment for a broken leg or a hospitalization for a serious illness—can use up your paychecks in a
hurry. For example, a fractured leg that requires surgery could cost up to $20,000 or more if you don’t have insurance.
An X-ray alone can cost several hundred dollars.
Health insurance will typically cover some of those expenses, making it less financially traumatic. Owing only a portion of
the full amount (i.e. deductible amount and/or copays) is much easier on your bank account than having to pay the full
regular fees.
GET THE CARE YOU NEED
If you don’t have insurance and can’t afford to pay out-of-pocket, you might have to skip or skimp on medical care for
yourself or a family member. Having health insurance ensures you can get the care you and your family need. In
addition, health insurance helps you pay for routine and preventive health care to keep you healthy in the first place.
Health insurance covers many preventive services (such as health screenings or immunizations) without you having to
pay out-of-pocket. Preventive care is intended to prevent or catch diseases and other health problems before they
become serious.
INDIVIDUAL MANDATE PENALTY
A final incentive to get health insurance coverage is the Affordable Care Act’s (ACA) individual mandate. The ACA
requires most individuals to obtain health insurance. As of 2014, if you don’t have health insurance, you will be subject
to a penalty fee. Visit www.healthcare.gov/what-if-i-dont-have-health-coverage for more information on obtaining
insurance or paying a penalty.
4

The information in this Benefits Overview is presented for illustrative purposes and is based on information provided by the employer. In case of discrepancy between the Benefits Overview and the actual plan documents, the actual plan documents will prevail.
5

The information in this Benefits Overview is presented for illustrative purposes and is based on information provided by the employer. In case of discrepancy between the Benefits Overview and the actual plan documents, the actual plan documents will prevail.
6

The information in this Benefits Overview is presented for illustrative purposes and is based on information provided by the employer. In case of discrepancy between the Benefits Overview and the actual plan documents, the actual plan documents will prevail.
Health Plan Options
Option 1: SimplyBlue 25-1,000
Excellus Blue Cross Blue Shield
Option 2: Signature Deductible 3 ($2,600/$5,200)
Excellus Blue Cross Blue Shield
Option 3: Signature Deductible 3($5,500/$11,000)
Excellus Blue Cross Blue Shield
Note: Plan information can be found on the following pages.
Cost
Plan #1 Name: SimplyBlue 25-1,000
Monthly Plan Cost ($)
Monthly Employee Cost Share ($)
Monthly Employer Cost
Employee Cost Per Pay Period
Employer Cost Per Pay Period
Single $788.74 $217.25 $571.49 $100.27 $263.76 Employee + Spouse $1,641.69 $916.69 $725.00 $423.09 $334.62 Family $2,264.68 $1,539.68 $725.00 $710.62 $334.62
Plan #2 Name: Signature Deductible 3 ($2,600/$5,200)
Monthly Plan Cost ($)
Monthly Employee Cost Share ($)
Monthly Employer Cost
Employee Cost Per Pay Period
Employer Cost Per Pay Period
Single $625.29 $58.03 $567.26 $26.78 $261.81 Employee + Spouse $1,301.45 $576.45 $725.00 $266.05 $334.62 Family $1,795.38 $1,070.38 $725.00 $494.02 $334.62
Plan #3 Name: Signature Deductible 3 ($5,500/$11,000)
Monthly Plan Cost ($)
Monthly Employee Cost Share ($)
Monthly Employer Cost
Employee Cost Per Pay Period
Employer Cost Per Pay Period
Single $509.37 $37.91 $471.46 $17.50 $217.60 Employee + Spouse $1,060.22 $335.22 $725.00 $154.72 $334.62 Family $1,462.55 $737.55 $725.00 $340.41 $334.62
UNDERSTANDING YOUR HEALTH/MEDICAL BENEFITS
7
These rates are for non-prevailing wage employees. Employees who work prevailing wage contract(s) that earn health and welfare have premiums calculated based on their contract(s).

SimplyBlue Hybrid$5/$35/$70, $0 Gen For Kids
Benefit Time Period: 01/01/2017 - 12/31/2017
Human Technologies Corp
904789-2 11/14/2016 01:25:07
General Information
Cost Sharing Expenses
Benefit Name In Network Out of Network Limits and Additional Information
Deductible - Single $1,000 $1,000One deductible for in and out of network
combined.
Deductible - Family $3,000 $3,000Each individual does not exceed the single
deductible.
Coinsurance 20% 40%
Annual Out of Pocket Maximum - Single $4,200 $4,200
Out-of-pocket maximums accumulate
coinsurance, copays and the deductible. Out-of-
pocket maximums exclude balances over
allowable expense and non-covered services.
Annual Out of Pocket Maximum - Family $12,600 $12,600
Out-of-pocket maximums accumulate
coinsurance, copays and the deductible. Out-of-
pocket maximums exclude balances over
allowable expense and non-covered services.
Annual Out of Pocket Maximum - Per Person
Cap$4,200 $4,200
The Out-of-Pocket Maximum Per Person Cap
includes deductible, coinsurance, copays and
prescription drugs. If a member under a family
contract meets the Out-Of-Pocket Maximum Per
Person Cap amount, the individual will no longer
pay for covered services and claims will be paid
at 100% of the allowable amount by the Health
Plan for the remainder of the plan year. The
remaining annual out-of-pocket maximum still
needs to be met by any combination of family
members on the contract before claims are paid
at 100% for the whole family.
Office Visit Cost Shares
Benefit Name In Network Out of Network Limits and Additional Information
Cost Share - Primary Care $25 Copayment40% Coinsurance
Subject to Deductible
$0 copayment for dependents to age 19 on all
In-Network PCP office visits.
Cost Share - Specialist $40 Copayment40% Coinsurance
Subject to Deductible
Plan Limits
Benefit Name In Network Out of Network Limits and Additional Information
Plan/Calendar Year Calendar Year Benefits
Diabetic Preauthorization and Step Therapy Yes
Who is Covered
Benefit Name In Network Out of Network Limits and Additional Information
Domestic Partner Coverage Covered
Inpatient Services
SimplyBlue 25-1,000
8

904789-2 11/14/2016 01:25:07
Inpatient Facility
Benefit Name In Network Out of Network Limits and Additional Information
Inpatient Hospital Services20% Coinsurance
Subject to Deductible
40% Coinsurance
Subject to Deductible
Mental Health Care20% Coinsurance
Subject to Deductible
40% Coinsurance
Subject to Deductible
Substance Use Detoxification20% Coinsurance
Subject to Deductible
40% Coinsurance
Subject to Deductible
Skilled Nursing Facility20% Coinsurance
Subject to Deductible
40% Coinsurance
Subject to Deductible
45 Days per year
Limits are combined INN and OON.
Physical Rehabilitation20% Coinsurance
Subject to Deductible
40% Coinsurance
Subject to Deductible
60 Days per year
Limits are combined INN and OON.
Maternity Care20% Coinsurance
Subject to Deductible
40% Coinsurance
Subject to Deductible
Inpatient Professional Services
Benefit Name In Network Out of Network Limits and Additional Information
Inpatient Hospital Surgery
PCP/Specialist - 20%
Coinsurance
Subject to Deductible
40% Coinsurance
Subject to Deductible
Anesthesia
PCP/Specialist - 20%
Coinsurance
Subject to Deductible
20% Coinsurance
Subject to Deductible
Includes anesthesia rendered for Inpatient,
Outpatient, Office Visit, and Maternity services.
Anesthesia does not require a preauth or
referral.
Outpatient Facility Services
Outpatient Facility Services
Benefit Name In Network Out of Network Limits and Additional Information
SurgiCenters and Freestanding Ambulatory
Centers Surgical Care
20% Coinsurance
Subject to Deductible
40% Coinsurance
Subject to Deductible
Diagnostic X-ray $40 Copayment40% Coinsurance
Subject to Deductible
Diagnostic Laboratory and Pathology Covered in Full40% Coinsurance
Subject to Deductible
Radiation Therapy $40 Copayment40% Coinsurance
Subject to Deductible
Chemotherapy $25 Copayment40% Coinsurance
Subject to Deductible
Infusion Therapy Inclusive of Primary Service Inclusive of Primary ServiceIs inclusive in the Home Care benefit and not
covered as a separate benefit.
Dialysis Covered in Full40% Coinsurance
Subject to Deductible
Mental Health Care $40 Copayment40% Coinsurance
Subject to DeductibleIncludes Partial Hospitalization
Substance Use Care $40 Copayment40% Coinsurance
Subject to DeductibleIncludes Partial Hospitalization
Home and Hospice Care
Home Care
Benefit Name In Network Out of Network Limits and Additional Information
Home Care Covered in Full25% Coinsurance
Subject to $50 Deductible
40 Visits per year
Limits are combined INN and OON.
Hospice Care
SimplyBlue 25-1,000
9

904789-2 11/14/2016 01:25:07
Benefit Name In Network Out of Network Limits and Additional Information
Hospice Care Inpatient Covered in Full40% Coinsurance
Subject to Deductible
Outpatient and Office Professional Services
Professional Services
Benefit Name In Network Out of Network Limits and Additional Information
Office Surgery
PCP - $25 Copayment
Specialist - $40 Copayment
$0 PCP Copay for members
to age 19.
40% Coinsurance
Subject to Deductible
Diagnostic X-rayPCP/Specialist - $40
Copayment
40% Coinsurance
Subject to Deductible
Diagnostic Laboratory and PathologyPCP/Specialist - Covered in
Full
40% Coinsurance
Subject to Deductible
Radiation TherapyPCP/Specialist - $40
Copayment
40% Coinsurance
Subject to Deductible
ChemotherapyPCP/Specialist - $25
Copayment
40% Coinsurance
Subject to Deductible
Infusion TherapyPCP/Specialist - Inclusive of
Primary ServiceInclusive of Primary Service
Is inclusive in the Home Care benefit and not
covered as a separate benefit.
DialysisPCP/Specialist - Covered in
Full
40% Coinsurance
Subject to Deductible
Mental Health CarePCP/Specialist - $40
Copayment
40% Coinsurance
Subject to Deductible
Maternity Care
PCP/Specialist - 20%
Coinsurance
Subject to Deductible
40% Coinsurance
Subject to Deductible
TeleMedicine ProgramPCP/Specialist - $10
CopaymentNot Covered
Covers online internet consultations between
the member and the providers who participate in
our telemedicine program for medical conditions
that are not an emergency condition.
Chiropractic CarePCP/Specialist - $40
Copayment
40% Coinsurance
Subject to Deductible
Allergy Testing
PCP - $25 Copayment
Specialist - $40 Copayment
$0 PCP Copay for members
to age 19.
40% Coinsurance
Subject to Deductible
Allergy Testing includes injections and scratch
and prick tests.
Allergy Treatment Including Serum
PCP - $25 Copayment
Specialist - $40 Copayment
$0 PCP Copay for members
to age 19.
40% Coinsurance
Subject to Deductible
Includes desensitization treatments (injections &
serums).
Hearing Evaluations RoutinePCP/Specialist - $40
Copayment
40% Coinsurance
Subject to Deductible
1 Exam Per Year
Limits are combined INN and OON.
SimplyBlue 25-1,000
10

904789-2 11/14/2016 01:25:07
Rehab and Habilitation
Outpatient Facility
Benefit Name In Network Out of Network Limits and Additional Information
Physical Rehabilitation $40 Copayment40% Coinsurance
Subject to Deductible
45 Visits per year
Includes aggregate of visits for INN and OON
and professional and facility covered services
for physical, speech, and occupational therapy.
Occupational Rehabilitation $40 Copayment40% Coinsurance
Subject to Deductible45 Visits per year
Speech Rehabilitation $40 Copayment40% Coinsurance
Subject to Deductible45 Visits per year
Outpatient Professional Services
Benefit Name In Network Out of Network Limits and Additional Information
Physical RehabilitationPCP/Specialist - $40
Copayment
40% Coinsurance
Subject to Deductible
45 Visits per year
Includes aggregate of visits for INN and OON
and professional and facility covered services
for physical, speech, and occupational therapy.
Occupational RehabilitationPCP/Specialist - $40
Copayment
40% Coinsurance
Subject to Deductible45 Visits per year
Speech RehabilitationPCP/Specialist - $40
Copayment
40% Coinsurance
Subject to Deductible45 Visits per year
Preventive Services
Preventive Professional Services Meeting Federal Guidelines*
Benefit Name In Network Out of Network Limits and Additional Information
Adult Physical ExaminationPCP/Specialist - Covered in
Full
40% Coinsurance
Subject to Deductible1 Exam per year
Adult ImmunizationsPCP/Specialist - Covered in
Full
40% Coinsurance
Subject to Deductible
Well Child Visits and ImmunizationsPCP/Specialist - Covered in
FullCovered in Full
Routine GYN VisitPCP/Specialist - Covered in
Full
40% Coinsurance
Subject to Deductible
Pre/Post-Natal CarePCP/Specialist - Covered in
Full
40% Coinsurance
Subject to Deductible
Mammography Screening ProfessionalPCP/Specialist - Covered in
Full
40% Coinsurance
Subject to Deductible
Colonoscopy Screening ProfessionalPCP/Specialist - Covered in
Full
40% Coinsurance
Subject to Deductible
Bone Density Screening ProfessionalPCP/Specialist - Covered in
Full
40% Coinsurance
Subject to Deductible
Preventive Facility Services Meeting Federal Guidelines*
Benefit Name In Network Out of Network Limits and Additional Information
Cervical Cytology Preventative Covered in Full40% Coinsurance
Subject to Deductible
Mammography Screening Facility Covered in Full40% Coinsurance
Subject to Deductible
Colonoscopy Screening Facility Covered in Full40% Coinsurance
Subject to Deductible
Bone Density Screening Facility Covered in Full40% Coinsurance
Subject to Deductible
SimplyBlue 25-1,000
11
904789-2 11/14/2016 01:25:07
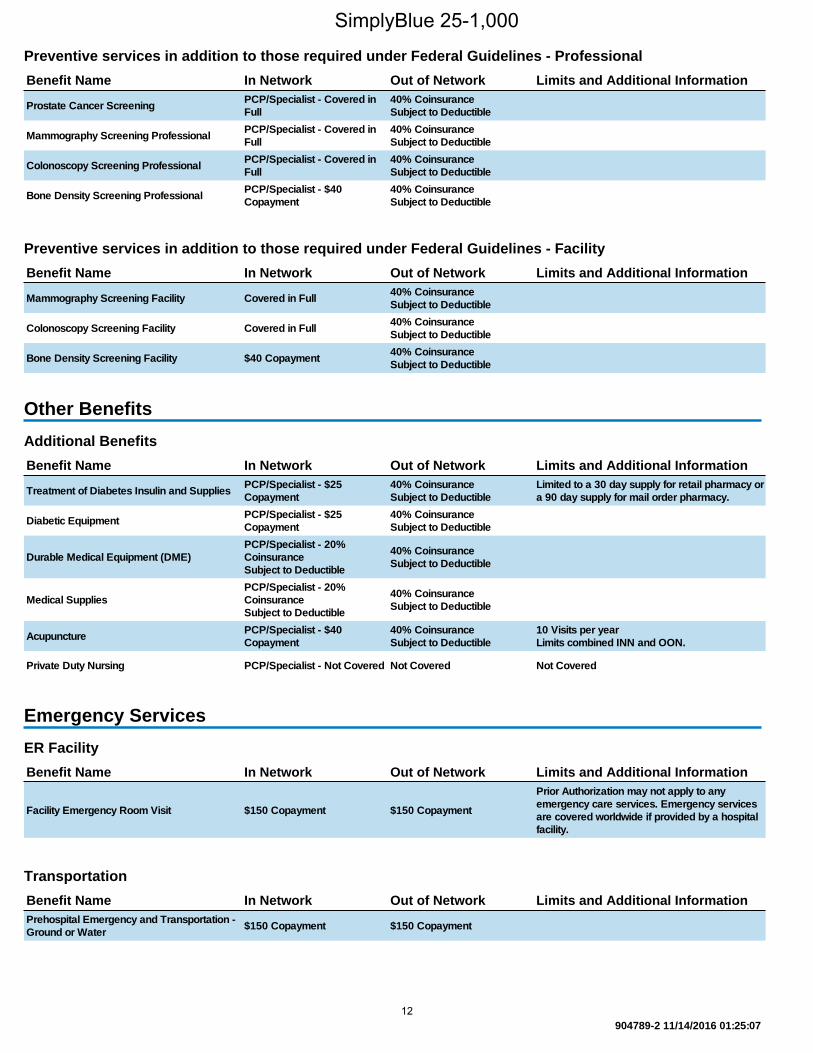
Preventive services in addition to those required under Federal Guidelines - Professional
Benefit Name In Network Out of Network Limits and Additional Information
Prostate Cancer ScreeningPCP/Specialist - Covered in
Full
40% Coinsurance
Subject to Deductible
Mammography Screening ProfessionalPCP/Specialist - Covered in
Full
40% Coinsurance
Subject to Deductible
Colonoscopy Screening ProfessionalPCP/Specialist - Covered in
Full
40% Coinsurance
Subject to Deductible
Bone Density Screening ProfessionalPCP/Specialist - $40
Copayment
40% Coinsurance
Subject to Deductible
Preventive services in addition to those required under Federal Guidelines - Facility
Benefit Name In Network Out of Network Limits and Additional Information
Mammography Screening Facility Covered in Full40% Coinsurance
Subject to Deductible
Colonoscopy Screening Facility Covered in Full40% Coinsurance
Subject to Deductible
Bone Density Screening Facility $40 Copayment40% Coinsurance
Subject to Deductible
Other Benefits
Additional Benefits
Benefit Name In Network Out of Network Limits and Additional Information
Treatment of Diabetes Insulin and SuppliesPCP/Specialist - $25
Copayment
40% Coinsurance
Subject to Deductible
Limited to a 30 day supply for retail pharmacy or
a 90 day supply for mail order pharmacy.
Diabetic EquipmentPCP/Specialist - $25
Copayment
40% Coinsurance
Subject to Deductible
Durable Medical Equipment (DME)
PCP/Specialist - 20%
Coinsurance
Subject to Deductible
40% Coinsurance
Subject to Deductible
Medical Supplies
PCP/Specialist - 20%
Coinsurance
Subject to Deductible
40% Coinsurance
Subject to Deductible
AcupuncturePCP/Specialist - $40
Copayment
40% Coinsurance
Subject to Deductible
10 Visits per year
Limits combined INN and OON.
Private Duty Nursing PCP/Specialist - Not Covered Not Covered Not Covered
Emergency Services
ER Facility
Benefit Name In Network Out of Network Limits and Additional Information
Facility Emergency Room Visit $150 Copayment $150 Copayment
Prior Authorization may not apply to any
emergency care services. Emergency services
are covered worldwide if provided by a hospital
facility.
Transportation
Benefit Name In Network Out of Network Limits and Additional Information
Prehospital Emergency and Transportation -
Ground or Water$150 Copayment $150 Copayment
SimplyBlue 25-1,000
12

904789-2 11/14/2016 01:25:07
Urgent Care
Benefit Name In Network Out of Network Limits and Additional Information
Urgent Care Center Facility Visit $40 Copayment40% Coinsurance
Subject to Deductible
Ancillary Benefits
Vision
Benefit Name In Network Out of Network Limits and Additional Information
Adult Eye Exams - Routine $40 Copayment40% Coinsurance
Subject to Deductible
1 Exam per year
Limits are combined INN and OON.
Adult Eyewear - Routine Covered Covered$60 Reimbursement per year
Includes Frames/Lenses or Contact Lenses
Pediatric Eye Exams - Routine $40 Copayment40% Coinsurance
Subject to Deductible
1 Exam per year
Limits are combined INN and OON.
Pediatric Eyewear - Routine Covered Covered$60 Reimbursement per year
Includes Frames/Lenses or Contact Lenses
Rx Benefits
Rx Plan
Benefit Name In Network Out of Network Limits and Additional Information
Rx Plan $5/$35/$70, $0 Gen For Kids
Rx Benefits
Benefit Name In Network Out of Network Limits and Additional Information
Days Supply Per Retail Order 30
Days Supply Per Mail Order 90
Copays Per Mail Order Supply 2
This document is not a contract. It is only intended to highlight the coverage of this program. Benefits are determined by the
terms of the contract. Any inconsistencies between this document and the contract shall be resolved in favor of the contract in
effect at the time services are rendered. All benefits are subject to medical necessity. All day and visit limits are combined
limits for both in and out of network benefits.
* For non-grandfathered groups, Preventive Services coverage required by the Patient Protection and Affordable Care Act are
not quoted herein. Please refer to the United States Preventive Services Task Force list of items and services rated "A" or "B"
that are covered pursuant to the Patient Protection and Affordable Care Act requirements.
SimplyBlue 25-1,000
13

Excellus BluePPO Signature Deduct 3$5/$35/$70, $0 gen for kids Integrated Rx, No Ded Prev Rx
Benefit Time Period: 01/01/2017 - 12/31/2017
HUMAN TECHNOLOGIES CORP
901647-1 09/16/2016 09:10:33
General Information
Cost Sharing Expenses
Benefit Name In Network Out of Network Limits and Additional Information
Deductible - Single $2,600 $5,200
Deductible - Family $5,200 $10,400
Coinsurance 0% 10%
Annual Out of Pocket Maximum - Single $5,500 $11,000
Out-of-pocket maximums accumulate
coinsurance, copays and the deductible. Out-of-
pocket maximums exclude balances over
allowable expense and non-covered services.
Annual Out of Pocket Maximum - Family $11,000 $22,000
Out-of-pocket maximums accumulate
coinsurance, copays and the deductible. Out-of-
pocket maximums exclude balances over
allowable expense and non-covered services.
Annual Out of Pocket Maximum - Per Person
Cap$6,550 $22,000
The Out-of-Pocket Maximum Per Person Cap
includes deductible, coinsurance, copays and
prescription drugs. If a member under a family
contract meets the Out-Of-Pocket Maximum Per
Person Cap amount, the individual will no longer
pay for covered services and claims will be paid
at 100% of the allowable amount by the Health
Plan for the remainder of the plan year. The
remaining annual out-of-pocket maximum still
needs to be met by any combination of family
members on the contract before claims are paid
at 100% for the whole family.
Office Visit Cost Shares
Benefit Name In Network Out of Network Limits and Additional Information
Cost Share - Primary Care0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Cost Share - Specialist0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Plan Limits
Benefit Name In Network Out of Network Limits and Additional Information
Plan/Calendar Year Plan Year Benefits
Diabetic Preauthorization and Step Therapy Yes
Who is Covered
Benefit Name In Network Out of Network Limits and Additional Information
Domestic Partner Coverage Covered
Signature Deductible 3 ($2,600/$5,200)
14
901647-1 09/16/2016 09:10:33
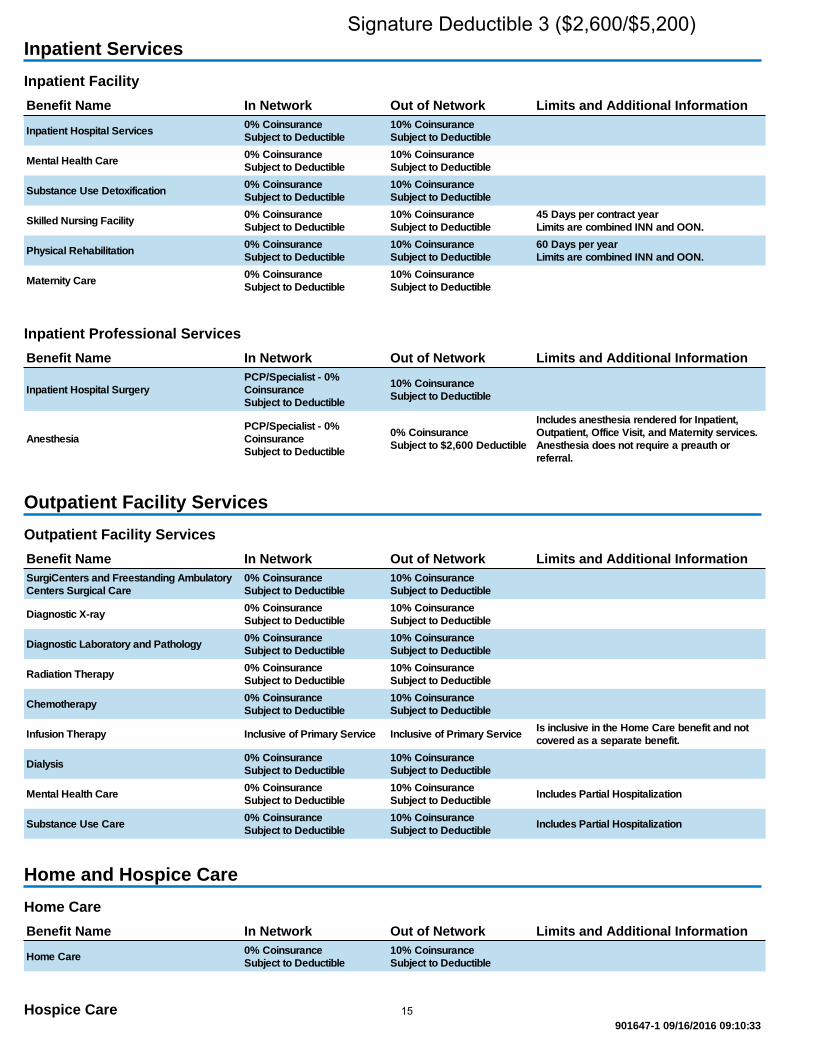
Inpatient Services
Inpatient Facility
Benefit Name In Network Out of Network Limits and Additional Information
Inpatient Hospital Services0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Mental Health Care0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Substance Use Detoxification0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Skilled Nursing Facility0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
45 Days per contract year
Limits are combined INN and OON.
Physical Rehabilitation0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
60 Days per year
Limits are combined INN and OON.
Maternity Care0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Inpatient Professional Services
Benefit Name In Network Out of Network Limits and Additional Information
Inpatient Hospital Surgery
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Anesthesia
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
0% Coinsurance
Subject to $2,600 Deductible
Includes anesthesia rendered for Inpatient,
Outpatient, Office Visit, and Maternity services.
Anesthesia does not require a preauth or
referral.
Outpatient Facility Services
Outpatient Facility Services
Benefit Name In Network Out of Network Limits and Additional Information
SurgiCenters and Freestanding Ambulatory
Centers Surgical Care
0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Diagnostic X-ray0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Diagnostic Laboratory and Pathology0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Radiation Therapy0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Chemotherapy0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Infusion Therapy Inclusive of Primary Service Inclusive of Primary ServiceIs inclusive in the Home Care benefit and not
covered as a separate benefit.
Dialysis0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Mental Health Care0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to DeductibleIncludes Partial Hospitalization
Substance Use Care0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to DeductibleIncludes Partial Hospitalization
Home and Hospice Care
Home Care
Benefit Name In Network Out of Network Limits and Additional Information
Home Care0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Hospice Care
Signature Deductible 3 ($2,600/$5,200)
15
901647-1 09/16/2016 09:10:33
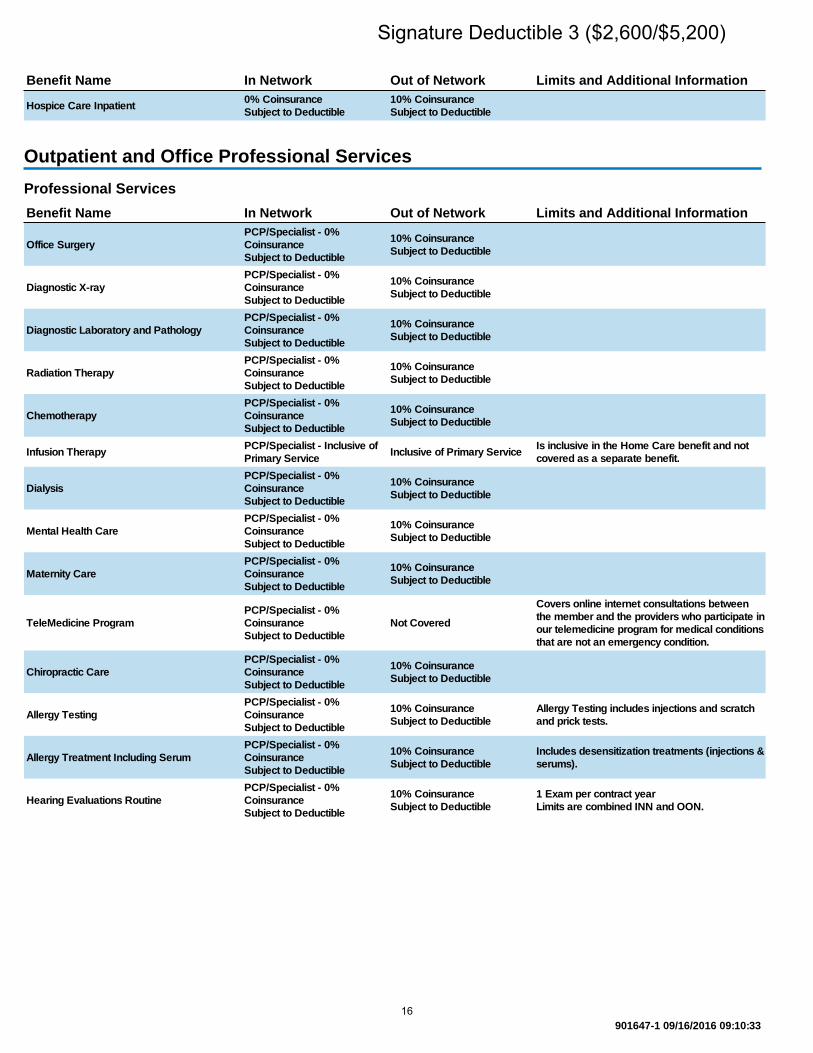
Benefit Name In Network Out of Network Limits and Additional Information
Hospice Care Inpatient0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Outpatient and Office Professional Services
Professional Services
Benefit Name In Network Out of Network Limits and Additional Information
Office Surgery
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Diagnostic X-ray
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Diagnostic Laboratory and Pathology
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Radiation Therapy
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Chemotherapy
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Infusion TherapyPCP/Specialist - Inclusive of
Primary ServiceInclusive of Primary Service
Is inclusive in the Home Care benefit and not
covered as a separate benefit.
Dialysis
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Mental Health Care
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Maternity Care
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
TeleMedicine Program
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
Not Covered
Covers online internet consultations between
the member and the providers who participate in
our telemedicine program for medical conditions
that are not an emergency condition.
Chiropractic Care
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Allergy Testing
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Allergy Testing includes injections and scratch
and prick tests.
Allergy Treatment Including Serum
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Includes desensitization treatments (injections &
serums).
Hearing Evaluations Routine
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
1 Exam per contract year
Limits are combined INN and OON.
Signature Deductible 3 ($2,600/$5,200)
16
901647-1 09/16/2016 09:10:33
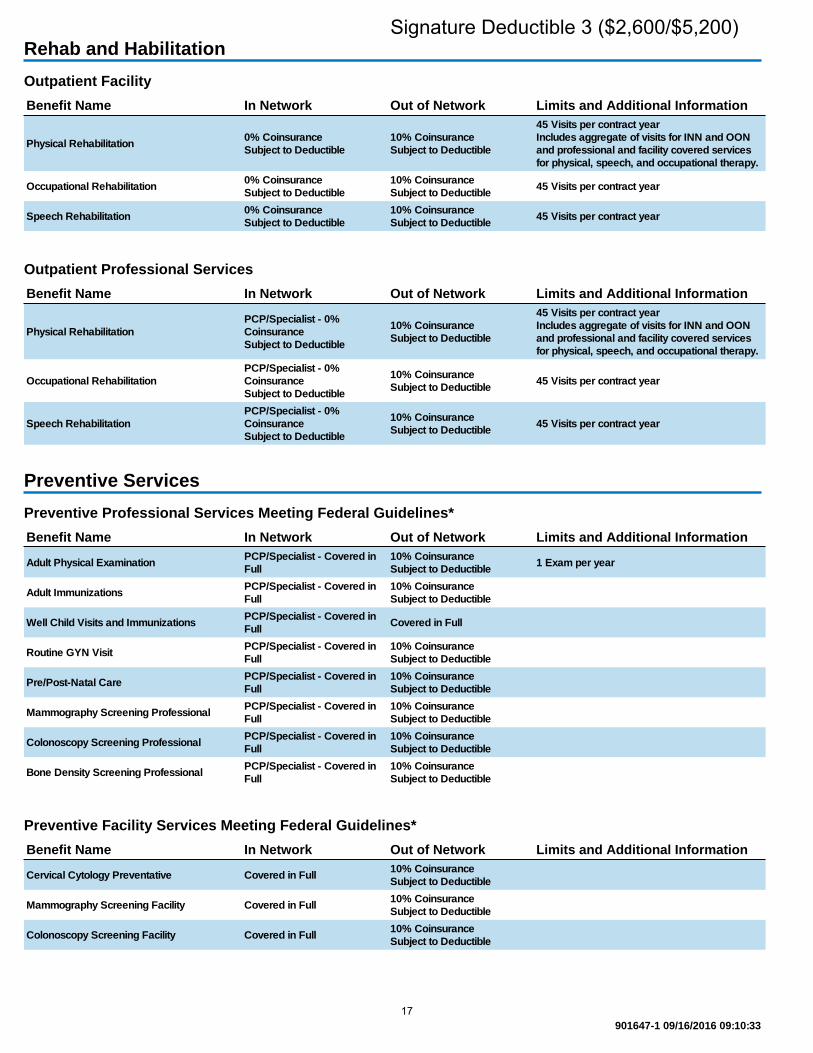
Rehab and Habilitation
Outpatient Facility
Benefit Name In Network Out of Network Limits and Additional Information
Physical Rehabilitation0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
45 Visits per contract year
Includes aggregate of visits for INN and OON
and professional and facility covered services
for physical, speech, and occupational therapy.
Occupational Rehabilitation0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible45 Visits per contract year
Speech Rehabilitation0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible45 Visits per contract year
Outpatient Professional Services
Benefit Name In Network Out of Network Limits and Additional Information
Physical Rehabilitation
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
45 Visits per contract year
Includes aggregate of visits for INN and OON
and professional and facility covered services
for physical, speech, and occupational therapy.
Occupational Rehabilitation
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible45 Visits per contract year
Speech Rehabilitation
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible45 Visits per contract year
Preventive Services
Preventive Professional Services Meeting Federal Guidelines*
Benefit Name In Network Out of Network Limits and Additional Information
Adult Physical ExaminationPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible1 Exam per year
Adult ImmunizationsPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Well Child Visits and ImmunizationsPCP/Specialist - Covered in
FullCovered in Full
Routine GYN VisitPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Pre/Post-Natal CarePCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Mammography Screening ProfessionalPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Colonoscopy Screening ProfessionalPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Bone Density Screening ProfessionalPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Preventive Facility Services Meeting Federal Guidelines*
Benefit Name In Network Out of Network Limits and Additional Information
Cervical Cytology Preventative Covered in Full10% Coinsurance
Subject to Deductible
Mammography Screening Facility Covered in Full10% Coinsurance
Subject to Deductible
Colonoscopy Screening Facility Covered in Full10% Coinsurance
Subject to Deductible
Signature Deductible 3 ($2,600/$5,200)
17
901647-1 09/16/2016 09:10:33
Benefit Name In Network Out of Network Limits and Additional Information
Bone Density Screening Facility Covered in Full10% Coinsurance
Subject to Deductible
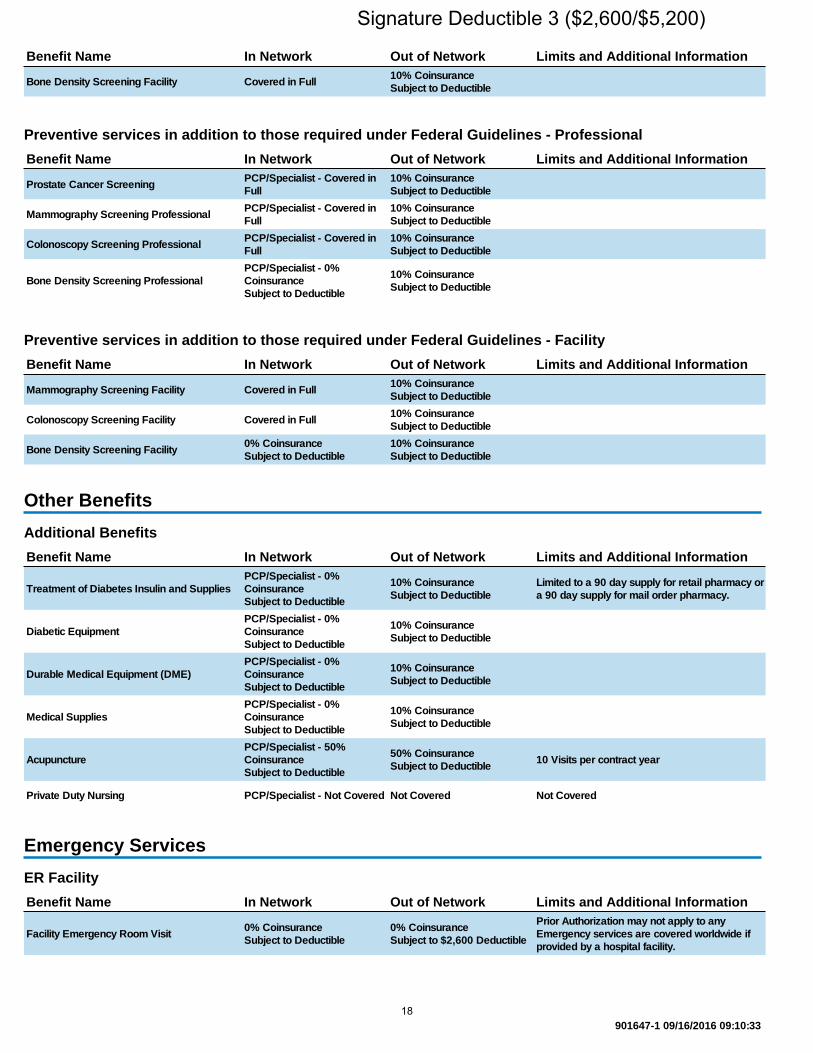
Preventive services in addition to those required under Federal Guidelines - Professional
Benefit Name In Network Out of Network Limits and Additional Information
Prostate Cancer ScreeningPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Mammography Screening ProfessionalPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Colonoscopy Screening ProfessionalPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Bone Density Screening Professional
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Preventive services in addition to those required under Federal Guidelines - Facility
Benefit Name In Network Out of Network Limits and Additional Information
Mammography Screening Facility Covered in Full10% Coinsurance
Subject to Deductible
Colonoscopy Screening Facility Covered in Full10% Coinsurance
Subject to Deductible
Bone Density Screening Facility0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Other Benefits
Additional Benefits
Benefit Name In Network Out of Network Limits and Additional Information
Treatment of Diabetes Insulin and Supplies
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Limited to a 90 day supply for retail pharmacy or
a 90 day supply for mail order pharmacy.
Diabetic Equipment
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Durable Medical Equipment (DME)
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Medical Supplies
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Acupuncture
PCP/Specialist - 50%
Coinsurance
Subject to Deductible
50% Coinsurance
Subject to Deductible10 Visits per contract year
Private Duty Nursing PCP/Specialist - Not Covered Not Covered Not Covered
Emergency Services
ER Facility
Benefit Name In Network Out of Network Limits and Additional Information
Facility Emergency Room Visit0% Coinsurance
Subject to Deductible
0% Coinsurance
Subject to $2,600 Deductible
Prior Authorization may not apply to any
Emergency services are covered worldwide if
provided by a hospital facility.
Signature Deductible 3 ($2,600/$5,200)
18

901647-1 09/16/2016 09:10:33
Transportation
Benefit Name In Network Out of Network Limits and Additional Information
Prehospital Emergency and Transportation -
Ground or Water
0% Coinsurance
Subject to Deductible
0% Coinsurance
Subject to $2,600 Deductible
Urgent Care
Benefit Name In Network Out of Network Limits and Additional Information
Urgent Care Center Facility Visit0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Ancillary Benefits
Vision
Benefit Name In Network Out of Network Limits and Additional Information
Adult Eye Exams - Routine0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible1 exam per contract year
Adult Eyewear - Routine Not Covered Not Covered Not Covered
Pediatric Eye Exams - Routine0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible1 exam per contract year
Pediatric Eyewear - Routine Not Covered Not Covered Not Covered
Rx Benefits
Rx Plan
Benefit Name In Network Out of Network Limits and Additional Information
Rx Plan$5/$35/$70, $0 gen for kids Integrated Rx, No
Ded Prev Rx
Rx Benefits
Benefit Name In Network Out of Network Limits and Additional Information
Days Supply Per Retail Order 30
Days Supply Per Mail Order 90
Copays Per Mail Order Supply 2
This document is not a contract. It is only intended to highlight the coverage of this program. Benefits are determined by the
terms of the contract. Any inconsistencies between this document and the contract shall be resolved in favor of the contract in
effect at the time services are rendered. All benefits are subject to medical necessity. All day and visit limits are combined
limits for both in and out of network benefits.
* For non-grandfathered groups, Preventive Services coverage required by the Patient Protection and Affordable Care Act are
not quoted herein. Please refer to the United States Preventive Services Task Force list of items and services rated "A" or "B"
that are covered pursuant to the Patient Protection and Affordable Care Act requirements.
Signature Deductible 3 ($2,600/$5,200)
19

Excellus BluePPO Signature Deduct 3Covered in Full Integrated Rx with $5/$35/$70 Preventive Rx
Benefit Time Period: 01/01/2017 - 12/31/2017
HUMAN TECHNOLOGIES CORP
901642-1 09/18/2016 04:58:22
General Information
Cost Sharing Expenses
Benefit Name In Network Out of Network Limits and Additional Information
Deductible - Single $5,500 $11,000
Deductible - Family $11,000 $22,000
Coinsurance 0% 10%
Annual Out of Pocket Maximum - Single $5,500 $11,000
Out-of-pocket maximums accumulate
coinsurance, copays and the deductible. Out-of-
pocket maximums exclude balances over
allowable expense and non-covered services.
Annual Out of Pocket Maximum - Family $11,000 $22,000
Out-of-pocket maximums accumulate
coinsurance, copays and the deductible. Out-of-
pocket maximums exclude balances over
allowable expense and non-covered services.
Annual Out of Pocket Maximum - Per Person
Cap$6,550 $22,000
The Out-of-Pocket Maximum Per Person Cap
includes deductible, coinsurance, copays and
prescription drugs. If a member under a family
contract meets the Out-Of-Pocket Maximum Per
Person Cap amount, the individual will no longer
pay for covered services and claims will be paid
at 100% of the allowable amount by the Health
Plan for the remainder of the plan year. The
remaining annual out-of-pocket maximum still
needs to be met by any combination of family
members on the contract before claims are paid
at 100% for the whole family.
Office Visit Cost Shares
Benefit Name In Network Out of Network Limits and Additional Information
Cost Share - Primary Care0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Cost Share - Specialist0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Plan Limits
Benefit Name In Network Out of Network Limits and Additional Information
Plan/Calendar Year Plan Year Benefits
Diabetic Preauthorization and Step Therapy Yes
Who is Covered
Benefit Name In Network Out of Network Limits and Additional Information
Domestic Partner Coverage Covered
Signature Deductible 3 ($5,500/$11,000)
20

901642-1 09/18/2016 04:58:22
Inpatient Services
Inpatient Facility
Benefit Name In Network Out of Network Limits and Additional Information
Inpatient Hospital Services0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Mental Health Care0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Substance Use Detoxification0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Skilled Nursing Facility0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
45 Days per contract year
Limits are combined INN and OON.
Physical Rehabilitation0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
60 Days per year
Limits are combined INN and OON.
Maternity Care0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Inpatient Professional Services
Benefit Name In Network Out of Network Limits and Additional Information
Inpatient Hospital Surgery
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Anesthesia
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
0% Coinsurance
Subject to $5,500 Deductible
Includes anesthesia rendered for Inpatient,
Outpatient, Office Visit, and Maternity services.
Anesthesia does not require a preauth or
referral.
Outpatient Facility Services
Outpatient Facility Services
Benefit Name In Network Out of Network Limits and Additional Information
SurgiCenters and Freestanding Ambulatory
Centers Surgical Care
0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Diagnostic X-ray0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Diagnostic Laboratory and Pathology0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Radiation Therapy0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Chemotherapy0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Infusion Therapy Inclusive of Primary Service Inclusive of Primary ServiceIs inclusive in the Home Care benefit and not
covered as a separate benefit.
Dialysis0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Mental Health Care0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to DeductibleIncludes Partial Hospitalization
Substance Use Care0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to DeductibleIncludes Partial Hospitalization
Home and Hospice Care
Home Care
Benefit Name In Network Out of Network Limits and Additional Information
Home Care0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Hospice Care
Signature Deductible 3 ($5,500/$11,000)
21

901642-1 09/18/2016 04:58:22
Benefit Name In Network Out of Network Limits and Additional Information
Hospice Care Inpatient0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Outpatient and Office Professional Services
Professional Services
Benefit Name In Network Out of Network Limits and Additional Information
Office Surgery
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Diagnostic X-ray
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Diagnostic Laboratory and Pathology
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Radiation Therapy
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Chemotherapy
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Infusion TherapyPCP/Specialist - Inclusive of
Primary ServiceInclusive of Primary Service
Is inclusive in the Home Care benefit and not
covered as a separate benefit.
Dialysis
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Mental Health Care
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Maternity Care
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
TeleMedicine Program
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
Not Covered
Covers online internet consultations between
the member and the providers who participate in
our telemedicine program for medical conditions
that are not an emergency condition.
Chiropractic Care
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Allergy Testing
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Allergy Testing includes injections and scratch
and prick tests.
Allergy Treatment Including Serum
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Includes desensitization treatments (injections &
serums).
Hearing Evaluations Routine
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
1 Exam per contract year
Limits are combined INN and OON.
Signature Deductible 3 ($5,500/$11,000)
22

901642-1 09/18/2016 04:58:22
Rehab and Habilitation
Outpatient Facility
Benefit Name In Network Out of Network Limits and Additional Information
Physical Rehabilitation0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
45 Visits per contract year
Includes aggregate of visits for INN and OON
and professional and facility covered services
for physical, speech, and occupational therapy.
Occupational Rehabilitation0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible45 Visits per contract year
Speech Rehabilitation0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible45 Visits per contract year
Outpatient Professional Services
Benefit Name In Network Out of Network Limits and Additional Information
Physical Rehabilitation
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
45 Visits per contract year
Includes aggregate of visits for INN and OON
and professional and facility covered services
for physical, speech, and occupational therapy.
Occupational Rehabilitation
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible45 Visits per contract year
Speech Rehabilitation
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible45 Visits per contract year
Preventive Services
Preventive Professional Services Meeting Federal Guidelines*
Benefit Name In Network Out of Network Limits and Additional Information
Adult Physical ExaminationPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible1 Exam per year
Adult ImmunizationsPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Well Child Visits and ImmunizationsPCP/Specialist - Covered in
FullCovered in Full
Routine GYN VisitPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Pre/Post-Natal CarePCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Mammography Screening ProfessionalPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Colonoscopy Screening ProfessionalPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Bone Density Screening ProfessionalPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Preventive Facility Services Meeting Federal Guidelines*
Benefit Name In Network Out of Network Limits and Additional Information
Cervical Cytology Preventative Covered in Full10% Coinsurance
Subject to Deductible
Mammography Screening Facility Covered in Full10% Coinsurance
Subject to Deductible
Colonoscopy Screening Facility Covered in Full10% Coinsurance
Subject to Deductible
Signature Deductible 3 ($5,500/$11,000)
23

901642-1 09/18/2016 04:58:22
Benefit Name In Network Out of Network Limits and Additional Information
Bone Density Screening Facility Covered in Full10% Coinsurance
Subject to Deductible
Preventive services in addition to those required under Federal Guidelines - Professional
Benefit Name In Network Out of Network Limits and Additional Information
Prostate Cancer ScreeningPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Mammography Screening ProfessionalPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Colonoscopy Screening ProfessionalPCP/Specialist - Covered in
Full
10% Coinsurance
Subject to Deductible
Bone Density Screening Professional
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Preventive services in addition to those required under Federal Guidelines - Facility
Benefit Name In Network Out of Network Limits and Additional Information
Mammography Screening Facility Covered in Full10% Coinsurance
Subject to Deductible
Colonoscopy Screening Facility Covered in Full10% Coinsurance
Subject to Deductible
Bone Density Screening Facility0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Other Benefits
Additional Benefits
Benefit Name In Network Out of Network Limits and Additional Information
Treatment of Diabetes Insulin and Supplies
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Limited to a 90 day supply for retail pharmacy or
a 90 day supply for mail order pharmacy.
Diabetic Equipment
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Durable Medical Equipment (DME)
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Medical Supplies
PCP/Specialist - 0%
Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Acupuncture
PCP/Specialist - 50%
Coinsurance
Subject to Deductible
50% Coinsurance
Subject to Deductible10 Visits per contract year
Private Duty Nursing PCP/Specialist - Not Covered Not Covered Not Covered
Emergency Services
ER Facility
Benefit Name In Network Out of Network Limits and Additional Information
Facility Emergency Room Visit0% Coinsurance
Subject to Deductible
0% Coinsurance
Subject to $5,500 Deductible
Prior Authorization may not apply to any
Emergency services are covered worldwide if
provided by a hospital facility.
Signature Deductible 3 ($5,500/$11,000)
24

901642-1 09/18/2016 04:58:22
Transportation
Benefit Name In Network Out of Network Limits and Additional Information
Prehospital Emergency and Transportation -
Ground or Water
0% Coinsurance
Subject to Deductible
0% Coinsurance
Subject to $5,500 Deductible
Urgent Care
Benefit Name In Network Out of Network Limits and Additional Information
Urgent Care Center Facility Visit0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible
Ancillary Benefits
Vision
Benefit Name In Network Out of Network Limits and Additional Information
Adult Eye Exams - Routine0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible1 exam per 2 contract years
Adult Eyewear - Routine Not Covered Not Covered Not Covered
Pediatric Eye Exams - Routine0% Coinsurance
Subject to Deductible
10% Coinsurance
Subject to Deductible1 exam per 2 contract years
Pediatric Eyewear - Routine Not Covered Not Covered Not Covered
Rx Benefits
Rx Plan
Benefit Name In Network Out of Network Limits and Additional Information
Rx PlanCovered in Full Integrated Rx with $5/$35/$70
Preventive Rx
Rx Benefits
Benefit Name In Network Out of Network Limits and Additional Information
Days Supply Per Retail Order 30
Days Supply Per Mail Order 90
Copays Per Mail Order Supply 2
This document is not a contract. It is only intended to highlight the coverage of this program. Benefits are determined by the
terms of the contract. Any inconsistencies between this document and the contract shall be resolved in favor of the contract in
effect at the time services are rendered. All benefits are subject to medical necessity. All day and visit limits are combined
limits for both in and out of network benefits.
* For non-grandfathered groups, Preventive Services coverage required by the Patient Protection and Affordable Care Act are
not quoted herein. Please refer to the United States Preventive Services Task Force list of items and services rated "A" or "B"
that are covered pursuant to the Patient Protection and Affordable Care Act requirements.
Signature Deductible 3 ($5,500/$11,000)
25

On-demand access to affordable, quality health care - Anytime, Anywhere.
Why wait for the care you need now? Excellus BlueCross BlueShield (BCBS) via our partner, MDLIVE, now offers another alternative to receive care. Visit with a U.S. board certified doctor right from your home, office or on the go for non-emergency medical conditions.
Powered by
When to use telemedicinew 24/7/365w If your primary care doctor is not availablew Instead of going to the ER or an urgent care center
(for a non-emergency issue)w To request prescription refills* w If traveling and in need of medical care
Common conditions treated
About the doctorsw On average, doctors have 15 years of experience
practicing medicine and are licensed in New York statew Specialties include primary care, pediatrics, emergency
and family medicinew You may even see your own doctor in the roster
Cost of a telemedicine visit for insured employeesw FREE registration w Once you’ve registered: Payment by credit card or
your health savings card will be required depending on your plan type:
- If you do not indicate you are an insured memberof Excellus BCBS: $49.00 charge
w Co-payment responsibility varies by group and plan w Our telemedicine service partner, MDLIVE, will be aware
of your co-payment amount when you contact them
*MDLIVE does not guarantee that a prescription will be written. MDLIVE does not prescribe DEA controlled substances, non-therapeutic drugs and certain other drugs which may be harmful because of their potential for abuse. MDLIVE physicians reserve the right to deny care for potential misuse of services. For complete terms of use visit mdlive.com/pages/terms.html
**Parents must be present on each call for children under age 18.
Disclaimers: MDLIVE does not replace the primary care physician. MDLIVE is not an insurance product nor a prescription fulfillment warehouse. MDLIVE operates subject to state regulation and may not be available in certain states. MDLIVE does not guarantee that a prescription will be written. MDLIVE does not prescribe DEA controlled substances, non-therapeutic drugs and certain other drugs which may be harmful because of their potential for abuse. MDLIVE physicians reserve the right to deny care for potential misuse of services. MDLIVE phone consultations are available 24/7/365, while video consultations are available during the hours of 7 am to 9 pm ET 7 days a week or by scheduled availability. MDLIVE and the MDLIVE logo are registered trademarks of MDLIVE, Inc. and may not be used without written permission. For complete terms of use visit www.mdlive.com/pages/terms.html 010113. MDLive is an independent company, offering telehealth services in the Excellus BlueCross BlueShield service area. Excellus BlueCross BlueShield is a nonprofit independent licensee of the Blue Cross Blue Shield Association.
w Allergiesw Asthmaw Bronchitisw Cold & Fluw Diarrheaw Ear Infectionsw Feverw Headache
w Infectionsw Insect Bitesw Joint Achesw Rashesw Sinus Infectionsw Skin Infectionsw Sore Throatw And More!
Pediatric Care**w Cold & Fluw Constipationw Ear Infectionsw Nauseaw Pink Eyew And More!
ExcellusBCBS.com/Telemedicine1-866-692-5045
B-5460 / 10448-16M
If Primary Care Physician office visit is....
Then telemedicine program benefit cost share is....
Covered with a copay $10 (or equal to the PCP copay if PCP copay is less than $10)
Covered with copay/ deductible
$10 copay subject to deduct-ible (or equal to the PCP copay if PCP copay is less than $10)
Covered deductible/ covered in full
Deductible/covered in full
Covered with deductible/co-insurance
Deductible/co-insurance
Covered with co-insurance only
Co-insurance only
26

The information in this Benefits Overview is presented for illustrative purposes and is based on information provided by the employer. In case of discrepancy between the Benefits Overview and the actual plan documents, the actual plan documents will prevail.
HEALTH FSA Note: this is intended only as a general overview of a Health FSA. See the “Understanding Your…” section for the specifics around the program offered to you.
Flexible Spending Account
A special account you put money into that you use to pay for certain out-of-pocket health care costs. You don't pay taxes on this money. This means you'll save an amount equal to the taxes you would have paid on the money you set aside. The FSA operates with a use-or-lose rule, meaning if you don’t use the money in your FSA by the end of the plan year, you will lose it (however, some employers relax the use-or-lose rule with one of two options: a grace period or a carry-over).
Paying for health expenses can be stressful, but planning ahead and putting money in a health flexible spending account
(FSA) will help you save on taxes while keeping a reserve of money available for health care costs.
Some examples of eligible expenses include:
Deductibles, Copays, and
Coinsurance
Hearing services, including
hearing aids and batteries
WHY HAVE A HEALTH FSA?
Vision services (contact
lenses, contact lens
solution, eye
examinations, eyeglasses)
Dental services and
orthodontia
Chiropractic services
Acupuncture
Health FSAs offer an option for setting aside money to use for qualified medical expenses. These accounts offer a
convenient way to prepare for out-of-pocket medical expenses while saving on taxes. In addition, you can use your
health FSA to pay not only for your medical expenses, but also for the medical expenses of your spouse and dependents
even if they are not covered by your employer’s plan.
Here are some of the advantages an FSA can provide:
TAX REDUCTIONS:The amount you contribute to a health FSA is not subject to federal income tax or social
security (FICA) tax—effectively adjusting your annual taxable salary. The taxes you pay each paycheck and collectively
each plan year can be reduced significantly.
Your employer can also contribute to your FSA, and this amount is also not considered taxable income toyou.
You can withdraw money from your FSA to pay for qualified medical expenses; your withdrawals are not taxed.
You do not have to report FSA amounts on your income taxreturn.
CONVENIENCE:After the initial election at the beginning of the year, your employer will take care of
transferring the allotted amount into your FSA through salary deferral.
FLEXIBILITY: You can withdraw health FSA funds at any time (for qualified medical expenses), even if the amount
has not yet been deposited into the account, as long as the amount is no more than your elected annual deferral
amount less any amount already used.
27

The information in this Benefits Summary is presented for illustrative purposes and is based on information provided by the employer. In case of discrepancy between the Benefits Summary and the actual plan documents, the actual plan documents will prevail.
Setting Up An FSA
If you have questions about setting up a FSA, contact Human Resources (contact information can be found on the
cover of this overview).
Contributions
Employee Contributes: This Amount Is To Be Determined By You (The Employee).
The FSA operates with a use-or-lose rule, meaning if you don’t use the money in your FSA by the end of the plan
year, you will lose it. However, there is a Carry Over which allows you to carry over up to $500 of any unused funds into
the next year.
After your initial contribution election, you ordinarily cannot change your election for a plan year during the year. Your
elected contribution amount can only be changed if you experience a permitted election change event, such as a
change in family status and your FSA permits you to change your election.
The amount you choose to transfer into your FSA should be based on the amount of qualifying medical expenses you
anticipate your family incurring during the plan year. Start by looking at your family’s medical expenses for the past year
and then determine whether your family will likely have those same expenses again and whether there will likely be any
new expenses. Use this estimate to help you choose what amount you would like to contribute to your FSA,
remembering that it is typically best to underestimate by a little than to overestimate and lose that money at the end of
the year.
Using your FSA Funds
When you are paying for a qualified medical expense that you would like to use your FSA funds for, you will use the
following method:
Health Payment Card
This is very similar to a debit or credit card. You can pay for eligible medical services or products by swiping the card
as you would a debit or credit card. The money will then be deducted from your FSA account.
Health care payment cards may be used only on eligible medical expenses that are not reimbursed or covered by
another source. Over-the-counter (OTC) medications are only eligible for reimbursement if they are prescribed to
you and if you present the prescription at the time of purchase. The only OTC medication that can be reimbursed
without a prescription is insulin.
Note: Funds do not need to be available in the account in order to be reimbursed; however, health care payment
cards may not be used to cover more than your annual elected amount.
Note: In 2017, the maximum amount that can be contributed to your FSA is $2,600.
UNDERSTANDING YOUR FLEXIBLE SPENDING ACCOUNT
28

The information in this Benefits Summary is presented for illustrative purposes and is based on information provided by the employer. In case of discrepancy between the Benefits Summary and the actual plan documents, the actual plan documents will prevail.
As a general rule, every claim paid with a health care payment card must be reviewed and substantiated. The IRS
guidance allows automatic adjudication for certain card transactions, meaning that receipts do not need to be
submitted for verification of expenses for which a health care payment card is used. This applies in three situations at
medical providers and 90-percent pharmacies (drug stores and pharmacies where at least 90 percent of the store’s
gross receipts during the prior taxable year consisted of medical expenses):
When the total cost of the transaction is equal to the standard copayment for the service(s) received
When the transaction is for recurring expenses that have previously been approved
When the merchant provides expense verification to the employer when the transaction takesplace
Recordkeeping
In most cases, you will have to submit receipts and other proof that you purchased an eligible medical service or product
in order to receive reimbursement. Make sure you retain all receipts, Explanation of Benefits (EOBs) and other
documents to ensure that you have the necessary proof to obtain reimbursement from your FSA.
29

The information in this Benefits Summary is presented for illustrative purposes and is based on information provided by the employer. In case of discrepancy between the Benefits Summary and the actual plan documents, the actual plan documents will prevail.
Note: this is intended only as a general overview of a health reimbursement arrangement. See the “Understanding Your…” section for the specifics around the program offered to you.
Health Reimbursement Arrangement
An employer-funded arrangement that reimburses employees for certain medical expenses. These arrangements are typically paired with a high deductible health plan.
A health reimbursement arrangement (HRA) can be a great way to take advantage of employer contributions for your
health care expenses. An HRA is entirely employer-funded, essentially boosting your salary with tax-free money for
health care expenses.
You can use your HRA funds to get reimbursed for your own eligible medical expenses, as well as your spouse’s and
dependents’ eligible medical expenses. Eligible medical expenses are unreimbursed medical care expenses, as defined
under Section 213(d) of the Internal Revenue Code. An employer can more narrowly define the expenses that can be
reimbursed from its HRA. Your HRA coverage must be in effect at the time the qualified medical expense is incurred in
order to receive reimbursement.
WHY HAVE AN HRA?
HRAs provide a tax-free, employer-funded amount of money for health care expenses. These arrangements are a great
way to pay for out-of-pocket qualified medical expenses while working to meet your plan deductible. If your employer
offers an HRA, it can be a tremendous advantage as you pay out-of-pocket medical expenses, especially with a high
deductible health plan. HRAs offer several benefits:
TAX SAVINGS
Your employer’s contributions to your HRA can be excluded from your gross income, meaning you don’t
pay taxes on that money.
Reimbursements from your HRA are tax-free when used to pay for qualified medical expenses (which are
the only expenses they can be used for).
OUT-OF-POCKET EXPENSE REDUCTION
Often paired with a high deductible health plan, reimbursement from your HRA will make it much easier to
meet your deductible while taking advantage of a health plan with lower premiums.
HEALTH REIMBURSEMENT ARRANGEMENT
30

The information in this Benefits Summary is presented for illustrative purposes and is based on information provided by the employer. In case of discrepancy between the Benefits Summary and the actual plan documents, the actual plan documents will prevail.
Setting Up An HRA
If you have questions about setting up a HRA, contact Human Resources (contact information can be found on the
cover of this overview).
Contributions
Employer Contributes:
HRA – Signature Deductible 3 ($2,600/$5,200)
Single $1,300
Employee + 1 $2,600
Family $2,600
Funded Quarterly
HRA – Signature Deductible 3 ($5,500/$11,000)
Single $2,500
Employee + 1 $5,000
Family $5,000
Funded Quarterly
Employee Contributes: Employees are NOT able to contribute toward the HRA.
Applicable Expenses
The funds in your HRA can be used toward the following expenses only:
Medical Deductible
Rx Expenses
Using your HRA Funds
When you are paying for a qualified medical expense that you would like to use your HRA funds for, you will use the
following method:
Health Payment Card
This is very similar to a debit or credit card. You can pay for eligible medical services or products by swiping the card as
you would a debit or credit card. The money will then be deducted from your HRA account.
Health care payment cards may be used only on eligible medical expenses that are not reimbursed or covered by
UNDERSTANDING YOUR HEALTH REIMBURSEMENT
31
The information in this Benefits Summary is presented for illustrative purposes and is based on information provided by the employer. In case of discrepancy between the Benefits Summary and the actual plan documents, the actual plan documents will prevail.
another source. Over-the-counter (OTC) medications are only eligible for reimbursement if they are prescribed to you
and if you present the prescription at the time of purchase. The only OTC medication that can be reimbursed without a
prescription is insulin. Health care payment cards may not be used to cover more than the maximum dollar amount of
coverage available in your HRA.
Note On Unused Funds: Any unused funds at the end of the plan year will not roll over
32

The information in this Benefits Overview is presented for illustrative purposes and is based on information provided by the employer. In case of discrepancy between the Benefits Overview and the actual plan documents, the actual plan documents will prevail.
DENTAL Note: this is intended only as a general overview of dental insurance. See the “Understanding Your…” section for the specifics around the plan(s) offered to you.
Dental Insurance Dental insurance is designed to pay a portion of the costs associated with dental care.
Aside from protecting your smile, dental care ensures good oral and overall health. Several studies suggest that oral
diseases, such as periodontitis (gum disease), can affect other areas of your body—including your heart. Understanding
and choosing dental coverage will help protect you and your family from the high cost of dental disease and surgery.
WHY SHOULD I HAVE DENTAL INSURANCE?
Professional dental care can diagnose or help prevent common dental problems including toothache, inflamed gums,
tooth decay, bad breath and dry mouth. If conditions like these remain untreated, they can worsen into painful and
expensive problems such as gum disease or even tooth loss. According to the American Dental Association, more than
16 million children in the United States suffer from untreated tooth decay, which is the most common chronic childhood
disease. Regular dental exams can not only treat dental problems but can also identify other serious health concerns,
including some types of cancer. Dental coverage will allow you to inexpensively receive preventive and diagnostic care.
WHAT DENTAL SERVICES ARE TYPICALLY COVERED?
Dental coverage focuses on preventive and diagnostic procedures in an effort to avoid more expensive services
associated with dental disease and surgery. The type of service or procedure received determines the amount of
coverage for each visit. Each type of service fits into a class of services according to complexity and cost.
In addition to the class of service, coverage also depends on other factors. Several common services are limited by
frequency. For example, most plans will only cover two cleanings and exams per year. For more complicated procedures
or surgeries, coverage is often limited to a maximum dollar amount. Age is yet another factor that determines coverage.
For example, fluoride treatments are typically covered for children, but not adults. Cosmetic procedures, such as teeth-
whitening, are rarely covered.
HOW HAS HEALTH CARE REFORM AFFECTED DENTAL COVERAGE?
Under the Affordable Care Act (ACA), dental services are an essential health benefit for children under the age of 19,
although individual states can choose to extend the age limit beyond this baseline. Declaring pediatric dental care an
essential health benefit means that, beginning in 2014, all non-grandfathered medical health plans must offer dental
benefits for children unless certified stand-alone coverage is available. Non-medically necessary orthodontia is not
included in the essential health benefits definition.
The essential health benefit status for dental coverage does not apply to adults. In addition, unlike medical insurance,
you do not have to obtain dental coverage to avoid penalties.
33

The information in this Benefits Overview is presented for illustrative purposes and is based on information provided by the employer. In case of discrepancy between the Benefits Overview and the actual plan documents, the actual plan documents will prevail.
Dental Plan Overview
Option 1: Dental PPO
Guardian
Note: Plan information can be found on the following pages.
Cost
Plan #1 Name: Guardian Dental PPO
Monthly Plan Cost ($)
Monthly Employee Cost Share ($)
Monthly Employer Cost
Employee Cost Per Pay Period
Employer Cost Per Pay Period
Single $34.12 $17.06 $17.06 $7.87 $7.87
Family $97.62 $80.56 $17.06 $37.18 $7.87
UNDERSTANDING YOUR DENTAL BENEFITS
34
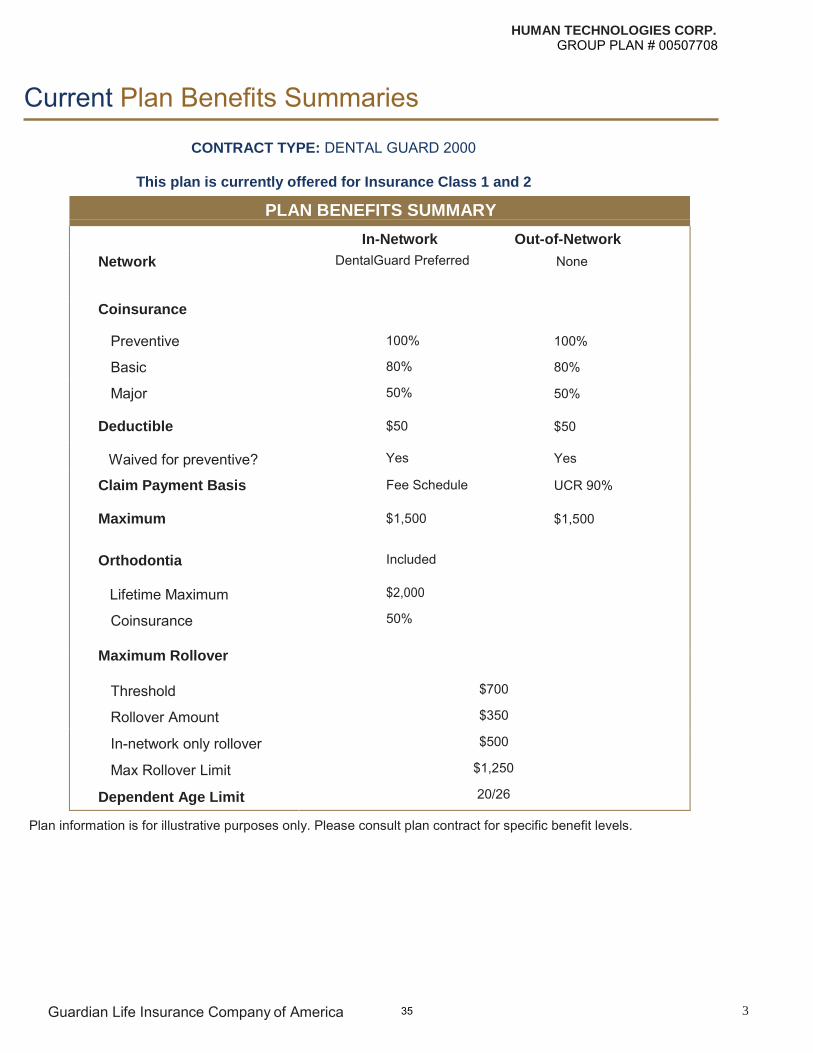
HUMAN TECHNOLOGIES CORP. GROUP PLAN # 00507708
Current Plan Benefits Summaries
CONTRACT TYPE: DENTAL GUARD 2000
This plan is currently offered for Insurance Class 1 and 2
PLAN BENEFITS SUMMARY
In-Network
DentalGuard Preferred
100%
80%
50%
$50
Yes
Fee Schedule
$1,500
Included
$2,000
50%
Out-of-Network
Network
Coinsurance
Preventive
Basic
Major
Deductible
Waived for preventive?
Claim Payment Basis
Maximum
Orthodontia
Lifetime Maximum
Coinsurance
Maximum Rollover
Threshold
Rollover Amount
In-network only rollover
Max Rollover Limit
Dependent Age Limit
None
100%
80%
50%
$50
Yes
UCR 90%
$1,500
$700
$350
$500
$1,250
20/26
Plan information is for illustrative purposes only. Please consult plan contract for specific benefit levels.
Guardian Life Insurance Company of America 3 35
The information in this Benefits Overview is presented for illustrative purposes and is based on information provided by the employer. In case of discrepancy between the Benefits Overview and the actual plan documents, the actual plan documents will prevail.
VISION Note: this is intended only as a general overview of vision insurance. See the “Understanding Your…” section for the specifics around the plan(s) offered to you.
Vision Insurance Vision insurance is designed to pay a portion of the costs associated with routine preventive eye care (eye exams) and prescription eyewear (eyeglasses and contact lenses).
Driving to work, reading a news article and watching television are likely activities you perform every day. Your ability to
do all of these, however, depends on your vision and eye health.
WHY SHOULD I HAVE VISION INSURANCE?
Routine eye exams will help maintain your vision as well as detect various eye problems and concerns about your overall
health. Obtaining vision insurance is a way to make sure you can continue enjoying good health as well as the sights
around you.
According to Gallup, approximately 70 percent of adult Americans report wearing some type of corrective lenses. A visit
with your eye doctor can determine whether you need corrective lenses and, if so, the correct prescription. Other eye
concerns that will be addressed in an eye exam include checking for conditions or diseases such as glaucoma and
cataracts, which can lead to vision loss. Regular eye exams can also identify overall health concerns, such as diabetes,
high cholesterol and risk of heart disease or stroke before you are even aware of any symptoms. You can then follow up
with a medical doctor, minimizing the effects of these conditions on your health and finances.
WHAT IS COVERED UNDER VISION INSURANCE?
Vision insurance generally provides coverage for basic care and eyewear. Most vision plans will cover the following
services:
Annual or biannual eye exams, includingdilation
Eyeglass frames
Eyeglass lenses
Contact lenses
Some plans may also cover other services, including laser vision care programs or even prescription protective eyewear
that is compliant with ANSI and OSHA safety guidelines.
Vision plans typically do not cover replacements for frames, eyeglass lenses or contact lenses, medical or surgical
treatment, vision training or experimental vision services or treatments.
36

The information in this Benefits Overview is presented for illustrative purposes and is based on information provided by the employer. In case of discrepancy between the Benefits Overview and the actual plan documents, the actual plan documents will prevail.
Vision Plan Overview
Option 1: Davis Vision
Guardian
Note: Plan information can be found on the following pages.
Cost
Plan #1 Name: Guardian Vision Plan - Davis Vision Network
Monthly Plan Cost ($)
Monthly Employee Cost Share ($)
Monthly Employer Cost
Employee Cost Per Pay Period
Employer Cost Per Pay Period
Single $7.93 $7.93 $0.00 $3.66 $0.00
Family $17.04 $17.04 $0.00 $7.86 $0.00
UNDERSTANDING YOUR VISION BENEFITS
37

HUMAN TECHNOLOGIES CORP. GROUP PLAN # 00507708
Current Plan Benefits Summaries
DAVIS
VOLUNTARY VISION
This plan is currently offered for Insurance Class 1 and 2
PLAN BENEFITS SUMMARY
In-Network Out-of-Network Frequency
Exam Copay $10 $10 Once per Calendar Year
Exam Allowance 100% $50 Once per Calendar Year
Materials Copay $20 $20
Base Lenses
Single Vision Allowance 100% $48 Once per Calendar Year Bifocal Allowance 100% $67 Once per Calendar Year Trifocal Allowance 100% $86 Once per Calendar Year Lenticular Allowance 100% $126 Once per Calendar Year
Contact Lenses
Elective Allowance $130 $105 Once per Calendar Year Therapeutic Allowance 100% $210 Once per Calendar Year
Frame Retail Allowance $130 $48 Every Other Calendar Year
Materials Allowance N/A N/A N/A
Plan information is for illustrative purposes only. Please consult plan contract for specific benefit levels.
Guardian Life Insurance Company of America 5 38

The information in this Benefits Overview is presented for illustrative purposes and is based on information provided
by the employer. The text contained in this Overview was taken from various summary plan descriptions and benefit
information. While every effort was taken to accurately report your benefits, discrepancies or errors are always
possible. In case of discrepancy between the Benefits Overview and the actual plan documents, the actual plan
documents will prevail. All information is confidential, pursuant to the Health Insurance Portability and Accountability
Act of 1996. If you have any questions about this summary, contact Human Resources.
The information in this Benefits Overview is presented for illustrative purposes and is based on information provided by the employer. In case of discrepancy between the Benefits Overview and the actual plan documents, the actual plan documents will prevail.
39






![Summary of Benefits CTC (2).pptjobs.dadeschools.net/recruitment/PDF/Summary of Benefits OPT.pdf · Title: Microsoft PowerPoint - Summary of Benefits CTC (2).ppt [Compatibility Mode]](https://img.dokumen.tips/doc/110x75/605ae534ecfee8670619b886/summary-of-benefits-ctc-2-of-benefits-optpdf-title-microsoft-powerpoint-.jpg)


![v > ] ( / v µ v } u v Ç E Á z } l / v ] À ] µ o } v À ... · NY Small Group Portfolio | Summary of Benefits Contents NY Platinum OFF ONLY 2 NY Gold OFF ONLY 3 NY Silver OFF](https://img.dokumen.tips/doc/110x75/5f488eba97cc76031f6c0e6e/v-v-v-u-v-e-z-l-v-o-v-ny-small-group.jpg)



















