Embed Size (px)
Citation preview

Emotional Processing During Eye Movement Desensit izat ion and Reprocessing Therapy of Vietnam Veterans With Chronic
Posttraumatic Stress Disorder
Roger K. Pitman, Scott P. Orr, Bruce Altman, Ronald E. Longpre, Roger E. Poir6, and Michael L. Macklin
This study examined emotional processing and out- come in 17 Vietnam veterans with chronic posttrau- matic stress disorder (PTSO) who underwent eye movement desensitization and reprocessing (EMDR) therapy, with and without the eye movement compo- nent, in a crossover design. Results supported the occurrence of partial emotional processing, but there were no differences in its extent in the eye-movement versus eyes-fixed conditions. Therapy produced a rood- est to moderate overall improvement, mostly on the Impact of Event Scale. There was slightly more ira- provement in the eyes-fixed than eye-movement con-
dition. There was little association between the extent of emotional processing and therapeutic outcome. In our hands, EMDR was at least as efficacious for combat- related PTSD as imaginal flooding proved to be in a previous study, and was better tolerated by subjects. However, results suggest that eye movements do not play a significant role in processing of traumatic informa- tion in EMDR and that factors other than eye move- ments are responsible for EMDR's therapeutic effect. This is a US government work, There are no restric. t ions on i ts use.
S INCE ITS INTRODUCTION several years ago, the novel psychotherapy currently re-
ferred to as eye movement desensitization and reprocessing (EMDR) ] has captured the atten- tion of the posttraumatic stress disorder (PTSD) clinical and research communities as has no other treatment. The procedure was discovered accidentally by Shapiro 2 when she noticed that her own recurrent, disturbing thoughts disap- peared when she moved her eyes in a "multi- saccadic" manner. She subsequently devised a therapeutic procedure based on this observa- tion, which involves inducing the patient to perform sets of eye movements tracking the therapist's hand as it travels back and forth in front of the patient's face, while the patient engages in therapist-assisted emotional and cog- nitive reprocessing of aspects of the traumatic event or other disturbing thoughts or memories. Shapiro and colleagues have trained thousands of therapists in the performance of EMDR, and its practice is now widespread.
The efficacy of EMDR in PTSD and related conditions is supported by numerous case re- ports, a growing number of case se r ies , 3-6 and uncontrolled 7 and controlled 8-1° studies. How- ever, not all studies have found EMDR helpful, especially in Vietnam combat veterans u,12 and the more seriously mentally ill. ~3 Studies of EMDR have been criticized on methodologic grounds, ~4,15 and the therapy has even been likened to mesmerism? 6
The therapeutic mechanism of EMDR re- mains unclear. Despite acknowledging the pos- sible contributions of exposure, distraction, trance,
suggestion, and therapist "demand characteris- tics," Shap i ro 17 assigned a pivotal role to the eye movements, speculating that these overcome "neu- ral blockage" and reverse neural pathology set in motion by the traumatic incident. Shapiro pro- posed that "the rhythmic, multi-saccadic eye move- ments used in EMDR may be the body's natural inhibitory mechanism, similar or identical to the 'rapid eye movement' (REM) dream state of sleep, during which unconscious material surfaces and may be desensitized and integrated. ''17 (p. 135) However, this analogy suffers from lack of phenom- enologic correspondence between the rhythmic eye movements induced by the EMDR procedure and the spontaneous, arrhythmic, nonsaccadic eye movements that occur during REM sleep. Al- though REM sleep may serve a physiologic informa- tion processing function, TM eye movements during REM sleep may represent only an epiphenomenon of dreaming--i.e., they result from, rather than induce, information processing. Other explana- tions advanced for the mechanism of action of the eye movements during EMDR include interfer- ence with the trace memory caused by neuronal
From the Research Service, Veterans Affairs Medical Center, Manchester, NH; and the Department of Psychiatry, Harvard Medical School, Boston, MA.
Supported by National Institutes of Mental Health Grant No. ROIMH42872 and a Veterans Administration Research Career Development Award (R.K.P. ).
Address reprint requests to Dr. Roger K. Pitman, VA Research Service, 228 Maple St, Manchester NH 03103.
This is a US government work. There are no restrictions on its use.
0010-440X/96/3706-000850. O0/0
Comprehensive Psychiatry, Vol. 37, No. 6 (November/December), 1996: pp 419-429 419

420 PITMAN ET AL
bursts associated with the eye movements, 17 inter- ference with the tracts connecting the frontal lobes with the hypothalamus and hippocampus by field currents generated by the eye movements, 3 and REM-induced muscular inhibition by way of the reticular formation.17
All neurophysiologic theories about the ac- tion of eye movements in EMDR are consider- ably blunted by dismantling studies that have shown that the eye movement component may be deleted from the procedure without loss of therapeutic benefit. In one study, 58 phobic subjects were treated with eye movement desen- sitization (EMD, an earlier version of EMDR) versus image confrontation (during which the eyes were closed and motionless). The two approaches were equally efficacious in reducing anxiety in a single-session crossover trial. 19 In another study, 23 subjects (21 of whom had PTSD) underwent therapy in three conditions: EMD, automated eye movements, and active visual attention without eye movements. Al- though the therapy was efficacious overall, there were no differences among conditions. 2° In another study, test anxiety in 15 pairs of stu- dents was treated in one of two conditions: EMD or finger tapping, an experimental substi- tute for eye movement. Both groups improved, but with no difference in conditions. 21
Another investigation focused on the role of eye movements in the intratherapy process. Thirty-six normal subjects who reported distress after exposure to loud, aversive electronic sounds, followed by viewing a photograph of a mutilated corpse, were treated with brief, single sessions of rapid EMD, slow EMD, and station- ary imagery performed during imagery of the aversive photograph. Subjective units of distress (SUDS; sometimes also called subjective units of disturbance or discomfort) ratings were elic- ited from subjects at 10-second intervals. Emo- tional processing, gauged by the course of SUDS ratings during the therapies, was significantly impaired in the rapid EMD compared to the slow EMD and stationary imagery groups. The investigators concluded that REM does not facilitate emotional processing. 22 However, the relevance of this study is limited by the use of normal subjects, a contrived stressor, and dis- crepancies between the rapid EMD method and the clinical EMDR procedure.
In contrast to the above dismantling studies that failed to find a contribution of eye move- ments to the procedure's therapeutic effect, in another study a nonsaccade treatment phase designed to control for the role of the eye movements preceded EMD treatment. Subjects only improved in the EMD phase. 23 However, the two phases in this study appear to have differed in important respects besides the pres- ence of eye movements. For example, the con- trol treatment was briefer and lacked instruc- tion to blank out the stressful image used in the EMDR procedure. The control treatment also lacked motion of the therapist's hand in front of the patient's face, a gesture which may convey psychologic meaning apart from the intended effect of inducing eye movements. Another investigation found that either reprocessing or music, accompanying eye movements, equally reduced psychology students' reports of acute pain induced by hand exposures to ice water over a no-eye-movement control intervention that merely instructed subjects that they were participating in an experiment testing their ability to cope with acute pain. 24 Again, the control intervention differed from the two ac- tive interventions in important respects besides the inclusion of eye movements, e.g., the control intervention lacked the components of therapist hand movements, activity on the part of the subject, and distraction (via music or reprocess- ing) from the painful stimulus.
This last study 24 may also be viewed as a dismantling procedure for EMDR's reprocess- ing component. The finding that substituting music for reprocessing did not diminish benefi- cial effect led the authors to conclude that reprocessing operations were not responsible for the procedure's efficacy. The fact that some studies have removed eye movements and oth- ers have removed reprocessing from the EMDR procedure, without loss of efficacy, suggests that other unidentified factors, such as distraction, suggestion, and therapist "demand characteris- tics," may be contributing to EMDR's therapeu- tic effect.
A few studies have incorporated psychophysi- ologic measures in assessing EMDR. One study reported a mean 13 beat per minute drop in the highest pulse rate occurring during elicitation of the traumatic memory in a single EMD treat-

EMOTIONAL PROCESSING DURING EMDR IN PTSD 421
ment session versus during a 1-month follow-up session. Unfortunately, the absence of control heart rate (HR) data made it impossible to rule out habituation to the experimenter or environ- ment as the cause of pulse rate decline. 8 An- other psychophysiologic investigation measured HR, skin conductance (SC), frontalis electro- myogram (EMG-frnt), and skin temperature responses during audiotaped verbal descrip- tions of subjects' traumatic combat memories before and after EMD or an exposure control therapy. Although SUDS ratings decreased dur- ing the therapy sessions (more so in the EMD group), there were no significant effects of treatment on physiologic responding, nor on psychometric outcome measures, including the Impact of Event Scale (IOES), Mississippi Scale for Combat-Related PTSD, and Clinician- Administered PTSD Scale (CAPS), for either the EMD or exposure control treatment. 11 An- other investigation incorporated HR and blood pressure measurements in baseline, nonsaccade control, EMD, and 1-week follow-up phases. Al- though HR and blood pressure decreased across these phases, the changes were not significant. 23
The title of EMDR implies a role for eye movements in what has been referred to as emotional processing, z5 We decided to test this role by performing a dismantling study that employed two therapy conditions, one with eye movements, the other with no eye movements, i.e., eyes fixed. The eyes-fixed condition re- tained therapist hand movements and all the other features of the EMDR procedure. To control for the possible role of activity on the part of the patient during the EMDR proce- dure, the eyes-fixed condition also substituted rhythmic finger tapping for the eye movements, as done in a previous study. 21
Critics have faulted early studies of EMD for lacking several important components of therapy outcome studies, including subject diagnostic information, objective or standardized symptom assessment (i.e., outcome) measures, indepen- dent raters, multiple baseline assessments, and control treatments, an The study reported here included all of these components except mul- tiple baseline assessments. However, the chro- nicity of PTSD in the present subjects made instability of the presenting symptoms prior to treatment (the reason for multiple baseline
assessments) unlikely. Shapiro has insisted that "any research that purports to test the efficacy of EMD(R) must involve the entire procedure as used in clinical practice, which contains many components assumed to have beneficial effect besides the eye movements alone. ''26 (p. 89) The present study also met this standard.
We hypothesized that, compared to the eyes- fixed control therapy, the active EMDR therapy would induce (1) more emotional processing, in the form of more physiologic and self-reported evidence of activation, within-(WSH) and across- session habituation (ASH); and (2) more im- provement in outcome measures. We also hy- pothesized that the extent of emotional processing would predict the amount of improve- ment. Because of its capability of measuring PTSD intrusion and avoidance symptomatology associated with a specific combat-related event that constituted the object of treatment, a priori emphasis was given to the IOES in assessing therapy outcome.
METHOD
Subjects Subjects were 17 male Vietnam combat veterans meeting
diagnostic criteria for PTSD as determined by the Struc- tured Clinical Interview for DSM-III-R (SCID). 27 To partici- pate, each subject had to describe two combat-related events he considered to have been emotionally traumatic and implicated in his subsequent symptoms. Subjects were recruited as part of an outreach effort and were not necessarily seeking treatment for their PTSD. Inpatients were excluded, as were subjects with an organic, psychotic, manic, or melancholic disorder, or with current alcohol or other substance dependence. Subjects who were enrolled in other individual or group psychotherapy were allowed to enter the study only if the concurrent therapy was support- ive in nature and was not expected to overlap or conflict with the research therapy. None of the subjects had partici- pated in our previously reported flooding study of PTSD. 28 Unlike that study, subjects were not required to discontinue any prescribed medication in order to participate. However, no subject underwent a change in prescribed medication regimen from 1 month prior to participation until after the conclusion of the present study. Subjects who were on nonprescribed medication or substances that could inter- fere with the physiologic responses to be measured were asked to abstain from their use for 1 month prior to and for the duration of the study. Subjects who were unwilling to meet this requirement were excluded.
Subject demographic and psychometric measures (mean _+ SD) were as follows: age, 44.2 ± 3.2; educational level (i.e., highest grade completed), 13.4 --- 1.7; combat exposure, 10.1 ± 3.5 on a 0 to 14 scale 29 and 28.7 ± 10.7 on a 0 to 41 scale. 3° Current comorbid axis I disorders included nine (53%) major

422 PITMAN ET AL
depression, seven (41%) dysthymia, two (12%) simple phobia, one (6%) social phobia, one (6%) panic without agoraphobia, one (6%) generalized anxiety, one (6%) obsessive-compulsive, one (6%) alcohol abuse, and one (6%) cocaine abuse. Some subjects had more than one comorbid disorder; none had no comorbid disorder.
All subjects were enrolled as Veterans Affairs (VA) Medical Center outpatients and were aware that their progress would be documented in their VA medical record. All gave written, informed consent for participation after the nature of the procedure and the risks and potential benefits had been disclosed to them.
Therapies One week before the first therapy session, a preparatory
session was devoted to rapport building between subject and therapist and training the subject in the procedure. Therapies were performed according to manuals (available on request) prepared separately for two therapy conditions: eye movement (M) and eyes fixed (F). The M therapy used the usual EMDR procedure. 1 The F therapy was identical to the M therapy, with the following exceptions: (1) the therapist continued to perform hand movements as called for in the EMDR procedure, but the subject was instructed to keep his head still and his eyes focused on an indicated spot in front of him during these movements; (2) the therapist observed the subject for compliance with this instruction and immediately corrected him if he started to follow the therapist's hand with his eyes; and (3) instead of eye movements, the subject was instructed to tap his finger rhythmically while the therapist moved his hand back and forth in front of the subject's face.
The therapists were three doctoral-level behavior thera- pists (B.A., R.E.L., and R.E.P.), all of whom had served in our previous PTSD flooding study. 2s The same therapist treated a subject throughout his participation--i.e., in both the M and F therapy conditions. Each therapist completed Dr. Francine Shapiro's beginning and advanced EMDR training seminars and received additional consultation from an expert in the field, Dr. Howard Lipke.
Dr. Lipke rated videotapes of approximately one quarter of the therapy sessions for integrity according to a score sheet (available on request) that used a 0 to 6 scale, with 0 indicating "unacceptable," 1 indicating "marginally accept- able," and 2 to 6 indicating "acceptable" in increasing degrees. Completed score sheets and suggestions for improv- ing the therapy were fed back to therapists as therapy progressed.
Each subject was randomly assigned to either the M or F condition for his first series of weekly therapy sessions, which focused on one of his two reported personal trau- matic combat events selected at random. There followed a second therapy series in the alternate condition focusing on the other reported personal traumatic combat event. The event that served as the focus of a given therapy series is referred to below as the "treated" (trt) event, the remaining event as the "untreated" (untrt) event. A therapy series was completed after six sessions, or after fewer than six sessions if peak SUDS ratings dropped to and remained at zero for two successive sessions.
Therapy Process Variables
Physiologic process variables consisted of HR, SC, EMT- frnt, and left corrugator EMG (EMG-corr), which were obtained according to instrumentation and techniques de- scribed elsewhere. 31,32 SUDS ratings constituted the single nonphysiologic process variable, and was verbally obtained from the subject by the therapist.
Procedure Therapy sessions were held in the psychophysiology
laboratory. On arrival, the technician had the subject empty his bladder and made him comfortable in a reclining chair in a dimly lit, sound-attenuated, temperature-controlled room adjacent to the laboratory housing the recording equip- ment. The technician then attached the recording elec- trodes.
Each session began with 10 minutes of baseline physi- ologic recording. The therapy was initiated by the thera- pist's reading the subject a brief (approximately 30 second) description of the combat event selected for treatment and asking him to visualize its most unpleasant aspect. After this visualization, the subject was asked to rate his SUDS on a 0 to 10 scale. The therapist then ascertained from the subject a negative cognition associated with the scene and an alternate positive cognition the subject would prefer to believe. The subject rated his feeling about "believability" of the positive cognition on a 0 to 10 scale. Therapy was initiated by asking the subject to hold the worst moment from the scene in mind and repeat the negative cognition to himself, while the therapist moved his hand back and forth in front of the patient's face. In the M condition, the patient tracked the therapist's moving hand with his eyes, whereas in the F condition, the patient tapped his fingers with his eyes fixed straight ahead. The patient was then instructed to take a deep breath, blank the scene out, and answer the prompt, "What comes up now?" As new material emerged, the process was repeated, with the therapist obtaining additional SUDS ratings as often as necessary to ascertain the status of the traumatic memory. Hand movements were also performed while the subject focused on the positive cognition. The session was terminated at the therapist's discretion after 70 to 110 minutes, or earlier if the SUDS rating had decreased to 0.
Physiologic variables were recorded continuously during each therapy session. However, to eliminate artifacts in the physiologic (especially facial EMG) data that might be associated with the act of talking, only data obtained from subjects during the therapist hand movement segments (when subjects were silent) were used in the analyses.
Unlike our previous flooding study, 28 and partly in re- sponse to psychiatric complications observed in some of that study's subjects, 33 participants in the present study who expressed concern that the therapy was having negative effects were not specifically encouraged to complete it in the hopes of an eventual positive result.
Therapy Process Measures Therapy process measures were calculated from the
therapy process variables according to a previously de- scribed technique. 28,34 For each process variable, an Activa-

EMOTIONAL PROCESSING DURING EMDR IN PTSD 423
tion ACT score was calculated for the first session of each (M or F) therapy series by subtracting the mean score during the 10-minute baseline recording segment from the mean score for the highest (peak) therapist hand movement segment during the same session. (Baseline SUDS was assumed to be zero, so the peak SUDS value during the session represented the SUDS-ACT score.) WSH was calculated by subtracting the mean score for the final (end) therapist hand movement segment from the peak segment mean score. ASH was calculated by taking the ACT score for the first therapy session of a (M or F) series minus the ACT score for the last session of the same series.
Outcome Measures
Each outcome measure was obtained 1 week before the beginning of the first (M or F) therapy series, between the two therapy series (usually 7 weeks later), and 1 week following completion of the second (F or M) therapy series (usually another 7 weeks later). Outcome measures in- cluded the I O E S y ,36 divided into its intrusion (IOES-int) and avoidance (IOES-avd) subscales, and collected sepa- rately for the subject's two reported personal traumatic combat events; the Mississippi Scale for Combat-Related PTSD37; the Symptom Check List-90-Revised Global Symp- tom Inventory (SCL-90-R GSI)38; the CAPS, 39 scored by an independent doctoral-level psychologist trained in the use of this instrument and blind to therapy condition; and the following additional outcome measure.
During each of the 3 assessment weeks indicated earlier, the subject was provided with a wrist watch programmed to sound a soft alarm at 10 AM, 2 PM, 6 eu, and 10 PM on 3 successive days. Each time the alarm sounded, the subject was instructed to record on a log (available on request) the number of intrusive combat memories that had occurred during the preceding 4 hours. Average number of intrusions per day were calculated and subjected to a square-root transforma- tion in order to reduce skewness and heteroscedasticity.
RESULTS
Course of Treatments
Ten subjects entered their first therapy series in the M condition. Two failed to complete it for nonclinical reasons (i.e., scheduling or availabil- ity problems) and were lost to follow-up. A third subject dropped out after two M sessions be- cause of confusion and frustration with the therapy and was lost to follow-up. Data from these subjects could not be included in the analyses. One subject completed the first M therapy series after four sessions, and five after six sessions. The remaining subject was hospital- ized after four M sessions for increasing depres- sion; data from this subject were retained in the analyses. This subject failed to enter the second therapy series in the F condition, as did two others for nonclinical reasons. The remaining
four subjects entered their second therapy se- ries in the F condition. Three completed it after six sessions. The fourth stopped after four sessions because he was more depressed; his data were retained.
Twelve subjects entered their first therapy series in the F condition. Two failed to complete it for nonclinical reasons and were lost to follow-up. Data from these subjects could not be included. One subject completed the first F therapy series after three sessions, and nine after six sessions. All 10 entered the second therapy series in the M condition. Of these, one completed it after two sessions, one after five sessions, and seven after six sessions. The re- maining subject failed to complete the second therapy series in the M condition for a nonclini- cal reason and was lost to follow-up; his M condition data could not be included.
In summary, of 20 subjects who entered the M therapy condition, two terminated it prema- turely because of negative clinical outcome; of 16 subjects who entered the F therapy condi- tion, one terminated it prematurely because of negative clinical outcome. Three subjects in the M and one in the F condition required less than six sessions to complete the therapy series. Quantitative process and outcome data were available for 17 subjects: 13 in both the M and F therapy series, three in the M series alone, and one in the F series alone. Due to the small sample sizes, data from subjects in both therapy series orders (M-first versus F-first) were com- bined for analyses. Mean number of therapy (M plus F) sessions per subject was 9.7.
Therapy Integrity
The rater assigned a mean overall integrity rating of 3.1 (moderately acceptable; SD, 1.1) to the therapy sessions in the M condition and 2.4 (low acceptable; SD, 1.8) to the therapy sessions in the F condition (t -- 1.1, P, not significant). Unacceptable (0) ratings were assigned to three therapy sessions, all in the F condition. Extracts from the rater's comments on these sessions follow: " . . . the therapist would ask another question instead of doing hand movements with images, sensations, or emotions the subject identified"; "Therapist seemed to be directing the client toward a specific aspect of experience rather than following.., frequently there would
424 P I T M A N ET AL
be reports of decrease in distress, and instead of following with more hand movements the thera- pist would initiate discussion"; "Only did a few sets of hand movements . . , subject reported 0 (SUDS) rating at end of session, but this doesn't fit with tension he had just reported..."
Process Variables and Measures
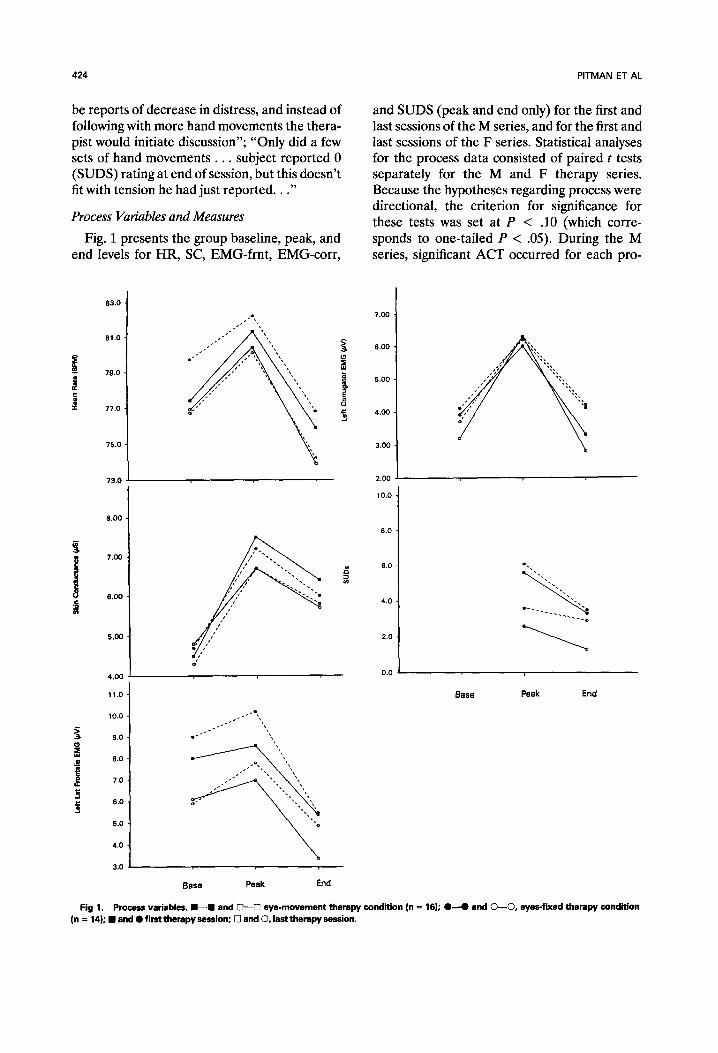
Fig. 1 presents the group baseline, peak, and end levels for HR, SC, EMG-frnt, EMG-corr,
and SUDS (peak and end only) for the first and last sessions of the M series, and for the first and last sessions of the F series. Statistical analyses for the process data consisted of paired t tests separately for the M and F therapy series. Because the hypotheses regarding process were directional, the criterion for significance for these tests was set at P < .10 (which corre- sponds to one-tailed P < .05). During the M series, significant ACT occurred for each pro-
83.0
81,0 .
79.0
J i
77.0
I
75.0
73.0
8.00
7.00
6.00
5.00
4.00
11.0
10.0
9 . 0
8 , 0
7.0
6.0
5.0
4 . 0
3,0
a
"-..~:
e t
e -
Base Peak End
7.00
6.00
5.00
4.00
3.00
2.00
10.0
8.0
8.0
4.0
2.0
0.0
" ' - - - e
Base Peak End
Fig 1. Process variables. I1--11 and [~--[] eye-movement therapy condition (n = 16); e - - O and 0 - - 0 , eyes-fixed therapy condition (n = 14); • and • first therapy session; [] and O, last therapy session.
EMOTIONAL PROCESSING DURING EMDR IN PTSD 425
cess variable except EMG-frnt; significant WSH occurred for each process variable; and signifi- cant ASH occurred for SC and SUDS. During the F series, significant ACT occurred for HR, SC and SUDS; significant WSH occurred for each process variable; and significant ASH oc- curred only for SUDS. Comparisons between the M and F therapy conditions were performed by analyses of variance for repeated measures (ANOVARs), with the criterion for significance set at P < .05. These analyses showed no significant differences between the M and F treatment conditions in ACT, WSH, or ASH for any process variable. Thus, the extent of emo- tional processing did not significantly differ in the M and F conditions.
Outcome Measures
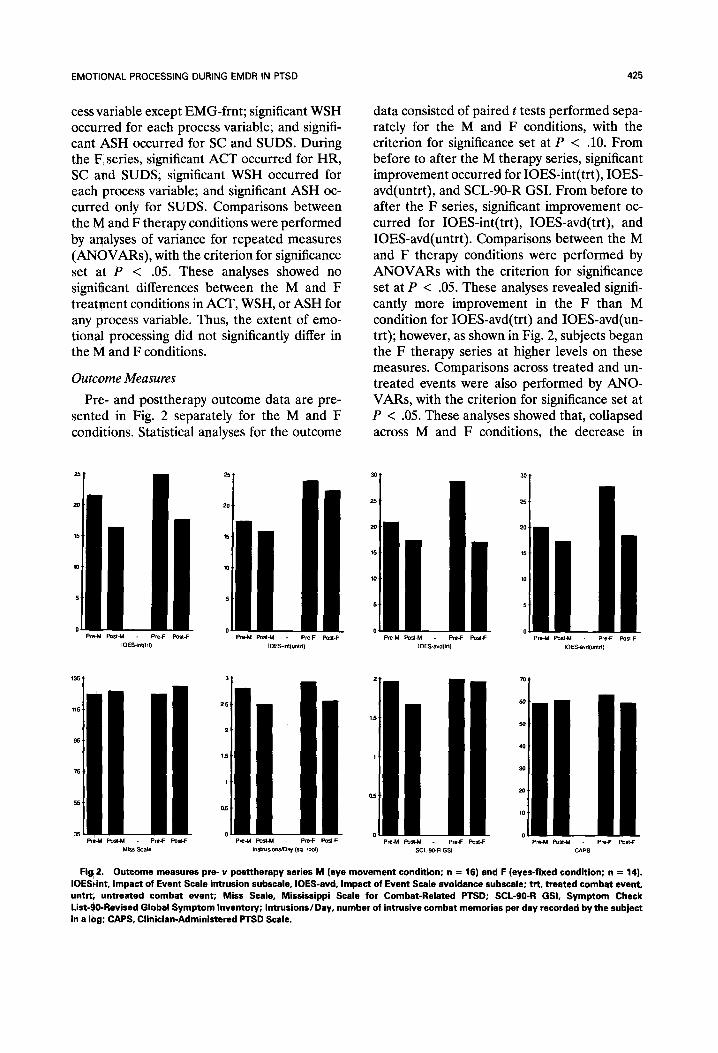
Pre- and posttherapy outcome data are pre- sented in Fig. 2 separately for the M and F conditions. Statistical analyses for the outcome
data consisted of paired t tests performed sepa- rately for the M and F conditions, with the criterion for significance set at P < .10. From before to after the M therapy series, significant improvement occurred for IOES-int(trt), IOES- avd(untrt), and SCL-90-R GSI. From before to after the F series, significant improvement oc- curred for IOES-int(trt), IOES-avd(trt), and IOES-avd(untrt). Comparisons between the M and F therapy conditions were performed by ANOVARs with the criterion for significance set at P < .05. These analyses revealed signifi- cantly more improvement in the F than M condition for IOES-avd(trt) and IOES-avd(un- trt); however, as shown in Fig. 2, subjects began the F therapy series at higher levels on these measures. Comparisons across treated and un- treated events were also performed by ANO- VARs, with the criterion for significance set at P < .05. These analyses showed that, collapsed across M and F conditions, the decrease in
P~-~M Post-M - PreJ = POSt-F Pre44 Post-M Pre~ = PostJ = Pre4*l POSt-M - Pre-F POSt-F IOES~nt(tr t} IOES-~nt(unld) IOES*avd{trt) IOES-avd(untrt)
Pr~M Post-M Pre-F Past4: Pre-M Post4d - Pm-F Post-F Pre-M POst-M PmF POSt4: PreJJ Post-M Pre4: POSt-F MiSS Scale Instrus~o~,sK)ay (sq. root) SCL-90-R GSI CAPS
Fig! 2. Outcome measures pre- v posttherapy series M (eye movement condition; n = 16) and F (eyes-fixed condition; n = 14). IOES~int, Impact of Event Scale intrusion subscale, IOES-avd, Impact of Event Scale avoidance subscale; trt, treated combat event, untrt i untreated combat event; Miss Scale, Mississippi Scale for Combat-Related PTSD; SCL-90-R GSI, Symptom Check List-90-Revised Global Symptom Inventory; Intrusions/Day, number of intrusive combat memories per day recorded by the subject in a 10g; CAPS, Clinician-Administered PTSD Scale.
426 PITMAN ET AL
IOES-int but not IOES-avd was significantly greater for treated than untreated combat events.
Correlations between therapy integrity rat- ings and pre- to posttherapy decreases in out- come measures were examined by means of Pearson product-moment correlations. Because the hypothesis that higher therapy rating would predict more improvement was directional, the criterion for significance for these tests was set at P < .10. There were significant correlations in the predicted direction between therapy integrity and CAPS score (r = .62) and SCL-90- GSI (r = .69) in the M condition, and between therapy integrity and CAPS score (r = .55) and intrusions per day (r = .65) in the F condition.
Process-Outcome Correlations
Analyses of relationships between process and outcome consisted of Pearson product- moment correlations between ACT, WSH, and ASH for the process variables shown in Fig. 1 versus the pre- to posttherapy decreases in the outcome measures shown in Fig. 2. Because of multiple correlations in the matrix, the criterion for significance for these correlations was set at P < .01. In the M condition, there were no significant correlations between process and outcome measures. In the F condition, there was only one significant correlation between SUDS-ASH and pre- to posttherapy decrease in IOES-avd(trt) (r = .73). Across the whole study (i.e., from pre- to post-M and -F therapy in 13 subjects, from pre- to post-M therapy in three subjects, and from pre- to post-F therapy in one subject), there were no significant process- outcome correlations.
DISCUSSION
Emotional Processing
Results of the present study support the occurrence of partial emotional processing of traumatic memories in PTSD combat veterans during EMDR therapy, as manifest in the signifi- cant ACT, WSH, and ASH of SUDS ratings and of some, but not all, physiologic process vari- ables. In contrast to flooding, which emphasizes the need for prolonged, continuous exposure to the traumatic image, 4° the EMDR technique uses multiple, brief exposures, periodically inter- rupted by an instruction to the subject to "blank
it (the image) out." The finding that emotional processing can occur with a technique that allows such interruptions challenges traditional notions that prolonged, continuous exposure is required to achieve extinction of conditioned responses in anxiety disorders such as PTSD.
Data do not support a role for eye movements in emotional processing during EMDR, be- cause there were no significant differences in any of the three process measures for any physiologic or self-reported variables between the EMDR therapy condition that incorporated the usual eye movements and a control condi- tion that kept the eyes fixed and substituted finger tapping for the eye movements. Sha- piro 1,26 has recently suggested that stimuli such as tapping may be considered an alternative to eye movements in the EMDR procedure. She added, "the REM hypothesis and proposed neurologic explanations in no way preclude the use of other external stimuli. ''26 (p. 89) We disagree. Scientific theories are meaningless if they are not falsifiable. The finding that eye movements may be deleted from the EMDR procedure without loss of emotional processing (and therapeutic benefit) necessarily falsifies neurologic (including REM) theories of the role of eye movements in EMDR's mechanism of action. Few scientific theories escape the need for modification with the availability of new data. Continued testing of the contribution of each of its components will allow EMDR to be reduced to its essentials, with the discovery of what is truly useful about this novel procedure. The need for any alternating external stimula- tion at all is a proper topic for research; some studies have found equal benefits without it. 19.20.22 Recently, Shapiro 41 conceded that in light of research developments EMDR is poorly named. We submit that removing the words "eye move- ment" from EMDR's title would bring this therapy in line with current scientific evidence.
Cogent theories of the therapeutic mecha- nism of EMDR have been advanced that are free of neurophysiologic speculation and do not require a critical role for the performance of eye movements. One incorporates principles of re- spondent- and operant-conditioning and emo- tional interference. 42 Another is based on the inhibiting effect of the orienting reflex on condi- tioned responses, the emergence of previously

EMOTIONAL PROCESSING DURING EMDR IN PTSD 427
suppressed, competing responses, and cognitive restructuring. 43 These theories merit further investigation. The contribution of more mun- dane variables such as exposure, distraction, trance, suggestion, and therapist demand char- acteristics 17 should also not be ignored in future research.
Therapeutic Outcome
Outcome measures echo process measures in offering no support for the role of eye move- ments in EMDR's therapeutic effect, given that subjects showed slightly more improvement in the eyes-fixed than in the eye-movement condi- tion. There was an overall 11% average improve- ment across the eight outcome measures shown in Fig. 2 in the eye-movement condition, and a 16% improvement in the eyes-fixed condition. The average overall improvement across all eye-movement and eyes-fixed therapy sessions (9.7 per subject) was a modest to moderate 23%. Similar to other results with EMDR, m treatment effects were greatest for the measure most specifically related to the traumatic event that was the object of therapy--i.e., the IOES. On this instrument's intrusion subscale, there was more improvement for treated than un- treated combat events.
We were surprised that the therapy integrity ratings fell only in the low to moderate accept- able range, considering that the same therapists had previously been rated as highly proficient in the performance of imaginal flooding in the same class of subjects, 28 and they had received more training in the EMDR technique than most therapists who are now performing this procedure. There may be subtleties to EMDR therapy that even experienced behavior thera- pists specially trained to perform it do not readily grasp. However, we cannot believe that our therapists were less proficient in EMDR procedure than practitioners with less experi- ence and training who have reported dramatic benefits with EMDR's use in a single session. Nevertheless, we cannot rule out the possibility tha t the subjects would have shown more im- provement had the therapists performed the therapies with a greater degree of proficiency. This possibility is supported by positive correla- tions between therapy integrity ratings and improvement. However, the frequent SUDS
ratings obtained by the therapists meant that the rater was not entirely blind as to how the therapy was affecting the subjects. It is possible that positive correlations between therapy integ- rity and improvement resulted, at least in part, from a natural propensity on the part of the rater to assign higher integrity ratings to those sessions in which subjects appeared to be re- sponding more to the therapy. It is also puzzling why the subjects should have improved slightly more in the eyes-fixed condition when therapy integrity ratings were slightly higher for the eye-movement condition.
Several factors that may have limited the amount of improvement observed in our previ- ous imaginal flooding study and discussed in detail therein 28 apply equally to the present study. These include the use of subjects who were not treatment-seeking but rather were enrolled by means of an outreach effort, the chronicity of the PTSD and high comorbidity in the subjects treated, and the disincentive for persons receiving compensation to report im- provement. Subjects not encumbered by these factors might well show more substantial im- provement with EMDR, as has been reported in a number of case reports, case series, and studies cited above.
Process-Outcome Relationship
The single significant process-outcome corre- lation, which occurred in the eyes-fixed condi- tion, indicated not surprisingly that subjects who gave lower peak SUDS ratings for a trau- matic combat event during the last (compared to first) therapy session were more likely to show pre- to posttherapy improvement on the IOES-avd for that event. In light of the absence of any other significant correlations between process and outcome measures, the overall results provide little support for the hypothesis that extent of emotional processing would pre- dict amount of improvement.
Comparison With Imaginal Flooding
Although they were not comprised within the same experiment, the similarity of methodolo- gies used in our previous imaginal flooding study 28 and the present study allows informal comparisons between the results of these two therapeutic approaches to chronic, combat-

428 PITMAN ET AL
related PTSD in the hands of the same thera- pists and investigators. A comparison of the process data of the two studies suggests that roughly comparable amounts of emotional pro- cessing took place with EMDR and imaginal flooding. The overall 23% improvement ob- served in the present study over a mean of 9.7 EMDR (eye-movement and eyes-fixed) therapy sessions is greater than the overall 13% improve- ment in PTSD combat veterans treated by the same therapists over a mean of 10.2 sessions of imaginal flooding. However, unlike the present EMDR study, subjects in our flooding study may have been handicapped by prior with- drawal from their psychotropic medication. Al- though inferences from mean improvement cal- culations are limited by the use of different outcome measures across disparate studies, they do allow a rough comparison of the outcome of EMDR in the present study compared with outcome in another study of Vietnam combat veterans using implosive (flooding) therapy. 44 In that study, overall pre- to posttherapy improve- ment over 14 to 16 sessions of implosive therapy (calculated by averaging the outcome measures appearing in Figs. 1 and 2 on pp. 251-252 of that publication) was 28%. These comparisons sug- gest that EMDR is about as efficacious as more traditional exposure therapy for combat-related PTSD. Other investigators have come to a
similar conclusion based on preliminary results of an ongoing study comparing these two ap- proaches. 45
Flooding has been criticized because of the high, lengthy anxiety it produces, with EMDR offered as an alternative. 46 We found EMDR to be less anxiety-provoking for patients (as well as therapists), better tolerated, and productive of fewer adverse complications than flooding. 33 For these reasons, and because it supplements exposure with an explicit cognitive component that may be important in the therapy of PTSD, based on our experience, we would prefer EMDR over imaginal flooding in the treatment of chronic, combat-related PTSD. However, we believe that further research is necessary to identify which specific components of each of these and other psychotherapeutic approaches to PTSD are necessary and/or sufficient for optimal improvement, and which are unneces- sarily stressful or superfluous and may be dis- carded.
ACKNOWLEDGMENT
Dr. Howard Lipke collaborated on writing the treatment manuals used in this work, consulted with the therapists in the implementation of the EMDR technique, and per- formed the therapy integrity ratings. Dr. Natasha Lasko performed the diagnostic assessments. Heike Croteau pro- vided technical assistance.
REFERENCES 1. Shapiro F. Eye Movement Desensitization and Repro-
cessing: Basic Principles, Protocols, and Procedures. New York, NY: Guilford, 1995.
2. Shapiro F. Eye movement desensitization: a new treatment for post-traumatic stress disorder. J Bebav Ther Exp Psychiatry 1989;20:211-217.
3. Marquis JN. A report on seventy-eight cases treated by eye movement desensitization. J Behav Ther Exp Psychiatry 1991;22:187-192.
4. Lipke H J, Botkin AL. Case studies of eye movement desensitization and reprocessing (EMDR) with chronic post-traumatic stress disorder. Psychotherapy 1992;29:591- 595.
5. Vaughan K, Wiese M, Gold R, Tarrier N. Eye- movement desensitization symptom change in post-trau- matic stress disorder. Br J Psychiatry 1993;164:533-541.
6. Goldstein AJ, Feske R. Eye movement desensitization and reprocessing for panic disorder: a case series. J Anxiety Disord 1994;4:351-362.
7. Forbes D, Creamer M, Rycrofl P. Eye movement desensitization and reprocessing in posttraumatic stress disorder: a pilot study using assessment measures. J Bebav Ther Exp Psychiatry 1994;25:113-120.
8. Shapiro F. Efficacy of the eye movement desensitiza- tion procedure in the treatment of traumatic memories. J Trauma Stress 1989;2:199-233.
9. Silver SM, Brooks A, Obenchain J. Treatment of Vietnam war veterans with PTSD: a comparison of eye movement desensitization and reprocessing, biofeedback, and relaxation training. J Trauma Stress 1995;8:337-342.
10. Wilson SA, Becker LA, Tinker RH. Eye movement desensitization and reprocessing (EMDR) treatment for psychologically traumatized individuals. J Consult Clin Psychol 1995;63:928-937.
11. Boudewyns PA, Stwertka SA, Hyer LA, Albrecht JW, Sperr EV. Eye movement desensitization for PTSD of combat: a treatment outcome pilot study. Behav Therapist 1993;16:29-33.
12. Jensen JA. An investigation of eye movement desen- sitization and reprocessing (EMD/R) as a treatment for posttraumatic stress disorder (PTSD) symptoms of Vietnam combat veterans. Behav Ther 1994;25:311-325.
13. Oswalt R, Anderson M, Hagstrom K, Berkowitz B. Evaluation of the one-session eye-movement desensitiza- tion reprocessing procedure for eliminating traumatic memo- ries. Psychol Rep 1993;73:99-104.

EMOTIONAL PROCESSING DURING EMDR IN PTSD 429
14. Herbert JD, Mueser KT. Eye movement desensitiza- tion: a critique of the evidence. J Behav Ther Exp Psychiatry 1992;23:169-174.
15. Lohr JM, Kleinknecht RA, Conley AT, Dal Cerro S, Schmidt J, Sonntag ME. A methodological critique of the currenlt status of eye movement desensitization (EMD). J Behav Ther Exp Psychiatry 1992;23:159-167.
16. Ellard J. Eye movement desensitization. Aust N Z J Psychiatry 1993;27:535.
17. Shapiro F. Eye movement desensitization & reprocess- ing procedure: from EMD to EMD/R--a new treatment model for anxiety and related traumata. Behav Therapist 1991;14:133-135.
18. Smith C. Sleep states and learning: a review of the animal literature. Neurosci Biobehav Rev 1985;9:157-168.
19. Sanderson A, Carpenter R. Eye movement desensiti- zation versus image confrontation: a single-session cross- over study of 58 phobic subjects. J Behav Ther Exp Psychiatry 1992;23:269-275.
20. Renfrey G, Spates CR. Eye movement desensitiza- tion: a partial dismantling study. J Behav Ther Exp Psychia- try 1994;25:231-239.
21. Bauman W, Melnyk WT. A controlled comparison of eye movements and finger tapping in the treatment of test anxiety. J Behav Ther Exp Psychiatry 1994;25:29-33.
22. Tallis F, Smith E. Does rapid eye movement desensi- tization facilitate emotional processing? Behav Res Ther 1994;32:459-461.
23. Montgomery RW, Ayllon T. Eye movement desensiti- zation across subjects: subjective and physiological mea- sures of treatment efficacy. J Behav Ther Exp Psychiatry 1994;25:217-230.
24. Hekmat H, Groth S, Rogers D. Pain ameliorating effect of eye movement desensitization. J Behav Ther Exp Psychiatry 1994;25:121-129.
25. Foa EB, Kozak MJ. Emotional processing of fear: exposure to corrective information. Psychol Bull 1986;99:20- 35.
26. Shapiro F. Alternative stimuli in the use of EMD(R). J Behav Ther Exp Psychiatry 1994;25:89.
27. Spitzer RL, Williams JBW. Structured Clinical Inter- view for DSM-III-R. New York, NY: Biometrics Research Department, New York State Psychiatric Institute, 1987.
28. Pitman RK, Orr SP, Altman B, Longpre RE, Poire RE, Macklin ML, et al. Emotional processing and outcome of imaginal flooding therapy in Vietnam veterans with chronic post-traumatic stress disorder. Compr Psychiatry 1996;37:409-418.
29. Egendorf A, Kadushin C, Laufer RS, Rothbart G, Sloan L. Legacies of Vietnam: Comparative Adjustment of Veterans and their Peers. Washington, D.C.: US Govern- ment Printing Office, 1981.
30. Keane TM, Fairbank JA, Caddell JM, Zimering RT, Taylor KL, Mora CA. Clinical evaluation of a measure to assess: combat exposure. Psychol Assess 1989;1:53-55.
31. Pitman RK, Orr SP, Forgue DF, de Jong JB, Claiborn JM. Psychophysiologic assessment of post-traumatic stress
disorder imagery in Vietnam combat veterans. Arch Gen Psychiatry 1987;44:970-975.
32. Pitman RK, Orr SP, Forgue DF, Altman B, de Jong JB, Herz LR. Psychophysiologic responses to combat imag- ery of Vietnam veterans with post-traumatic stress disorder versus other anxiety disorders. J Abnorm Psycho11990;99:49- 54.
33. Pitman RK, Altman B, Greenwald E, Longpre RE, Macklin ML, Poire RE, et al. Psychiatric complications during flooding therapy for post-traumatic stress disorder. J Clin Psychiatry 1991;52:17-20.
34. Kozak M J, Foa EB, Steketee G. Process and outcome of exposure treatment with obsessive-compulsives: psycho- physiological indicators of emotional processing. Behav Ther 1988;19:157-169.
35. Horowitz M, Wilner N, Alvarez W. Impact of Event Scale: a measure of subjective stress. Psychosom Med 1979;41:209-218.
36. Zilberg NJ, Weiss DS, Horowitz MJ. Impact of Event Scale: a cross-validation study and some empirical evidence supporting a conceptual model of stress response syn- dromes. J Consult Clin Psychol 1982;50:407-414.
37. Keane TM, Caddell JM, Taylor KL. Mississippi Scale for Combat-Related Posttraumatic Stress Disorder: three studies in reliability and validity. J Consult Clin Psychol 1988;56:85-90.
38. Derogatis LR. SCL-90-R: Administration, Scoring & Procedures Manual-II for the R(evised) Version. Towson, MD: Clinical Psychometric Research, 1983.
39. Blake DD, Weathers FW, Nagy LM, Kaloupek DG, Gusman FD, Charney DS, et al. The development of a clinician-administered PTSD scale. J Trauma Stress 1995;8: 75-90.
40. Lyons JA, Keane TM. Implosive therapy for the treatment of combat-related PTSD. J Trauma Stress 1989;2: 137-152.
41. Shapiro F. Eye movement desensitization and repro- cessing: evidence pro and con (discussion). Washington, DC: American Psychiatric Association Syllabus and Proceed- ings Summary 1995;148:166-167.
42. Dyck MJ. A proposal for a conditioning model of eye movement desensitization treatment for posttraumatic stress disorder. J Behav Ther Exp Psychiatry 1993;24:201-210.
43. Denny NR. An orienting reflex/external inhibition model of EMDR and thought field therapy. Traumatology: The E-Journal 1, Article 2, 1995.
44. Keane TM, Fairbank JA, Caddell JM, Zimering RT. Implosive (flooding) therapy reduces symptoms of PTSD in Vietnam combat veterans. Behav Ther 1989;20:245-260.
45. Boudewyns PA, Hyer LA, Peralme L, Touze J, Kiel A. Eye movement desensitization for combat-related PTSD: an early look. Washington, DC: American Psychiatric Asso- ciation 1995 Annual Meeting Syllabus and Scientific Pro- ceedings Summary 1995;148:167.
46. Spector J, Huthwaite M. Eye-movement desensitiza- tion to overcome post-traumatic stress disorder. Br J Psychia- try 1993;163:106-108.





























