Embed Size (px)
Citation preview

Emerging ID issues:Drug Resistant Bacteria &
Spreading Viruses
Paul S. Sehdev, MD, MS, FACP, FIDSAInfectious Disease Consultants &
The Traveler’s ClinicProvidence St. Vincent’s Hospital
October 14, 2011

Trends in S. aureus Disease• Emergence of MRSA• Emergence of VISA• Emergence of VRSA• Emergence of hVRSA• Community acquired MRSA• Resistance to new agents
• Linezolid • Daptomycin

Emergence of Methicillin Resistance
• 1961: Methicillin introduced• 1962: MRSA identified• 1980: 5-10% hospital isolates MRSA• 1991: 25% hospital isolates MRSA• 2003: 64% isolates in NNISS
Chambers. Emerg Inf Dis;7:178

Methicillin Resistance: Mechanism• MecA gene
– Encodes a low affinity PBP (PBP2a)– Affects all -lactam drugs– 5 types
• Variable patterns of drug susceptibilities
– Acquired from unknown locus– Mobile transposon-like element – Resistance profiles continue to change

http://phsnet.phsor.org/laboratory/micro/antibiotics/QTR%204%202008PSVMCMRSA.pdf

What is an Extended-Spectrum -Lactamase (ESBL)?
• Variant of standard TEM & SHV -lactamases• Result of point mutations • Mutated -lactamase has extended spectrum
• Degrades 3rd generation cephalosporins
• Transmitted via plasmids• Over 150 ESBLs identified to date• E.Coli & K.pneumoniae
Rice LB. Pharmacotherapy. 1999;19(8 Pt 2):120S.

Molecular Basis of ESBLsAmino Acid Position
EnzymeCTZ MIC
102 162 237
TEM-1 <0.12 Glu Arg Glu
TEM-12 4-32 Glu Ser Glu
TEM-10 64 Glu Ser Lys
TEM-26 >256 Lys Ser Glu
Rice LB. Pharmacotherapy. 1999;19(8 Pt 2):120S.

ESBLs Detection Methods: Inhibition by Clavulanic Acid

Inoculum Effect in K. pneumoniae Isolates Containing ESBLs
Antibiotic
MIC90 (g/mL)
105 CFU/mL % Susceptible
107 CFU/mL % Susceptible
Meropenem 0.06 100 4 100
Cefotetan 1 100 16 90
Ceftazidime 1,024 11 >1,024 5
Cefotaxime 32 67 >1,024 5
Ceftriaxone 64 56 >1,024 0
Cefepime 16 89 >128 0
Pip/Tazo 1,024 67 >1,024 22
Thomson KS. Antimicrob Agents Chemother. 2001;45:3548.

Therapy of ESBL Infections• Carbapenems best option • Cephalosporins:
– In vitro & in vivo discordance– Failure of Ceftazidime in bacteremic patients– Reports of Ceftriaxone & Cefotaxime success
• Meningitis and bacteremia• Few patients
• Little data • Trimethoprim/ sulfamethoxazole• Aminoglycosides• Fluoroquinolones
Wong-Beringer A. Pharmacotherapy 2001;21:583.

This is Neisseria gonorrhea

Resistance in N.gonorrhea
• Emerged in 1970’s• Penicillin resistance• Tetracycline resistance
• DOC in 1980’s became ciprofloxacin• Fluoroquinolone resistance emerged
– AsiaHawaii Californiaeverywhere else• 2007, CDC recommended cephalopsorins
• Ceftriaxone im or cefixime

N. gonorrhea: Cephalosporin Resistance 2000-2010
www.cdc.gov/mmwr/preview/mmwrhtml/mm6026a2.htm?s_cid=mm6026a2_w#fig2

New kid on the block:New Delhi metallo-ß-lactamase-1 (NDM-1)
• 2009, first report• UTI after travel to India• Isolate was K. pneumoniae• Resistant to all beta-lactam drugs• E.coli possessing NDM-1 found in patient’s stool
• 2010 USA• 3 cases with 3 different organisms
• 2011 Cases on all continents• Except Antarctica & S. America

NDM-1
• Encodes for broad spectrum B-lactamase• Resistant to all B-lactam drugs• Sensitive to tigecycline & colistin
• Resides on a plasmid• Transferable between bacteria
• Within a species• Across species
• Prevalence rates• USA low• India 4% of enteric Gram-negative bacilli

Why the easy spread?Horizontal transfer

NDM-1: It’s in the water
• Prevalence study from New Dehli, India• September-October 2010
• Sampled water • Seepage (puddles & rivulets)• Public tap water
• 221 samples (171 seepage & 50 tap H2O• 51 of 171 (29%) & 2 of 50 (4%) positive• 11 different bacteria possessed• Including V. cholera & Shigella species
• Huge implications for developing world • Worldwide interconnectedness makes further spread likely
http://www.ncbi.nlm.nih.gov/pubmed/21478057
Containing NDM-1
• This will NOT just go away!• Infection control is paramount
• High index of suspicion• Contact isolation• Good hand hygiene• Active surveillance
• Limiting broad spectrum antibiotic use• Reduces “pressure” that enables resistant bugs to thrive
• Reserve active agents• Few (no?) new antibiotics in pipeline
Chickungunya

Chikungunya Background
• 1st described in 1952– Outbreaks of febrile polyarthritis
• Makonde word– “that which contorts or bends up”
• Virus was isolated in 1953• Spread throughout South-Central Africa• Spread to Thailand in 1958• Now, endemic in S. Asia• Indian Ocean outbreak ongoing since 2004

Indian Ocean Outbreak
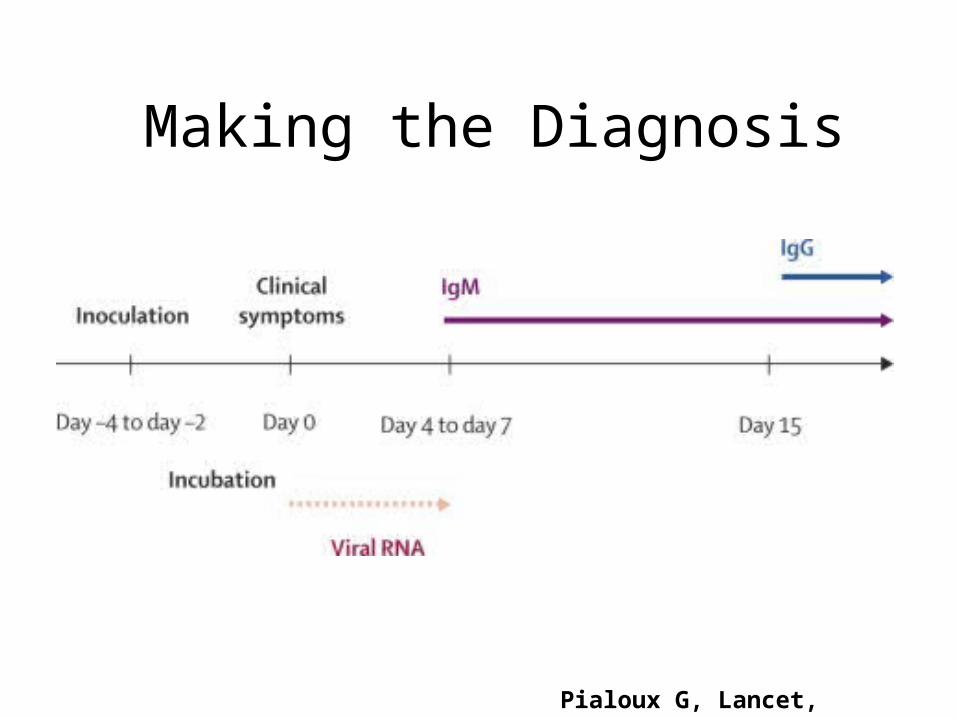
Pialoux G, Lancet, 2007;7:319-27

Epicurves Reunion & France
Pialoux G, Lancet, 2007;7:319-27


Clinical Manifestations• Primary infection features
– Fever 86-100%– Arthralgias 96-100%
• Hands, wrists & ankles– Headache 47%– Rash 40%
• Secondary – Chronic polyarthralgia 5-10%– Persists for months to years– Mechanism for disease unknown
• Mortality <1%
Simon F, Med Clin N Am 2008;92:1323-43

Simon F, Med Clin N Am 2008;92:1323-43
Clinical Manifestations
Pialoux G, Lancet, 2007;7:319-27
Making the Diagnosis

Treatment & Prevention
• Supportive therapy• DEET to repel mosquitoes• Vaccine
• Live attenuated vaccine candidate (TSI-GSD-218)• Phase II trials• Single dose vaccine• 98% developed neutralizing antibody at day 28• 85% remained sero-positive at 52 weeks• Trials shelved in 2002
• Future uncertain
Edelman R, Am J Trop Med Hyg 2000;62(6):681-5


Dengue Viruses• Flavivirus
• Single stranded, nonsegmented RNA virus
• 4 distinct serotypes• Each serotype provides lifelong immunity• Infection does not confer cross protection• All can cause severe manifestations• Can be infected up to 4 times• Subsequent infections may be severe
• Main reservoir is humans• Non-human primates may be infected
Dengue Disease Burden
• Most common arboviral disease• Endemic in 100 countries• 2.5 billion persons at risk• 100 million cases yearly• 250,000 cases of Dengue hemorrhagic fever• 25,000 deaths yearly

Aedes Mosquitoes
• Highly susceptible to Dengue infection• Preferred nourishment is human blood• Thrives in urban environments• Bites during daytime• Bite is nearly imperceptible• May bite several people to obtain a blood meal

Spread & Distribution of Dengue
http://www.who.int/csr/disease/dengue/impact/en/

Dengue in Puerto Rico 2009-11

Dengue Clinical Syndromes
• Undifferentiated fever• Classic dengue fever• Severe Dengue
– Dengue hemorrhagic fever– Dengue shock syndrome

Classic Dengue Fever• Sudden onset fever • Headache & retro-orbital pain• Severe myalgia & arthralgia
• “Break-bone fever”
• Skin rash• Appears around time of defervescence
• Mild hemorrhagic manifestations• Tourniquet tests
• Laboratories• Leukopenia, lymphopenia & thromobocytopenia• Transaminitis

Wilder-Smith A and Schwartz E. N Engl J Med 2005;353:924-932
Tourniquet Test

Chikungunya vs. DengueChikungunya Dengue
Fever Common Common
Rash Day 1-4 Day 3-7
Retro-orbital pain Rare Common
Myalgia Possible Very common
Polyarthritis Very common None
Tenosynovitis Common None
Hypotension Possible Common
Minor Bleeding Possible Common
Sequalae Chronic polyarthritisTenosynovitisRaynaud’s
Fatigue

Dengue Hemorrhagic Fever: CDC Case Definition
• 4 criteria—must meet all• Fever• Hemorrhagic manifestations• Platelet count <100,000/mm3 • “Leaky capillaries”
• Hematocrit >20% above baseline)• Low albumin• Pleural or other effusions

Dengue Shock Syndrome• 4 criteria for DHF plus• Circulatory failure:
• Rapid and weak pulse• Pulse pressure < 20 mm Hg• SBP <90 mmHg
• Duration of shock is short• 12-24 hours• Supportive care only intervention
• Morality ranges from 0.2%-20%• 2 deaths in USA from 1993-2000

DHF Mechanism
• Antibody mediated enhancement• Cross reacting Abs bind virus• They do no neutralize bound virus• Complexes bind Fc receptors• Replicate in dendritic cells & macrophages• Viral load is increased• Killer cells & T-cell are activated• “Cytokine storm” ensues• Endothelial damage & capillary leakage

Wilder-Smith A and Schwartz E. N Engl J Med 2005;353:924-932

Dengue Prevention
• Insect precautions are mainstay• Vaccines
– 2 candidates in phase 2-3 trials• Both live attenuated viruses• Both tetravalent vaccines• Immunogenic, but not reactogenic• Field trials in planning stages
• Vector control• Must be multi-modal

Sehdev P Clin Inf Dis 2002;35(9):1071–1072

Yellow Fever• 1st outbreak in New World 1648• Yet, thought to originate from Africa• Global epidemics
• 1793: Philadelphia 10% population died• 1878: Mississippi Valley 100,000 cases
• Sanitary measures reduced burden• Serendipitous• Vector was not known at time
• Virus isolated in 1927• Vaccine developed in 1928

Yellow Fever Map 2007
http://www.cdc.gov/ncidod/dvbid/yellowfever/YF_GlobalMap.html

Estimated Disease Burden
• 200,000 cases per year• 30,000 deaths• Epidemic attack rates
• 30 cases per 1,000 persons
• Case fatality rates• 20-50% in endemic areas
• Imported cases rare, but deadly• 6 cases USA & Europe 1996-2004
http://wwwn.cdc.gov/travel/yellowbook/ch4/yellow-fever.aspx

YF Transmission Cycle
Monath TP, Lancet ID 2001;1:11-20

Stages of Yellow Fever
Monath TP, Lancet ID 2001;1:11-20

Diagnosis & Treatment
• Mainstay is serology• Single positive IgM • Fourfold rise in IgG titer
• PCR positive early (days 1-6)• But, not readily available
• Culture is gold standard• Therapy is supportive
• Ribavirin has been tried, but doesn’t work• Immunoglobulin not useful

Yellow Fever Vaccine• Live, attenuated virus (17D strain)• 95% effective, 10 year protection• HA, fever & myalgia• Immediate hypersensitivity (1/131,000)• Vaccine associated neurotrophic disease
– 16/23 case age < 9 months• Vaccine associated viscerotropic disease
– 10 cases since 1996• Contraindications
– Egg allergy & age < 9 months
MMWR 2002;51:RR-17





























