Embed Size (px)
Citation preview

Article ID: WMC003342 ISSN 2046-1690
Emerging and Re-emerging Infectious Diseases:Hepatitis C
Corresponding Author:Ms. Zainab Shakoor,Medical Student, Liverpool - United Kingdom
Submitting Author:Mr. Muhammed R Siddiqui,Registrar, Mayday Hospital, 23 Malvern Road, TN24 8HX - United Kingdom
Article ID: WMC003342
Article Type: Review articles
Submitted on:08-May-2012, 02:56:26 AM GMT Published on: 08-May-2012, 08:32:25 PM GMT
Article URL: http://www.webmedcentral.com/article_view/3342
Subject Categories:INFECTIOUS DISEASES
Keywords:Infectious diseases; Hepatitis C
How to cite the article:Shakoor Z, Siddiqui MR. Emerging and Re-emerging Infectious Diseases: Hepatitis C .WebmedCentral INFECTIOUS DISEASES 2012;3(5):WMC003342
Copyright: This is an open-access article distributed under the terms of the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the originalauthor and source are credited.
Source(s) of Funding:
None
Competing Interests:
None
Webmedcentral > Review articles Page 1 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
Emerging and Re-emerging Infectious Diseases:Hepatitis CAuthor(s): Shakoor Z, Siddiqui MR
Abstract
Aim: To explore new developments in anti-viraltherapy used to treat hepatitis C.
Background: Hepatitis C is a blood-borne viruscurrently affecting 175 million people worldwide.Infection with the virus can predispose to chronicinfection, cirrhosis and hepatocellular carcinoma. Thevirus can be contracted through exposure with ahepatitis C infected person’s blood. Intravenous druguse is the most common mode of transmission. Thoseinfected with the virus may experience vaguesymptoms such as malaise and fatigue, or they mayshow symptoms of liver disease or any othercomplications of the infection. As symptoms may benon-specific and are not often detected in the earlystages of infection the hepatitis C virus (HCV) is in thissense known as a silent killer, as the liver may beextensively damaged before infection with the virus isdetected. Anti-viral therapy for treating chronichepatitis C currently remains the only option inpreventing cases of liver cirrhosis and hepatocellularcarcinoma. Currently no vaccines have beendeveloped.
Method: An insight and understanding of HCV wasgained by using books, journals and the internet.Electronic databases used were used to conduct aliterature search for articles regarding the developmentof anti-viral drugs; the outcome of this is shown in theresults table. An inclusion and exclusion criteria wasapplied to the articles generated and the most suitablearticles were selected for discussion.
Results: The results of almost all of the anti-viral drugsresearched were successful in attaining a decrease inthe HCV RNA levels and achieving a sustained viralresponse.
Conclusion: The results of the clinical trials researchedshow some promise for future developments inanti-viral therapy. A successful treatment regime whichcan eliminate the hepatitis C virus is in great demand,given the substantial amount of morbidity and mortalitycaused by the virus.
Introduction
Aim: To investigate new developments in anti-viraltherapy used to treat hepatitis C.
Infectious diseases are defined as diseases which are caused by “pathogenic microorganisms, such asbacteria, viruses, parasites or fungi; the diseases canbe spread, directly or indirectly, from one person toanother”(1). Emerging infections such as hepatitis C may emerge in a new population or area or may be recognized in a changing environment. Theymay also be caused by changes in the currentmicroorganisms or become identified by the realizationthat they are a cause of a known chronic disease (2). The burden of infectious diseases is significant with20% of deaths worldwide and a staggering 50% inAfrica due to infectious causes (3).
Hepatitis C emerged in 1989 as non A-non B hepatitisafter the virus was identified and cloned as the causeof most cases of post -transfusion of hepatitis (4).Contracting the virus can lead to fibrosis, cirrhosis andhepatocellular carcinoma (HCC) of the liver.Transmission of hepatitis C (HCV) is mostly parenteralas it is a blood borne virus and because of this, 90% ofintravenous drug users are at greater risk ofcontracting the virus (5).
HCC is the sixth most common cause of cancerworldwide, and the third most common cause ofcancer death. It is the leading cause of liver diseasein the United States of America (6). These studieshave also suggested that over the next two decadesthe number of deaths caused by hepatitis C infectionwill continue to increase. Therefore it is vital that stepsare taken to help reduce transmission of HCV andtreatments derived to help treat those who are infectedby either clearing the virus or supressing it to delay theprogression of liver disease.
Epidemiology
The WHO estimates that the global disease burden ofhepatitis C is 175 million worldwide, this reflects 3% ofthe world’s population. Each year a staggering 3-4million people are infected with the virus (5). Recentdata shows that 100,000 of
250,000 people affected in the UK are unaware oftheir infection with HCV (7).
Webmedcentral > Review articles Page 2 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
Hepatitis C is a widespread with over 130 countriesreporting cases of the infection. There is significantvariation of the virus worldwide, thus demonstratingthe virus? high mutation rate and rapid evolution. Lessdeveloped countries such as Southern Europe, Africaand Egypt report higher incidence rates, compared tonorthern European countries with the lowest levels,such as Great Britain, Germany and France (4).
The virus has 6 different genotypes classified from oneto six, with seventy subtypes (3). The genotypes varysignificantly in their geographical prevalence (8).Genotype 1 is most common with 40-50% of all HCVinfected patients in the UK with this genotype (9).There may be some overlap in features betweengenotypes and infection with two strains at the sametime or re-infection with the same strain is alsopossible (10). Differences between genotypes may bepresent in terms of their replication method. Otherdifferences may be their mutation rate and the typeand severity of liver damage that can be detected orcaused (4). As the virus mutates easily duringreplication, any antibodies produced in response toone strain do not provide protection for other strains aperson may become infected with because it is anRNA virus with many different serotypes, causingdifficulties in developing vaccines (11).
Classification of Hepatitis C
All the hepatitis viruses have an RNA genome, apartfrom hepatitis B which contains DNA. The hepatitisviruses all belong to different families. Hepatitis C is amember of the
Flavivirdae family and the Hepacivirus genus (13).
Virology
Hepatitis C is a small spherical virus. The moleculehas a diameter of 50nm, whilst the diameter of thecore RNA strand is 30nm3. A single strand of RNAwith positive ending polarity is enveloped by thenucleocaspid, which is the virus? protein coat (15).The virus is isohedral and many small surface bindingproteins such as the glycoproteins E1 and E2 projectfrom its surface (3).
Signs and Symptoms
Acute hepatitis C is defined as infection within 6months of contracting the hepatitis c virus. If HCV haspersisted for more than 6 months, this is classed aschronic HCV infection (17). Only 10% of those infectedwill show symptoms in the acute phase (18). An
acute symptomatic period is rare, whilst a longasymptomatic period is common (19). In this sense thevirus was named the ‘silent epidemic’ as the cause ofany symptoms experienced are often not detected
until a significant time after contracting the virus,because they are often rare, mild and non-specific andat this point the liver may already have beenextensively damaged. Patients may be diagnosedincidentally by routine tests or after investigating anysymptoms they may have experienced. 80% of thoseinfected with HCV will develop chronic hepatitis,regardless of the mode of onset (20). Symptoms suchas fatigue can complicate chronic infection, althoughthis does not correlate with the extent of liver damage.Symptoms of cirrhosis or liver disease may alsocomplicate HCV infection (18). Extra-hepaticmanifestations such as skin rashes, diarrhoea, arthritisand various auto-immune diseases may also beexperienced by some patients (21).
Transmission of Hepatitis C
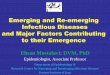
Hepatitis C can be transmitted by various methods asshown in table 1:
Diagnosis
The following diagnostic tests may be performed onindividuals at risk or suspected to have contractedhepatitis C.
Immunoblotting and „ELISA? tests may be conductedinitially to detect the presence of antibodies in infectedpeople with the HCV protein. There is a window periodof 6 to 12 weeks following acute infection until theseantibodies may be detected although these antibodiesmay spontaneously persist in the blood stream afterthe virus has been cleared or following treatment (18).Immunoglobulin M (Ig M) anti HCV antibodiessuggests acute infection, whilst Ig G antibodiesindicate past exposure or chronic infection (23). Liverfunction tests (LFTs) may also be conducted. Serumtransaminases levels may be normal or fluctuatebetween 50-200U/L, although they have no correlationwith histological changes (18).
The presence of HCV RNA in a patient’s serumindicates that there is on-going infection with hepatitisC. Testing the genome confirms the results of antibodytesting or is used to test those suspected to havecontracted the virus but who have negative serology(18,19).
A liver biopsy may be performed to more accuratelyidentify the extent of fibrosis and cirrhosis as serumtransaminase levels are a poor reflection of theamount of fibrosis. Monitoring liver cirrhosis patientswho are at risk of developing hepatocellular carcinomacan also be done (18) The Metavir system iscommonly used as a non-invasive method ofassessing liver fibrosis (19).
Molecular analysis is used to identify which hepatitis C
Webmedcentral > Review articles Page 3 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
genotype a patient is infected with. This is helpful indetermining the most suitable treatment as thetreatment response depends on the genotype.However it doesn’t predict the effect of infection or theprogression of liver disease varies worldwide.
An ultrasound of the liver may also be conducted toassess the extent of cirrhosis and therefore is useful inmonitoring patients chronic HCV who are at risk ofdeveloping cirrhosis.
Treatment
Current treatment will be discussed later (6). Anti-viraltherapy is used to eliminate HCV and clearance of thevirus is indicated when HCV RNA levels remainundetectable in an infected person’s serum 6 monthsafter therapy (8). The level of treatment a patientreceives depends on the nature of the infection i.e.acute or chronic, and the progression and severity ofliver disease. The rate of disease progressiondepends on the viral load and genotype of HCV,amongst other factors such as alcohol. Early treatmentis another factor which can impact the effectiveness ofviral clearance or suppression and delay diseaseprogression in those who HCV clearance cannot beachieved (11).
Management for acute HCV infection is mainlyfocused on patient education, advice and support.Symptoms such as fever which may be experiencedwill be treated with medication (10).
The treatment of choice currently used andrecommended by the National Institute of ClinicalExcellence (NICE) is pegylated-interferon incombination with ribavirin, for mild to severe chronichepatitis C (11).
Interferon molecules are glycoproteins which areconsidered as the “backbone” of anti-viral therapy (5).They increase the immune response against HCV,and have anti- viral and anti-proliferative effects incells (23). The pegylated interferon molecule is formedby a covalent bond between a polyethylene glycol andinterferon molecule. The addition of polyethyleneglycol increases the half-life of the interferon, leadingto sustained plasma levels, fewer adverse effects andbetter efficiency compared to interferon monotherapy(5,8). Once weekly subcutaneous injections are onlyneeded so current therapy is more convenient.Ribavirin is a guanosine analogue which is alwaysused in combination with other anti-viral drugs as itincreases the sustained viral response (SVR) of thetreatment. It is taken twice a day and the dose isadjusted according to weight.
Patients with the HCV genotype 1, 4, 5 or 6 areadvised to take treatment for 48 weeks. Those with
genotypes 2 and 3 show better responses to treatmenttherefore only need therapy for 24 weeks. 50% of HCVgenotype 1 patients achieve an SVR of 50%,compared to 80% achieved by those with genotype 2or 3 (25).
During treatment blood tests may be conductedregularly to ensure the patient is stable whilst on thetreatment. Regular monitoring of HCV RNA is donethroughout therapy and weekly full blood counts areconducted weekly in the first month of treatment andthyroid function tests are done every 3 months (10).
Over half of the patients taking combination therapywill experience side effects. Doses may need to bereduced so that the efficiency of treatment is notimpaired.
Complications
Chronic hepatitis C carriage, liver cirrhosis or HCC arethe most common complications of HCV. Hepaticfailure in the acute phase affects 0.5% of thoseinfected (18). Other complications which may beexperienced are very rare, such as dryness of themouth and eyes, lichen planus, glomerulonephritis andsensitivity to light. Changes in the thyroid gland activity,insulin resistance, diabetes, gallbladder disease,cryoglobulinaemia and non-Hodgkin’s lymphoma maybe experienced (26).
Prognosis
The rate of progression of HCV will depend onnumerous factors such as their age, HCV genotypeand viral load. The length of infection and the extent ofliver damage are other important factors. Theirresponse to treatment and any other health conditionswill affect a person’s prognosis (9). Following anti-viraltreatment only 15-20% of people eradicate the virus.20-30% of those who remain infected with the viruswill go on to develop cirrhosis over 10-20 years. Thedevelopment of cirrhosis predisposes to hepatocellularcarcinoma in 1-5% of those chronically infected withthe virus.
Methods
Initially background reading on infectious diseases thathave emerged in the last thirty years was conducted.Having chosen hepatitis C as the infectious disease tobe discussed numerous books and websites such asthe Health Protection Agency, Centres for DiseaseControl and Prevention and the World HealthOrganization were used to gain an understanding ofthe virus.
A literature search was then carried out using various
Webmedcentral > Review articles Page 4 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
databases and search engines as shown in the resultstable. Any duplicate articles generated between thesearch engines were eliminated.
Discussion
The hepatitis C virus has the potential to producevirons at a rate of 10 per day (27,28) and drugresistant mutants. The anti-viral drugs in the moreadvanced stages of clinical trials, will be discussed(29,30).
Entry inhibitors are currently being investigated to seeif they can effectively inhibit the entry of the HCV intopermissive cells and achieve reduction or eliminationof the virus. It was found that CD81 surface receptors,class B type 1 binding lectins (SCARB1) and theclaudin 1 protein (CLDN1) are essential in the entryand fusion of the virus (29). This allowed entryinhibitors to be designed which inhibit one or more ofthe steps needed in this process, and thereforepreventing viral replication.
Monoclonal and polyclonal antibodies which areknown to interfere with viral attachment have alsobeen tested. An open label RCT study was undertakenin patients undergoing a liver transplant. The humanhepatitis c immunoglobulin (HICG) antibody was takeneither at 75mg/kg or 200mg/kg for 14 weeks althoughfollowing treatment the HCV-RNA levels did notreduce (28). Another antibody, the human anti-E2monoclonal antibody which acts by neutralisinginvading antigens was also tested in infected patientsreceiving a liver transplant. The control group takingthe placebo drug achieved a decrease in HCV-RNAlevels of 1.5log10 (31). The group receiving the drugwere given a dose between 20 and 240mg ofHCV-AB68. It was found that the levels of HCV-RNAdecreased from the baseline level by a median of 1.8and 2.4 log10 in the group receiving between 120 and240mg respectively. However the difference in HCVRNA levels between the control and treatment groupwas not sustained when all doses taken were reducedafter seven days. Polymerase or NS5A inhibitors areanother anti-viral drug being developed. They regulatethe anti-viral interferon response and are involved inthe assembly and replication of the virus. A-832 andBMS-790052 are two STAT-C NS5A compounds withspecific anti-viral therapy that are at currently phase 1and phase 2 of clinical trials respectively. In adouble-blinded study a placebo group and singleascending dose method was used (32). The 18participants in the study were split equally into 3groups, taking doses of 1, 10 or 100mg ofBMS-790052. Successful anti-viral therapy was
demonstrated across all HCV genotypes. When testedin vivo following treatment a dramatic decline in theamount of HCV-RNA was observed. No adverseeffects reported (33). BMS-790052 was also tested onhepatitis C infected patients of the genotype 1, in aphase 1 RCT. The single doses were tolerated well;no adverse effects were experienced and a level ofsafety similar to that of the placebo drug was achieved. After forty eight hours in the group taking 100mg, themaximum mean decline in HCV RNA was 3.6log10,and this was sustained for 144 hours. The outcomesof this study therefore support the use of once-dailydosing. Multiple ascending studies are now beingconducted on BMS-790052. The encouraging resultsachieved with NS5A inhibitors in these clinical trialsprovide scope for further advancement in polymeraseinhibitors.
The protease inhibitors telaprevir and boceprevirpreviously known as VX-950 and SCH503034respectively have both reached phase 3 of clinicaltrials. Telaprevir is s STAT-C drug has beenextensively researched. It is a specific inhibitor of HCVas it was developed in accordance with the structureof HCV and acts by inhibiting the serine protease HCVNS3.4A. It resembles the HCV polypeptide that needsto be cleaved in viral replication by the viral protease.A 3 dosing arm study (34,16) was conducted with 20genotype 1 participants. The greatest mediandecrease in HCV RNA was shown in those takingtelaprevir in addition to peg-interferon alpha 2a. Adecrease in HCV RNA of 5.5log 10group wasachieved compared to telaprevir mono-therapy whichattained a decrease of 4log10 in the telaprevir HCVRNA.
Another study conducted used 12 genotype 1 chronicHCV participants. A rapid viral response was shown inall 12 patients as by the 28th day of therapy HCV RNAlevels were undetectable. 5 patients experienced arash although this was resolved during or aftertelaprevir treatment. Participants received telaprevir750mg every 8 hours in combinat ion withpeg-IFN-alpha 2a 180ug/week and ribavirin 1000 or1200mg/day. Phase 2 trials were then conductedunder the name of ‘PROVE’ (protease inhibition forviral eradication). Two phase 3 studies were thenconducted. ‘ADVANCE’ was the first, and was used toassess triple combination lead-in therapy of 8 and 12weeks, followed by different variations in standards ofcare in treatment naïve patients. ‘REALIZE’ is the nextphase 3 trial to be conducted and is similar to‘ADVANCE’ although treatment experienced patientswere used. Boceprevir is another protease inhibitorwhich is currently at phase 3 of clinical trials. The
Webmedcentral > Review articles Page 5 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
results of a RCTS in its phase 1b trial demonstratethat the greatest decrease in HCV RNA was foundwhen using with boceprevir in combination withpegylated interferon (28,29). A decrease of log10 2.88was achieved compared to boceprevir mono-therapyand pegylated-interferon alpha 2b mono-therapy whichachieved a maximum mean decrease of log 10 1.26and log 10 1.6 respectively. Phase 2 trials were thenconducted with the aim of defining the most effectivetreatment regime for treatment-naive genotype 1individuals and to assess their SVR. A 4 week lead intherapy of peginterferon-alpha2b or ribavirin followedby peginterferon-alpha2b, ribavirin or boceprevirshowed the greatest SVR (28,29).
The results of phase 2 studies with telaprevir andboceprevir also suggest that the ideal length oftreatment with these protease inhibitors is 24 weeks,rather than 48 weeks as a shorter treatment lengthhas the potential to produce higher response rates.
However, a significant disadvantage of telaprevir isthat viral resistance often occurs quickly and telapreviris known to produce common adverse effects such asanaemia and rashes. Thrice daily doses of telaprevirand boceprevir must be taken. The toxicity of proteaseinhibitors is another aspect of treatment to considerespecially when used in combination with pegylatedinterferon and ribavirin as the toxicity will be increased.The results of phase 2 studies with telaprevir foundthat ribavirin was needed to enhance the SVR and tominimise the breakthrough of viral resistance andrelapse.
Phase 3 studies are currently underway with the aimof defining a lead-in strategy for treatment-naïvepatients, and to find out if response rates of those whopreviously showed no response to treatment can beincreased.
Conclusion
Having researched current anti-viral therapydevelopments some promising results were shown,especially in the case of telaprevir and boceprevir.Although the other anti-viral drugs researcheddemonstrated a decrease in HCV RNA levels and aSVR with treatment, this was not as great as thatachieved by these phase 3 protease inhibitors.However the clinical trials which were conducted willbe useful in providing a platform for future anti-viraldrug developments. Given the significant amounts ofmorbidity and mortality caused by HCV, there is aneed for anti-viral drugs which have the capacity tosuccessfully eliminate HCV across all genotypes,
regardless of any previous lack of treatment andwithout significant adverse effects or any relapses.
References
1. World Health Organization. Hepatitis C. Meetingr e p o r t , 2 0 0 2 .www.who.int/csr/disease/hepatitis/whocdscsrlyo2003/en/index.html (accessed 9 April 2011).2. Health Protection Agency. Hepatitis C. Meetingr e p o r t , 2 0 1 1 .www.hpa.org.uk/Topics/InfectiousDiseases/InfectionsAZ/HepatitisC (accessed 9 April 2011).3. Naish J, Revest P, Court DS. Pathology andImmunology. Medical sciences. Edinburgh: SaundersElsevier, 2009:239-243.4. Hepatitis C. An epidemic for anyone. Meeting report,2 0 1 1 .www.epidemic.org/theFacts/hepatitisC/introduction(accessed 9 April 2011).5. Munir S, Saleem S, Idrees M, Tariq A, Butt S, RauffB et al. Hepatitis C Treatment: Current and FuturePerspectives. Virol J 2010; 7:296.6. Suk-Fong Lok A. Does antiviral therapy for hepatitisB and C prevent hepatocellular carcinoma? JGastroen Hepatol 2011; 26:221-7.7. BBC Health. Hepatitis C. Meeting report, Feb 2009.www.bbc.co.uk/health/physical_health/conditions/hepatitisc1.shtml (accessed 9 April 2011).8. Ballinger A, Patchett S, Kumar P, Clark M. HepatitisC. Clinical Medicine. Edinburgh: Saunders Elsevier,2007:142-3.9. Patient UK. Hepatitis C. Meeting report, 2011.www.patient.co.uk/doctor/Hepatitis-C.html (accessed 9April 2011).10.Nash KL, Bentley I, Hirshcfield GM. Managinghepatitis C virus infection. BMJ 2009; 338:b2366.11. British Liver Trust. Fighting Liver Disease. Meetingr e p o r t , 2 0 1 1 .www.britishlivertrust.org.uk/home/health-professionals/literature-for-professionals/a-professionals-guide-to-hepatitis-c-and-injecting-drug-use/testing-for-hepatitis-c.aspx (accessed 9 April 2011).12. Hepatitis C. Epidemiology. Meeting report, 18 Mar2007. www.microbes.wordpress.com/2007/03(accessed 9 April 2011).13. Mycek MJ, Harvery RA, Champe PC. Lippincott’sillustrated reviews. Lippincott Williams and Wilkins,2001:273-4.14. The physicians research network notebook. Modelof the Human Hepatitis C Virus. Meeting report, 2001.www.prn.org/images/prn_nb_cntnt_images/models/hcv_model_q1.jpg (accessed 9 April 2011).
Webmedcentral > Review articles Page 6 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
15. Levinson W, Jawetz E. Hepatitis C Virus. MedicalMicrobiology and Immunology Examination and BoardReview. Lange medical books, 2002:263-4.16. Bruijne J. de, Weegink CJ, Jansen PLM, ReesinkHW. New developments in the anti-viral treatment ofhepatitis C. Internl Soc of Blood Transfn 2009; 97:1-12.(http://onlinelibrary.wiley.com/doi/10.1111/j.1423-0410.2009.01187.x/pdf).17. Wikipedia. Hepatitis C. Meeting report, 20 Apr2011. www.wikipedia.org/wiki/HepatitisC (accessed 20April 2011).18. Sam AH, Teo JTH. Hepatitis C. Rapid medicine.Malaysia: Wiley- Blackwell, 2010: 107-8.19. Colledge NR, Walker BR, Ralston SH. Hepatitis C.Davidsons principles and practice of medicine.Edinburgh: Saunders Elsevier, 2010:953-4.20. Viral Hepatitis Preventive Service. Hepatitis C.Department of Health. The government of the HongKong special administrative region. Meeting report, 2J u n e 2 0 0 8 .www.info.gov.hk/hepatitis/english/hep_c_set.html(accessed 14 April).21. Bruijne J. de, Weegink CJ, Jansen PLM, ReesinkHW. New developments in the anti-viral treatment ofhepatitis C. Internl Soc of Blood Transfn 2009; 97:1-12.22. Fanning LJ. Anti-Viral therapies for Hepatitis Cvirus infection: current options and evoking candidatedrugs. Lett drug des discov 2005; 2:150-61.23. Fox RK, Wright TL. Viral Hepatitis. Currentdiagnosis and treatment. Gastroenterlogy 2003;2:446-562.24. NHS choices. Hepatitis C. Meeting report, 29 Dec2 0 0 9 .www.nhs.uk/conditions/hepatitis-c/pages/introduction.aspx (accessed 9 April 2011).25. Suzuki T, Ishii K, Aizaki H, Wakita T. Hepatitis Cviral l i fe cycle. Adv Drug Deliv Rev 2007;59(12):1200–1212.26. Giannini EG, Marabotto E, Savarino V, Trevisani F,Anna di Nolfo M, Poggio DP et al. Hepatocellularcarcinoma in patients with cryptogenic cirrhosis. ClinGastroenterol Hepatol 2009; 7(5):580–585.27. Schiano TD, Charlton M, Younossi Z, Galum E,Pruett T, Tur-Kaspa R et al. Monoclonal antibodyGCV-AbXTL68 in patients undergoing l ivertransplantation for HCV: results of phase 2randomised study. Liver Transpl 2006; 12:13181-1389.28. Bruijne J. de, Weegink CJ, Jansen PLM, ReesinkHW. New developments in the anti-viral treatment ofhepatitis C. Internl Soc of Blood Transfn; 2009;97:1-12.29. Schinazi RF, Bassit L, Gavegnano C. HCV drugdiscovery aimed at viral eradication. J Viral Hepatitis2010; 17:77-90.
30. Roberts SK, Cooksley G, Dore GJ et al. Robustantiviral activity of R1626, a novel nucleoside analog:a randomized, placebo-controlled study in patientsw i t h c h r o n i c h e p a t i t i s C . H e p a t o l o g y2008;48(2):398–406.31. Nettles R, Chein C, Persson A, Min GaoBelema M,Meanwell NA, DeMicco M et al. BMS-790052 is afirst-in class potent hepatitis C virus (HCV) NS5Ainhibitor for patients with chronic HCV infection:Results from a proof-of-concept study. Presented atthe 59th annual meeting of the Americal Associationfor the Study of Liver Diseases. October 31-November 4, 2008, San Francisco, CA.32. Sarrazin C, Rouzier R, Wagner F, Foresteir N,Larrey D, Gupta SK et al. SCH 503034, a novelhepatitis C virus protease inhibitor, plus pegylatedinterferon alpha-2b for genotype 1 non-responders.Gastroenterology 2007; 132:1270-1278.33. Health Protection Agency. Emerging Infections.M e e t i n g r e p o r t , 9 F e b 2 0 1 0 . www.hpa.org.uk/web/HPAwebFile/HPAweb_C/1204100434554 (accessed 1 April 2011)
Webmedcentral > Review articles Page 7 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
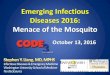
Search Engine used Search Terms used Number of articlesgenerated
Number of articlesused of those generated
Ovid-Medline Hepatitis C and Anti-Viraltherapy
158 1
Scopus Hepatitis C and Anti-Viraltherapy
41 1
Pubmed Hepatitis C and Anti-Viraltherapy
26 1
Google Scholar Hepatitis C and Anti-Viraltherapy
24600 0
Journal ofGastroenterology andHepatology
Hepatitis C and Anti-Viraltherapy
111 0
Journal of ViralHepatitis
Hepatitis C and Anti-Viraltherapy
90 1
Journal of MedicalVirology
Hepatitis C and Anti-Viraltherapy
58 0
17
Illustrations
Illustration 1
Results
Webmedcentral > Review articles Page 8 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
Sources of transmission of hepatitis C
Injection and other illicit drug use
Most common mode of acquisition in developed countries
-use of intranasal cocaine has been associated with acquisition
History of blood product transfusion
Screening of blood and blood products introduced in the UK in 1991; patients who received blood products before thatdate or in other countries may be at risk
History of having surgery abroad
Having had surgery in a country where sterilising of instruments may be suboptimal is a risk factor
Haemodialysis
Hepatitis C antibody testing was introduced in 1992
Needle stick injuries
The Incidence of seroconversion following needle stick injury is 3% to 4%
Illustration 2
Table 1
Webmedcentral > Review articles Page 9 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
Sexual activity
People in the long term monogamous relationships are at low risk of acquisition (0 to 0.6% per year); those with multiplesexual partners, particularly those engaging in traumatic sexual activity, are at greater risk
Tattooing or body piercing
Vertical Transmission
Incidence of infection is about 5% among infants born to women with the infection (risk increased with HIV co-infection);breast feeding does not seem to transmit infection, and babies may carry maternal antibodies until age 18 months
Webmedcentral > Review articles Page 10 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
Reviews
Review 1
Review Title: Emerging and Re-emerging infectious Diseases: Hepatitis CPosted by Faculty Dr. Ragini Gupta on 16 Jun 2012 06:09:58 PM GMT
What are the main claims of the paper and how important are they?: Current status of the hepatitis C virus infections and their control.
Authors have not presented a new data. They have merely reviewed the existing literature.
NA
NA
If a protocol is provided, for example for a randomized controlled trial, are there any important deviationsfrom it? If so, have the authors explained adequately why the deviations occurred? NA
NA
Reorganization needed.
Reorganization needed.
Rating: 2
Comment: 1. Title, Aim and content do not align. Authors claims to have mainly discussed anti-viral therapy for hepatitis Cvirus. In the light of this AIM, I dont understand the elaborated discussion on other topics such as DIAGNOSIS.
2. Chunks of the information are clubbed together in a disorganised way. A reading and re-reading of their ownmanuscript would have helped the author to shapen it properly. Very poor presentation. Use of terminology isinappropriate.
3. Authors claim to have browsed hundreds of articles for writing this manuscript. Yet they have used only few.Then what is the use of employing this many search engines and databases for collection of the articles?
4. Caption must have been given to tables.
Competing interests: No
Invited by the author to make a review on this article? : No
Have you previously published on this or a similar topic?: No
Experience and credentials in the specific area of science: 7 years experience of working, reading and writing on Microbiology (Infectious diseases).
How to cite: Gupta R.Emerging and Re-emerging infectious Diseases: Hepatitis C[Review of the article'Emerging and Re-emerging Infectious Diseases: Hepatitis C ' by ].WebmedCentral 1970;3(6):WMCRW001928
Webmedcentral > Review articles Page 11 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
Review 2
Review Title: Hepatitis C Virus: A comprehensive review including antiviraltherapyPosted by Dr. Venkataramana Kandi on 06 Jun 2012 05:20:08 PM GMT
What are the main claims of the paper and how important are they?: Title of the paper not appropriate. Hepatitis C was always there but we have ignored either due to the nature ofits spread or more importantly because many poor and developing countries could not afford routine testing. Thepoint which the authors intended to convey should be appreciated. At the same time authors could have done somuch to improve the presentation.
Have not evaluated
Have not evaluated
Have not evaluated
If a protocol is provided, for example for a randomized controlled trial, are there any important deviationsfrom it? If so, have the authors explained adequately why the deviations occurred? NA
NA
PAPER WAS INTENDED TO PROVIDE INSIGHT IN TO THE THERAPY. BUT AUTHORS HAVE NOTJUSTIFIED AS THEY HAVE INCLUDED THE NATURE OF VIRUS, LABDIAGNOSIS WHICH HAVE NOTCHANGED
PAPER WAS INTENDED TO PROVIDE INSIGHT IN TO THE THERAPY. BUT AUTHORS HAVE NOTJUSTIFIED AS THEY HAVE INCLUDED THE NATURE OF VIRUS, LABDIAGNOSIS WHICH HAVE NOTCHANGED
Rating: 4
Comment: NA
Competing interests: NONE
Invited by the author to make a review on this article? : No
Have you previously published on this or a similar topic?: No
Experience and credentials in the specific area of science: AS A MICROBIOLOGIST INVOLVED IN DIAGNOSIS
How to cite: Kandi V.Hepatitis C Virus: A comprehensive review including antiviral therapy[Review of the article'Emerging and Re-emerging Infectious Diseases: Hepatitis C ' by ].WebmedCentral 1970;3(6):WMCRW001878
Webmedcentral > Review articles Page 12 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
Review 3
Review Title: Hepatitis CPosted by Lead Faculty Dr. William J Maloney on 05 Jun 2012 09:40:51 PM GMT
What are the main claims of the paper and how important are they?: It explores new developments in anti-viral therapy intreating Hepatitis C.
yes
yes
yes
If a protocol is provided, for example for a randomized controlled trial, are there any important deviationsfrom it? If so, have the authors explained adequately why the deviations occurred? NA
yes
No
No
Rating: 9
Comment: This article is essential reading for anyone involved in direst patient care. It uses solid methodology and isencouraging to see that there is great promise in the treatment of hepatitis c. 15-20% of people treated withanti-viral treatment will have the virus eradicated over the next 10-20 years. 20 to 30% of those who remaininfected will go on to develop cirrhosis. This is of particular importance because the development of cirrhosis is apredisposing factor in leading to hepatocellular carcinoma in 1-5% of those chronically infected with the virus.
Competing interests: no
Invited by the author to make a review on this article? : No
Have you previously published on this or a similar topic?: No
Experience and credentials in the specific area of science: Clinical Associate Professor
How to cite: Maloney W.Hepatitis C[Review of the article 'Emerging and Re-emerging Infectious Diseases:Hepatitis C ' by ].WebmedCentral 1970;3(6):WMCRW001876
Webmedcentral > Review articles Page 13 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
Review 4
Review Title: Hepatitis CPosted by Faculty Prof. Jayendra R Gohil on 05 Jun 2012 06:59:39 AM GMT
What are the main claims of the paper and how important are they?: To explore new developments in anti-viral therapy used to treat hepatitis C.
An important questin.
Yes, Partially. Many things are already known. Ref 34 is missing from ref. list. Biopsy slide photos may be added.Discussion may have sub-headings.
Yes
Yes
If a protocol is provided, for example for a randomized controlled trial, are there any important deviationsfrom it? If so, have the authors explained adequately why the deviations occurred? NA.
NA. However search methods are mentioned.
Consider to answer- 'Does antiviral therapy for hepatitis C prevent hepatocellular carcinoma?' Though difficult aslong follow-up is required.
Difference in incidence and response in children vs adults ?
Consider to answer- 'Does antiviral therapy for hepatitis C prevent hepatocellular carcinoma?' Though difficult aslong follow-up is required.
Difference in incidence and response in children vs adults ?
Rating: 5
Comment: A good article overall.
Competing interests: no
Invited by the author to make a review on this article? : No
Have you previously published on this or a similar topic?: No
Experience and credentials in the specific area of science: treating children with Hepatitis in a medical college attached hospital.
How to cite: Gohil J.Hepatitis C[Review of the article 'Emerging and Re-emerging Infectious Diseases: HepatitisC ' by ].WebmedCentral 1970;3(6):WMCRW001871
Webmedcentral > Review articles Page 14 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
Review 5
Review Title: Emerging and Re-emerging Infectious Diseases: Hepatitis CPosted by Dr. Guadalupe García on 05 Jun 2012 02:18:47 AM GMT
What are the main claims of the paper and how important are they?: To explore new developments in anti-viral therapy use to treat hepatitis C. Anti-viral therapy for treating chronichepatitis C currently remains the only option in preventing cases of liver cirrhosis and hepatocellular carcinoma.
These claims are not novel, but, the review is interesting.
Yes.
Yes.
If a protocol is provided, for example for a randomized controlled trial, are there any important deviationsfrom it? If so, have the authors explained adequately why the deviations occurred? Not applicable.
Yes.
Not applicable.
Not applicable.
Rating: 4
Comment: Since this is a review, should not lead the section "Discussion", the content should go under "Treatment."Make no reference 2011-12.
Competing interests: No
Invited by the author to make a review on this article? : No
Have you previously published on this or a similar topic?: Yes
References: Pérez-López JA, García-Elorriaga G, del Rey-Pineda G, Manjarrez-Téllez B. Anticuerpos contra hepatitis Bdespués de vacunación en trabajadores de la salud. Salud Pública de México. 2011; 53(3):205-206.
How to cite: García G.Emerging and Re-emerging Infectious Diseases: Hepatitis C[Review of the article'Emerging and Re-emerging Infectious Diseases: Hepatitis C ' by ].WebmedCentral 1970;3(6):WMCRW001865
Webmedcentral > Review articles Page 15 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
Review 6
Review Title: Emerging and Re-emerging Infectious Diseases: Hepatitis CPosted by Prof. Thomas V Chacko on 05 Jun 2012 01:47:21 AM GMT
What are the main claims of the paper and how important are they?: That Hepatitis C is emerging as a common cause of preventable liver cancer. This knowledge has policy andpractical implications
It is already a known fact and hence weakens the originality of this one.
A comparison of the extent of the problem - current Vs past or a graph showing trends over time would haveestablished that the disease is emerging/ re-emerging
The "Results" section is missing or is not explicitly finding a place - it merges in the Introduction and then authorsjump straight to discussion. A summary of findings could have been made and shown in the results section tohelp clarify to the audience what were the findings from the review of literature
If a protocol is provided, for example for a randomized controlled trial, are there any important deviationsfrom it? If so, have the authors explained adequately why the deviations occurred? not applicable
Methodology is vague. details of search strategy , key words used etc are not given and so the results cannot bereproduced.
Only in one of the Tables labelled crudely as "Results" does one find that the search term used was
"Hepatitis C and Anti-Viral therapy" which is very broad
The title is misleading as compared to the stated aim of the study "To explore new developments in ant i -viral therapy used to treat hepatitis C" . This is not reflected in the title
The results are not systematically presented
The titles of the tables are not self explanatory
The conclusions para doesn't clearly capture the gist / conclusion that the authors have reached
The title is misleading as compared to the stated aim of the study "To explore new developments in ant i -viral therapy used to treat hepatitis C" . This is not reflected in the title
The results are not systematically presented
The titles of the tables are not self explanatory
The conclusions para doesn't clearly capture the gist / conclusion that the authors have reached
Webmedcentral > Review articles Page 16 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
Rating: 2
Comment: It appears as a Post Graduate seminar which does not clarify much but confuses. A systematic way of classifyingand presentation of findings would have made the audience of the seminar worth attending.
Authors have to decide whether they want to highlight recent advances in treatment of the Viral Hepatitis orsimply pad it with lot of epidemiological stuff which is already well known and presented in any textbook.
In its present form is not fit for publication in a journal unless improved drastically
Competing interests: none
Invited by the author to make a review on this article? : No
Have you previously published on this or a similar topic?: No
Experience and credentials in the specific area of science: Expertise in epidemiology and study designs
How to cite: Chacko T.Emerging and Re-emerging Infectious Diseases: Hepatitis C[Review of the article'Emerging and Re-emerging Infectious Diseases: Hepatitis C ' by ].WebmedCentral 1970;3(6):WMCRW001864
Webmedcentral > Review articles Page 17 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
Review 7
Review Title: Emerging and Re-emerging Infectious Diseases: Hepatitis CPosted by Faculty Dr. Avnish Kumar on 09 May 2012 02:13:39 AM GMT
1 Is the subject of the article within the scope of the subject category? Yes
2 Are the interpretations / conclusions sound and justified by the data? Yes
3 Is this a new and original contribution? No
4 Does this paper exemplify an awareness of other research on the topic? Yes
5 Are structure and length satisfactory? Yes
6 Can you suggest brief additions or amendments or an introductory statement that will increasethe value of this paper for an international audience?
Yes
7 Can you suggest any reductions in the paper, or deletions of parts? No
8 Is the quality of the diction satisfactory? Yes
9 Are the illustrations and tables necessary and acceptable? Yes
10 Are the references adequate and are they all necessary? Yes
11 Are the keywords and abstract or summary informative? Yes
Rating: 6
Comment: The Author can write more literature about Hepatitis C. The number of reference must be more.
Competing interests: Nil
Invited by the author to make a review on this article? : No
Have you previously published on this or a similar topic?: No
Experience and credentials in the specific area of science: No
How to cite: Kumar A.Emerging and Re-emerging Infectious Diseases: Hepatitis C[Review of the article'Emerging and Re-emerging Infectious Diseases: Hepatitis C ' by ].WebmedCentral 1970;3(5):WMCRW001787
Webmedcentral > Review articles Page 18 of 19

WMC003342 Downloaded from http://www.webmedcentral.com on 17-Jun-2012, 01:00:01 AM
DisclaimerThis article has been downloaded from WebmedCentral. With our unique author driven post publication peerreview, contents posted on this web portal do not undergo any prepublication peer or editorial review. It iscompletely the responsibility of the authors to ensure not only scientific and ethical standards of the manuscriptbut also its grammatical accuracy. Authors must ensure that they obtain all the necessary permissions beforesubmitting any information that requires obtaining a consent or approval from a third party. Authors should alsoensure not to submit any information which they do not have the copyright of or of which they have transferredthe copyrights to a third party.
Contents on WebmedCentral are purely for biomedical researchers and scientists. They are not meant to cater tothe needs of an individual patient. The web portal or any content(s) therein is neither designed to support, norreplace, the relationship that exists between a patient/site visitor and his/her physician. Your use of theWebmedCentral site and its contents is entirely at your own risk. We do not take any responsibility for any harmthat you may suffer or inflict on a third person by following the contents of this website.
Webmedcentral > Review articles Page 19 of 19