Embed Size (px)
Citation preview

21/07/2017
1
EMDRIA 2017 CONFERENCE: BELLEVUE, WA, USA AUGUST 2017
Dr Derek Farrell CPsychol, PhD, Csci, AFBPsS
University of Worcester – Institute of Health & SocietyChartered Psychologist, Principal Lecturer in PsychologyEMDR Europe Accredited Trainer and ConsultantBABCP Accredited Cognitive Behavioural PsychotherapistVice-President EMDR EuropePresident Trauma Aid Europe
©Derek Farrell/July 2017
1
Overview of what is OCD and theoretical concepts
Theoretical Rationale for the use EMDR Therapy with client’s with OCD
Exploring EDR Therapy Protocol Options Standard Protocol Flash-forward Blind 2Therapist Protocol
Pluralism & Integrationism in working with OCD
Empirical Evidence in support of the EMDR Therapy with OCD
Case Material demonstrating use of EMDR Therapy
Self-experience
Implications for future research and development
©Derek Farrell/July 2017 2
21/07/2017
2
• During this workshop we will be engaging in various exercises and self-experience
• All exercises and self-experiences are entirely voluntary
• You are responsible for your own well-being
• Please feel free to utilize any self-care or internal resources as you feel necessary
• All material shared is confidential
• You are clinically responsible for how you practice EMDR Therapy
©Derek Farrell/July 2017 3
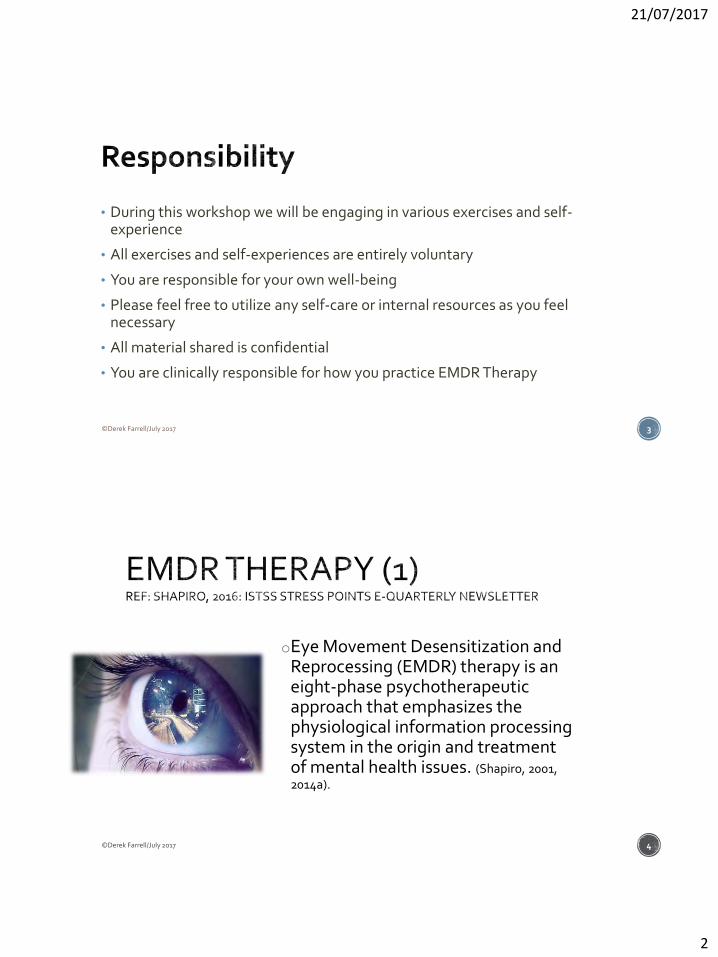
oEye Movement Desensitization and Reprocessing (EMDR) therapy is an eight-phase psychotherapeutic approach that emphasizes the physiological information processing system in the origin and treatment of mental health issues. (Shapiro, 2001, 2014a).
©Derek Farrell/July 2017 4

21/07/2017
3
o Its theoretical basis is the Adaptive Information Processing (AIP) model, which holds that the primary source of psychopathology is the presence of memories of adverse life experiences that have been inadequately processed.
oThese inappropriately stored episodic memories, which include the perceptions, sensations, beliefs and emotions that occurred at the time of the adverse life event, can be triggered by current internal and external stimuli, contributing to ongoing dysfunction.
©Derek Farrell/July 2017 5
oThis model was developed in the early 1990s and since then has been supported by research demonstrating the role played by disturbing life events in the genesis of many forms of psychological and somatic symptomology (e.g., Affifi et al., 2012; Felitti et al., 1998).
EMDR Therapy (3)Ref: Shapiro, 2016: ISTSS Stress Points e-Quarterly Newsletter
©Derek Farrell/July 2017 6

21/07/2017
4
1. Access a Dysfunctionally Stored Trauma Memory
2. Stimulate – Bilaterally and via Dual Attention
3. Move it oNeurobiological
oArchitecture
oCharacter - SUD
oConstruct and meaning
©Derek Farrell/July 2017 7
oEMDR therapy is a trans-diagnostic, integrative psychotherapy approach that is intrinsically ‘Client-Centered’ at its core. It has been extensively researched and proven effective for the treatment of adverse life experiences. It utilises a theoretical framework known as adaptive information processing (AIP).
oThe context of AIP is that adverse life experiences cause imbalance in the nervous system thus creating blockages or incomplete information processing – namely trauma memories
o [Farrell (2015) Trans-generational Trauma and EMDR Therapy, BACP Private Practice Journal, Winter Edition 2015]
©Derek Farrell/July 2017 8

21/07/2017
5
For CBT the pathology lies in the presence of dysfunctional beliefs and behaviours, and hence the treatment proceeds by manipulating these beliefs and behaviours.
For EMDR Therapy the pathology is deemed to stem from unprocessed, physiologically stored memories, and hence the treatment aims to access and process these past memories, present triggers and future templates (Shapiro 2014)
©Derek Farrell/July 2017 9
CBT – Disturbance from the Adverse Life Event is generated by the MEANING that is attributed to this experience rather than the experience itself Therefore beliefs/ cognitions are INDEPENDENT
VARIABLES
EMDR Therapy – Disturbance from the Adverse Life Event is generated by the MEMORY of the experience which is then DYSFUNCTIONALLY STORED Therefore beliefs/ cognitions are DEPENDENT
VARIABLES
©Derek Farrell/July 2017 10
21/07/2017
6
People with OCD have also encountered ADVERSE LIFE EVENTS Adaptive Information Processing Case (AIP) Conceptualisation
Reformulation of the OCD (PAST)
Dysfunctional Memory Network
Compulsions reinforce OCD – Safety Behaviour (Present)
OCD is driven by a ‘Worst Fear/ Catastrophic Event (Future) Dysfunctional Memory Network
©Derek Farrell/July 2017 11
1. Adaptive Information Processing Case Conceptualisation
2. Trauma Stabilisation and Resourcing
3. Trauma Processing and Confrontation
4. Therapeutic Relationship and Attunement
©Derek Farrell/July 2017 12

21/07/2017
7
What is Obsessive Compulsive Disorder?
OCD is a mental disorder that includes obsessions and/or compulsions.
Most people experience both obsessions and compulsions – however some just obsessions (known as “pure ‘O’”.
These obsessions and compulsions are very upsetting, and cause great distress and impairment
©Derek Farrell/July 2017 13
• Intrusive thoughts, Images and Impulses
• Obsessions and or Compulsions
• Compulsions are meaningfully related to fears
• By definition, the person seeks to ignore or supress intrusions
• Key to diagnosis: distress/disability
©Derek Farrell/July 2017 14

21/07/2017
8
15
16

21/07/2017
9
17
18

21/07/2017
10
What is Obsessive Compulsive Disorder?
OCD is a mental disorder that includes obsessions and/or compulsions.
Most people experience both obsessions and compulsions – however some just obsessions (known as “pure ‘O’”.
These obsessions and compulsions are very upsetting, and cause great distress and impairment
©Derek Farrell/July 2017 19
It is estimated that some 112 million people in the world suffer from OCD and is one of the leading causes of disability
The average age that OCD becomes clinically significant is around 19 and a half years old. That being said, it can start in early childhood, with males often getting the disorder earlier.
Additionally, most people have some symptoms before the disorder reaches a clinically significant threshold.
©Derek Farrell/July 2017 20

21/07/2017
11
Phobias
Substance Abuse Disorders
Major Depressive Disorders (MDD)
Obsessive Compulsive Disorder (OCD)Co-morbidity
Alcohol/ Substance misuse Generalised Anxiety Disorder Specific Phobia Eating Disorders Personality Disorder
©Derek Farrell/July 2017 21
Currently there is no known complete or permanent cure for OCD exists; however, with proper treatment the symptoms can be made much more manageable, or kept completely under control.
Cognitive behavioural therapy (CBT) is a common technique used for people struggling with OCD.
This method teaches people with OCD how to confront their fears and reduce anxiety without acting out on compulsions.
The most effective type of CBT for OCD is called Exposure and Response/Ritual Prevention (abbreviated as either ERP or EX/RP).
©Derek Farrell/July 2017 22
21/07/2017
12
Research also supports the usage of Antidepressant medications. This helps to reduce obsessions
Combination approach indicates the best results - Antidepressant & ERP
ERP is the best and most durable solution for OCD.
If someone is properly treated with ERP, the OCD can be very well controlled if not almost eliminated.
However, even if the OCD is mostly gone, the sufferer will need to be on guard to prevent it from returning. So, relapse prevention is an important part of treatment as well.
©Derek Farrell/July 2017 23
Each time a person with OCD gives into an obsession by performing a compulsion, it strengthens the OCD.
The opposite also holds true that each time one does not give into the obsessions, the fear weakens.
So, with ERP one is in effect strengthening the brain by forging out a new pathway.
ERP is more than ‘willpower’ - most OCD sufferers have tried to resist the obsessions, but it must be done properly to work, and so willpower alone is not enough.
ERP takes a graduate approach, and this has been scientifically developed and proven, to give people the tools to control their OCD.
©Derek Farrell/July 2017 24
21/07/2017
13
Medication is an effective treatment for OCD.
About 7 out of 10 people with OCD will benefit from either medication or Exposure and Response Prevention (ERP)
Research indicates that for the people who benefit from medication, they usually see their OCD symptoms reduced by 40-60%.
Medical advise is to continue to take medication regularly
However about half of OCD patients stop taking their medication due to side effects or for other reasons.
©Derek Farrell/July 2017 25
Tricyclic Antidepressants – Ineffective for treating OCD Amitriptyline
Imipramine
Serotonin Selective Re-uptake Inhibitors (SSRI’s) more effective Fluvoxamine (Luvox®)
Fluoxetine (Prozac®)
Sertraline (Zoloft®)
Paroxetine (Paxil®)
Citalopram (Celexa®)
Venlafaxine (Effexor®)
Escitalopram (Lexapro®)
©Derek Farrell/July 2017 26

21/07/2017
14
27
Despite strong empiricism for CBT [ERP] in the treatment of OCD it should be acknowledged that not all clients respond well to this particular psychological treatment approach and that recovery levels vary significantly (Roth and Fonagy 2006).
Cognitive Therapy may not be as effective as ERP (Purdon, 2009)
Group interventions not as effective as individual treatment (McClean, 2001)
Rector et al (2009) reports high ‘drop out’ rates amongst clients diagnosed with OCD and treated with CBT.
©Derek Farrell/July 2017 28

21/07/2017
15
CBT is effective at reducing the intensity of OCD symptoms for about 50 to 60% of patient's who complete treatment
However ‘Full remission’ of OCD symptoms (e.g. recovery is used as an index of improvement the efficacy drops to 25% (Fisher & Wells 2005)
Maher el al (2010) consider that EX/RP is less than appropriate or effective for around 50% of those treated
©Derek Farrell/July 2017 29
o Although Ex/RP can be highly effective for around 50% of people who complete treatment, there are a number of recognised drawbacks (Marr 2012)
oEx/RP is much less effective in clients who experience obsessive ruminations rather than overt compulsions
o The actual level of improvement is extremely variable (Roth 2006)
o High Drop out rates [40%], (Rector et al 2009)
o High relapse rates [57.3%] (WHO 2010)
©Derek Farrell/July 2017 30

21/07/2017
16
Phase 1: History Taking Developing a collaborative therapeutic relationship
Ascertaining degree of motivation for change
OCD through the lens of AIP
Behavioural Analysis of pattern of behaviour & cognitions
Maintenance factors and ‘contributions to chaos’
OCD & Secondary Gain
Ascertaining goals for treatment
EMDR Therapy/ AIP Target Selection
©Derek Farrell/July 2017 31
Outlining the struggle with OCD
First experiences/ recollections/ memory of OCD
Other issues that may have been going on at the time
Worst OCD experience/ memory
Viewing OCD through the lens of: Past – Present – Future
Impact of the OCD on life’s journey: relationships, family, friendships, work, social, etc.,
How might your life be different if you were free from OCD?
©Derek Farrell/July 2017 32

21/07/2017
17
Obsessions Current Past
o Aggression
o Contamination
o Sexual Obsessions
o Hoarding/ Saving
o Religious obsessions
o Symmetry and exactness
o Miscellaneous: lucky numbers, sounds, colours, remembering things, etc.,
o Somatic
©Derek Farrell/July 2017 33
Compulsions Current Past
o Cleaning/ washing
o Checking
o Repeating
o Counting
o Ordering/ Arranging
o Hoarding/ Collecting
o Miscellaneous: mental rituals, needing to touch, ritualised eating, superstition, hair pulling
©Derek Farrell/July 2017 34

21/07/2017
18
Cognitive Behavioural Therapy EMDR Therapy/ Adaptive Information Processing
oObsessionsoCompulsionsoAvoidance
Primary Focio Obsessionso Compulsionso Avoidanceo Maintenance factors
Primary Focio Dysfunctionally stored memory
networks – past, present and futureo Obsessions, compulsions and
avoidance and maintenance factors seen as consequences
©Derek Farrell/July 2017 35
Weight loss
Sleep changes
Loss of appetite
Lack of energy
Feelings of sadness
Crying or frequent tearfulness
Suicidal thoughts – with or without intent
Feelings of hopelessness/ despair/ helplessness
Lack of interest
Lack of joy
©Derek Farrell/July 2017 36

21/07/2017
19
Phase 2: Preparation Stabilisation & Resourcing
Psychoeducation
Paradigm Approach – pluralism, integrationism, etc.
Recruiting co-therapists
Identification of ‘Core Beliefs’ & maintenance factors
©Derek Farrell/July 2017 37
Phase 3 – 7 Target Selections for processing Interventions – Target Focussed
Standard Protocol
Standard Protocol & In-vivo Desensitisation
Interventions – Underlying Conflicts
Flash-forward
Flash-forward & Imaginal Exposure
©Derek Farrell/July 2017 38

21/07/2017
20
“Imagine all these parts of your brain screaming at you when your OCD symptoms are at their worst: The thalamus sends messages from other parts of your body, making you hyperaware of everything
going on around you
The caudate nucleus opens the gate and lets in unwanted intrusive thoughts
The orbital cortex mixes thoughts and emotions, then tells you, ‘Something is wrong here! Take cover!’
The cingulate gyrus tells you to perform compulsions to relieve the anxiety the rest of your brain has heaped on you
Meanwhile, your synaptic clefts are screaming, ‘Send in some Serotonin! We’re running short here’
With all this going on – ‘No wonder I have problems’
©Derek Farrell/July 2017 39
‘Keeping Eyes on the Prize’ Resolution or ‘symptom reduction’
Type I and Type II OCD
Managing relapses
Dealing with future obsessions
©Derek Farrell/July 2017 40

21/07/2017
21
Worst Picture
Image, Cognitions (beliefs, Emotions & Body Sensations)
Traumatic Memory
(Past)Compulsion triggering situation
Stimulus Focus
Imaginary/ Real Trigger (Obsessions)
©Derek Farrell/July 2017 41
Flash-Forwards
Underlying validation / Catastrophe scenario
Worst Case Scenario
Automatic & Intrusive Mental Images
Flash-Forward
Future Orientated
Targets
©Derek Farrell/July 2017 42

21/07/2017
22
Future Anticipatory Anxiety (Standard Protocol)
Compulsion cannot be executed
Blocking Compulsion
Imagery
Standard Protocol
Image, Cognitions (beliefs, Emotions & Body Sensations)
Underlying Conflict
©Derek Farrell/July 2017 43
Experience (Event) – Real or Fantasy
Worst Fear
Representation of an Event
Generalisation
Sound
Perpetrator/ Relationship
Emotion
Somatic Experience
Cognitions/ Belief Systems
Unspoken
©Derek Farrell/July 2017 44

21/07/2017
23
Obsessional thoughts in OCD are very similar to Negative Cognitions in EMDR Therapy
Rationality and Irrationality (Client insight)
In search of empiricism – Cognitive Gymnastics
Exploring the link between ‘core beliefs’ and ‘target selection’
Challenging risk
©Derek Farrell/July 2017 45
All or nothing thinking:
Magical thinking
Overestimating risk/ danger
Perfectionism
Hyper-morality
Over-responsibility
Thought, Action, Fusion
Over-importance of thought
Exclusivity error
Nobility Gambit (Martyr syndrome)
‘What if’
Intolerance of uncertainty
©Derek Farrell/July 2017 46
21/07/2017
24
Derek Farrell
©Derek Farrell/July 2017
47
NAZARI, ET AL (2011) COMPARISON OF EMDR WITH CITALOPRAM IN THE TREATMENT OF OCD.
• 90 subjects with a diagnosis of OCD were randomly assigned into two groups. They either received EMDR or Citalopram over 12 weeks.
• Both groups assessed using Y-BOC, pre and post treatment. Both groups demonstrated significant improvement, however in the short term EMDR was shown to be more effective.
©Derek Farrell/July 2017 48

21/07/2017
25
EMDR & OCD (BOHM & VODERHOLZER, 2010)
3 case studies, applying EMDR in different ways EMDR followed by ERP. (early traumatic memories) : [checking behaviours] ERP followed by EMDR: [Intrusive thoughts] EMDR (resource instillation and future template) : [cleaning compulsions]
All 3 clients showed 60% improvement [Y-BOC, BDI, DES, SUDS
©Derek Farrell/July 2017 49
• Treated (14-16 sessions) 4 subjects using EMDR Therapy Phobia Protocol.
• The Adapted EMDR Phobia Protocol: (start with current triggers –OCD Obsession and Compulsions then future template, then past related disturbing memories [if there are any] and the Adapted EMDR Phobia Protocol with Video Playback. (Client plays a video/memory of the first time they remember being scared by their obsessional thought, when the client is aware of feeling stressed, stop, identify image, NC, PC, VOC, SUD and Body sensation –process in the usual way-. Video playback is then used to monitor desensitisation and identify other stressors.
• Marr’s work is based on the theoretical view that OCD is a self perpetuating disorder, with OCD compulsions and obsessions and current triggers reinforcing and maintaining the disorder (Marr 2012)
• Clients were assessed using the Yale-Brown Obsessive Compulsive Inventory (Goodman et al 1989), (Y-BOC) significant improvement was noted in all clients at the end of therapy and at follow up.
©Derek Farrell/July 2017 50

21/07/2017
26
o 8 subjects, who have been diagnosed with OCD, have had CBT intervention within the last 5 years but symptoms have not abated.
o Subjects will be excluded from the project, if they have an active psychotic condition, are suffering with a sever clinical depression ,are actively suicidal or over using benzodiazepines, alcohol or street drugs.
o Following assessment (participant information and consent to engage in project), subjects will complete 4 psychometric questionnaires:
o Y-BOC (Goodman et al 1989)
o PHQ-9 (Kroenke et al 2001)
o GAD-7 (Spitzer et al 2006)
o Each subject will receive 8 sessions of EMDR, [in an effort to mirror IAPT services] plus 2 follow up appointments (EMDR will not be administered at follow up)
o Normal EMDR protocol will be used for clients with past aversive life events (PALE); EMDR focussing on “Intolerance of uncertainty”will be used where no PALE was identified.
©Derek Farrell/July 2017 51
Age - ranged from 20 – 59 with the average being 40 years old
Gender - 50:50
87.5% in employment
62.5% on anti-depressant medication
All research participants had been previously diagnosed by either a Consultant Psychiatrist or Psychologist as meeting the DSM 5 criteria for OCD
©Derek Farrell/July 2017 52

21/07/2017
27
Ref: Treating Obsessive Compulsive Disorder (OCD) using Eye Movement Desensitisation and Reprocessing (EMDR) Therapy: An Ethno-Phenomenological Case Series (Keenan & Farrell et al, in press)
©Derek Farrell/July 2017 53
0
1
2
3
4
5
6
7
8
9
10
Pre Processing Post Processing
SUD 0-10 VOC 1-7
Ref: Treating Obsessive Compulsive Disorder (OCD) using Eye Movement Desensitisation and Reprocessing (EMDR) Therapy: An Ethno-Phenomenological Case Series (Keenan & Farrell et al, in press)
©Derek Farrell/July 2017 54

21/07/2017
28
0
5
10
15
20
25
Pre Post 1-month 3-Months
Y-BOC GAD-7 PHQ-9
Ref: Treating Obsessive Compulsive Disorder (OCD) using Eye Movement Desensitisation and Reprocessing (EMDR) Therapy: An Ethno-Phenomenological Case Series (Keenan & Farrell et al, in press)
©Derek Farrell/July 2017 55
0
5
10
15
20
25
Pre Post 1-month 3-month
Flash-forward Standard Protocol
Ref: Treating Obsessive Compulsive Disorder (OCD) using Eye Movement Desensitisation and Reprocessing (EMDR) Therapy: An Ethno-Phenomenological Case Series (Keenan & Farrell et al, in press)
©Derek Farrell/July 2017 56

21/07/2017
29
0
2
4
6
8
10
12
14
Pre 3-month
YBOC Sub-score: Compulsions N=8
Flash-forward Standard Protocol
0
2
4
6
8
10
12
Pre 3-month
Y-BOC Sub-score: Obsessions N=8
Flash-forward Standard Protocol
Ref: Treating Obsessive Compulsive Disorder (OCD) using Eye Movement Desensitisation and Reprocessing (EMDR) Therapy: An Ethno-Phenomenological Case Series (Keenan & Farrell et al, in press)
©Derek Farrell/July 2017 57
0
2
4
6
8
10
12
Pre Post 1-month 3-month
GAD-7 Scores N=8
Flash-forward Standard Protocol
0
2
4
6
8
10
12
Pre Post 1-month 3-month
PHQ-9 Scores N=8
Flash-forward Standard Protocol
Ref: Treating Obsessive Compulsive Disorder (OCD) using Eye Movement Desensitisation and Reprocessing (EMDR) Therapy: An Ethno-Phenomenological Case Series (Keenan & Farrell et al, in press)©Derek Farrell/July 2017
58

21/07/2017
30
EMDR Therapy has demonstrated that it is a safe and well tolerated treatment for Obsessive Compulsive Disorder
The Theoretical paradigm of EMDR Therapy – Adaptive Information Processing is useful part of case conceptualisation
EMDR Therapy is effective Reducing SUD Increasing VOC Reduction in YBOC, GAD-7 & PHQ-9
More research is needed to further explore the utilisation of EMDR Therapy with OCD populations
©Derek Farrell/July 2017 59
Past
Present - Flash-forward
Future - Future Template
©Derek Farrell/July 2017 60

21/07/2017
31
o Flash-forward procedure is identical to the standard EMDR protocol, except that the target relates to a feared catastrophic future event rather than a past one
o The therapist may ask the client to say what they believe will happen if they are not able to avoid the fearful situation anymore
o Main characteristics of Flash-forwardo Primary focus - worst-case scenario
o A detailed and still picture
o Contains catastrophic elements of what might happen in the future
o Context specific and conceptually related to client’s symptoms
o Intrusive and disturbing
o “Death is not Enough”
©Derek Farrell/July 2017 61
Engelhard et al
…fear of future danger is common after a threatening event, and may take the form of future-oriented mental images. These may appear like ‘Flash-forwards’, echoing ‘flashbacks’ in posttraumatic stress disorder (PTSD) and possess sensory qualities, being vivid, compelling, and detailed. (Engelhard et al., 2011, p. 599).
©Derek Farrell/July 2017 62

21/07/2017
32
BLIND 2 THERAPIST PROTOCOLS IN EMDR THERAPYDr Derek Farrell CPsychol, PhD, Csci, AFBPsS
©Derek Farrell/July 2017
63
Shame
Fear
Retribution
Secrecy
Disgust
Transference/ Counter-transference
Quasi Power and Control
©Derek Farrell/July 2017 64

21/07/2017
33
"Fundamentally, words can't integrate the disorganized sensations and action patterns that form the core imprint of the trauma…. To do effective therapy, we need to do things that change the way people regulate these core functions, which probably can't be done by words and language alone."
©Derek Farrell/July 2017 65
(FARRELL ET AL, 2016)
Kurdistan I Research Project 2: Blind 2 Therapist Protocol
Derek Farrell©Derek Farrell/July 2017
66

21/07/2017
34
High levels of Shame-Based Trauma within Yezidi survivors
In addition high levels of Shame-Based Trauma amongst Kurdish Population/ Participants
Research based on Shapiro (2001), Blore et al (2009; 2013) and slight modification by research team
“Where there are no words’
Cultural sensitivity and adaptability
Treatment versus No Treatment
©Derek Farrell/July 2017 67
First experimental design study using Blind 2 Therapist Protocol
Research took place during a intensive 6 day EMDR Therapy Level 2 Training (May 2016)
Participants – Jiyan Foundation Therapists during Self-experience Practicum
Each EMDR Therapy session supervised live by EMDR Europe Accredited Consultant
Control Group [N=59] – Standard Protocol
Experimental Group [N=39] – Blind 2 Therapist Protocol
Null Hypothesis
©Derek Farrell/July 2017 68

21/07/2017
35
Rape
Witnessing a murder
Recent Trauma
Sports injury
Bereavement
Road Traffic Collision
Bullying
War related conflicts & incidents
Torture
Dog attack
Imprisonment
Vicarious trauma
Gender-based violence
©Derek Farrell/July 2017 69
0
1
2
3
4
5
6
7
8
9
Pre Post 6 month Pre Post 6 month
Control Group - Standard Protocol [N=59] Experimental Group - B2T Protocol [N=39]
SUD (0-10) VOC (1-7)
©Derek Farrell/July 2017 70

21/07/2017
36
90% of the research participants would NOT have worked on their trauma experience without using the B2T protocol
95% Disclosed their trauma after EMDR Therapy
B2T Protocol was SAFE
Omission of C-, C+ and VOC still proved effective
Script of Protocol had to be adapted slightly to make more specific
Clear definition of what was meant by ‘CHANGE’ during processing
©Derek Farrell/July 2017 71
Modified Version of the Blind 2 Therapist ProtocolPhase 3: Modified Assessment of the Target Memory (B2T)
Target Word
- Memory
Current
Emotion
Subjective
Level of
Disturbance
(SUD)
Location of
Body
Sensation
©Derek Farrell/July 2017 72
21/07/2017
37
Chapter 7 EMDR Therapy and Head and Throat Cancer
Derek Farrell and Kate Reid
©Derek Farrell/July 2017 73
More complex the case – more important is the THERAPEUTIC RELATIONSHIP
Exposure and Response/ Ritual Prevention (ERP)
Anti-depressant Medication (SSRI’s)
Collaborative Partnerships
EMDR Therapy AIP Case Conceptualisation Trauma Stabilisation and Resourcing Trauma Processing & Confrontation
Standard Protocol – disclosed traumas Blind 2 Therapist – shame-based traumas Flash-Forward – future catastrophic scenarios
©Derek Farrell/July 2017 74

21/07/2017
38
Contact details:
Dr Derek FarrellUniversity of WorcesterEmail: [email protected]
©Derek Farrell/July 2017 75