Embed Size (px)
Citation preview

Ellen Jo Baron, Ph.D., D(ABMM)Director of Medical Affairs, Cepheid
Professor Emerita, Pathology, Stanford University
Minimal TAT, Maximum Impact on Infection Control for C. difficile

• Employee of Cepheid
• Consultant for: Merck, OpGen, NanoMR, MorphDesign, MicroPhage
• Stock holdings: Cepheid, ImmunoSciences, PolyRemedy
• Other renumeration: Royalties for contributions to Infectious Diseases Alert newsletter, Palo Alto VAMC, and from various IVD industry consulting companies
• Founder & board member of NGO: Diagnostic Microbiology Development Program (www.DMDP.org)
E.J. Baron’s Conflicts of Interest
PAGE | 3
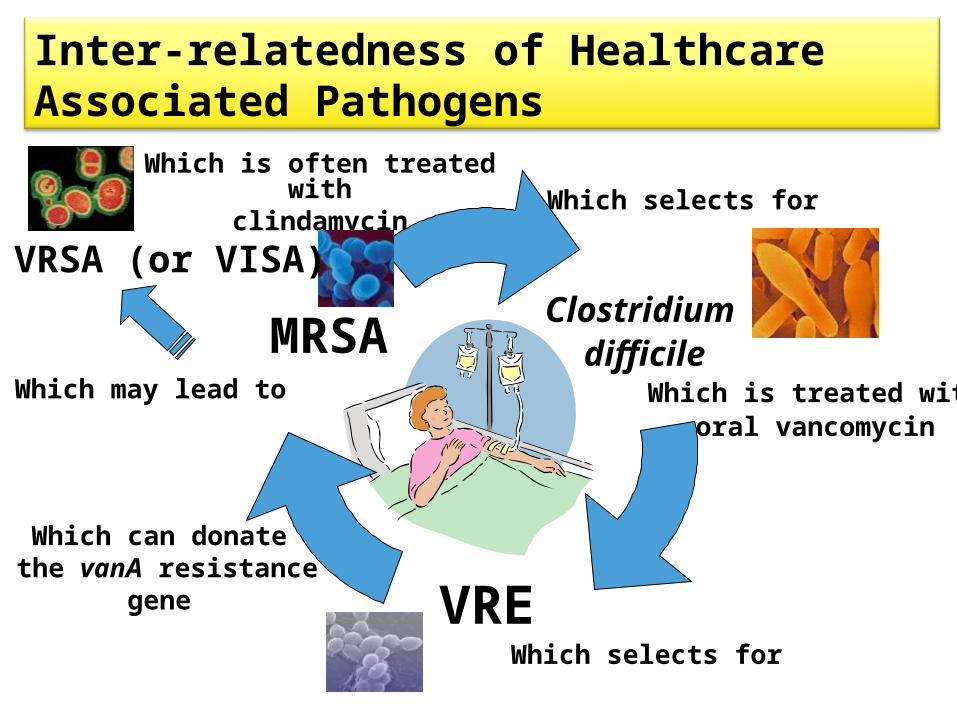
Inter-relatedness of Healthcare Associated Pathogens
Which is often treated withclindamycin Which selects for
Which selects for
Which can donate the vanA resistance
gene
Which may lead to
Clostridium difficile
VRE
MRSAWhich is treated with
oral vancomycin
VRSA (or VISA)
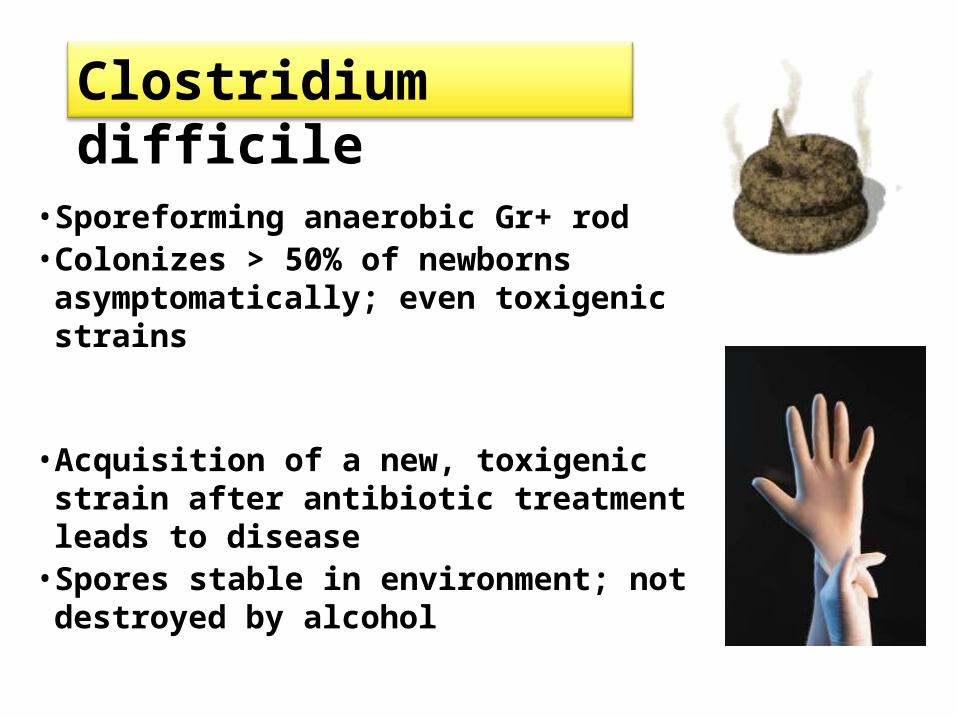
• Sporeforming anaerobic Gr+ rod• Colonizes > 50% of newborns
asymptomatically; even toxigenic strains
• Acquisition of a new, toxigenic strain after antibiotic treatment leads to disease
• Spores stable in environment; not destroyed by alcohol
Clostridium difficile

U.S. Numbers and Cost/yr
The newest HAI
>$32 million
Healthcare-Associated Infections (HAI)
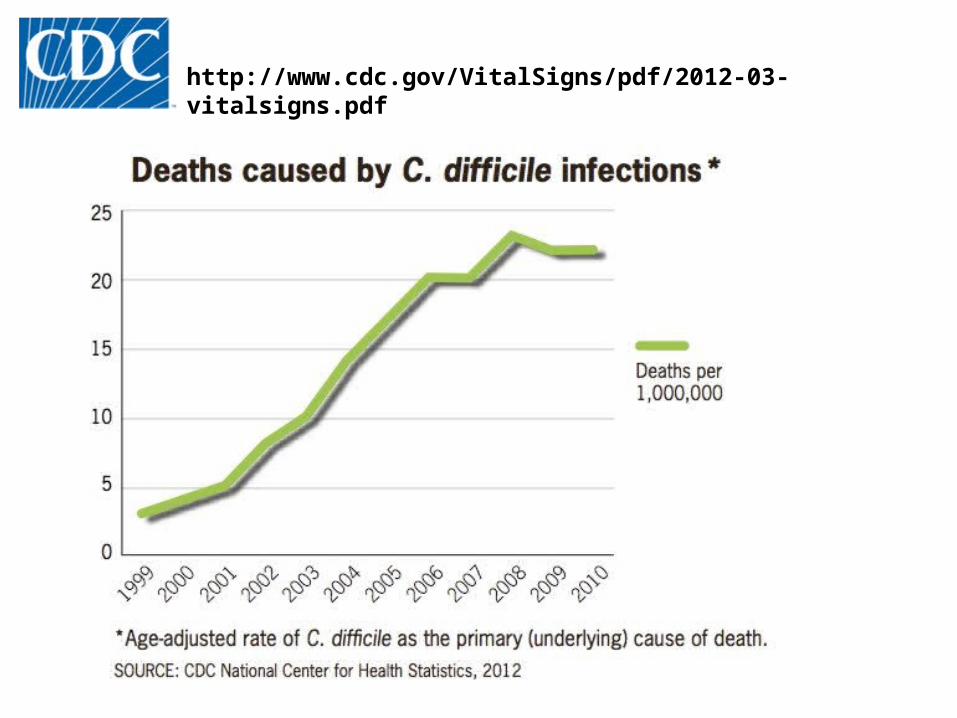
http://www.cdc.gov/VitalSigns/pdf/2012-03-vitalsigns.pdf

• 3 times more CDI hospitalizations in last 10 years• Half of infections in patients >65 yrs but 90% of deaths• 75% of infections first show in nursing home patients or
those seen in clinic recently• Half of patients have CDI at time of admission • Based on 2008 U.S. APIC survey:
Average cost $32.1 million Average extra hospital days = 40,200 Mortality= 14,000 patients/year
Current statistics from CDC
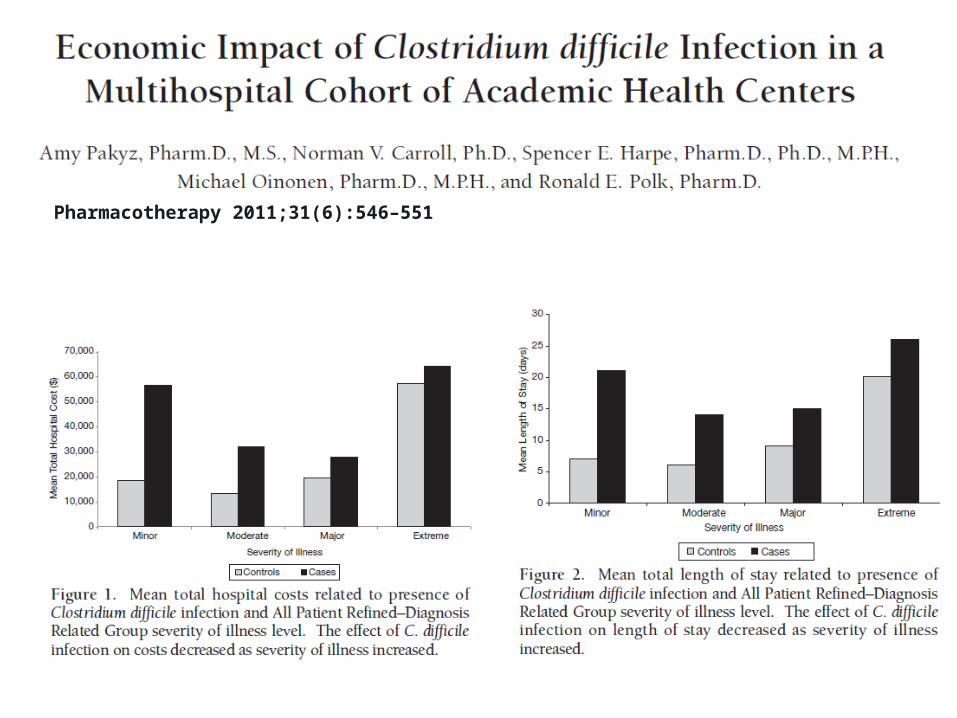
Pharmacotherapy 2011;31(6):546–551

Rapidly increasing numbers
Average 10-20% of all stools tested =
Positive
Wide spectrum of CDI
1 recurrence 10-25% ptsRisk of 2nd recurrence ~65%
• Associated with hospital outbreaks of severe disease• Associated with severe morbidity (toxic mega-colon,
sepsis-like syndrome)• High case-fatality rate• Fluoroquinolone resistant• Produces >20x more toxin B (due to a deletion in TcdC
toxin production regulatory gene) & a binary toxinbinary toxin• Produces larger #s of spores, leading to larger inocula
and easier transmission
Toxinotype III
Emergence of an epidemic strain BI/NAP-1/027

Hand hygiene; gloves & gowns Switch to soap & water from gels Private room, contact precautions,
private commode – duration of diarrhea Remove environmental sources Chlorine cleaning agents Reduce non-essential antibiotics Antibiotic stewardship program
SHEA/IDSA Infect Control and Prevention Guidelines

Toxigenic culture is gold standard Toxigenic culture is gold standard
Cycloserine-cefoxitin-fructose agar with taurocholate
• Grow the organism • Test isolates for toxin
Plate direct or plate from
broth enrichment
Anaerobic incubation
<1% of U.S. labs doing this test and it takes at
least 4 days

Previous gold standard (2+ day TAT)Detection of Cytotoxin B direct from stool in cell culture Previous gold standard (2+ day TAT)Detection of Cytotoxin B direct from stool in cell culture
Normal, negative or toxin + antitoxin = neutralized (no effect)
Positive - CPE
Stool supernatant
<1% of U.S. labs doing this test and it takes at
least 2 days
Rapid antigen detection CDI assays Enzyme immunoassays and LFAs for toxins A&B or GDH
Enzyme immunoassays and LFAs for toxins A&B or GDH
>50% of U.S. labs still using this test type !!
Vidas
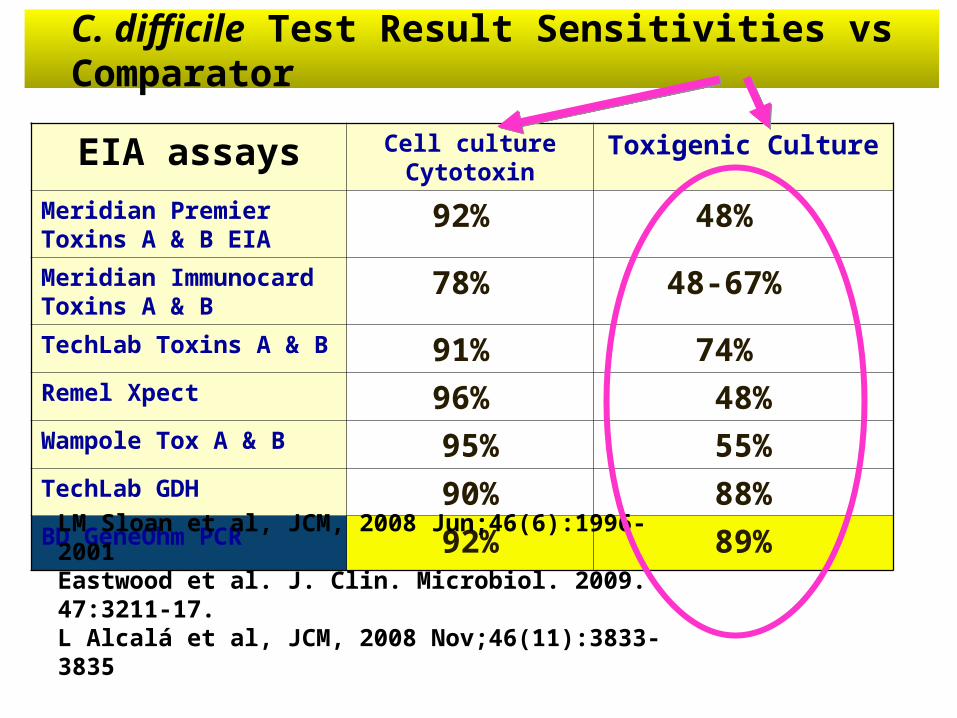
C. difficile Test Result Sensitivities vs Comparator
EIA assays Cell culture Cytotoxin
Toxigenic Culture
Meridian Premier Toxins A & B EIA
92% 48%
Meridian Immunocard Toxins A & B
78% 48-67%
TechLab Toxins A & B 91% 74% Remel Xpect 96% 48%Wampole Tox A & B 95% 55%TechLab GDH 90% 88%BD GeneOhm PCR 92% 89%
LM Sloan et al, JCM, 2008 Jun;46(6):1996-2001Eastwood et al. J. Clin. Microbiol. 2009. 47:3211-17.L Alcalá et al, JCM, 2008 Nov;46(11):3833-3835

Clinical and Infection Control Implications of C. difficile Infection With Negative Enzyme Immunoassay for ToxinGuerrero et al. 2011. CID 53:287-. (Cleveland VAMC)
• 132 PCR+ patients (unformed stools)• 43 (32%) EIA negative for toxin A or B (would have been missed if only EIA used for testing or determining whom to treat)
• No difference in presentations: (9 pts had severe CDI and one patient died of fulminant CDI)
• All patients had equal shedding of spores onto body and environment (same ribotype)
• Of 150 strains typed, 50% were 027 (significantly higher in EIA+ than EIA- patients)

Repeat test NOT needed for the diagnosis of CDI if PCR is the methodRobert F. Luo, Niaz Banaei (Stanford UMC) J. Clin. Microbiol. 2010. 48:3738-
Result following the first test with a negative result
293 patients (24% of all pts)406 repeat tests (ave. 1.5/pt)PCR Sens 87.2%; Spec 98.6%
7 new TP’s at ≥7 days
<1% repeat tests gave +
result <7 days
Evaluation of the Cepheid Xpert Clostridium difficile Epi assay for diagnosis of Clostridium difficile infection and typing of the NAP1 strain at a cancer hospital Babady et al. 2010. J Clin Microbiol 48:4519
• 126 patients; 60 had 027. Compared to patients with non 027 strains, they were more likely to:‒Die by day 90 after diagnosis‒Be older and/or residents of a LTCF‒Be treated for a longer duration of time‒Have therapy switched from metro to vanco
• Age, ICU admission, Charlson score, and infection with 027 were significant predictors of mortality
(hazard ratio 2.77)
In revision

EIA only GDH + EIA GDH + Xpert
Xpert C. diff
Sensitivity 58.3% 55.6% 86.1% 94.4% Specificity 94.7% 98.3% 97.8% 96.3%
PPV 68.9% 87.0% 95.8% 84.0%
NPV 91.9% 91.7% 97.2% 98.8%

C. diff PCR vs GDH in Clinical Trials for 027 vs Non-027 Isolates
Sensitivity P value
Ribotype Xpert GDH EIA
027 (11) 90.9% 90.9% 1.0
Non-027 (36) 91.7% 72.2% 0.001
Tenover, et al. 2010. JCM Vol. 48.
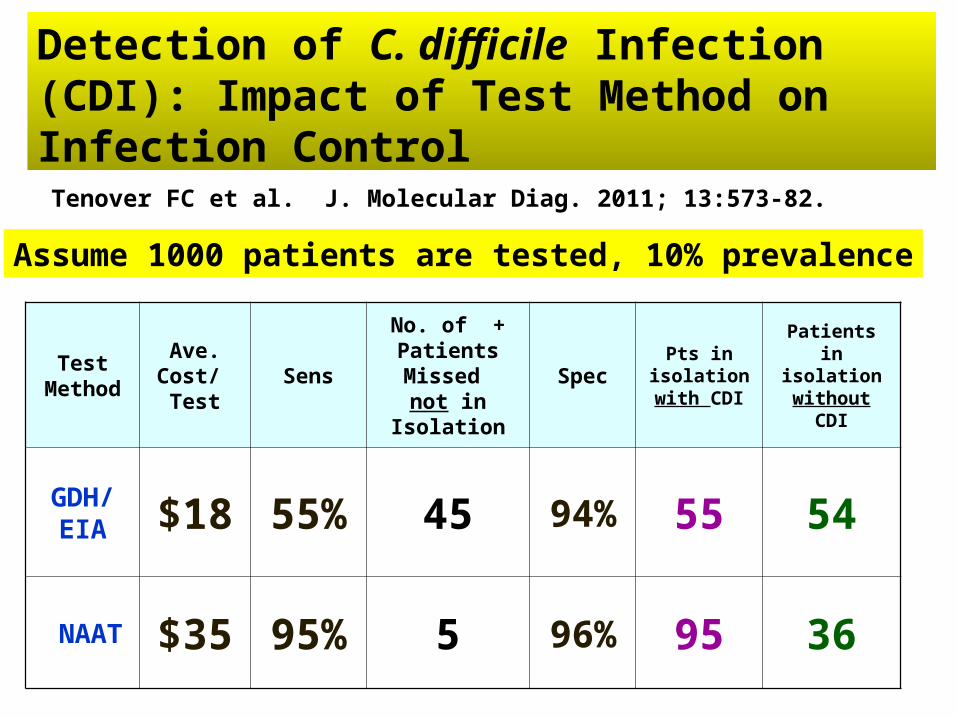
Detection of C. difficile Infection (CDI): Impact of Test Method on Infection Control Tenover FC et al. J. Molecular Diag. 2011; 13:573-82.
TestMethod
Ave. Cost/ Test
Sens
No. of + Patients Missed not in
Isolation
SpecPts in
isolation with CDI
Patients in isolation
without CDI
GDH/EIA $18 55% 45 94% 55 54
NAAT $35 95% 5 96% 95 36
Assume 1000 patients are tested, 10% prevalence

Photo by Dr. Curtis Donskey (Case Western)

Environmental Control Issues
(Am J Infect Control 2009;37:15-9.)(027/BI)
105 non-isolation rooms surveyed by culture 16% contaminated with toxin-producing C. difficile Outside of patient rooms:
9 of 29 (31%) physician work areas positive 1 of 10 (10%) nurse work areas 9 of 43 (21%) piece of portable equipment 50% of strains typed were epidemic NAP1 strain

Patient Death vs Binary Toxin Bacci et al. 2011. EID; 17:976-
027 Binary+
Non-027 Binary+
A+B+ Binary-
Non-typed
Relative risk of death in 30 days = 28% (RR 1.6-1.8) vs 17% death from CDI with non-binary toxin producing strain

Recurrence Rates for Fidaxomicin vs. VancoRecurrence Rates for Fidaxomicin vs. Vanco
Louie et al. 2011. Fidaxomicin versus Vancomycin for Clostridium difficile Infection. NEJM 364:422-31.
For pts. with 027 strain, recurrence rates were higher with Fidaxomicin than Vanco.
% recur-rence

Fecal transplant for CDI relapses orpatients non-responsive to antibiotics
Bakken et al. 2011. Treating Clostridium difficile Infection With Fecal Microbiota Transplantation. Clin. Gastroent. Hepatol. 9:1044–1049
van Nood et al. 2013. Duodenal infusion of donor feces for recurrent Clostridium difficile. NEJM. 368:407-15
% cured•Vanco•V+bowel lavage•V+BL+FMT
Poopsickle

MRSA surveillance: some data about one approach

• Patients are more ill with MRSA infections; more interventions, more resources• 18,650 deaths in U.S.A. each year• They cost more than infections with MSSA• MRSA infections = longer length of stay
$$$$$$ Days in hospitalDays in hospital
How will preventing MRSA infections reduce costs?
MRSA Cost data (Duke Univ. Med. Ctr.)
2009 vol 4 pg:e8305 -e8305
Patients with MRSA infections were 30 x more likely to be readmitted and 7 times more likely to die within 90 days.
Patients with MRSA infections cost $61,681 more than patients without infections and $38,000 more than with infections due to MSSA.
Therefore: prevention of one MRSA infection will save the hospital >$61,000.

Evaluation of rapid screening and pre-emptive contact isolationfor detecting and controlling methicillin-resistant Staphylococcusaureus in critical care: an interventional cohort studyHarbarth et al. 2006. Crit. Care Med.10:128.
93h TAT 22h TATPre-emptive
Isolation(or <1 h TAT)
Infected
Colonized

Broth enriched culture results (48 hrs) Sensitivity ~same as PCR. Wolk et al.
CA
MS- Broth enriched
orfX PCR
MrsaSel
“PCR is the improved gold standard..”
JCM 2009. 47: 3933-

VA Hospital systems1 Lucey Chrom Agar -> GeneXpert
2 Lucey Undecided3 Starr Undecided
4 Syed IDI-MRSA
5 Syed Chrome Agar
6 Braden Undecided VA Durham in process of renting Gx7 Jones Unknown Multiple mtgs set8 Jones Unknown
9 Vickery/Lucero IDI-MRSA Interest in Gx10 LaFave Chrome Agar -> ??
11 LaFave
15 Lucero16 Vickery/Moore17 Moore
18 Litavis/Moore
19 Moreno/Bell20 Bell21 Moreno
22 Litavis
23 Francis/Lucero
2121
2222
2323
2020
2020
1818
2121 88
881717
161677
66
111212
151599
111144
5533
1616
1919
1010

59% decrease in MRSA HAIs
Veterans Affairs Initiative to Prevent Methicillin-Resistant Staphylococcus aureus Infections
Jain et al. 2011. NEJM 364:1419-• 61% decrease in C. diff
in non-ICUs• 73% decrease in VRE
infections in non-ICUs
Massachusetts General Hospital adopts automated system for MRSA surveillance
A Randomized Controlled Trial Comparing Passive and Active Screening with Culture and Polymerase Chain Reaction. Shenoy et al. 2013, CID Sr. Author Dr. David Hooper
>2000 tests per day !

Patients removed from isolation if MRSA negative by active surveillance
• Nasal swabs cultured for 48 hours on BD Chromagar• Colonies confirmed by Gram stain and tube coagulase;
– culture took 5 days to complete– PCR took <1 day to complete
• 457 patient included in the analysis– Completion of the protocol: 10% in non-intervention arm ( standard
of care with no active enrollment)– Completion of protocol: 73% in intervention arm (i.e., all 3 cultures
and PCR tests were collected)• Results
– 66 patients in intervention arm were positive for MRSA in at least one culture; 60 were positive on the first culture, 3 on second, and 3 on third
– Discontinuation of contact precautions was 4 times more likely in the intervention (active surveillance) arm
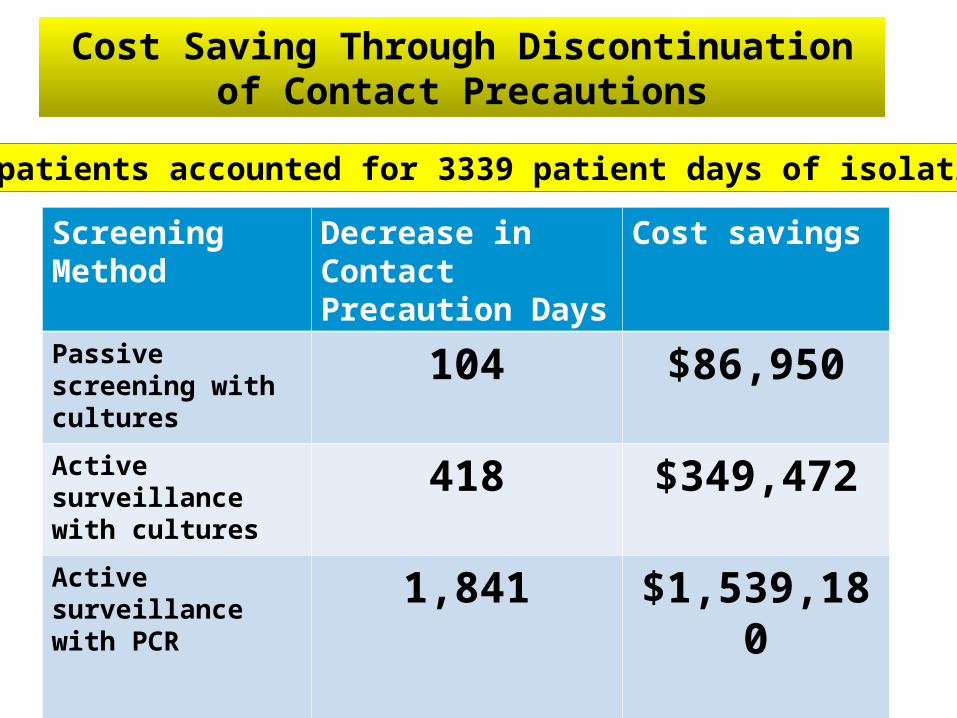
Cost Saving Through Discontinuation of Contact Precautions
Screening Method
Decrease in Contact Precaution Days
Cost savings
Passive screening with cultures
104 $86,950
Active surveillance with cultures
418 $349,472
Active surveillance with PCR
1,841 $1,539,180
457 patients accounted for 3339 patient days of isolation


















![Emerita Augusta[1]](https://img.dokumen.tips/doc/110x75/557201d74979599169a26e6d/emerita-augusta1.jpg)










