Embed Size (px)
Citation preview
INTRODUCTION
Primary oral diseases can be subdivided into conditions affect-ing the tooth, the periodontium or other oral tissues (Table 47-1). Diseases that affect tooth structure (Figure 47-1) may resultin lesions of the periodontal apparatus, oral mucosa or both.Diseases affecting the periodontium may result in exfoliation ofteeth. Additionally, primary diseases of other organs may causeoral lesions and are important considerations in formulatingdifferential diagnoses. Furthermore, oral disease can contributeto diseases of other organs and body systems.
Periodontal disease is the principal cause of tooth loss in dogsand cats. Food can influence periodontal disease through con-trol of plaque and thus is the primary focus of this chapter. Oralhealth is achieved through professional care and effectivehomecare; however, compliance is a significant issue in veteri-nary dentistry (Box 47-1). Traditional methods of plaque con-trol such as toothbrushing may be difficult for clients to accom-plish.Therefore use of an effective dental food can be an appro-
priate and effective means of daily plaque control and oralhealth maintenance for dogs and cats.
The steps in promoting oral health in dogs and cats include:1) controlling plaque, the cause of periodontal disease, 2) as-sessing the level of plaque control necessary to prevent gingivi-tis in each patient, 3) determining each pet owner’s ability tocontrol substrate accumulation and selecting methods mostlikely to ensure compliance, 4) feeding a food with an appropri-ate texture and nutritional profile and 5) recognizing that oralhealth may affect systemic health; therefore, a healthy oral cav-ity may affect longevity and quality of life.
CLINICAL IMPORTANCE
Prevalence of Periodontal DiseasePeriodontal disease is the most common disease of adult dogsand cats. As early as 1899, Eugene Talbot described “interstitialgingivitis or so-called pyorrhoea alveolaris” found in dogs atnecropsy (1899). In 1939, Wright noted that “the incidence of
Chapter
47Periodontal
Disease
Ellen I. Logan
Robert B. Wiggs
Dale Scherl
Paul Cleland
“Because periodontal disease is the most common problem affecting dogs and cats of all age groups, programs to prevent
periodontal disease should be considered among the most important prophylactic services we can offer.”
Gregg A. Dupont

disease of the teeth in the dog is so high that dental surgeryoccupies a prominent place in the work of the veterinarianengaged in small-animal practice. The most common affectionnecessitating surgical interference is paradontal disease” (1939).
Periodontal disease has been observed in dogs and cats ofvarying breed, gender and age. Surveys from several countriesreport prevalence rates of periodontal disease that range from60 to more than 80% of dogs and cats examined (Gray, 1923;Bell, 1965; Rosenberg et al, 1966; Saxe et al, 1967; Gad, 1968;Hamp et al, 1975; Hamp and Lindberg, 1971; Sorensen et al,1980; Page and Schroeder, 1979; Golden et al, 1982; Reichartet al, 1984; Isogai et al, 1989; Harvey, 1992; Hoffman andGaengler, 1996).
Data from the National Companion Animal Study represent-ing 54 veterinary practices across the United States confirmedthat oral disease was the most frequent diagnosis in all age cat-egories of 39,556 dogs and 13,924 cats (Lund et al, 1999).
PATIENT ASSESSMENT
HistoryA complete history is important to diagnosis and treatmentplanning and is an integral tool for developing a complete
health maintenance program for pets. An adequate health his-tory must include: 1) information about previous medical andsurgical procedures, 2) current preventive measures such as vac-cination status and heartworm medication administration, 3)the pet’s general environment, including confinement, 4) infor-mation about other household pets and 5) who in the house-hold is responsible for primary care.
Inquiries specific to nutrition and oral care should includepast and present information about: 1) oral hygiene and level ofcompliance, 2) presence of any signs that may be related to oraldysfunction, 3) chewing behavior, 4) access to rocks and othermaterials that may cause occlusal trauma, 5) access to dentaltreats and toys, 6) eating behavior and 7) foods eaten, with spe-cial attention given to texture and other factors.
Physical ExaminationInitial Oral ExaminationExamination of the skull and oral cavity should be a regularpart of every physical examination. An extraoral examinationshould be done before opening the mouth to inspect the skulland facial areas for any abnormalities, such as muscle atrophy,swelling, draining tracts and ocular or nasal discharge. Extraoralexamination should also include inspection for facial symmetry,
Small Animal Clinical Nutrition980
Table 47-1. Conditions affecting the oral cavity.
Conditions primarily affectingConditions primarily the periodontium/oral affecting teeth mucosaAbrasion Chemical or thermal burnsAttrition Gingival hyperplasiaErosion GingivitisFracture GingivostomatitisIntrinsic staining NeoplasiaOdontoclastic resorption Periapical abscessPulpitis Periodontitis
Ulcers
Oral health is achieved through an effective periodontal man-agement program that includes professional care and client-provided homecare. Appropriate homecare recommendationsconsider the client and patient preferences and specificallyaddress the degree of oral pathologic change present and clientand patient compliance.
Compliance is critical to effective homecare. Clients must bewilling and able to perform the recommended hygiene and thepatient must accept oral hygiene procedures. Noncompliancemay result from lack of an effective recommendation by the vet-erinary health care team. A comprehensive study of compliancedemonstrated that appropriate periodontal therapy was not pro-vided for approximately 15.5 million dogs and cats with record-ed periodontal disease scores of 2, 3 or 4. No recommendationfor periodontal management was given in 66% of cases with arecorded periodontal disease score of 1. In the same study, 19%of patients lacked any notation of periodontal examination orscore in health records.
Even with client education and good pet compliance, someowners are unable to provide routine and effective plaque con-trol. Compliance failure may be due to: 1) lack of skill, 2) lack ofperceived benefit, 3) unpleasantness of procedure, 4) lack ofnoticeable impact and 5) lifestyle constraints. Emphasizing thebenefits, including improved oral and systemic health, lessbreath odor, cost effectiveness and strengthening of the owner-pet bond, may increase compliance.
The most important part of periodontal therapy is how well apatient maintains oral health. Long-term success depends onthe degree of plaque control the client is capable of providingbetween professional visits.
Box 47-1. Compliance and DentalHomecare.
Figure 47-1. Normal tooth and periodontal anatomy.
palpation of the temporomandibular joints, regional lymphnodes and salivary glands and thorough inspection of the skinand lips. Extraoral abnormalities related to oral dysfunctionmay include mucopurulent discharge from the eyes or nostrils,soft or hard swellings, crepitus, salivation and an inability toopen or close the mouth (Marretta, 1987, 1992; Kapatkin et al,1991; Ramsey et al, 1996).
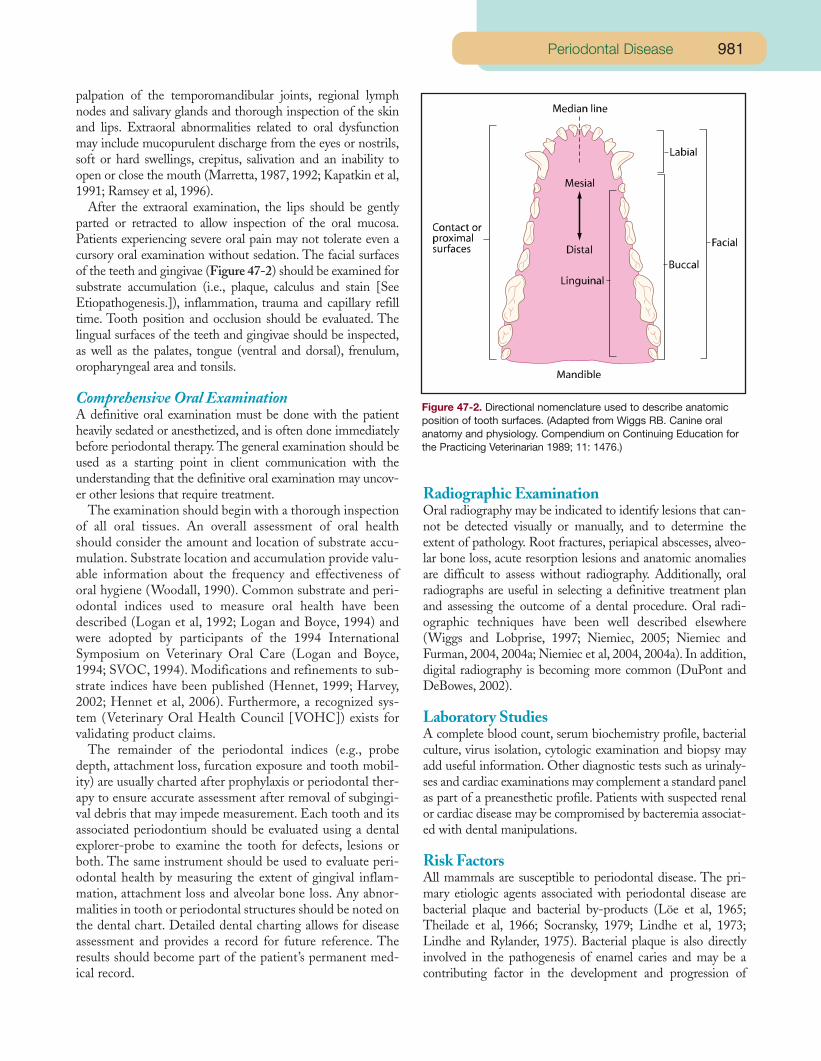
After the extraoral examination, the lips should be gentlyparted or retracted to allow inspection of the oral mucosa.Patients experiencing severe oral pain may not tolerate even acursory oral examination without sedation. The facial surfacesof the teeth and gingivae (Figure 47-2) should be examined forsubstrate accumulation (i.e., plaque, calculus and stain [SeeEtiopathogenesis.]), inflammation, trauma and capillary refilltime. Tooth position and occlusion should be evaluated. Thelingual surfaces of the teeth and gingivae should be inspected,as well as the palates, tongue (ventral and dorsal), frenulum,oropharyngeal area and tonsils.
Comprehensive Oral ExaminationA definitive oral examination must be done with the patientheavily sedated or anesthetized, and is often done immediatelybefore periodontal therapy. The general examination should beused as a starting point in client communication with theunderstanding that the definitive oral examination may uncov-er other lesions that require treatment.
The examination should begin with a thorough inspectionof all oral tissues. An overall assessment of oral healthshould consider the amount and location of substrate accu-mulation. Substrate location and accumulation provide valu-able information about the frequency and effectiveness oforal hygiene (Woodall, 1990). Common substrate and peri-odontal indices used to measure oral health have beendescribed (Logan et al, 1992; Logan and Boyce, 1994) andwere adopted by participants of the 1994 InternationalSymposium on Veterinary Oral Care (Logan and Boyce,1994; SVOC, 1994). Modifications and refinements to sub-strate indices have been published (Hennet, 1999; Harvey,2002; Hennet et al, 2006). Furthermore, a recognized sys-tem (Veterinary Oral Health Council [VOHC]) exists forvalidating product claims.
The remainder of the periodontal indices (e.g., probedepth, attachment loss, furcation exposure and tooth mobil-ity) are usually charted after prophylaxis or periodontal ther-apy to ensure accurate assessment after removal of subgingi-val debris that may impede measurement. Each tooth and itsassociated periodontium should be evaluated using a dentalexplorer-probe to examine the tooth for defects, lesions orboth. The same instrument should be used to evaluate peri-odontal health by measuring the extent of gingival inflam-mation, attachment loss and alveolar bone loss. Any abnor-malities in tooth or periodontal structures should be noted onthe dental chart. Detailed dental charting allows for diseaseassessment and provides a record for future reference. Theresults should become part of the patient’s permanent med-ical record.
Radiographic ExaminationOral radiography may be indicated to identify lesions that can-not be detected visually or manually, and to determine theextent of pathology. Root fractures, periapical abscesses, alveo-lar bone loss, acute resorption lesions and anatomic anomaliesare difficult to assess without radiography. Additionally, oralradiographs are useful in selecting a definitive treatment planand assessing the outcome of a dental procedure. Oral radi-ographic techniques have been well described elsewhere(Wiggs and Lobprise, 1997; Niemiec, 2005; Niemiec andFurman, 2004, 2004a; Niemiec et al, 2004, 2004a). In addition,digital radiography is becoming more common (DuPont andDeBowes, 2002).
Laboratory StudiesA complete blood count, serum biochemistry profile, bacterialculture, virus isolation, cytologic examination and biopsy mayadd useful information. Other diagnostic tests such as urinaly-ses and cardiac examinations may complement a standard panelas part of a preanesthetic profile. Patients with suspected renalor cardiac disease may be compromised by bacteremia associat-ed with dental manipulations.
Risk FactorsAll mammals are susceptible to periodontal disease. The pri-mary etiologic agents associated with periodontal disease arebacterial plaque and bacterial by-products (Löe et al, 1965;Theilade et al, 1966; Socransky, 1979; Lindhe et al, 1973;Lindhe and Rylander, 1975). Bacterial plaque is also directlyinvolved in the pathogenesis of enamel caries and may be acontributing factor in the development and progression of
981Periodontal Disease
Figure 47-2. Directional nomenclature used to describe anatomicposition of tooth surfaces. (Adapted from Wiggs RB. Canine oralanatomy and physiology. Compendium on Continuing Education forthe Practicing Veterinarian 1989; 11: 1476.)

tooth resorption and other oral inflammatory lesions. Any fac-tor that enhances bacterial accumulation or affects the resist-ance of the periodontium may influence the disease process.Specific risk factors that contribute to the severity and progres-sion of periodontal diseases include: 1) breed, 2) age, 3) im-munocompetence, 4) nutrition and food characteristics, 5)chewing behavior and 6) systemic health (Wiggs, 1995).
BreedBreed plays a major role in the development of dental disease.Small, toy and brachycephalic breeds are prone to malocclusivedisorders including overcrowding and rotation of teeth,retained deciduous teeth and supernumerary teeth. Occlusalabnormalities provide plaque retentive areas and increase thedifficulty of oral hygiene procedures. Brachycephalic breeds arealso predisposed to mouth breathing, which tends to dry andirritate oral tissues (West-Hyde and Floyd, 1995). Periodontaldisease, tooth resorption and gingivostomatitis have been re-ported to occur with relatively greater frequency in purebredcats, particularly Asian breeds such as Siamese and Abyssinians(Van Wessum et al, 1992). Ulcerative stomatitis has been doc-umented to occur in family clusters of Maltese dogs (Harveyand Emily, 1993).
AgeSeveral surveys have reported that older pets have a greater fre-quency and an increased severity of dental disease. One reportof a survey of owners of 1,350 dogs noted that calculus deposi-tion, gingival inflammation, tooth mobility, furcation exposure,attachment loss and missing teeth all increased significantlywith increasing age (Harvey et al, 1994). In an evaluation of4,776 cats aged seven to 25 years and 8,692 dogs aged 10 to 25years, oral disease was the most frequent diagnosis reported(Lund et al, 1999).
It has long been reported that periodontal disease in people
increases in severity with increasing age. Recent data suggestthat the severity may represent a lifetime disease accumulationand not necessarily be an age-specific condition (Page, 1984;Van der Velden, 1984; Johnson et al, 1989).There may be someage-related changes that could negatively affect oral health,such as decreased salivary flow and antioxidant capacity (Doddset al, 2005; Aejmelaeus et al, 1997; Navazesh, 2002). It is notsurprising that geriatric pets with little history of oral hygieneor veterinary oral care demonstrate an increased prevalence andseverity of periodontal disease.
ImmunocompetenceThe host immune response protects against systemic infectionfrom periodontal pathogens. An over exaggerated immune re-sponse can cause severe local periodontal destruction. An inad-equate immune response may predispose pets to opportunisticor overwhelming systemic infection (Genco, 1992).
Nutrition and Food CharacteristicsThe dramatic difference in food form represented by commer-cial dog and cat foods as compared with the natural prey of wildcanids and felids is often implicated as a significant cause of thedegree of periodontal disease diagnosed in domestic dogs andcats (Gray, 1923; Colyer, 1990; Watson, 1994). Colyer exam-ined 1,157 wild canid skulls and reported that periodontal dis-ease as suggested by alveolar bone destruction was present inonly 2% of specimens (1990). The subject of how well specificcommercial food types promote oral health is discussed below.
Box 47-2 reviews a common concern of pet owners regard-ing food sugar content and dental caries and Box 47-3 discuss-es the role of topical coatings of dry cat foods in feline toothresorption. Although not associated with periodontal disease,these text boxes are included because the topics relate to foodand dental diseases.
EtiopathogenesisTooth-Accumulated MaterialsSeveral materials accumulate on tooth surfaces and participatein the pathophysiology of dental and periodontal disease. Thesesubstances are commonly referred to as tooth-accumulatedmaterials or dental substrates and are categorized as: 1) acquiredenamel pellicle, 2) microbial plaque, 3) materia alba/debris, 4)calculus and 5) stain. These substrates accumulate in a dynamiccontinuum, initiated by the adsorption of salivary constituentsonto tooth surfaces (Fedi, 1985; Schwartz et al, 1971).
Saliva is a critical oral fluid primarily recognized for its diges-tive functions. However, saliva also bathes the oral cavity witha fluid rich in proteins (e.g., enzymes), glycoproteins, elec-trolytes, lipids, antioxidants, antimicrobial peptides (defensins),immunoglobulins, bicarbonate ions and mucins that provide aninitial protective barrier to pathogenic invasion, lubricate andclean the oral cavity and aid in the transportation of solids(Lingström and Moynihan, 2003; Mizukawa et al, 1999). Inpeople, diminished salivary function (xerostomia) is associatedwith increased prevalence of caries and periodontal disease,mucosal irritation, difficulties in chewing and swallowing and
Small Animal Clinical Nutrition982
The role of digestible (soluble) carbohydrates (sugars) in the de-velopment of dental caries has been well documented in peopleand rodents. Dental caries, however, occurs infrequently in dogsand cats. One study demonstrated that dogs do not develop car-ious lesions even after long periods of consuming carbohydrate-rich foods. Carlsson and Egelberg reported that the addition ofsucrose to a soft food resulted in no difference in plaque accu-mulation and gingival inflammation in a group of 12 mongreldogs. Human studies have demonstrated that larger amounts ofplaque were formed when sucrose was the primary sugar con-sumed. Commercial and homemade pet foods typically containlarge quantities of digestible carbohydrates, usually in the formof starch.
The Bibliography for Box 47-2 can be found at www.markmorris.org.
Box 47-2. Digestible Carbohydrates and Their Role in Oral Health of Dogs and Cats.

impaired taste. Saliva initiates film formation on all oral sur-faces (Scannapieco and Levine, 1990; Navazesh, 2002).
ENAMEL PELLICLEEnamel pellicle is a thin film or cuticle. Early enamel pellicle
is composed of proteins and glycoproteins deposited from sali-va and gingival crevicular fluid. Early enamel pellicle protectsand lubricates. However, as pellicle ages, existing constituentsare modified and additional salivary, crevicular and bacterialcomponents are incorporated. Enamel pellicle and its compo-nents provide a framework for initial bacterial colonization andalso function in the maturation of dental plaque (Scannapiecoand Levine, 1990; Rolla, 1983).
DENTAL PLAQUEPellicle deposition and subsequent bacterial colonization
occur almost immediately after a dental prophylaxis. Studieshave demonstrated that within minutes after polishing, ap-proximately one million organisms are deposited per mm2 ofenamel surface (Lindhe, 1989). Aggregates of bacteria com-bine with salivary glycoproteins, extracellular polysaccharidesand occasionally epithelial and inflammatory cells to form asoft adherent plaque that covers tooth surfaces. Dental plaqueis not easily removed by normal tongue actions, water drink-ing or forced water spray, but can be affected by mechanicaland chemical means.
Dental plaque has a specific composition and structure thatchanges with time (DuPont, 1997). Supragingival dentalplaque forms above and along the free gingival margin; subgin-gival dental plaque is formed entirely within the gingival sulcus.Growth and maturation of supragingival plaque are necessaryfor subsequent colonization of subgingival surfaces by dentalplaque (Kornman, 1986). Supragingival and subgingival plaqueare distinct compositional masses that influence the inflamma-tory reaction of gingival tissues. Studies in people have demon-strated an organized progression of microbial colonization andgrowth that leads to the development of mature pathogenicdental plaque (Lindhe, 1989).
Canine and feline studies characterizing the microbial com-position of supragingival and subgingival plaque have beenreported. Supragingival plaque in dogs with clinically healthygingivae is primarily composed of gram-positive aerobic organ-isms. As plaque matures, the bacterial composition shifts to apredominately gram-negative anaerobic flora (Courant et al,1968; Soames and Davis, 1974; Wunder et al, 1976; Syed et al,1980, 1981; Svanberg et al, 1982; Isogai et al, 1988; Malloneeet al, 1988; Hennet and Harvey, 1991, 1991a, 1991b; Boyce etal, 1995; Harvey et al, 1995). Several sources have detailed listsof specific bacteria associated with periodontal diseases of dogs(Hardham et al, 2005; Syed et al, 1980; Wunder et al, 1976;Hennet and Harvey, 1991, 1991a, 1991b; Allaker et al, 1997;Isogai et al, 1989; Svanbert et al, 1982) and cats (Mallonee etal, 1988). The inflammation and destruction that accompaniesperiodontal disease results from the direct action of bacteria andtheir by-products on periodontal tissues and the indirect activa-tion of the host immune response (Genco, 1990). Thus, bacte-
rial plaque is the most important substrate in the developmentof periodontal disease.
MATERIA ALBA AND OTHER ORAL DEBRIS Materia alba is a soft mixture of salivary proteins, bacteria,
desquamated epithelial cells and leukocyte fragments. Materiaalba and dental plaque are two distinct materials. Materia alba
983Periodontal Disease
Although the etiology of tooth resorption in cats is unknown,examination of skulls that pre-date the 1960s revealed a lowerprevalence of tooth resorption than current estimates, whichsuggests a relatively recent increase. Commercial foods havebeen implicated as a causative factor in the increased detectionof tooth resorption in cats based on several physical and chem-ical properties of these foods.
Questions have been raised that relate to the common prac-tice of applying an acidic coating to dry cat foods (i.e., felinedigest) to enhance palatability. Human studies have demonstrat-ed that consumption of a food or beverage with an acidic pHcontributes to erosive lesions. Additionally, chronic vom-iting/regurgitation have been associated with these lesionsbecause vomitus is acidic. To address this issue, Zetner andSteurer investigated the tooth surface pH of cats with 1) toothresorption, 2) chronic oral inflammatory disease and 3) cats withno oral lesions. These researchers also measured tooth surfacepH after cats consumed either a commercial moist food or acommercial acid-coated dry food. Results from this studydemonstrated that cats with tooth resorption had lower tooth-surface pH values than healthy cats, but that consumption of thedry food was not associated with the pathogenesis of odonto-clastic resorptive lesions.
It has also been suggested that hard dry cat foods causemicrofractures that predispose teeth to infection and initiate theinflammatory cascade leading to odontoclastic activation.However, it must also be noted that teeth that are not normallyassociated with mechanical forces related to consuming dryfoods are also susceptible to tooth resorption.
Finally, recent work has implicated dietary vitamin D in the eti-ology of tooth resorption. Evidence in support of this theoryincludes the correlation between cats with tooth resorption andincreased blood levels of 25-hydroxyvitamin D, and histologiccomparisons of the effects of excessive intake of vitamin D tothe effects of tooth resorption. Because cats cannot synthesizevitamin D, they must rely on their diet to supply the nutritionalrequirement.
Definitive studies that document a cause-and-effect relation-ship implicating a single etiologic factor have not yet been done,and care must be taken to maintain distinctions between casu-al and causal relationships when evaluating current information.In addition, it is possible that tooth resorption has a multifactor-ial etiology, highlighting the complexity of the problem andemphasizing the need for additional research.
The Bibliography for Box 47-3 can be found at www.markmorris.org.
Box 47-3. Do Commercial Cat FoodsCause Tooth Resorption?

does not have the organized bacterial structure or the adherenceproperties of dental plaque (Schwartz et al, 1971); it can gener-ally be washed off with a forced water spray. The role of mate-ria alba in the etiopathogenesis of plaque accumulation andperiodontal disease remains unclear.
Other debris commonly observed in the oral cavity of dogsand to some extent in cats includes food, impacted hair andmiscellaneous foreign materials acquired through chewingbehaviors. Food debris retained in the mouth after eating canusually be removed by the action of the tongue and saliva.
Dogs and cats fed soft, sticky foods, particularly those breedscompromised by occlusal abnormalities, may retain more fooddebris. No reports directly correlate retention of food debriswith increased plaque accumulation and periodontal disease indogs and cats. Egelberg reported that neither the frequency offeeding nor bypassing the oral cavity by tube feeding affectedthe accumulation of plaque and the development of gingivitisin a group of six mixed-breed dogs with medium to large bodysize (1965). The effect of food retention in small and brachy-cephalic breeds is unknown. Retained or impacted debris mayact as a nidus for plaque accumulation and exacerbate gingivalinflammation. The role of food type and texture in oral healthand disease is discussed below.
DENTAL CALCULUSDental calculus is mineralized plaque. Calculus is a hard
substrate formed by the interactions of salivary and crevicularcalcium and phosphate salts with existing plaque. Dental cal-culus is observed frequently in dogs and cats (Harvey, 1992;Harvey et al, 1994; Richardson, 1965; Coignoul and Cheville,1984) but differs in its composition. Feline calculus is com-prised mostly of carbonate-containing hydroxyapatite, where-as canine calculus is comprised mostly of calcium carbonate(calcite) (Clarke, 1999; Legeros and Shannon, 1979).Calculus accumulates supragingivally and subgingivally; cal-culus deposits thicken with time. Undisturbed calculus isalways covered by vital dental plaque. Aged calculus may chipor break off with mastication; however, a film of plaqueremains that is rapidly mineralized. Calculus provides aroughened surface to enhance plaque attachment and accu-mulation and chronically irritates gingival tissues (Lindhe,1989a; Mandel, 1990; Schroeder, 1969). A study in dogsdemonstrated that calculus control in the absence of plaquecontrol is cosmetic only; thus, preventive or therapeutic pro-tocols to control periodontal disease should always includeanti-plaque measures (Warrick et al, 2003).
DENTAL STAINAcquired dental stain (extrinsic stain) is initially stained pel-
licle that becomes part of the mineralized, layered laminate ofpellicle, plaque and calculus. Dental stain occurs frequently indogs (Schemehorn et al, 1982). Various nutritional, chemicaland bacterial factors affect the presence and intensity of stain.Although nonpathogenic, dental stain is of aesthetic concern topet owners and may signal teeth abnormalities.
Enamel staining (intrinsic stain) occurs due to trauma or
antibiotic administration during development or before tootheruption. Erupted teeth may also be injured with resulting dis-coloration due to hemorrhage into the dentinal tubules.
Enamel staining varies in intensity and distribution of discol-oration and is distinguished from acquired stain by its irre-versible nature (Robinson et al, 1983).
Pathophysiologic Basis of Clinical SignsPERIODONTAL DISEASEIn susceptible patients, plaque accumulation along the gingi-
val margin induces inflammation in adjacent gingival tissues.Without plaque removal or control, gingivitis progresses inseverity to include local changes that allow subsequent bacterialcolonization of subgingival sites. Inflammatory mediators dam-age the integrity of the gingival margin and sulcular epithelium,allowing further infiltration of bacteria. The immune responseof the host attempts to localize the invasion of periodontal tis-sues; the result may be further destruction of local tissues due tocytokines released from inflammatory cells (Grove, 1982;Genco, 1984, 1990; DeBowes, 2000; Harvey, 2005).
Periodontal disease is episodic with periods of active tissuedestruction followed by periods of inactivity and healing(Figure 47-3). Additionally, not all teeth are affected at thesame rate or to the same degree. Periodontal disease beginswith gingivitis and progresses through increased destruction ofthe periodontal apparatus, resulting in tooth mobility and even-tual tooth loss. Generally, a stage classification system is used,beginning with a healthy periodontium and ending with toothexfoliation (Table 47-2 and Figure 47-4) (Wiggs and Lobprise,1997a).
Periodontal disease is often a silent process that progresseswithout detection. Even in severe cases, dogs and cats may notdemonstrate obvious discomfort. One signal often noticed bypet owners is oral malodor (Hennet et al, 1995), but even then,pet owners may not link bad breath to periodontal disease. Oraldisease is a primary cause of offensive breath odor, but othermetabolic processes may be involved (Tonzetich, 1977, 1978;Preti et al, 1992; Chen et al, 1970). A positive correlation be-tween periodontal disease and malodor has been found in bea-gles (Simone et al, 1997).
Other signs of periodontal disease include: 1) accumulationof dental substrates on tooth surfaces, 2) gingival redness, 3)swelling and bleeding of the gingival margin, 4) gingival reces-sion, 5) periodontal pocket formation, 6) accumulation of puru-lent material in the gingival sulcus or periodontal pocket and 7)tissue destruction with loss of attachment, furcation exposureand tooth mobility (Table 47-3).
Systemic Complications of Periodontal DiseasePeriodontal disease may predispose affected pets to systemic
complications. In people, periodontal disease has been linked toarthritis, low birth weight and pre-term birth, cardiovasculardisease, stress and anxiety, diabetes, obesity and stroke (Ham-ilton, 2005; Mandel, 2004; Newman, 1996; O’Reilly andClaffey, 2000; Rutkauskas, 2000; Gaffar and Volpe, 2004;Klages et al, 2005; Roman, 2003; Dorfer et al, 2004).
Small Animal Clinical Nutrition984

Although much of the evidence is based on documentationof correlations between oral and systemic health, and the effectof systemic diseases on the health of the oral cavity (particular-ly in the case of diabetes) (Mealey, 1998; Levin et al, 1996), dataare emerging that suggest a more causal and two-way relation-ship that makes a case for periodontal therapy as an adjunctivetreatment to classic disease therapies (D’Aiuto et al, 2004;Montebugnoli et al, 2005; Montebugnoli, 2004; Farooqi et al,2004; Kiran et al, 2005; Mealey, 2000; Miller et al, 1992;Pucher and Stewart, 2004; Taylor et al, 2004; Rahman et al,2005; Mercanoglu et al, 2004).
In dogs, numerous reports speculate on the associationbetween chronic periodontal disease and conditions affectingthe heart valves and pulmonary airways (Hamlin, 1990;Prueter and Sherding, 1985; Calvert and Dow, 1990; Bona-gura, 1981). Furthermore, a positive correlation has beenfound between the severity of periodontal disease andhistopathologic changes in the kidneys, myocardium and liver(DeBowes et al, 1996). Periodontal infections allow bacterialmigration into lymphatic and blood vessels, resulting in bac-teremia and are associated with increased levels of many of thesystemic markers associated with the diseases describedabove, including C-reactive protein, proinflammatory cyto-kines, serum cholesterol, plasma fibrinogen, white blood cellsand blood glucose (Harari et al, 1993, 1991; Slade et al, 2000;
Ide et al, 2004; D’Aiuto et al, 2004, 2005; Joshipura et al,2004; Lowe, 2004; Holzhausen et al, 2004). The host defens-es of normal healthy pets can effectively clear transient bac-teremia; however, blood-borne bacteria may colonize distantsites in patients impairing immune function and/or compro-mising organ function, including development of atheroscle-rotic lesions (Calvert and Green, 1986; Glurich et al, 2002).
985Periodontal Disease
Figure 47-3. Host-bacterial interactions in the pathogenesis of periodontal disease. Periodontal disease is cyclic with bursts of tissue destruc-tion followed by periods of healing and relative quiescence. Four stages in the pathogenesis of periodontal disease have been proposed: 1)Microbial colonization. Salivary pellicle is deposited on the enamel surface and is soon colonized by oral bacteria that multiply forming plaque.2) Microbial invasion. Plaque bacteria and their by-products invade the gingival tissues and initiate a host inflammatory response. 3) Tissuedestruction. Direct toxic effects of bacteria and their by-products and indirect host-mediated toxic responses lead to destruction of periodontaltissue. 4) Healing. Periods of disease remission are characterized by a reduction in the inflammatory response and gingival healing. (Adaptedfrom Genco RJ, Goldman HM, Cohen WD, eds. Contemporary Periodontics. St Louis, MO: CV Mosby Co, 1990; 189.)
Table 47-2. Stages of periodontal disease.*
Stage 0 Clinically normalNo gingival inflammation or periodontitis clinically evident.
Stage 1 Gingivitis onlyNo attachment loss. Height and architecture of the alveolar margin are normal.
Stage 2 Early periodontitisLess than 25% attachment loss or Stage 1 furcationinvolvement in multirooted teeth.
Stage 3 Moderate periodontitis25 to 50% attachment loss or Stage 2 furcationinvolvement in multirooted teeth.
Stage 4 Advanced periodontitisGreater than 50% attachment loss or Stage 3 furca-tion involvement in multirooted teeth.
*Adapted from AVDC.org. Wolf HF, Rateitschak EM, RateitschakKH, et al. Color atlas of dental medicine: Periodontology, 3rd ed.Stuttgart, Germany: Georg Thieme Verlag, 2005.

Key Nutritional FactorsThe key nutritional factors for oral health should provide a suf-ficient level of plaque control to prevent periodontal disease andgingivitis. Proper food texture and composition can directlyaffect the oral environment through: 1) maintenance of tissue
integrity, 2) alteration of bacterial plaque metabolism, 3) stim-ulation of salivary flow, 4) cleansing of tooth and oral surfacesby appropriate physical contact and/or 5) chelation of calculo-genic constituents (Box 47-4). However, control of calculus is asecondary consideration because calculus control by itself hasnot been shown to decrease gingivitis and periodontal disease.Calculus along with stain and malodor are more of a cosmeticconcern.
Assessing the relative efficacy of an oral health related keynutritional factor is complex. It is more practical to determinethe overall benefit of these constituents in a finished product.However, it can be very confusing for veterinarians, and partic-ularly for pet owners, to discern which products provide signif-icant dental benefits and thus warrant use as oral hygieneagents. The Center for Veterinary Medicine of the Food andDrug Administration (CVM-FDA) monitors and regulatesdental health claims in the United States. Cosmetic claims arenot objectionable and structure-function claims are not strin-gently regulated; thus, the wide availability of products thatmake some type of plaque or calculus claim with little or noresearch to document their effectiveness. Phrases such as“cleans teeth, freshens breath” are commonplace on commercialfood and treats packages. Because “crunchy” texture provideslittle dental benefit, the purported ability of these types of prod-ucts to provide any significant level of oral hygiene is a misrep-resentation to pet owners.
However, standardized scientific methods by which plaque(and calculus) accumulation are measured in dogs and cats forevaluating product efficacy have been established by the inter-national veterinary dental community (Boyce, 1992; Logan andBoyce, 1994; SVOC, 1994; Harvey, 1995; Logan et al, 1995;Logan, 1996, 1996a; Hennet, 1999; Harvey, 2002; Hennet etal, 2006). Box 47-5 discusses these methods and the VOHCSeal of Acceptance. The presence of a VOHC Seal of Ac-ceptance for plaque or plaque and calculus and/or publishedevidence-based studies helps determine which products areeffective.
Because foods that provide dental health benefits replace reg-ular maintenance foods, several key nutritional factors are in-cluded because of their relationship to general health ratherthan specific benefits for periodontal disease. The key nutri-tional factors for dental foods for dogs and cats are summarizedin Table 47-4 and discussed in more detail below.
Food TextureThe physical consistency, or texture, of foods and treats has longbeen thought to affect the oral health of dogs and cats. Manyof the recommendations made about the effect of food textureon oral health are unsubstantiated and several have turned outto be untrue when exposed to rigorous study, including “natu-ral foods” (Box 47-6). However, food texture can be a veryeffective means of controlling dental plaque and ultimatelyperiodontal disease.
Numerous studies have reported that dogs and cats fed softfoods have increased accumulation of plaque and calculus and ahigher prevalence or severity of periodontal disease when com-
Small Animal Clinical Nutrition986
Figure 47-4. Photographic representations of mild, moderate andsevere periodontal disease in dogs. (Top) Mild periodontal disease.Some accumulation of plaque and calculus is evident on toothcrowns. There is slight gingival recession around the maxillarycanine tooth and the gingival margins are slightly rounded, particu-larly around the caudal premolar teeth. (Middle) Heavy plaque andcalculus accumulation is evident on most teeth. Accumulations areabundant on the maxillary fourth premolar and first molar. A distinctmargin of gingival inflammation is present around the maxillaryfourth premolar. Inflammatory changes including swelling, reddeningand recession are evident around most teeth. (Bottom) Gross plaqueand calculus accumulation is present on premolar and molar teeth.Distinct marginal gingivitis with severe gingival recession and peri-odontal tissue loss is present. Impaction of hair and foreign materialoccurs commonly at sites of severe tissue destruction.

pared with the same parameters in pets fed hard foods. Thesestudies are difficult to compare because different methods wereused to assess substrate accumulation and gingival health, anddifferent populations of patients were studied.
Feeding recommendations for oral health commonlyinclude feeding a dry pet food. Hard food purportedly in-creases mastication, which aids oral health by exercising thegums, increasing keratinization of the gingivae and reducingaccumulation of plaque and calculus (O’Rourke, 1947). Butmany of the studies traditionally cited to substantiate claimsthat dry foods reduce accumulation of plaque and calculus areold reports that used small numbers of subjects, had varyingevaluation methods and did not report data analysis(Burwasser and Hill, 1939; Egelberg, 1965a; Krasse and Brill,1960; Studer and Stapley, 1973).
Consumption of soft foods may promote plaque accumula-tion. However, the general belief that dry foods provide signif-icant oral cleansing should be regarded with skepticism. Amoist food may perform similarly to a typical dry food inaffecting plaque, stain and calculus accumulation (Figure 47-5)(Boyce and Logan, 1994). In a large epidemiologic survey, dogsconsuming dry food alone did not consistently demonstrateimproved periodontal health when compared with dogs eatingmoist foods (Harvey et al, 1996). Also, periodontal disease is
the most common disease in dogs and cats (Lund et al, 1999);however, most dogs and cats eat dry foods.
Thus, typical commercial dry dog and cat foods contribute
987Periodontal Disease
Table 47-3. Clinical signs associated with periodontal disease.
Anorexia Red, swollen or bleeding gingivaeBehavioral changes Substrate accumulation (plaque, Difficulty eating calculus, stain)Halitosis Tooth mobilityHead shaking Ulcerations on gingivae or oral mucosaPtyalism
Table 47-4. Key nutritional factors for foods for dogs and catsfor prevention of periodontal disease and maintenance of overallhealth.*
Factors Dogs CatsFood texture VOHC Seal for VOHC Seal for
plaque control plaque controlAntioxidants
Vitamin E (IU/kg) ≥400 ≥500Vitamin C (mg/kg) ≥100 100-200Selenium (mg/kg) 0.5-1.3 0.5-1.3
Phosphorus (%) 0.4-0.8 0.5-0.8Sodium (%) 0.2-0.4 0.2-0.5Magnesium (%) - 0.04-0.1Average urinary pH - 6.2-6.4Key: VOHC = Veterinary Oral Health Council Seal of Acceptancefor plaque control.*All values are amounts in food on a dry matter basis unless otherwise stated.
Calcium chelators such as hexametaphosphate (HMP) aresequestrants that bind salivary calcium, making it unavailablefor incorporation into the plaque biofilm to form calculus. HMPis delivered as a coating on various treats, dental chews andfoods. The purported benefits of these compounds are that theyare released during chewing and remain for prolonged periodsof time in the oral cavity. It has been demonstrated that the addi-tion of HMP to the surface of baked biscuit treats, rawhidechews and dry foods results in reduced calculus accumulation.However, there is also evidence that shows no significant differ-ences in plaque or calculus accumulation in dogs fed dry foodsplus HMP-coated biscuits. Polyphosphates like HMP have noknown direct effect on oral microflora populations or plaqueaccumulation. An effective plaque control regimen should al-ways be the primary recommendation for prevention or post-therapeutic care of periodontal disease.
The Bibliography for Box 47-4 can be found atwww.markmorris.org.
Box 47-4. Hexametaphosphate andTartar Control.
The Veterinary Oral Health Council (VOHC) was established in1997 after 10 years of open meetings, which included repre-sentatives from the American Veterinary Dental College,Academy of Veterinary Dentistry, American Veterinary DentalSociety, American Veterinary Medical Association, AmericanAnimal Hospital Association, United States Food and Drug Ad-ministration, private practice and industry. The purpose of theVOHC is to provide an independent, objective and crediblemeans of recognizing veterinary dental products that effectivelycontrol accumulation of plaque and/or calculus (tartar). TheVOHC system is similar to the American Dental Association(ADA) Seal of Acceptance system and is recognized worldwide.
The VOHC does not conduct efficacy testing; the councilreviews results of tests performed in accordance with approvedprotocols set by the VOHC. The VOHC awards the Seal in twoclaim categories: 1) Helps control plaque and 2) Helps controltartar. It is important to recognize the difference between the twoclaims; plaque is the primary cause of periodontal disease andtartar control in the absence of plaque control is primarily cos-metic. If a product with the “helps control tartar” claim is recom-mended it is critical to recommend a proven plaque controlmethod. In addition to noting the type of Seal awarded, it isimportant to be aware of the study design and application (feed-ing) recommendations associated with meeting the claimrequirements. A product that is awarded the Seal based on aspecific application (daily) may not perform similarly whenapplied less frequently.
The first canine and feline dental products to receive theVOHC Seal of Acceptance were Hill’s Prescription Diet t/dCanine and t/d Feline, respectively. A complete list of productsthat have been awarded the VOHC Seal of Acceptance is avail-able at vohc.org.
Box 47-5. Veterinary Oral HealthCouncil: A System for RecognizingEffective Veterinary Dental Products.

little dental cleansing. As a tooth penetrates a kibble or treatthe initial contact causes the food to shatter and crumble withcontact only at the coronal tip of the tooth surface (Figure 47-6). To provide effective mechanical cleansing, a food shouldpromote chewing and maximize contact with the tooth sur-face (Figure 47-6).
Foods with enhanced textural characteristics promote oralhealth. Several maintenance pet foods are available that provideclinically significant oral cleansing compared with regular com-mercial dry or moist foods and/or snacks. Numerous studies
have demonstrated that foods possessing an appropriate combi-nation of shape, size and mechanical structure provide signifi-cant plaque, calculus and stain control in dogs and cats (Logan,1996, 1996a; Boyce, 1992; Jensen et al, 1995; Logan et al, 1995;Finney, 1996). A six-month study investigating the effects offood on plaque accumulation and gingival inflammation in 40adult mongrel dogs reported that dogs fed the test food had 39%less plaque accumulation and 36% less gingival inflammationthan dogs fed the control food (Figure 47-7).These studies useda clean-tooth model in which plaque, calculus and stain wereevaluated at a specified time following a dental prophylaxis.
One study reported that feeding a food with appropriatephysical characteristics to beagles with existing plaque, calculusand gingivitis resulted in a significant decrease in mean plaqueand calculus indices after two weeks and in the gingival indexafter six weeks (Figure 47-8). Beagles eating the control foodhad a significant increase in plaque and calculus accumulationand no change in gingival inflammation over the 16-week testperiod (Finney et al, 1996).
Fiber-containing foods have long been viewed as “nature’stoothbrush.” Investigators have theorized that fibrous foods: 1)exercise the gums, 2) promote gingival keratinization and 3)clean the teeth. Fiber in foods, especially as it relates to texture,has been shown to affect plaque and calculus accumulation andgingival health in dogs and cats (Watson, 1994; Boyce andLogan, 1994; Logan, 1996). Certain types of fiber combinedwith specific manufacturing processes can affect a food’s tex-ture. Fiber characteristics that maximize tooth contact time(e.g., orientation within the kibble matrix), combined with asize and shape that promote chewing, are critical to obtaining adental benefit. A typical dry food does not possess the mechan-ical characteristics for adequate dental cleansing. Simply en-larging the kibble or varying the shape of the product is like-wise inadequate. In the absence of effective plaque control
Small Animal Clinical Nutrition988
Early literature reported that the typical foods of wild canids andfelids had a plaque-retardant effect and that wild canids andfelids were not afflicted with the generalized form of periodontaldisease seen in domesticated pets. Pet food commercializationis often implicated as a contributing factor to the increasedprevalence and severity of periodontal disease in domestic dogsand cats (Box 47-3). The constituents of natural foods for wildcanids and felids probably depend on geographic location, envi-ronmental season and individual hunting capabilities. However,historically a natural food refers to small rodents/mammals thatwould typically fall prey to wolves, coyotes, etc. Colyer specifi-cally refers to “flesh that the animals must rend with their teeth.”Wild canids in particular probably eat fruits and vegetables andan array of tissues including blood, intestines plus contents,muscle, cartilage, bone marrow and bones.
Despite these assertions, there are no published data thatcompare controlled populations of domestic dogs or cats con-suming natural food sources with those consuming a commer-cial food. In addition, even if it were possible to make such com-parisons, confounding variables might include dramatic changesin food form (moist, semi-moist, dry and evolving pet ownerpreferences) through development of commercial pet foods,specific nutrient variation and selective breeding, which hasresulted in dramatic differences in body size and head types ofdogs and cats.
Reports exist about the oral condition of small populations ofdogs and cats consuming natural foods. One study involved 67English foxhounds, one to nine years of age that were routinelyfed raw carcasses consisting of the bony skeleton, muscle andassociated tissues. Oral examinations revealed that all dogs hadvarying signs of periodontal disease as well as a high prevalenceof tooth fractures. Another study examined 45 small feral catsfrom an Australian national park and reported conditions includ-ing calculus deposits, periodontal disease, fractured teeth, attri-tion and tooth resorption. Examination of gastrointestinal con-tents of these cats revealed the presence of natural foodsources including small mammals, birds, lizards and insects.These findings cast skepticism on the long-held view that a nat-ural food source prevents development of oral disease, particu-larly periodontal disease, in dogs and cats. Box 47-8 describesthe role of chew toys in periodontal health.
The Bibliography for Box 47-6 can be found at www.markmorris.org.
Box 47-6. Natural Food Sources andPeriodontal Disease.
Figure 47-5. Comparison of plaque, stain and calculus accumulationin dogs fed a specialty brand moist food (Moist A), a grocery brandmoist food (Moist B) and a grocery brand dry food. There is no signif-icant difference in substrate accumulation among dogs fed the threefoods. Moist foods do not always promote increased plaque and cal-culus formation in comparison to dry foods.

through other measures, or in cases demanding adjunctiveplaque control, mechanical attenuation of plaque and calculusaccumulation daily with a maintenance dental food is a reason-able alternative. Given the prevalence of periodontal disease indogs and cats, effective homecare products that improve ownercompliance can be a valuable addition to an oral health main-tenance regimen.
One way to assess whether the texture of a specific dog or catfood is effective in preventing accumulation of dental plaque (orcalculus) is whether or not the product’s label carries the VOHCSeal of Acceptance, specifically stating that the product is effec-tive in controlling plaque. Published Grade 1 or 2 evidence-based studies are also reliable indicators of product efficacy.
AntioxidantsOxidative stress may be important in the etiology of peri-odontal disease. In one study, dogs with severe periodontitishad gingival crevicular fluid and serum with lower total anti-
oxidant capacity than dogs with gingivitis or mild periodon-titis (Pavlica et al, 2004). The body synthesizes many antiox-idants but relies on food for others. Vitamins E and C andselenium are proposed as antioxidant key nutritional factorsfor foods for periodontal disease because: 1) they are biologi-cally important, 2) they act synergistically (e.g., vitamin C andselenium-containing glutathione peroxidase regenerate vita-min E after it has reacted with a free radical) and 3) much isknown about their safety.
VITAMIN E Vitamin E (α-tocopherol) is the main lipid-soluble antioxi-
dant in plasma, erythrocytes and tissues (NRC, 2006). It is oneof the most effective antioxidants for protecting cell membraneconstituent polyunsaturated fatty acids from oxidation. VitaminE inhibits lipid oxidation by scavenging lipid peroxyl radicalsfaster than these radicals can react with adjacent fatty acids ormembrane proteins (Gutteridge and Halliwell, 1994).
989Periodontal Disease
Figure 47-6. This illustration depicts the mechanical cleansing prop-erties of commercial dog and cat foods. The top illustration demon-strates what occurs when a dog or cat chews a typical dry food. Thekibble crumbles providing little to no mechanical cleansing. The bot-tom illustration demonstrates what happens when a dog or catchews a dental food. The kibble stays together, maintaining contactwith the tooth surface and providing mechanical cleansing.
Figure 47-7. The effects of commercial dog foods on plaque accu-mulation and gingival health in dogs. These graphs compare plaqueaccumulation and gingival inflammation in dogs fed two differentfoods for six months. Each group of dogs began the study with aplaque index of zero and clinically healthy gingivae. At all time points,the dogs consuming the test food (Prescription Diet t/d Canine) hadsignificantly lower scores for plaque accumulation and gingivalinflammation than the dogs consuming the control food (Purina DogChow).

Research indicates that a level of vitamin E higher than therequirement confers specific biologic benefits (Hayes et al,1969; Hall et al, 2003; Meydani et al, 1998; Jewell et al, 2002).Based on antioxidant biomarker studies in dogs and cats, forimproved antioxidant performance, foods for oral health shouldcontain at least 400 IU/kg dry matter (DM) (dog foods) and atleast 500 IU/kg DM (cat foods) ( Jewell et al, 2000).
VITAMIN CVitamin C (ascorbic acid), is the most powerful reducing
agent available to cells. Ascorbic acid: 1) regenerates oxidizedvitamin E, glutathione and flavonoids, 2) quenches free radi-cals intra- and extracellularly, 3) protects against free radical-mediated protein inactivation associated with oxidative burstsof neutrophils, 4) keeps transition metals in reduced form and5) may quench free radical intermediates of carcinogenmetabolism.
Although dogs and cats can synthesize enough vitamin C tofulfill minimum requirements (Naismith, 1958), in vitro stud-ies indicated that dogs and cats have from one-quarter to one-tenth the ability to synthesize vitamin C as other mammals(Chatterjee et al, 1975). Whether or not this translates to a re-duced ability in vivo is unknown. For improved antioxidantperformance, and in conjunction with recommended levels ofvitamin E, foods for adult dogs and cats should contain at least100 and 100 to 200 mg vitamin C/kg DM, respectively.
SELENIUMGlutathione-peroxidase is a selenium-containing antioxidant
enzyme that defends tissues against oxidative stress by catalyz-ing the reduction of H2O2 and organic hydroperoxides and byregenerating vitamin E. The minimum requirement for seleni-um in foods for dogs and cats is 0.13 mg/kg DM (Wedekindet al, 2003, 2003a). Animal studies and clinical intervention tri-als in people have shown selenium to be anticarcinogenic at lev-els much higher (five to 10 times) than the recommendedallowances for people or the minimal requirements for dogs andcats (Combs, 2001; Neve, 2002). Therefore, for increasedantioxidant benefits, the recommended range of selenium fordog and cat foods is 0.5 to 1.3 mg/kg DM.
Phosphorus, Sodium, Magnesium and Urinary pHPhosphorus and sodium are considered key nutritional factorsfor apparently healthy adult dogs and cats for purposes of ame-liorating or slowing the progression of subclinical kidney dis-ease and/or hypertension. The recommended allowances forphosphorus and sodium in foods for adult dogs are 0.4 to 0.8%and 0.2 to 0.4% DM, respectively. For foods for adult cats, therecommended allowances for phosphorus and sodium are 0.5to 0.8% and 0.2 to 0.5% DM, respectively. In addition, for adultcats, magnesium and urinary pH are also key nutritional fac-tors, based on their role in feline lower urinary tract disease.The recommended allowance for magnesium in foods for adultcats is 0.04 to 0.1% DM. Foods for adult cats should produce aurinary pH in the range of 6.2 to 6.4. For more information seeChapters 13 and 20.
Small Animal Clinical Nutrition990
Figure 47-8. The effects of commercial dog foods on existingplaque, calculus and gingivitis in dogs. Each group of dogs enteredthe study with similar amounts of plaque, calculus and gingivitis.Dogs were fed either a control food (Purina Dog Chow) or a test food(Prescription Diet t/d Canine). Plaque, calculus and gingivitis wereevaluated over a four-month period. Dogs eating the test fooddemonstrated a highly significant reduction in plaque, calculus andgingival inflammation whereas dogs eating the control food had asignificant increase in plaque, a highly significant increase in calculusand no significant change in gingivitis.

Other Nutritional FactorsCalciumFoods deficient in calcium and excessive in phosphorus maylead to secondary nutritional hyperparathyroidism and signifi-cant loss of alveolar bone (Bawden et al, 1995; Becks and Web-er, 1931). Experiments in dogs have demonstrated resorption ofalveolar bone following consumption of a food with a low ratioof calcium to phosphorus (Henrikson, 1968). Krook and col-leagues proposed that periodontal disease results from a nutri-tional deficiency of calcium, an excess of phosphorus or both(1972, 1972a). Svanberg and colleagues reported that nutri-tional secondary hyperparathyroidism occurred in a group ofbeagles fed a food deficient in calcium. The food did not haveany effect on the initiation or rate of progression of periodontaldisease when compared with findings in a control group fed anutritionally adequate food (1973). It is unlikely that dietarydeficiencies in calcium and phosphorus are primary causes ofperiodontal disease; however, they may contribute to the pro-gression of the disease process and exacerbate bone loss.Calcium deficiency occurs rarely in dogs and cats that consumecommercial pet foods that contain calcium levels that meetAssociation of American Feed Control Officials’ (AAFCO)allowances (2007). Improperly formulated homemade foodsare more likely to be deficient in calcium.
Vitamin Deficiencies Adequate vitamin content can be a problem in improperly for-mulated homemade foods. Vitamins that have been studied inrelation to periodontal disease include A, B, C, D and E.Vitamin A deficiencies have been reported to cause marginalgingivitis, gingival hypoplasia and resorption of alveolar bone(King, 1940; Reifen, 2002). Deficiencies of B-complex vitamins(including folic acid, niacin, pantothenic acid and riboflavin)have been associated with gingival inflammation, epithelial ne-crosis and resorption of alveolar bone (Becks et al, 1943).Vitamin C, besides functioning as an antioxidant (discussedabove), also plays a key role in collagen synthesis. Ascorbic aciddeficiencies reportedly affect periodontal tissues adversely inpeople, including gingival inflammation (Ismail, 1983; Leggottet al, 1986). Vitamin D helps regulate serum calcium concentra-tions. Vitamin D deficiencies affect calcium homeostasis andreportedly affect the gingivae, periodontal ligament and alveolarbone (Becks and Weber, 1931). Deficiencies of these vitaminsare highly unlikely to occur in dogs and cats fed commercialfoods that contain levels that meet AAFCO allowances.
Vitamin E is an antioxidant and in one study, dogs withmore severe periodontitis also had lower total antioxidantcapacity of their gingival crevicular fluid and serum than dogswith gingivitis or mild periodontitis (Pavlica et al, 2004).
FEEDING PLAN
How to Feed Dogs and Cats for Optimal OralHealthIf properly fed as puppies and kittens (Box 47-7), most dogsand cats enter adulthood with healthy mouths. In most cases,
periodontal disease can be prevented with appropriate plaquecontrol. The level of plaque control necessary to maintain oralhealth must be assessed for each individual patient. Frequentplaque removal (daily, if possible) is widely recommended.Brushing, when done correctly and conscientiously, is a veryeffective method for achieving the level of plaque control nec-essary to control gingivitis.
After oral disease is present, it should be treated with appro-priate professional therapy. However, aftercare, or continueddental hygiene provided by the pet owner, will determine theoverall success of professional therapy. A regimen of soft foodmay be recommended after invasive or advanced proceduresduring the initial healing phase. Chemical plaque controlshould be provided in these instances until mechanical plaquecontrol can be resumed. However, many pets can resume theirnormal food regimen immediately after receiving professionalcare, provided the client has been instructed in appropriateplaque control procedures (Box 47-1).
If the pet owner is able to provide effective plaque controlthrough toothbrushing, then an oral benefit from foods and/ortreats may be of less concern (Lindhe and Rylander, 1975;Tromp et al, 1986, 1986a). Realistically, however, compliancewith toothbrushing is a problem for many pet owners. In addi-tion, certain patients may require aggressive plaque controlcombined with frequent professional care to maintain optimaloral health. Thus, in many cases, a food/treat approach toplaque control is necessary. The feeding plan includes assessingand selecting the best food and feeding methods for the indi-vidual patient.
Assess and Select the FoodAfter the oral and general health status of the patient has beenassessed and the key nutritional factors and their target levelshave been determined, the adequacy of the food can be as-sessed. The steps to assessing foods include: 1) assuring thenutritional adequacy of the food by a credible regulatory agencysuch as AAFCO and 2) comparing the food’s key nutritionalfactors with the recommended levels. Because dental foods areused in place of regular maintenance foods, the key nutritional
991Periodontal Disease
Puppies and kittens are born edentulous. However, the nutritionthey receive from the bitch or queen can affect oral develop-ment. The bitch or queen should receive an appropriategrowth/lactation food during lactation to ensure adequate milkproduction and to meet ongoing needs. Deciduous teeth beginto erupt at about three weeks of age. Most puppies and kittenscan be given access to soft food at this age. Full deciduous den-tition should be present in puppies by 12 weeks of age and inkittens by six weeks of age. The permanent tooth bud willalready be formed, so it is essential to dental health that pup-pies and kittens receive appropriate nutrition during the earlyweeks of development. This is also the ideal time to train a petto accept oral hygiene.
Box 47-7. Feeding Puppies and Kittensfor Optimal Dentition.

factors include those for promoting long-term general healthby managing certain other important disease risk factors.
Besides providing the recommended levels of key nutritionalfactors, Tables 47-5 and 47-6 provide key nutritional factorprofiles for selected commercial foods marketed to provide adental benefit for dogs and cats, respectively. Special emphasisshould be given to the presence of the VOHC Seal of Ac-ceptance for plaque control. If the food in question cannot befound in this table, contact the manufacturer. Manufacturers’addresses, websites and toll-free customer service numbers arelisted on pet food labels. If the manufacturer cannot provide thenecessary information, consider switching to a food for whichthis information is available. Optimal nutrient balance is criti-cal to overall health and should not be overlooked when assess-ing whether a food or treat is appropriate for periodontalhealth. Thus, it is important that a dental food or treat provideoptimal nutritional balance for dogs and cats for their lifestage.Comparing a food’s key nutritional factor content with the rec-ommended levels is fundamental to food selection.
Another criterion for selecting a food that may becomeincreasingly important in the future is evidence-based clinical
nutrition. Practitioners should know how to determine risksand benefits of nutritional regimens and counsel pet ownersaccordingly. Currently, veterinary medical education and con-tinuing education are not always based on rigorous assessmentof evidence for or against particular management options. Still,studies have been published to establish the nutritional benefitsof certain pet foods. Chapter 2 describes evidence-based clini-cal nutrition in detail and applies its concepts to various veteri-nary therapeutic foods. Evidence Grade 1 (the highest level)and Grade 2 exist for foods that confer dental benefits for catsand dogs, respectively.a,b
Treats are often considered for their purported dental bene-fits, as well as a reward. From a strictly nutritional standpoint,small amounts of treats (less than 10% of the total food intake)will not importantly affect a pet’s overall daily nutrient intake.Excessive feeding of treats, however, can markedly affect afood’s cumulative nutritional profile. Therefore, it is importantto assess the impact of treats with respect to the dietary needsof individual dogs or cats.
The impact of treats on daily nutrient intake depends onthree factors: 1) the nutrient profile of the treat, 2) the number
Small Animal Clinical Nutrition992
Table 47-5. Key nutritional factor content of selected dry commercial dog foods marketed for dental health compared to recommended levels.*
VOHC Seal for plaque
control Vitamin E Vitamin C Selenium Phosphorus Sodium Factors (Yes/No) (IU/kg) (mg/kg) (mg/kg) (%) (%)Recommended levels Yes ≥400 ≥100 0.5-1.3 0.4-0.8 0.2-0.4Hill’s Prescription Diet t/d Canine Yes 652 79 0.50 0.40 0.22Hill’s Prescription Diet t/d Small Bites Canine Yes 652 79 0.50 0.40 0.22Hill’s Science Diet Adult Oral Care Yes 564 175 0.62 0.65 0.24Medi-Cal Dental Formula No na na na 0.90 0.40Purina Veterinary Diet DH Dental Health No 1,171 na na 1.25 0.57Purina Veterinary Diet DH Dental Health
Small Bites No 1,169 na na 1.24 0.61Royal Canin Veterinary Diet Dental DD 20 No 604 na 0.44 0.66 0.38Royal Canin Veterinary Diet Dental DS 23
Small Breed No 725 na 0.44 0.66 0.77Key: VOHC = Veterinary Oral Health Council Seal of Acceptance for plaque control, na = information not available from manufacturer.*All values are amounts in food on a dry matter basis unless otherwise stated.
Table 47-6. Key nutritional factor content of selected dry commercial cat foods marketed for dental health compared to recommended levels.*
VOHC Seal for plaque
control Vitamin E Vitamin C Selenium Phosphorus Sodium Magnesium Urinary Factors (Yes/No) (IU/kg) (mg/kg) (mg/kg) (%) (%) (%) pHRecommended levels Yes ≥500 100-200 0.5-1.3 0.5-0.8 0.2-0.5 0.04-0.1 6.2-6.4Hill’s Prescription Diet t/d Feline Yes 811 83 0.59 0.80 0.33 0.065 6.34Hill’s Science Diet Adult Oral Care Yes 670 171 0.55 0.75 0.37 0.058 6.30Medi-Cal Dental Formula No na na na 0.70 0.60 na naPurina Veterinary Diets DH
Dental Health Yes 722 na na 1.50 0.63 0.10 naRoyal Canin Veterinary Diet
Dental DD 27 No 710 na 0.34 0.81 0.65 0.097 naKey: VOHC = Veterinary Oral Health Council Seal of Acceptance for plaque control, na = information not available from manufacturer. *All values are amounts in food on a dry matter basis unless otherwise stated.

of treats provided daily and 3) the nutrient composition of thepatient’s regular food. Because meeting nutrient requirementsis not the primary reason pet owners provide treats, commercialtreats often are not complete and balanced. (See package la-bels.) If treats are fed, recommend that they be commercialtreats that match the key nutritional factor profile recommend-ed for the patient’s lifestage. Generally, feeding excessiveamounts (>10% of the total food intake on a volume or caloriebasis) of any treat is not recommended. Ideally, the nutritionalcomposition of treats and food should be combined and as-sessed as the entire dietary regimen. From a dental benefitstandpoint, the efficacy of treats and non-food items such asrawhide chews should be evaluated just like dental foods. Thesafety of such products should also be considered.
Plain baked biscuits, although long thought of as “dental”treats, provide little additional plaque and calculus reductionwhen compared with feeding dry dog food alone (Figure 47-9).Additionally, manufacturers of some feline treats make a calcu-lus control claim;c,d however, two studies have failed to dem-onstrate an effect on plaque and calculus accumulation com-pared with feeding dry or moist foods alone (Logan, 1996a;Logan et al, 1997). Figure 47-10 describes the effect of dentaltreats on plaque and calculus accumulation in cats fed dry andmoist foods with and without supplemental treats.
The addition of hexametaphosphate (HMP) (Box 47-4) to
the surface of baked biscuitse significantly reduced calculusaccumulation in beagles over a four-week period comparedwith a regimen of plain baked biscuits and dry food alone(Stookey et al, 1995, 1996). One three-week study, however,demonstrated no significant differences in plaque and calculusaccumulation in dogs fed dry food, dry food plus baked biscuitsor dry food plus HMP-coated biscuits.f A treat made of riceand whey and formed into a bone shapeg to promote chewingactivity has been reported to reduce plaque and calculus accu-mulation in small dogs over a four-week period (Gorrel andRawlings, 1996). The disadvantages of these products mayinclude pet acceptance, potential for gastrointestinal side ef-fects, cost of the recommended feeding dosage and nutritionalinfluences such as caloric excess and nutrient imbalances(Crane, 1990).
993Periodontal Disease
Figure 47-9. The effects of four different food regimens on plaqueand calculus accumulation in dogs. Forty mongrel dogs were fed oneof four food regimens: 1) Control (Purina Dog Chow), 2) Control plustwo hexametaphosphate-coated biscuits/day (Tartar Check), 3)Control plus seven medium or four large (based on manufacturer’sfeeding directions) plain biscuits/day (Milk Bone) or 4) PrescriptionDiet t/d Canine. There was no significant difference in plaque or cal-culus accumulation in dogs fed Purina Dog Chow or Purina DogChow plus Milk Bone or Tartar Check biscuits. Dogs fed PrescriptionDiet t/d Canine had significantly less accumulation of plaque and cal-culus than dogs fed Purina Dog Chow or Purina Dog Chow plus MilkBone or Tartar Check biscuits.
Figure 47-10. The effects of “dental” treats in cats fed commercialdry or moist foods. The top graph illustrates plaque accumulation incats fed a moist or dry cat food or the same food plus dental treats.The bottom graph illustrates calculus accumulation in cats fed moistcat food or the same food plus dental treats. There was no significantdifference in plaque or calculus accumulation with the addition ofdental treats to either a dry or a moist cat food.

Besides commercial treats, rawhide strips have been reportedto control calculus accumulation, provided the dog activelychews the strips daily (Lage et al, 1990). Two rawhide chewseach day are typically recommended.h Compacted rawhidetreats in the shape of balls and bones can cause tooth fracturesif chewed aggressively or if used as “catch” toys. Flat rawhidechews coated with an enzymatic systemi are also available com-mercially; however, there are no published data demonstratingthat these products are any more effective than plain rawhidestrips. Although not foods, chew toys are a category of chew-able products that claim an oral benefit for dogs. Box 47-8 pro-vides a brief discussion of the potential benefits vs. risks of theseproducts.
Assess and Select the Feeding MethodThe method of feeding is often not altered in the nutritionalmanagement of periodontal disease. If a new food is fed, theamount to feed can be determined from the amount of the pre-vious food being fed (calorie basis), particularly if the patient isin optimal body condition (body condition score of 2.5/5 to3.5/5). The food dosage may need to be changed if the caloricdensity of the new food differs from that of the previous food.Otherwise product labels or other supporting materials can beused as starting points. The food dosage and feeding methodshould be altered if the patient’s body weight and condition aresuboptimal. Initially, the patient should be weighed every twoweeks or so to ensure the food dosage is correct. Although mosthealthy dogs and cats do not experience digestive upsets withtypical food changes, a gradual transition to a new food maybenefit some patients. Progressively exchanging the new foodfor the usual food over four to seven days will minimize unto-
ward effects and food refusal. Chapter 1 contains more in depthinformation about feeding methods and food transitions.
Good compliance is necessary for effective clinical nutrition.Enabling compliance includes limiting access to other foodsand knowing who feeds the pet. Communicating the need forand the methods of effective plaque control may improve oralhygiene compliance.
REASSESSMENT
Monitoring depends on the: 1) degree of oral pathology, 2)level of periodontal therapy and 3) ability of the owner to pro-vide routine oral hygiene. An annual oral examination and pro-fessional prophylaxis should be adequate for adult dogs and catswith good oral health and normal occlusion. As the severity oforal disease increases, the degree of periodontal therapy re-quired to treat the condition will increase as well. An increasedlevel of oral hygiene will be necessary to prevent disease pro-gression toward advanced stages of periodontal disease (e.g.,periodontitis, etc.).
Initially, patients should be rechecked weekly to monitorhealing and oral hygiene. If both are satisfactory, the timebetween recalls can increase to three-month intervals. If thepatient has severe pathology affecting plaque retention or if theowner is unable to provide effective plaque control, the timebetween periodontal therapies will need to be adjusted to main-tain oral health. These recommendations are initial guidelines.Veterinarians must decide appropriate recall for each case, de-pending on the degree of oral pathology, periodontal therapyand owner compliance.
Small Animal Clinical Nutrition994
Chew toys are a category of products that claim an oral benefit fordogs (Figure 1). Many varieties are available with claims rangingfrom “flosses teeth” to “reduces harmful plaque;” however, fewdata in the literature substantiate these claims. One report claimedless calculus accumulation in 14 of 20 client-owned dogs whendogs were allowed access to a urethane chewing devicea for onemonth. Anecdotal reports of oral trauma (e.g., gingival lacerationsand tooth fractures) resulting from aggressive chewing of somedental toys can also be found in the veterinary dental literature.
ENDNOTEa. Nylabone. Nylabone Products, Neptune, NJ, USA.
The Bibliography for Box 47-8 can be found at www.markmorris.org.
Box 47-8. Chew Toys and Periodontal Disease in Dogs and Cats.
Figure 1. Manufacturers of many toys and devices make dentalclaims. Some of these claims include, “removes/reduces tartar,massages gums and flosses teeth.” In most cases, no scientificstudies substantiate these claims and pet owners can easily bemisled. There is clinical evidence, however, that suggests gumlacerations and fractured teeth may result from inappropriateuse of toys and devices, including failure to match toy size topet size, use of hard toys, particularly with puppies and toy usewith pets that chew aggressively.

CASE 47-1
Oral Foreign Body in a Doberman PinscherRobert B. Wiggs, DVM, Dipl. AVDCCoit Road Animal HospitalDallas, Texas, USA
Patient AssessmentA five-year-old, 30-kg, male Doberman pinscher was presented for removal of a large beef knucklebone that was lodged in itsmouth. The dog was excited, salivating profusely and difficult to handle. The bone was lodged caudal to the canine teeth betweenthe dental arcades and was holding the dog’s mouth open to the point of causing strain upon the jaws. Attempts to remove the bonewhile the patient was awake were unsuccessful. The dog’s excited condition and the obstructing bone made a complete physical andoral examination impossible before sedation. After the dog was sedated, it was possible to gradually extricate the bone without fur-ther damaging the teeth or oral tissues (Figures 1A and 1B). The dog was intubated and anesthetized to allow a comprehensiveoral examination.
ACKNOWLEDGMENTS
The authors and editors acknowledge the contributions of Drs.Karl Zetner and John J. Hefferren in the previous edition ofSmall Animal Clinical Nutrition.
ENDNOTES
a. Prescription Diet t/d Feline. Hill’s Pet Nutrition, Inc.,Topeka, KS, USA.
b. Prescription Diet t/d Canine. Hill’s Pet Nutrition, Inc.,Topeka, KS, USA.
c. Pounce Tartar and Plaque Control. Del Monte Pet Products,Pittsburgh, PA, USA.
d. Whisker Lickin’s Tartar Control Treats. Nestle Purina PetCare Products, St. Louis, MO, USA.
e. Tartar Check. Del Monte Pet Products, Pittsburgh, PA,USA.
f. Logan EI. Unpublished data. December 1996.g. Pedigree Dentabone. Kal Kan Foods, Vernon, CA, USA.h. Purina Chew-eez. Nestle Purina Pet Care Products, St.
Louis, MO, USA.i. C.E.T. Chews. Virbac Animal Health, Ft. Worth, TX, USA.
REFERENCES
The references for Chapter 47 can be found at www.markmorris.org.
995Periodontal Disease
Figure 1A. A large bone lodged in the oral cavity of a Dobermanpinscher.
Figure 1B. The same patient after the bone was removed. Note thesize of the bone in relation to the patient’s head and mouth.

The jaw had a full range of movement and no crepitation wasdetected over the temporomandibular joints. A laceration about7 mm long and of moderate depth was found ventrally on theright side of the tongue in the proximity of the distal premolars.This laceration probably occurred as a result of the tongue press-ing against the lower premolars.
The right carnassial teeth (maxillary fourth premolar andmandibular first molar) had Class VI/VI, cusp-type slab frac-tures. A slab of tooth was lost from the buccal side of the maxil-lary fourth premolar (Figure 2) and from the lingual side of themandibular first molar. This type of injury commonly affectsthese tooth surfaces. Both fractures involved the pulp chamber;the exposed sites were dark and open. The pulp of these teethwas nonvital. Calculus accumulation and gingivitis were presenton both arcades.
Assess the Food and Feeding MethodThe owner had been feeding the dog various dry commercial dog foods sometimes mixed with water or moist foods. When thedog was examined and vaccinated by the referring veterinarian approximately seven months earlier, the owner had been informedthat the teeth were in generally good shape but there was slight calculus accumulation. The veterinarian had recommended a den-tal prophylaxis, which the owner declined. Shortly thereafter, the owner had begun feeding bones to the dog at the suggestion of afriend who said that bones could clean the dog’s teeth. All bones had been cooked before they were given to the dog. This was thefirst time the dog had received a large knucklebone.
Questions1. What are the treatment options for the two fractured teeth?2. What safety concerns are associated with feeding bones to dogs?3. What recommendations should be made concerning the dog’s food?4. When should a dog’s teeth be cleaned?
Answers and Discussion1. There are typically six options for treating fractured teeth: 1) leave them as they are, 2) smooth the fractured edges and seal the
dentinal tubules, 3) place a restoration, 4) perform a pulp capping, 5) perform a root canal or 6) extraction. Small enamel chipsof vital teeth may be left as is; however, the jagged edges of these teeth should be smoothed. In this case, the pulp was exposed;therefore, leaving the teeth untreated could lead to abscessation or more likely to a chronic active granuloma at the root apex ortip. Chronic shedding of bacteria into the bloodstream may gradually damage organs such as the heart, kidneys and liver. It wouldbe medically unsound to leave these teeth untreated. The most common repair technique for fractures of vital teeth that extendinto the dentin is to smooth the fracture edges and seal the dentinal tubules with a dentinal bonding agent and possibly apply arestorative agent. This technique is also used in association with a pulp capping or root canal procedure. For this patient, thistreatment would be appropriate only if done in conjunction with an endodontic procedure. Restoratives, such as a metal, com-posite, glass, porcelain or porcelain fused to a metal crown or inlay, are also used to repair fractures of vital teeth that extend intothe dentin. These are also used in association with a pulp capping or endodontic procedure. Treatment with a restorative wouldbe appropriate for this dog only in conjunction with an endodontic procedure. Pulp capping procedures are used for repair offractured teeth with pulp exposure in which the pulp is still vital or alive. Successful pulp capping procedures inconsistently main-tain the vitality of the tooth. At least 20% of the procedures fail even when performed under optimal circumstances. The sever-ity of the trauma, amount of contamination, elapsed exposure time and degree of pulp exposure all play a crucial role in the suc-cess of pulp capping procedures. In this case, the teeth have Class VI/VI fractures and the pulp is nonvital, so a pulp capping pro-cedure would be inappropriate.
Root canal or complete endodontic procedures are used when fractured teeth have pulp cavity exposure and the pulp is eitherin a state of irreversible pulpitis or already nonvital. A root canal procedure is an option for this patient. The determining factorsfor selecting this treatment include the extent of damage to the tooth crown, the state of the external root structure, the condi-tion of the pulp cavity, the status of the periodontal tissues and the ability of the owner to eliminate or nullify causative agents.If these conditions are all favorable, this procedure plus some form of restoration would be the treatment of choice to maintainthe function of the carnassial teeth.
The above procedures require advanced training and dental equipment. Extraction (exodontia) is a treatment option for dam-aged teeth, teeth affected by severe periodontal disease, highly mobile teeth that cannot be stabilized and teeth with root frac-
Small Animal Clinical Nutrition996
Figure 2. Slab fracture (dark arrows) of the maxillary fourth premo-lar with an exposed pulp chamber (white arrow).

tures. The tooth type and location, number of roots, status of surrounding periodontal tissues and supporting bone and indica-tions of root abnormalities (i.e., dilacerated, ankylosed, etc.) determine the type of extraction process. Extraction is a reasonablealternative for veterinarians who lack the training or equipment to perform the treatments discussed above.
2. Some pet owners believe that feeding cooked bones to domesticated pets helps control calculus accumulation. However, there areno reliable, published studies showing dental benefits derived from bone chewing. This practice has gradually fallen into disfavoramong many veterinarians because bone consumption often results in health problems such as fractured teeth, bone lodgments,constipation, intestinal or rectal blockages and esophageal, gastric and intestinal perforations.
Recently, some veterinarians have again begun recommending the feeding of bones. However, the recommendation is to feedraw bones with meat attached, sometimes designated “raw and meaty bones.” Current theory proposes that uncooked bones arenot as hard as cooked bones and do not fracture teeth or cause other problems associated with cooked bones. However, anecdot-al reports suggest the health concerns presented with cooked bones also occur commonly with raw, meaty bones. Feeding raw,whole chicken or chicken parts has been suggested as providing dental benefits without the risk of dental fractures because chick-en bones are smaller. However, feeding raw meats, particularly chicken, raises food safety concerns (Chapter 11). The safety andefficacy of feeding bones, regardless of type, remain undetermined. Veterinarians should be cautious about recommending bonesfor dental benefits.
3. There is little reliable scientific information about the dental benefits of most commercial dog and cat foods or about the dentalbenefits of one food compared with those of another. In general, dry foods have been accepted as causing less calculus and plaqueaccumulation than moist foods, even though controversies and inconsistencies exist in the literature. A commercial canine vet-erinary therapeutic food, Prescription Diet t/d Caninea has valid data documenting effective dietary cleansing. Research hasdemonstrated this food influences the control or reduction of plaque, calculus, stain and gingivitis. Prescription Diet t/d Caninewould be an appropriate food for this dog.
4. Teeth cleaning and professional dental prophylaxis are not always synonymous. The term prophylaxis means to prevent disease,whereas teeth cleaning means to prevent or treat disease. Teeth should be cleaned when calculus accumulations occur, or whenstomatitis and periodontal disease develop. The professional dental prophylaxis, if taken literally, must be performed at intervalsneeded to prevent stomatitis or periodontal disease from developing.There are no definitive time intervals for the veterinary pro-fessional dental prophylaxis. The veterinarian must combine information about the pet’s health status, oral and tooth pathology,degree of successful homecare, foods offered to the pet and the pet’s chewing behavior to customize a professional dental pro-phylaxis program. A reasonable starting point is every six to 12 months for large-breed dogs.
Progress NotesThe tongue laceration was sutured and a comprehensive oral examination was completed at the initial visit. The clinical findingsand treatment options were discussed with the owner. Three days after the original incident, a root canal procedure was performedon the dog’s two fractured carnassial teeth and the tooth crowns were prepared for restoration. A dental prophylaxis was also per-formed at that time. About two weeks later the crowns were cemented, seated and adjusted. Initial owner instructions includedrestricting the dog’s access to all bones and excessively hard chew toys. After endodontic treatment and crown preparation, the dogwas fed a soft food to avoid injury to the prepared teeth. Following crown placement the dog was fed Prescription Diet t/d Canine.
The tongue had healed well when examined at the time of crown placement. When the dog was reexamined six months afterthe incident, no calculus accumulation was present and the gingivitis had resolved. The dog’s general condition was very good. Itscurrent weight was 31 kg with a body condition score of 3/5.
Endnotea. Hill’s Pet Nutrition, Inc., Topeka, KS, USA.
BibliographyEmily P, Penman S. Endodontics. In: Handbook of Small Animal Dentistry. New York, NY: Pergamon Press, 1990: 65-80.Emily P. Problems associated with diagnosis and treatment of endodontic disease. Problems in Veterinary Medicine: Dentistry1990; 2: 152-182.Gorrell C, Robinson J. Endodontics in small carnivores. In: Crossley DA, Penman S, eds. Manual of Small Animal Dentistry, 2nded. London, UK: British Small Animal Veterinary Association, 1995; 168-192.Holmstrom SE, Frost P, Gammon RL. Veterinary Dentistry Techniques for the Small Animal Practitioner. Philadelphia, PA: WBSaunders Co, 1992; 207-266.Shipp AD, Farhenkrug P. Practitioners’ Guide to Veterinary Dentistry. Beverly Hill’s, CA: Dr. Shipp’s Lab, 1992; 77-94.Wiggs RB, Lobprise HB, eds. Basic endodontic therapy. In: Veterinary Dentistry: Principles and Practice. Philadelphia, PA:Lippincott-Raven, 1997; 280-324.
997Periodontal Disease

CASE 47-2
Inappetence in a CatRobert B. Wiggs, DVM, Dipl. AVDCCoit Road Animal HospitalDallas, Texas, USA
Patient AssessmentA three-year-old, 3.4-kg, neutered female domestic shorthair cat (body condition score 3/5) was referred for inappetence, saliva-tion, periodic gagging and resistance to oral examination. The condition began suddenly two days earlier. The cat’s abdomen waspainful when palpated. Cervical lymph nodes and the thyroid glands were normal, although the patient resented palpation of thelower neck region. Eyes and ears were normal.
The cat’s resistance to the oral examination limited the initial assessment. Moderate calculus accumulation and gingivitis werenoted, however. A raised, non-inflamed mass of gingival tissue was present where the crown of the lower left third premolar shouldhave been located. Due to the cat’s agitation, the teeth and their associated sulci could not be examined with a dental explorer/probe.The lips, alveolar mucosa, dorsal surface of the tongue and hard and soft palate appeared normal. Examination of the ventral tonguebase revealed a string foreign body.
Following sedation, the string was found to extend across the base and caudally around the lateral sides of the tongue into thepharyngeal region. The two leaders of the string extended into the esophagus. The tongue was lifted and the string grasped withBrown-Adson thumb forceps and gently pulled rostrally out of the mouth with no resistance. The string appeared to be a cotton-like material, 32 cm long. Endoscopic and radiographic examination of the esophagus and stomach were recommended.
The cat was intubated and anesthetized with isoflurane. Radiography showed the left mandibular gingival mass covered the rootsof the lower third molar and that the majority of the crown was absent. The mass appeared to be a Stage V feline tooth resorption(Table 1). Other findings included moderate calculus accumulation and mild gingivitis.
A dental prophylaxis was performed and the cat was given antibiotics for 10 days.
Assess the Food and Feeding MethodThe cat was fed a variety of moist foods purchased from grocery outlets.
Questions1. What are the safety concerns of string-type chew toys?2. What should be done concerning the gingival mass?3. What recommendations should be made concerning the cat’s food?
Answers and Discussion1. The foreign body was similar to material from one of the cat’s toys. When purchased, the toy was a ball made from loops of a
cotton-like string, which purportedly would help clean and floss the teeth when the cat chewed on the toy. The toy came with apackage of coarsely ground dried catnip with instructions to sprinkle the catnip on the toy to entice the cat to play with and chewon it. The owners said that it was one of the cat’s favorite toys, especially when the catnip was applied. String, thread and piecesof fabric commonly cause problems when ingested by cats. Apparently, the type, diameter and length of fiber and the propor-tional length of fiber to cat size all play an important role in whether these fibers cause problems or pass through the gastroin-testinal tract. No studies concerning these factors have been published. Short lengths of a multi-stranded, absorbable materialwould seem more appropriate, but more research is needed to determine safety requirements. Some string and rope chew toysare promoted for their “flossing effect.” However, no research documents these claims. Additionally, some packages instruct theowner to use the toys in a tug-of-war with the pet to attain the flossing action. Strings tangled around teeth can avulse or frac-ture teeth. Therefore, these types of chew toys for dogs and cats should be recommended with extreme care, particularly forpatients with moderate to advanced periodontal disease and mobile teeth. Clients who use string and rope-type chew toys shouldbe encouraged to supervise their use and dispose of them at the first sign of unraveling or fraying.
2. The gingival mass was a Stage V feline tooth resorption (Table 1). There are three options for treating these lesions: 1) restora-tion of the tooth, 2) extraction of the tooth and 3) no treatment (leave the lesion as it is). Restorations, usually with glass ionomers,are generally used in repair of Stage I and, to a limited degree, Stage II lesions. Success of restoration for Stage II lesions is gen-erally poor, but is an option the client should be given. Stage II to IV lesions can be extremely painful and should be treated.Careful extraction of tooth roots should be considered in Stage V lesions if inflammation is present in the gingival area overly-ing the retained roots. If inflammation is not present and the lesion is not painful or sensitive to the patient, the roots may be leftin place. Often the roots will completely resorb with no further problems. In this case, there was no inflammation associated with
Small Animal Clinical Nutrition998

the mass and no treatment was performed.3. Commercial cat foods are available that provide effective dietary cleansing through mechanical reduction of plaque and calculus
accumulation (Prescription Diet t/d Felinea , Friskies Dental Dietb and Purina Veterinary Diets DH Dental Health Brand FelineFormula.c
Progress NotesFiberoptic and radiographic examination of the esophagus and stomach revealed no abnormalities. The cat’s food was changed toPrescription Diet t/d Feline. The cat was reexamined three weeks after the initial presentation. The gingival mass appearedunchanged to slightly smaller with no inflammation. The cat was eating well and no calculus accumulation was present.
Endnotesa. Hill’s Pet Nutrition, Inc., Topeka, KS, USA.b. Friskies Pet Care Co., Glendale, CA, USA.c. Nestlé Purina PetCare Co., St Louis, MO, USA.
BibliographyHarvey CE, Emily PP. Atlas of oral pathology of the dog and cat. In: Small Animal Dentistry. St. Louis, MO: Mosby-Year Book,Inc, 1993; 48-56.Wiggs RB, Lobprise HB, eds. Domestic feline oral and dental disease. In: Veterinary Dentistry: Principles and Practice.Philadelphia, PA: Lippincott-Raven, 1997; 482-517.Wiggs RB, Lobprise HB. Dental disease. In: Norsworthy GD, ed. Feline Practice. Philadelphia, PA: JB Lippincott Co, 1993; 290-304.
CASE 47-3
Periodontal Disease in a Geriatric Miniature SchnauzerRobert B. Wiggs, DVM, Dipl. AVDCCoit Road Animal HospitalDallas, Texas, USA
Patient AssessmentA 12-year-old, 10-kg male miniature schnauzer was examined for severe halitosis and reluctance to eat dry food. Physical exami-nation revealed a grade 1/6 heart murmur and a body condition score of 3/5. Abnormal oral findings included moderate accumu-lations of plaque and calculus on both dental arcades, gingivitis, furcation exposure and attachment loss, most prominent aroundthe mandibular caudal premolar and molar teeth.
After the initial oral examination, the dog was given enrofloxacin (Baytrila) to control infection while further evaluations wereperformed. Results of a complete blood count were normal. Results of a serum biochemistry profile were normal except for mildazotemia (BUN = 42 mg/dl, normal = 10 to 25). A cardiac evaluation indicated mild valvular endocardiosis.
Assess the Food and Feeding MethodThe owner had been feeding various commercial dry and moist grocery brand dog foods. Approximately six months earlier the dogbecame reluctant to eat dry foods and was currently eating only moist foods.
999Periodontal Disease
Table 1. Staging feline dental resorptive lesions.
Stage I Lesion extends into cementum or enamel onlyStage II Lesion extends into the dentinStage III Lesion extends into the pulp cavityStage IV Extensive structural damage to tooth, root or bothStage V Root retention with complete loss of crown

Questions1. At what age should periodontal therapy be discontinued due to anesthetic risks?2. When are antibiotics appropriate in periodontal therapy?3. What medications may have adverse oral effects, particularly in geriatric dogs?4. Is maintenance of alveolar bone under the tooth (alveolar ridge) a concern when extracting permanent teeth?5. Outline an appropriate feeding plan for this geriatric patient.
Answers and Discussion1. Many owners and veterinarians are reluctant to anesthetize geriatric patients for periodontal procedures. There is no specific age,
however, when a patient cannot be anesthetized. An appropriate preanesthetic assessment should be made in all cases to identi-fy potential risks and define an appropriate anesthetic regimen. Placing an intravenous catheter and administering fluids duringperiodontal procedures reduces the risk of anesthetic complications. Periodontal disease is associated with bacterial infection.Thepotential for systemic disease due to chronic showering of the bloodstream with oral bacteria may pose a greater risk to the patientthan the anesthesia required for appropriate periodontal therapy.
2. Antibiotics may be used before, during or after dental procedures. Each period has specific justification. Antibiotics used beforedental procedures help control the existing periodontal infection, thereby decreasing inflammation, which allows for more accu-rate clinical assessment and helps when making therapeutic choices. Antibiotics used during dental procedures are generallyadministered to protect the body from infection resulting from bacteremia. Healthy immunocompetent patients clear this bac-teremia within 20 minutes. However, patients with organ pathology or a compromised immune system may be predisposed tosequential infection. Antibiotics given after dental procedures are generally prescribed to prevent oral reinfection during the heal-ing stages.
3. Many medications can affect oral physiology, particularly salivary flow. Saliva is rich in proteins, glycoproteins, electrolytes andlipids and provides a protective barrier to oral tissues. Reduced salivary flow is associated with an increased prevalence of caries,periodontal disease and oral irritation in people. Patients receiving medications that alter the oral environment may need addi-tional professional or homecare to maintain oral health. Examples of such drugs include narcotic analgesics, anticonvulsants, anti-histamines, antiarrhythmics, antineoplastics, antiemetics, diuretics and tranquilizers.
4. Alveolar ridge maintenance is a concern, particularly if the mandibular incisor, canine or carnassial teeth are extracted. Atrophyof the alveolar ridge and mandibular weakening are common following extraction of these teeth, and may result in future patho-logic or iatrogenic fractures. Packing extraction sites with osseopromotive material may reduce and in some cases prevent alveo-lar ridge atrophy.
5. Because aging affects all body systems, there is a high likelihood of multiple problems in older pets. A thorough systems review,which should include a complete history, physical examination and extended laboratory database, is important in older pets. Thisreview enables the veterinarian to define problems accurately, prioritize the problems and establish appropriate diagnostic, ther-apeutic and feeding plans. Chronic valvular heart disease (endocardiosis) and renal failure are common causes of morbidity andmortality in older dogs. Because these conditions are so common, geriatric dogs may benefit from a food that avoids excess lev-els of phosphorus, protein, sodium and chloride (Chapters 36 and 37). Other nutrient levels and the feeding method may needto be adjusted based on body condition of the patient and results of the comprehensive systems review.
This dog has clinical and laboratory evidence of dental disease, chronic valvular heart disease and renal disease. Accordingly, itmay benefit from a food that avoids excess levels of phosphorus, protein, sodium and chloride. In addition, oral care at homeshould be initiated to prevent accumulation of dental substrates and further periodontal disease. A food or dental treat thatenhances mechanical cleansing or teeth would be appropriate.
Prescription Diet t/d Canineb is a dry veterinary therapeutic food formulated to reduce accumulation of plaque and calculusand reduce gingivitis. This food is most effective when fed as the sole maintenance food for adult dogs. However, some pets withdental disease should receive food(s) with different nutrient profiles because of concurrent disease.
Progress NotesThe dog was given a vasodilator (isosorbide dinitrate) and a moist veterinary therapeutic food that avoids excess phosphorus, pro-tein, sodium and chloride (Prescription Diet k/d Canineb).
Therapeutic options for the oral problems were discussed with the owner and the decision was made to proceed with periodon-tal therapy. The dog was anesthetized with isoflurane (administered via mask and intubation), and supragingival scaling followedby root planing and subgingival curettage was performed. Severe periodontal disease was present around the left mandibular fourthpremolar and first molar teeth. Advanced bone loss was noted around the distal roots (Figure 1); a mobility index of 3/3 (severemobility) was present. Both teeth were extracted by crown sectioning and elevation. The alveolar sockets were curetted and bonyspicules were smoothed. An osseopromotive bioactive material (Bioglassc) was placed into the sockets to aid in alveolar ridge main-tenance.The extraction sites were closed with sutures and the remaining teeth were polished. Oral clindamycin (Antirobed), an oralascorbic acid/zinc gluconate rinse (Maxiguarde) and the moist veterinary therapeutic food (Prescription Diet k/d Canine) were pre-
Small Animal Clinical Nutrition1000

scribed for two weeks. After two weeks, the dog was reexamined.The extraction sites were healing well and the owner comment-ed that the dog was more active than it had been for manymonths. The dog was fed the dry form of the same renal food(Prescription Diet k/d Canine) and the owner was instructed toprovide daily oral care through toothbrushing and feeding fourkibbles of Prescription Diet t/d Canine/day.The combined foodswere calculated to deliver approximately 500 kcal/day (2.1MJ/day).
Endnotesa. Bayer Animal Health, Shawnee, KS, USA.b. Hill’s Pet Nutrition, Inc., Topeka, KS, USA.c. Nutramax Laboratories, Inc., Baltimore, MD, USA.d. Upjohn Veterinary Products, Kalamazoo, MI, USA.e. Addison Laboratories, Fayette, MO, USA.
BibliographyEdgar WM, O’Mullane DM, eds. Factors influencing salivary flow rate and composition. In: Saliva and Dental Health. BritishDental Association, 1990.Maretta SM. Oropharynx. In: Birchard SJ, Sherding RG, eds. Manual of Small Animal Practice. Philadelphia, PA: WB SaundersCo, 1994; 607-629.Wiggs RB, Lobprise HB, eds. Periodontology. In: Veterinary Dentistry: Principles and Practice. Philadelphia, PA: Lippincott-Raven, 1997; 186-231.
1001Periodontal Disease
Figure 1. Radiographic evaluation indicating severe alveolar boneloss around the distal roots of the mandibular fourth premolar andfirst molar.






























