Embed Size (px)
Citation preview

Eliminating Racial Disparities in Birth Outcomes Eliminating Racial Disparities in Birth Outcomes
Conference on Ending Family HomelessnessConference on Ending Family HomelessnessWorkshop: Workshop: Healthcare Matters: Providing Health Services to Healthcare Matters: Providing Health Services to
Diverse PopulationsDiverse Populations
February 7, 2008February 7, 2008
Susan Barkan, Public Health Seattle & King CountySusan Barkan, Public Health Seattle & King County
Melanie Whitfield, People of Color Against AIDS NetworkMelanie Whitfield, People of Color Against AIDS Network Maria Carlos, Public Health Seattle & King CountyMaria Carlos, Public Health Seattle & King County

AcknowledgementsAcknowledgementsSusan BarkanSusan Barkan
Kathy Carson Kathy Carson
Maria CarlosMaria Carlos
Eva Wong Eva Wong Doctoral Student, Department of Epidemiology, Doctoral Student, Department of Epidemiology, University of WashingtonUniversity of Washington
Alice ParkAlice Park
Mei Castor Mei Castor Urban Indian Health InstituteUrban Indian Health Institute
Shira RutmanShira Rutman
Jim La RocheJim La Roche
Leslie RandallLeslie Randall Northwest Portland Area Indian Health BoardNorthwest Portland Area Indian Health Board
Leah Henry Leah Henry Native American Women’s Dialog on Infant Native American Women’s Dialog on Infant Tanner Tanner Mortality (NAWDIM)Mortality (NAWDIM)
Jim GaudinoJim Gaudino Oregon State Department of HealthOregon State Department of Health
Parent Child Health, Public Health-Seattle & King Parent Child Health, Public Health-Seattle & King CountyCounty

0
2
4
6
8
10
12
81-8
3
82-8
4
83-8
5
84-8
6
85-8
7
86-8
8
87-8
9
88-9
0
89-9
1
90-9
2
91-9
3
92-9
4
93-9
5
94-9
6
95-9
7
96-9
8
97-9
9
98-0
0
99-0
1
00-0
2
01-0
3
02-0
4
Rat
e p
er 1
,000
Liv
e B
irth
s United States
Seattle
Washington State
King County
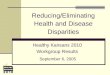
2004 Infant Mortality Rates:
United States (2003): 6.9 Washington State: 5.5 King County: 4.4 Seattle: 5.4 King County outside Seattle: 4.1
King County outside of Seattle
Infant Mortality RatesInfant Mortality RatesUS, Washington State, King County, US, Washington State, King County,
SeattleSeattleThree Year Rolling Average, 1981-2004Three Year Rolling Average, 1981-2004

Contributions to the Overall Decline Contributions to the Overall Decline in Infant Mortality in King Countyin Infant Mortality in King County
First StepsFirst Steps: MaternityMaternity support and expansion of Medicaid coverage of support and expansion of Medicaid coverage of prenatal servicesprenatal services
Safe Sleep: Safe Sleep: Back to Sleep CampaignBack to Sleep Campaign
Medical Advances: Medical Advances: Neonatal intensive careNeonatal intensive care
Behavioral:Behavioral:Decline in use of tobacco, alcohol, unintendedDecline in use of tobacco, alcohol, unintended pregnancies pregnancies

4.0
11.1
17.2
4.55.5
0
5
10
15
20
25
Rate per 1,000
Live Births
African American
American Indian/ Alaska Native
White
Latino/HispanicAsian
Infant Mortality Rates by Race/Ethnicity, King County, Three Year Rolling
Averages, 1985-2004

Perinatal Periods Of Risk Perinatal Periods Of Risk (PPOR) Approach(PPOR) Approach
A A simple approachsimple approach..
identify gapsidentify gaps in the community. in the community.
target resourcestarget resources for prevention activities. for prevention activities.
mobilize the communitymobilize the community to action. to action.

PPOR guides strategies to PPOR guides strategies to improve birth outcomesimprove birth outcomes
Prematurity and low birthweight Prematurity and low birthweight lead to infant mortality.lead to infant mortality.
PPOR method gives information that PPOR method gives information that guides community strategies to help guides community strategies to help infants be born healthy.infants be born healthy.

PPOR FindingsPPOR FindingsWA State, 2000-2004WA State, 2000-2004
Infant HealthInfant Health is the highest contributor is the highest contributor to preventable FIMR among American to preventable FIMR among American Indian/Alaska Natives Indian/Alaska Natives
Maternal Health/PrematurityMaternal Health/Prematurity is the is the highest contributor among African highest contributor among African Americans and the second highest Americans and the second highest contributor among AI/AN.contributor among AI/AN.
Maternal Care is the third highest Maternal Care is the third highest contributor to among AI/AN.contributor to among AI/AN.
Newborn Care is consistently the lowest Newborn Care is consistently the lowest and is similar for all racial/ethnic groups.and is similar for all racial/ethnic groups.

Implications/”Opportunity Implications/”Opportunity Gaps”Gaps”
Maternal Health/
Prematurity
Infant Health
Preconception Health Health BehaviorsPerinatal Care
+ EXPAND STRATEGIES to address social factors giving rise to disparities
Sleep Position Breast Feeding Injury PreventionMedical Care for Infections and Chronic Conditions

% of Births 2000-2002
Time Trend 1993-2002
% of Births 2000-2002
Time Trend 1993-2002
% of Births 2000-2002
Time Trend 1993-2002
Low Birth Weight (< 2500 g) 10.5* -- 6.6 -- 5.3 2* 1.3Very Low Birth Weight (< 1500 g) 2.2* -- 1.9* 0.8 -- 2.6* 2.3*Preterm (<37 weeks gestation, calc.) 18.9* -- 16.9* -- 11.9 1.6* 1.4*Multiple Birth (twins, triplets, etc.) 4.1 3.2 3.6 1.2 0.9Mother's Age < 18 4.0* 6.4* 1.5 2.7* 4.2*Single Mother 54.1* 58.7* -- 20.5 2.6* 2.9*Late (3rd) or No Prenatal Care 4.8* 6.5* 2.0 2.4* 3.3*Inadequate Prenatal Care (Kotelchuck) 19.2* 18.8* 7.7 2.5* 2.4*Smoking During Pregnancy 11.1* 19.8* 8.0 1.4* 2.5*Alcohol Use During Pregnancy 1.6 4.0 2.7 0.6 1.5
Rates and rate ratios followed by an asterisk (*) are statistically significantly higher than the rate for whites. Indicates a statistically significant increase over the period 1993-2002. Indicates a statistically significant decrease over the period 1993-2002.
American Indian/Alaska Native: White
Rate Ratio(2000-2002)
African Americans American Indian/
Alaska Natives WhitesAfrican
American: White Rate Ratio
(2000-2002)
Prevalence and Trends in Birth Risk Factors Prevalence and Trends in Birth Risk Factors by Race, King Countyby Race, King County

How Stress Can Affect Health:How Stress Can Affect Health: Increased cortisol (fight/flight hormones) results in increased Increased cortisol (fight/flight hormones) results in increased
cardiovascular function cardiovascular function
Can lead to high blood pressure, depressed immune function with Can lead to high blood pressure, depressed immune function with increased vulnerability to infection, and depression. All of these can increased vulnerability to infection, and depression. All of these can contribute to risk of preterm delivery.contribute to risk of preterm delivery.
These stress responses are designed to help us deal with short term These stress responses are designed to help us deal with short term threats, but for many, the stressors don’t go away. threats, but for many, the stressors don’t go away.
Long-term, chronic stress does not allow for system recovery and Long-term, chronic stress does not allow for system recovery and predisposes to adverse health effectspredisposes to adverse health effects

Reported Stressful Life Events During Year Before Delivery
King County, 1999-2001
Stress EventsAfrican
American
American Indian/Alask
a Native White
Changed residence (moved) 44%* 53%* 33%
Argued with partner more than usual 36%* 43%* 17%
Had bills and couldn't pay 31%* 42%* 14%
Someone close died 24%* 25% 15%
Close family member ill and hospitalized 24% 22% 24%
Separated or divorced from partner 20%* 19%* 5%
Someone close had drinking/drug problem 15% 28%* 13%
Partner said he didn't want pregnancy 15%* 21%* 8%
Husband/partner lost job 14% 20%* 8%
Mother lost job 21%* 15%* 5%
Mom or partner went to jail 10%* 22%* 4%
Involved in a physical fight 7% 12%* 4%
Homeless 11%* 15%* 1%
Reported 5 or more stress events 12%* 23%* 4%
Stress factor prevalences followed by an asterisk (*) are statistically significantly higherthan the estimate for whites.
Data Source: Pregnancy Risk Assessment Monitoring System (PRAMS)

Lack of Social Support During Pregnancy by Race/Ethnicity,
King County, 1999-2001
29%
22%
16%
21%24%
17%
11%15%
13%10%
7% 7%
0%
5%
10%
15%
20%
25%
30%
35%
40%
No one to loanme $50
No one to helpme if I was sick
& in bed
No one to give me a ride to the
doctor
No one to talk with aboutmy problems
Pe
rce
nt
African American
American Indian/Alaska Native
White
Data Source: Pregnancy Risk Assessment Monitoring System (PRAMS)

INSTITUTIONALIZED RACISM/INSTITUTIONALIZED RACISM/Historical TraumaHistorical Trauma
DiscriminatioDiscriminationn
PovertyPoverty AbuseAbuse Internalized Internalized RacismRacism• Health CareHealth Care
• HousingHousing• Legal SystemLegal System• EmploymentEmployment• Refused care Refused care
over IHS over IHS statusstatus
• Affordable HousingAffordable Housing• Moving frequentlyMoving frequently• Adequate Adequate
EducationEducation• EmploymentEmployment• Access to Health Access to Health
CareCare• Perceived as Perceived as
wealthywealthy STRESSSTRESS
Direct Effects: Endocrine System Response - Increased cortisol Direct Effects: Endocrine System Response - Increased cortisol levels, decreased immune function, increased levels, decreased immune function, increased vulnerability to infection, trigger onset of laborvulnerability to infection, trigger onset of labor
Indirect Effects: Maternal Behaviors – Smoking, alcohol, substance Indirect Effects: Maternal Behaviors – Smoking, alcohol, substance use, poor nutrition, survival supersedes wellnessuse, poor nutrition, survival supersedes wellness
DISPARITIES IN BIRTH DISPARITIES IN BIRTH OUTCOMEOUTCOME
• InstitutionalInstitutional• InterpersonInterperson
alal• CyclesCycles• Substance Substance
• HopelessnessHopelessness• Self-hatred and blameSelf-hatred and blame• Inability to see family/ Inability to see family/
community as supportcommunity as support• Ancestry seen as Ancestry seen as
hindrance to life’s hindrance to life’s goalsgoals
Mayet Dalila, IntraAfrikan Konnections

Indigenist model of trauma, coping, and Indigenist model of trauma, coping, and health outcomes for American Indian health outcomes for American Indian
women women (Walters K. 2002)(Walters K. 2002)

What more needs to be done:What more needs to be done: Continue support of pregnant women’s Continue support of pregnant women’s
health care: prenatal care, MSS/ICM, health care: prenatal care, MSS/ICM, outreach.outreach.
Find support for community mobilization Find support for community mobilization effortsefforts
Community collaboration around housing, Community collaboration around housing, income equity, access to quality education, income equity, access to quality education, access to culturally relevant, culturally access to culturally relevant, culturally appropriate health care. . .appropriate health care. . .
Decrease the impact of inequalities and Decrease the impact of inequalities and racism on women and families through racism on women and families through community support. community support.
NAWDIM & Brown Sugar BabiesNAWDIM & Brown Sugar Babies

What more needs to be done:What more needs to be done:
Continue the PPOR analysis and community engagement process Continue the PPOR analysis and community engagement process to use the data to target prevention efforts and support the work of to use the data to target prevention efforts and support the work of the communitythe community
Need for prevention to focus on preconceptional health, health Need for prevention to focus on preconceptional health, health behaviors, and specialized perinatal care services behaviors, and specialized perinatal care services
Sustained need for early and continuous prenatal care services, Sustained need for early and continuous prenatal care services, referral of high-risk pregnancies and good medical management of referral of high-risk pregnancies and good medical management of medical problemsmedical problems
Continued need for programs that support infant health such as Continued need for programs that support infant health such as SIDS prevention, access to a medical home, and injury preventionSIDS prevention, access to a medical home, and injury prevention

What You Can Do:What You Can Do:
Work on adequate housing, income equity, quality education, access to culturally appropriate health & social services.
Provide culturally appropriate mental health services for people of color & low-income folks.
Get training on undoing institutionalized racism Undoing Institutionalized RacismUndoing Institutionalized Racism, People’s Institute for Survival & Beyond, People’s Institute for Survival & Beyond PBS Video: PBS Video: Race: The Power of IllusionRace: The Power of Illusion PBS Video: PBS Video: Unnatural Causes: Is Racism Making Us Sick?Unnatural Causes: Is Racism Making Us Sick? (March, 2008) (March, 2008)
Involve community members, clients, consumers in defining your work.
“Injustice anywhere is a threat to justice everywhere.”
Martin Luther King, Jr.

Thank you!Thank you!