Embed Size (px)
Citation preview

Sharon Silow-Carroll and Jennifer n. edwardS health ManageMent aSSoCiateS
Abstract: One of the most common types of health care–associated infections is the cen-tral line–associated bloodstream infection (CLABSI), which can result when a central venous catheter is not inserted or maintained properly. About 43,000 CLABSIs occurred in hospitals in 2009; nearly one of five infected patients died as a result. This report synthe-sizes lessons from four hospitals that reported they did not experience any CLABSIs in their intensive care units in 2009. Lessons include: the importance of following evidence-based protocols to prevent infection; the need for dedicated teams to oversee all central line insertions; the value of participation in statewide, national, or regional CLABSI collabora-tives or initiatives; and the necessity for close monitoring of infection rates, giving feed-back to staff, and applying internal and external goals. The report also presents ways these hospitals are spreading prevention techniques to non-ICU units, and strategies for prevent-ing other health care–associated infections.
EXECUTIVE SUMMARYWith growing pressures on hospitals to improve patient safety and contain costs, reducing health care–associated infections (HAIs) has become a priority.1 Between 4 percent and 5 percent of hospital admissions result in an HAI, an infection that a patient acquires during the course of receiving treatment for other conditions within a health care setting. The annual direct cost of providing treat-ment for a preventable infection is substantial; estimates range from $28 billion to $45 billion (in 2007 dollars).2 Such estimates do not include indirect costs related to lost productivity or nonmedical costs, and do not factor in the intangi-ble cost associated with a patient’s diminished quality of life.
Eliminating central line–associated bloodstream infections (CLABSIs), one type of health care–associated infection, is a particularly promising area of activity. CLABSIs are infections introduced when a central line (also known as central venous catheter or tube) is placed in a large vein in the neck, chest, or arm to enable the rapid administration of fluids, blood, or medications to criti-cally ill patients.3 Central venous catheters disrupt the integrity of the skin, mak-ing infection with bacteria and/or fungi not only possible but also dangerous, as the infection may spread to the bloodstream.4 The Centers for Disease Control and Prevention (CDC) defines a CLABSI as a primary bloodstream infection (i.e., with no apparent infection elsewhere in the body) in a patient who had a
To download this publication and learn about others as they become available, visit us online at www.commonwealthfund.org and register to receive Fund e-Alerts.
Commonwealth Fund pub. 1559 Vol. 21
The mission of The Commonwealth Fund is to promote a high performance health care system. The Fund carries out this mandate by supporting independent research on health care issues and making grants to improve health care practice and policy. Support for this research was provided by The Commonwealth Fund. The views presented here are those of the authors and not necessarily those of The Commonwealth Fund or its directors, officers, or staff.
For more information about this study, please contact:
Sharon Silow-Carroll, M.B.A., M.S.W.Health Management [email protected]
Eliminating Central Line Infections and Spreading Success at High-Performing Hospitals
Synthesis Report • December 2011

2 the CoMMonwealth fund
central line inserted within 48 hours of developing the infection.
Although guidelines and protocols to prevent CLABSIs have been developed, tested, and recom-mended to hospitals, infections persist. There were an estimated 43,000 CLABSIs in hospitals in 2009, with most occurring in intensive care units (ICUs), where 48 percent of patients have central venous catheters.5 According to the CDC, nearly one of five patients who contract a CLABSI dies from it.6
This report synthesizes the findings and lessons from four hospitals that experienced zero CLABSIs in their ICUs in 2009. These hospitals—Bronson Methodist Hospital of Kalamazoo, Mich.; Englewood Hospital and Medical Center of Englewood, New Jersey; Presbyterian Intercommunity Hospital of Whittier, Calif.; and Southern Ohio Medical Center of Portsmouth, Ohio—employed many of the same strat-egies and tools to achieve this result, including:
• The adoption of standardized, evidence-based pro-tocols to focus staff attention on proven methods of preventing CLABSIs. These protocols call for the use of full-barrier precautions, chlorhexidine antiseptic, and sterile dressing; optimal vein selec-tion; increased attention to hand hygiene; and the prompt removal of central line catheters.
• The use of dedicated, specially trained teams to conduct and/or oversee all line insertions and maintenance. Nurses from these teams monitor lines, change dressings, and advise critical care and floor nurses about line management. They are empowered to stop a central line insertion if a physician is not following the evidence-based pro-tocol. All of the hospitals also employ critical care intensivists, which helps to standardize ICU prac-tices and promote infection tracking and continuity of care for patients with central venous catheters.
• The use of checklists that reinforce the protocols and “daily goals” sheets that focus on the goals of care, both of which spur discussion and documen-tation of readiness to remove a central line or sub-stitute a less risky type of catheter.
• Participation in statewide, national, or regional CLABSI collaboratives or initiatives.
As a result of these and other efforts, the four hospitals eliminated CLABSIs within their ICUs in 2009 (the latest period for which widespread infection data were available at the start of this study). Many have experienced multiple years without an infection.
The hospitals attribute their success in part to promoting an infection prevention culture through physician “champions,” collaborative educational pro-grams, and performance measurement. All rely heavily on the data they collect on infection rates for bench-marking and goal-setting, as well as for internal and public reporting. The data are provided to staff so they are able to monitor their progress. In some instances, performance bonuses are tied to meeting infection and safety goals.
This report details the hospitals’ efforts to pre-vent central line infections and spread these techniques to non-ICU units. It also examines their efforts to pre-vent other health care–associated infections, such as catheter-associated urinary tract infections (CAUTIs), ventilator-associated pneumonia (VAP), and surgical site infections (SSIs).
While spreading prevention techniques to other units and to other health care–associated infections has proven challenging, the hospitals have identified some promising techniques. These include: maximizing the use of hospitalists to spread new protocols quickly and consistently, communicating prior success with CLABSI prevention, limiting line insertion to a small group of specially trained teams or individuals, and placing a dedicated nurse educator on every unit to ensure new tools and processes are understood, imple-mented, and sustained.
The feasibility of eliminating CLABSIs in intensive care, and greatly reducing other hospital-acquired infections, points to three policy opportuni-ties to promote further success. The first is to support hospitals and clinicians’ competitive desire to be the best by expanding on improvement projects such as “On the Cusp,” and spreading best practices from innovative hospitals.7 Accreditors can also continue to

eliMinating Central line infeCtionS and Spreading SuCCeSS at high-perforMing hoSpitalS: SyntheSiS report 3
emphasize the importance of following infection pre-vention protocols, use of specialty staff for line inser-tion, and internal reporting. In 2010, Congress allo-cated $34 million to support new projects in hospitals to reduce HAIs.
Second, states could follow the federal govern-ment’s lead by requiring public reporting of infection rates by all hospitals, which are increasingly reporting performance data on their own Web sites and promot-ing their quality and safety records in marketing.
Third, the Centers for Medicare and Medicaid Services (CMS), many state Medicaid programs, and other large health care purchasers have moved to non-payment for certain types of errors and infections. If all payers refused to pay for hospital-acquired infec-tions, hospitals would increase their efforts to avoid them.
BACKGROUND Guidelines and protocols to prevent central line–asso-ciated bloodstream infections have been developed, tested, and recommended to hospitals. The most com-monly used are the CDC guidelines that were initially published in 2002. The guidelines include recommen-dations for increasing or encouraging:
• hand hygiene;
• the use of full-barrier precautions (sterile hat, mask, gloves, and gown) during insertion of a central line;
• cleaning the patient’s skin with the antiseptic chlorhexidine;
• application of a sterile dressing after a line is inserted;
• optimal vein selection (the subclavian vein is the preferred site for non-tunneled catheters); and
• daily review of line necessity, with prompt removal of unnecessary lines.
The CDC and the Healthcare Infection Control Practices Advisory Committee, which provides guid-ance to the CDC, released updated and expanded
guidelines in April 2011. The new guidelines empha-size the importance of the steps above, as well as edu-cating and training health care personnel, avoiding routine replacement of certain catheters, and tracking and reporting infection rates, among other strategies.8
The Institute for Healthcare Improvement (IHI), a nonprofit organization promoting health care improvement, teaches that reducing central line infec-tions requires adherence to five key components (hand hygiene, maximal barrier precautions, chlorhexidine, optimal site selection, and daily review of necessity), collectively known as the “central line bundle.” A hos-pital assessing its compliance with the standard as part of the IHI improvement strategy must achieve all five components of the bundle.9
Local, state, and national collaboratives have also encouraged and assisted hospitals in the adoption of the recommended practices. The Keystone Intensive Care Unit Project (Keystone Project), which began in Michigan in 2003, was one of the first widespread efforts to reduce CLABSIs. More than 70 hospitals working with the Michigan Hospital Association and the Johns Hopkins University Quality and Safety Research Group led by Peter J. Pronovost, M.D., were coached to use a framework and tools that were proven to facilitate the adoption of key prevention strategies.10
ICUs participating in the Keystone Project reduced infections on average from 2.5 infections per 1,000 line days in 2004 to .83 infections per 1,000 line days in 2009.11 Further, 60 percent of the ICUs evalu-ated prevented central line infections for a year or more, and 26 percent went without infections for at least two years.12 Among six hospitals that were part of the Michigan Keystone Project, on average, 29.9 catheter-related bloodstream infections and 18.0 cases of ventilator-associated pneumonia were averted per hospital annually. The average cost of the intervention per infection averted ($3,375) was significantly less than the estimated cost per infection episode (ranging from $12,208 to $56,167).13 The Agency for Health Care Research and Quality has since supported the spread of this effort through “On the CUSP: Stop

4 the CoMMonwealth fund
BSI,” in which 43 states are seeking to replicate the Keystone ICU model.14
Congress appropriated $34 million to the Agency for Healthcare Research and Quality for fiscal year 2010 for projects to prevent and reduce health care–associated infections. It funded 22 projects in hospitals, ambulatory care settings, long-term care facilities, and other settings.15
In addition, public health and professional asso-ciations—including the CDC, the IHI, and the Association for Professionals in Infection Control and Epidemiology, are making guidelines, educational materials, and toolkits available for hospital use.16 The Commonwealth Fund’s WhyNotTheBest.org Web site provides comparative data, case studies, and improve-ment tools that can be used to prevent CLABSIs.
Monitoring and Use of Performance Incentives To track progress and encourage improvement, public reporting of CLABSIs is growing. Starting in 2011, hospitals must track and report CLABSIs among adult, pediatric, and neonatal ICU patients in order to receive an annual 2 percent increase in Medicare payments in fiscal year 2013.17 Hospitals must report their infection rates to the CDC’s National Healthcare Safety Network (NHSN). The data are shared with CMS and will be made public on its Hospital Compare Web site. The U.S. Department of Health and Human Services has also set a national goal of reducing CLABSIs by 50 percent by 2013.
Before this national requirement, 16 states had already required hospitals to report CLABSI data, including several states that audit the hospital-reported data for accuracy. On a national level, about 1,600 hospitals were voluntarily submitting CLABSI data to the NHSN in 2009. In addition, hospitals participating in the Leapfrog Group’s Hospital Recognition Program have been submitting CLABSI data for several years, and their scores contribute to Leapfrog’s overall qual-ity and safety ratings. In 2010, the Consumer’s Union, an independent, nonprofit testing and information organization and publisher of Consumer Reports, began tallying hospital-provided data to create a
national profile of CLABSI incidence, and this infor-mation is available on The Commonwealth Fund’s WhyNotTheBest.org.
Accreditation and financial incentives are also used to promote CLABSI prevention. Since 2008, vas-cular catheter-associated infections do not qualify for higher Medicare payment rates, which puts hospitals at risk for assuming the direct costs associated with treat-ing these infections. Beginning in 2010, U.S. hospitals seeking accreditation with the Joint Commission are expected to implement best practices or evidence-based guidelines to prevent CLABSIs.
Success, But Major Challenges RemainThere have been significant successes associated with adoption of CLABSI prevention best practices, including:
• an estimated 25,000 fewer CLABSIs in 2009 com-pared with 2001, which represents a 58 percent reduction;
• between 3,000 and 6,000 lives and $414 million in potential excess health care costs were saved in ICUs in 2009; and
• approximately $1.8 billion in cumulative excess health care costs and up to 27,000 lives were saved between 2001 and 2010.18
Despite this success and the availability of evi-dence-based standards, wide variation in CLABSI rates across hospitals remains. This suggests disparities in adoption, compliance, and sustainment of recom-mended protocols. Also, CLABSI reduction is largely focused on ICUs; the spread of successful practices to other hospital units and outpatient settings (particularly outpatient hemodialysis centers), and to other infec-tions, remains a major challenge.
IMPLEMENTATION STRATEGIES AT CASE STUDY HOSPITALSIn an effort to identify innovative strategies and tools that help hospitals reduce CLABSIs and spread their successes to other units and infections, this report

eliMinating Central line infeCtionS and Spreading SuCCeSS at high-perforMing hoSpitalS: SyntheSiS report 5
profiles four hospitals that reported zero CLABSIs in 2009 (see Appendix for methodology used.) These hospitals are:
• Bronson Methodist Hospital (Bronson) of Kalamazoo, Michigan, the flagship hospital of a system that has one main competitor in the area and a hospital that has been actively involved in state infection prevention initiatives;
• Englewood Hospital and Medical Center (Englewood) of Englewood, New Jersey, a subur-ban community hospital that is unaffiliated with a system, faces fierce competition in the area, and engaged in some collaboration with other hospitals;
• Presbyterian Intercommunity Hospital (Presbyterian) of Whittier, California, a large, free-standing hospital unaffiliated with a system that has begun to integrate its operations with physi-cians in the competitive Los Angeles market; and
• Southern Ohio Medical Center (Southern Ohio) of Portsmouth, Ohio, which is the only hospital in a system that operates in a rural and economically depressed area with little competition and which participates in national quality improvement efforts.
Reducing CLABSIs in the ICU The strategies used by these hospitals are fairly consis-tent. They focus attention on the importance of pre-venting CLABSIs and encourage staff to strictly adhere to evidence-based protocols.
Standardization Using Evidence-Based Protocols All four hospitals used the CDC’s CLABSI prevention guidelines, listed above, to redesign and standardize their line insertion and maintenance protocols. The hospitals also found the IHI bundle to be useful for teaching. Additional clinical interventions included use of an antimicrobial dressing that may help prevent migration of normal skin flora into the bloodstream and the use an ultrasound vessel finder probe to guide
line placement and decrease the need for multiple nee-dle sticks.
The hospitals all reported that training was criti-cal to achieving consistency. Each new physician, resi-dent, or nurse to work on a line team was trained in the proper CLABSI protocols before getting hands-on experience.
Introducing Protocols Through Collaboratives and Staff Engagement Activities The hospitals found the way the protocols were intro-duced to key staff was critical to their acceptance. Three of the four hospitals point to participation in collaboratives as a turning point in CLABSI reduction. The structure of the collaboratives differed, but each provided access to experts as well as peers who were facing similar challenges. Through these initiatives, the hospitals learned about evidence-based protocols for preventing CLABSIs; the importance of measure-ment, data, and teams; and strategies for implementing and sustaining the protocols at their institution.
The hospitals’ experiences suggest that learning about successful quality efforts and meeting with peers are highly motivating. Two of the hospitals reported that pairing staff members—such as nurses with physi-cians or administrative with clinical leaders—in col-laboratives promoted good working relationships.
Adoption of the standardized protocols was also facilitated by clinical “champions,” who were often identified and encouraged by hospital leaders. Typically, these champions were intensivists or ICU physicians, teamed with nurse managers, who were passionate about the need to implement new practices. One of the hospitals also found it helpful to bring in a national expert to educate and motivate staff. Another hospital, as part of an education campaign, used a large, colorful display in the break room to illustrate how each component of the CLABSI protocol is a key to saving a patient’s life.
Central Line Kits and Carts Procedure carts with pre-packaged central line inser-tion kits are used to ensure the right supplies are avail-able and used for each line placement so that staff do

6 the CoMMonwealth fund
not have to risk contamination or waste time searching for materials. The kits typically include a sterile mask, cap, gloves, full drape, disinfectants, lines, needles, syringes, and often guidelines or a checklist designed to reinforce the protocol. The central line carts move with the team from room to room. One hospital com-bines the standardized pre-packaged kits with physi-cian-specific items to optimize efficiency and encour-age use of appropriate supplies.
Checklists and Nurse Empowerment Checklists delineate, guide, and document completion of each step in the central line insertion process. In addition, checklists become a source of data for qual-ity departments to verify adherence to the protocol. The checklist is completed by a nurse, and if there is a deviation or a step missed, nurses in these hospitals have been taught to speak up and “stop the line.” The hospitals report that they are able to do so because of staff member’s focus on patient safety and strong backing by nurse and physician management.
Intensivists and Highly Specialized Teams These high-performing hospitals use a small group of intensivists to insert lines (or oversee insertion) in ICU patients and manage overall care. The intensivists have special training in critical care, are accessible 24 hours a day, and consistently follow care protocols—all of which leads to more accurate and consistent tracking of infections and greater accountability. These hospi-tals also had physician champions among their inten-sivists who focus other clinical staff in the unit on the need to adopt new practices.
The full teams involved in CLABSI elimination have taken a variety of configurations, depending on the size and scope of the ICU. All are interdisciplinary, include at least one specially trained nurse and ICU physician, and were formed with the expectation that the risk of infection would decline when a small, select group of people perform a specific task such as insert-ing central lines.
Focus on Post-Insertion Care Well aware that a patient may become infected as long as a line is in a central vein, all four hospitals strictly
adhere to line maintenance guidelines. Designated, specially trained nurses monitor lines, change dress-ings, and advise and educate critical care and floor nurses on line management.
Avoiding Central Lines and Expediting Removal CDC guidance to hospitals encourages the reassess-ment of central line necessity on a daily basis and advocates removing the line or moving it to a less risky part of the body as soon as possible. These hos-pitals perform daily reviews of the lines—typically during interdisciplinary rounds—to assess the need for the central line to remain in place. Nurses must docu-ment on “daily goals” sheets that the issue was dis-cussed and the reason for continued need if the line is not removed.
SPREADING CLABSI SUCCESS THROUGHOUT HOSPITAL After achieving significant success in preventing CLABSIs in the medical ICU, these hospitals began extending CLABSI protocols to other critical care units and hospital floors where central lines are inserted with less frequency. Success at preventing CLABSIs also has guided the hospitals’ efforts to eliminate other types of hospital-acquired infections, such as catheter-associated urinary tract infections (CAUTIs), ventilator-associated pneumonia (VAP), and surgical site infections (SSI), efforts that are described in more detail below. These efforts have led to infection rates much closer to zero and have pro-duced results that exceed national benchmarks.
Investment in Quality and Safety Improvement The four case study hospitals attribute much of their success in controlling infections to a strong, hospital-wide culture that promotes clinical excellence. Hospital administrators devote significant resources to the measurement of clinical indicators, goal-setting (including infection rates), benchmarking, internal and public reporting, feedback on performance, review of standards and best practices, and participation in col-laboratives. Their commitment to clinical excellence is also reflected in their hiring, nurturing, and support for

eliMinating Central line infeCtionS and Spreading SuCCeSS at high-perforMing hoSpitalS: SyntheSiS report 7
physician and nurse champions, who often take the lead in quality improvement initiatives. Some of the hospitals conduct a culture of safety survey to assess organizational progress and instill accountability by including infection rates as part of annual salary or bonus reviews.
Task Forces and Use of Infection Preventionists The case study hospitals created infection prevention task forces and/or hired infection preventionists to facilitate spread of best practices. Multidisciplinary task forces study, modify, and disseminate recom-mended protocols to reduce CLABSIs and other infec-tions throughout the hospital. They also monitor infec-tions and investigate the root cause of each case. Infection preventionists, who are certified in infection control, educate existing and new staff in protocols and conduct hospital-wide surveillance to track infec-tion rates.
Electronic Health Records Use of electronic health records (EHRs) can facilitate infection surveillance and documentation of compli-ance with infection prevention protocols, though man-ual tracking has also been working at these hospitals. Most of the hospitals are in the process of implement-ing or upgrading their EHR systems, and expect that the new systems will improve tracking and adherence to infection control standards. For example, EHRs can record total central line days, which form the denomi-nator in CLABSI rates, thus enabling hospitals to eas-ily track rates by unit and over time. One hospital leader noted that their new EHR will help staff moni-tor whether they have successfully removed Foley catheters within two days of an operation, a require-ment of the CAUTI reduction protocol.
Hand Hygiene Alcohol-based sanitizer placed in every patient room can increase hand hygiene compliance. The waterless sanitizer is faster and less drying than washing with soap and water, so nurses and physicians have been more likely to use it. Hospitals audit and post results of hand hygiene compliance, which helps to motivate staff.
Private Patient Rooms Reduce Infection Rates One of the case study hospitals underwent a redesign and built only private patient rooms, which reduce risk of patient-to-patient infections and the need for room transfers. The hospital reports an 11 percent decline in infections and a positive return on investment as sav-ings in averted infections outweighed the extra costs associated with private rooms.
Challenges to Spread Extending CLABSI control practices from the medical ICU to other hospital units and different health care–associated infections has not been simple or straight-forward. Introducing protocols to other critical care units (such as cardiac, neonatal, and surgical ICUs) has required getting buy-in from clinical leaders who did not participate in the CLABSI collaboratives nor in the initial adoption of the protocols. Also, the larger size and diversity of the clinical staff caring for patients on non-ICU inpatient units has made it harder to achieve strict adherence to protocols.
The hospitals also found it difficult to collect data on the rates of infections outside of the ICU since most other units do not track the number of days patients have a central line—information needed to calculate infection rates. In addition, ICU staff are more vigilant than staff elsewhere about prevention because their patients are often at greater risk of a bad outcome from an infection due to their weakened con-ditions, and their higher staff-to-patient ratio facilitates this focus. Finally, hospital leaders have found that the protocols are not necessarily foolproof, as the root cause of some infections are not discernable and/or may be out of staff’s control.
The methods these high-performing hospitals used to address such challenges are described below.
Limit Line Insertions and Oversight to Specially Trained Teams A key component to reducing CLABSIs in other hos-pital units or floors is the use of specially trained, ded-icated teams or individuals who oversee and/or per-form all line insertions and maintenance throughout

8 the CoMMonwealth fund
the hospital. Each of the four hospitals has a dedicated line team outside of the ICU.
Kits and Checklists Combining the use of pre-packaged central line kits with checklists helps ensure line insertions are con-ducted according to protocol; however, the placement of central line kits must be coupled with monitoring to ensure their use. One hospital found that it was neces-sary to assign a nurse to be responsible for restocking kits in the emergency department, which can be extremely busy.
Hospitalists All four hospitals found that using hospitalists to man-age the care of a large portion of patients has facili-tated and sped dissemination and consistent use of evi-dence-based practices—including CLABSI proto-cols—to the floors. As with intensivists, the hospital-ists provide round-the-clock coverage, are fully accountable to the hospital, and tend to be well informed of national standards and willing to adopt new protocols and perform them consistently.
Hospital-Wide Education and Feedback Initial and ongoing education of staff throughout the hospital is critical for disseminating and sustaining best practices. Throughout the hospitals, unit leaders and staff were more likely to accept the protocols after seeing the evidence of their impact. One of the hospi-tals has a dedicated educator (generally a nurse) on every unit to instruct staff on the latest protocols and ensure that a new process is maintained. This is espe-cially important when introducing infection protocols in emergency departments, where a broader group of individuals (e.g., rotating residents) may be involved in central line insertion. Tracking CLABSI rates and feeding the data back to unit managers, physicians, and staff also help to keep staff focused and motivated.
Applying Prevention Framework to Other Health Care–Associated Infections The hospitals’ success in preventing CLABSIs moti-vated them to work to eliminate other health care–associated infections. Their efforts built on the
CLABSI infection prevention framework and focused on adopting standardized, recommended protocols for the following infections.
Catheter-Associated Urinary Tract Infections All four hospitals have implemented many of the CDC-recommended steps to avoiding catheter-associ-ated urinary tract infections (CAUTIs), such as using catheters only when necessary and emphasizing hand hygiene and proper bag placement.19 Practices that support adherence to the guidelines include: participa-tion in learning initiatives such as IHI’s Web-based CAUTI Expedition; use of strict nurse protocols that define criteria for insertion, help nurses assess risk versus benefit, and reduce the use of catheters for nurses’ convenience; the use of a standard post-surgi-cal order set (based on the Joint Commission’s Core Measure program) calling for removal of Foley cathe-ters within two days of an operation; and requirement for daily review and documentation of catheter necessity.20
One hospital screens all patients arriving with a urinary catheter to determine if they have an infection, thus speeding treatment and removal of the catheter and reducing avoidable hospital days. It also estab-lishes that the infection was not acquired in the hospi-tal, an important distinction that avoids Medicare’s non-payment for hospital-acquired conditions. Since the two-step urinalysis and urine culture process was implemented in 2008, incidence of CAUTIs has declined significantly at this hospital.
At least one hospital attributed its reduction in CAUTIs in part to use of silver-impregnated catheters. Another cited use of a new collection device and bar-rier cloths that decrease the occurrence of incontinent dermatitis, which can cause bacterial infection, skin ulcerations, and extreme discomfort. These products enable the nurses to remove a urinary catheter, while still preventing the risk of skin breakdown for inconti-nent patients.
Education is critical for patients and their care-givers, especially if a patient is going home with a catheter. Through printed materials and verbal instruc-tions, bedside nurses teach caregivers how to keep

eliMinating Central line infeCtionS and Spreading SuCCeSS at high-perforMing hoSpitalS: SyntheSiS report 9
catheters clean and reduce the risk of infection. Patients and family members demonstrate they under-stood the information by describing the procedure to the nurse.
Ventilator-Associated PneumoniaThe hospitals use recommended guidelines to reduce ventilator-associated pneumonia (VAP), generally implementing and monitoring these steps as a bundle, meaning all of them must be completed for a patient’s care to be deemed in compliance. The IHI ventilator bundle, part of the 100,000 Lives Campaign, requires semi-recumbent patient positioning (meaning the head of the bed is elevated at least 30 degrees); daily “seda-tion vacations” and assessment of extubation readi-ness; peptic ulcer disease prophylaxis; deep-vein thrombosis prophylaxis; and daily oral care with chlorhexidine.21
The case study hospitals have implemented innovative practices and tools that support and stan-dardize the recommended protocols. In one hospital, the EHR system automatically initiates an order sheet with recommended steps for all mechanically venti-lated patients in the ICU. The hospitals use a “wake up and breath” protocol that pairs spontaneous awak-ening and spontaneous breathing, accelerating efforts to wean patients off the ventilator. One hospital cre-ated an ICU Sedation and Delirium Data Collection tool to better track adherence to these practices.
The hospitals also hang an oral care kit at the bedside to enable easy access and provide staff with a visual reminder to perform mouth cleaning every two hours. Also, a visual indicator shows whether the head of the bed is at a 30-degree angle, a measure that ther-apists, intensivists, and the nurse manager are encour-aged to check multiple times per day. Elevation moni-toring may be accompanied by epiglottal suctioning by respiratory therapists. One of the hospitals established a goal of extubating open heart surgery patients in the operating room or within six hours of surgery. And a basic checklist in the patient chart helps ensure recom-mended steps are taken and improves communication across shifts.
Surgical Site Infections The CDC recommends a core set of guidelines to reduce surgical site infections, including maintaining proper body temperature and blood glucose levels, strict hygiene procedures and barrier precautions, and timely starting and stopping of antibiotics. 22 Case study hospitals reported a few ways they improved compliance with these recommendations, including providing surgeons with chlorhexidine antiseptic wipes and requiring the application of the wipes all over the body, not just at the surgical site. One hospital added a question to its pre-surgery registration checklist to determine whether the patient had a chlorhexidine sponge bath that morning.
The hospitals reported testing and treating patients for infections they may be carrying when they arrive for a surgical procedure. This may include nasal cultures to determine whether a patient is carrying the staph organism. One hospital added to their surgery pre-registration checklist a question determining whether the patient has had a Methicillin-resistant Staphylococcus aureus screening.
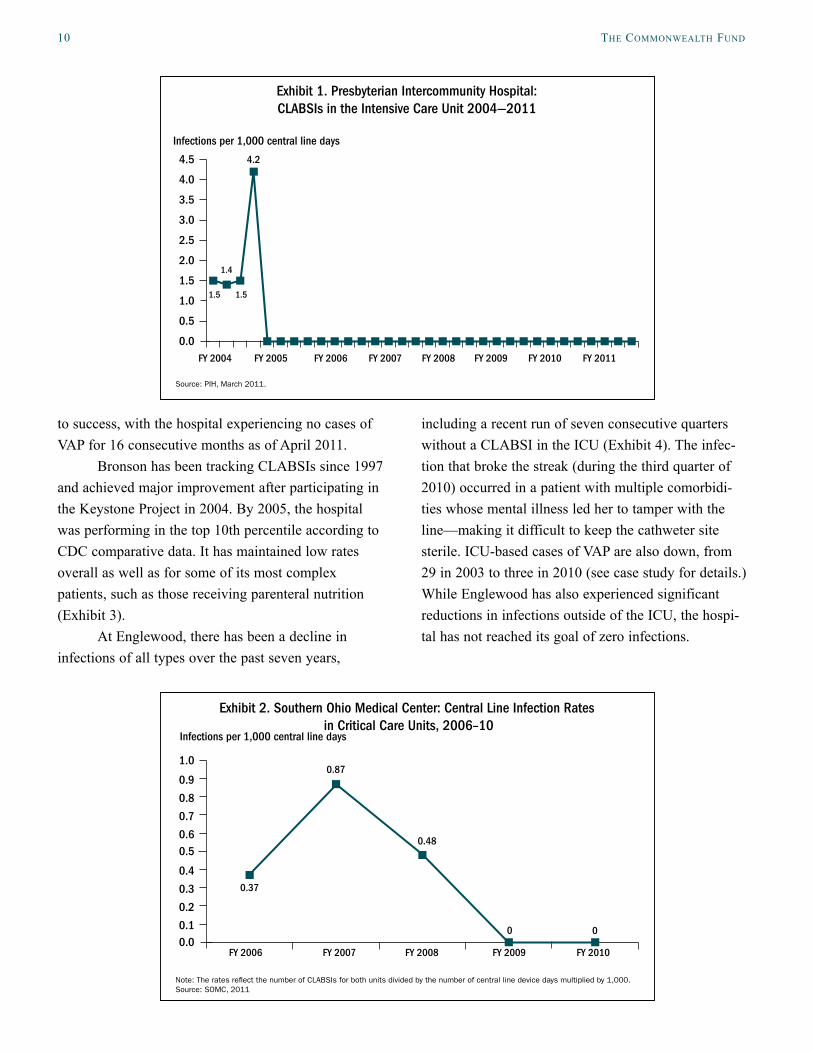
RESULTS OF INFECTION CONTROL EFFORTSAll four hospitals were selected for study on the basis of reporting no CLABSIs in 2009. Presbyterian has maintained zero CLABSIs in the ICU since 2005 (Exhibit 1).
When Presbyterian spread their CLABSI reduc-tion strategies to the neonatal intensive care unit and the medical/surgical floors, infection rates in those sites fell dramatically too. Last year, the hospital had just one infection in the neonatal ICU and one on all of the medical/surgical floors combined. Their CAUTI rate is also declining, but not as rapidly as it did for CLABSIs (see case study for details.)
There were no CLABSIs in Southern Ohio’s ICU and cardiac care unit in 2009 and 2010 (Exhibit 2). The last CLABSI in the ICU was in November 2007—with April 2011 marking 40 months of zero CLABSIs in the ICU (see case study for details). Applying a similar focus on VAP appears to have led
10 the CoMMonwealth fund
to success, with the hospital experiencing no cases of VAP for 16 consecutive months as of April 2011.
Bronson has been tracking CLABSIs since 1997 and achieved major improvement after participating in the Keystone Project in 2004. By 2005, the hospital was performing in the top 10th percentile according to CDC comparative data. It has maintained low rates overall as well as for some of its most complex patients, such as those receiving parenteral nutrition (Exhibit 3).
At Englewood, there has been a decline in infections of all types over the past seven years,
including a recent run of seven consecutive quarters without a CLABSI in the ICU (Exhibit 4). The infec-tion that broke the streak (during the third quarter of 2010) occurred in a patient with multiple comorbidi-ties whose mental illness led her to tamper with the line—making it difficult to keep the cathweter site sterile. ICU-based cases of VAP are also down, from 29 in 2003 to three in 2010 (see case study for details.) While Englewood has also experienced significant reductions in infections outside of the ICU, the hospi-tal has not reached its goal of zero infections.
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
FY 2004 FY 2005 FY 2006 FY 2007 FY 2008 FY 2009 FY 2010 FY 2011
1.4
1.5
4.2
1.5
Exhibit 1. Presbyterian Intercommunity Hospital: CLABSIs in the Intensive Care Unit 2004—2011
Source: PIH, March 2011.
Infections per 1,000 central line days
0.00.1
0.2
0.3
0.4
0.50.6
0.7
0.8
0.9
1.0
FY 2006 FY 2007 FY 2008 FY 2009 FY 2010
0.37
0.87
0.48
0 0
Exhibit 2. Southern Ohio Medical Center: Central Line Infection Rates in Critical Care Units, 2006–10
Note: The rates re�ect the number of CLABSIs for both units divided by the number of central line device days multiplied by 1,000. Source: SOMC, 2011
Infections per 1,000 central line days

eliMinating Central line infeCtionS and Spreading SuCCeSS at high-perforMing hoSpitalS: SyntheSiS report 11
LESSONSThere are both internal and external pressures on hos-pitals to reduce or eliminate CLABSIs and other health care–associated infections. Clinical and administrative leaders and staff at the case study hospitals were moti-vated by their desire to ensure patient safety and achieve clinical excellence. But like most institutions these hospitals are facing external pressures—require-ments for public reporting as well as financial
incentives by Medicare and other payers—to reduce CLABSIs and other infections.
There are national standards for reducing CLABSIs that have proven to be effective, as well as resources and opportunities to learn how to implement them. Hospitals that are not using recommended proto-cols, or are not using them consistently and univer-sally, should investigate why and work to remove obstacles that stand in the way of compliance.
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.55.0
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
2.1
2.2
00 0
3.9
2.4
1.1 1.10.7
1.71.9
0.08
Exhibit 3. Bronson Methodist Hospital: Catheter-Related Infections per 1,000 Catheter Days in Total Parenteral Nutrition (TPN) Patients, 1997–2009
Note: The hospital attributes the rise of catheter-related infections in TPN patients in 1998 to an increase in TPN patients and duration of TPN therapy.Source: Bronson Methodist Hospital, 2010.
Infections per 1,000 central line days
Exhibit 4. Englewood Hospital & Medical Center: Central Line Infection Rates in the ICU, August 2005–May 2010
Source: Englewood Hospital and Medical Center, April 2011.
3.583.69
3.212.82
3.583.39 3.15
3.95
3.16 3.16
3.45
4.24
Infections per 1,000 central line days
Month
0 0 0
-1
0
1
2
3
4
5
6
7
8
Aug—
05
Oct—
05
Dec—
05
Feb—
06
Apr—
06
Jun—
06
Aug—
06
Oct—
06
Dec—
06
Feb—
07
Apr—
07
Jun—
07
Aug—
07
Oct—
07
Dec—
07
Feb—
08
Apr—
08
Jun—
08
Aug—
08
Oct—
08
Dec—
08
Feb—
09
Apr—
09
Jun—
09
Aug—
09
Oct—
09
Dec—
09
Feb—
10
May
—10
0 0 0 0 0 0 0 0 0 00 0 0 0 0 0 0 00 0 0 00 0 0 00 0 0 00 0 0 00 0 0 00 0 0 0 0

12 the CoMMonwealth fund
Hospitals should also work to extend their infection prevention framework to other health care associated–infections.
The hospitals featured here have not solved all of their infection control problems, but they have achieved much success and appear to be on the right track. Other hospitals can learn from their experiences, which are summarized in the following lessons:
• Participate in infection control collaboratives and other learning opportunities and share your chal-lenges and best practices with other hospitals so that you may learn from others.
• Involve physician champions and multidisciplinary teams in adopting, adapting, and ensuring compli-ance with national standards and protocols.
• Use checklists and “daily goals” sheets to rein-force evidence-based guidelines.
• Use small, specially trained teams and individuals (including intensivists in the ICUs) to conduct and/or oversee line insertion and maintenance throughout the hospital.
• A dedicated infection preventionist, PICC (periph-erally inserted central catheter) team, and line nurse can help sustain improvements, even when multiple issues are competing for staff attention.
• Avoid using central lines when possible, maintain them well, and get them out as soon as possible.
• Sustain best practices with ongoing education, monitoring, and adjustments and provide perfor-mance data to staff to keep them focused on outcomes.
• Use transparency and incentives to foster a culture dedicated to patient safety and to validate and reinforce infection control efforts.
More testing, development, and dissemination of protocols to eliminate CAUTIs, cases of VAP, surgi-cal site infections, and other health care–associated infections are needed. But there are many existing standards and strategies that hospital leaders and staff can pursue to reduce infection rates. Public reporting of infection data and financial incentives will reinforce the infection control efforts of hospitals and other health care institutions.

eliMinating Central line infeCtionS and Spreading SuCCeSS at high-perforMing hoSpitalS: SyntheSiS report 13
noteS
1 Also sometimes referred to as hospital-acquired infections.
2 See http://www.cdc.gov/ncidod/dhqp/pdf/Scott_CostPa-per.pdf.
3 A central venous catheter inserted into a vein in the arm rather than a vein in the neck or chest is called a peripher-ally inserted central catheter, or PICC line.
4 The terms central line–associated bloodstream infection (CLABSI) and catheter-associated/related bloodstream infection (CA-BSI or CR-BSI) are often used inter-changeably; however, the term CLABSI is broader in scope than catheter-related bloodstream infections (CA-BSIs or CR-BSIs) and is used for surveillance of patient populations.CR-BSIsaredefinedbypreciselaboratoryfindingsthatidentifybacteriainthecentralvenouscath-eter as the source of the bloodstream infection.
5 In addition, an estimated 37,000 CLABSIs occurred among patients receiving outpatient hemodialysis in 2008. (A. Srinivasan, M. Wise, M. Bell et al., “Vital Signs: Central Line-Associated Blood Stream Infec-tions—United States, 2001, 2008, and 2009,” Morbidity and Mortality Weekly Report, March 4, 2011 60(8):243–48, http://www.ihi.org/IHI/Topics/CriticalCare/Inten-siveCare/ImprovementStories/PursuingPerfectionReport-fromHealthPartnersonReducingVAPCRBSI.htm).
6 See http://www.infectioncontroltoday.com/arti-cles/2007/07/catheters-and-infection-prevention.aspx.
7 See http://www.onthecuspstophai.org/about-us/.
8 N. P. O’Grady, M. Alexander, L. A. Burns et al., “Guide-lines for the Prevention of Intravascular Catheter-Related Infections Clinical Infectious Diseases,” Clinical Infec-tious Diseases, published online April 2011, http://cid.oxfordjournals.org/content/early/2011/03/30/cid.cir257.full.
9 Institute for Healthcare Improvement, implementation of central line bundle, http://www.ihi.org/knowledge/Pages/Changes/ImplementtheCentralLineBundle.aspx.
10 A. Lipitz-Snyderman, D. M. Needham, E. Colantuoni et al., “The Ability of Intensive Care Units to Maintain Zero Central Line-Associated Bloodstream Infections,” Archives of Internal Medicine, May 2011 171(9):856–58.
11 P. J. Pronovost, D. Needham, S. Berenholtz et al., “An In-tervention to Decrease Catheter-Related Bloodstream In-fections in the ICU,” New England Journal of Medicine,
Dec. 28, 2006 355(26):2725–32, http://www.nejm.org/doi/pdf/10.1056/NEJMoa061115; and Michigan Hospital Association Keystone: ICU Project overview, available at http://www.mhakeystonecenter.org/icu_overview.htm.
12 Five key steps intended to promote adoption of recom-mended guidelines are: educate staff on the science of safety; complete a staff assessment of patient safety culture; a senior hospital executive partners with the unit to improve communications and educate leadership; staff learn from unit defects; and staff use tools, including checklists, to improve teamwork, communication, and other systems. For more information, see http://www.ahrq.gov/qual/cusp.htm.
13 H. R. Waters, R. Korn, Jr., E. Colantuoni et al., “The Business Case for Quality: Economic Analysis of the Michigan Keystone Patient Safety Program in ICUs,” American Journal of Medical Quality, Sept./Oct. 2011 26(5):333–39.
14 For more information about CUSP, see http://www.ahrq.gov/qual/cusp.htm.
15 For descriptions of the funded projects, see http://www.ahrq.gov/qual/haify10.htm.
16 See www.cdc.gov/HAI/prevent/prevention_tools.html; www.ihi.org/IHI/Topics/HealthcareAssociatedInfec-tions/InfectionsGeneral/; www.apic.org/AM/Template.cfm?Section=Education; www.whynotthebest.org.
17 Hospitals that do not submit the CLABSI data to NHSN are subject to a 2 percentage point reduction in their Medicare inpatient annual payment update for FY 2013.
18 Srinivasan, Wise, Bell et al., “Vital Signs,” 2011.
19 For more information about CAUTI prevention, see http://www.cdc.gov/hicpac/pdf/CAUTI/CAUTIguideline-2009final.pdf and http://www.cdc.gov/hicpac/CAUTI_fastFacts.html.
20 For more information about IHI’s work to prevent CAU-TIs, see http://www.ihi.org/IHI/Programs/AudioAndWeb-Programs/ExpeditionPreventingCatheterAssociatedUrin-aryTractInfectionsAug10.htm?player=wmp.
21 For more information about IHI’s “Ventilator Bundle, see http://www.ihi.org/IHI/Topics/CriticalCare/IntensiveC-are/Changes/ImplementtheVentilatorBundle.htm.
22 For more information about the CDC’s surgical site infection prevention guidelines, see http://www.cdc.gov/HAI/ssi/ssi.html and http://www.cdc.gov/hicpac/pdf/guidelines/SSI_1999.pdf.

14 the CoMMonwealth fund
Appendix. Purpose and Methodology for CLABSI Case Study Series
To better understand how some hospitals have succeeded in eliminating CLABSI in their ICUs, The Commonwealth Fund supported Health Management Associates in conducting an analysis of high-performing hospitals. This report synthesizes the findings and lessons from that analysis, which focused on four hospitals that experienced zero CLABSIs in their ICUs in 2009. The authors examined:
• how CLABSI prevention techniques were implemented and sustained;
• whether and how CLABSI prevention practices were extended beyond the ICU to other units and hospital floors;
• whether the infection prevention framework was extended to other health care–associated infections;
• what challenges hospitals faced in implementing and/or extending infection control interventions; and
• what organizational and cultural factors supported the successful adoption and continuation of best infection control practices.
To select the hospitals for study, the authors reviewed data made available to The Commonwealth Fund by a special arrangement with Consumer Reports Health, which integrated data from 15 states that require hospitals to report CLABSIs, and the Leapfrog Group, which collects infection data voluntarily reported by hospitals in 45 states. In all, the authors examined data from some 964 hospitals. These hospital-specific data are available on The Commonwealth Fund’s WhyNotTheBest.org Web site.
The authors selected four hospitals from approximately 100 with zero CLABSIs and a standardized infection ratio of zero in calendar year 2009. The standardized infection ratio (SIR) represents total reported infections divided by total predicted infections. For CLABSI data, a SIR of 1.0 indicates that a hospital is performing just as would be predicted from national rates. A SIR greater than 1.0 indicates the hospital had more infections than pre-dicted from national rates, and a SIR of less than 1.0 indicates it had fewer infections than predicted. Individual hos-pitals tend to report CLABSI rates (i.e., number of infections per 1,000 central line days), rather than SIRs.
The final selection was based on preferences for: hospitals with the highest number of central line days (indi-cating more opportunities for infections); those that are not well below average in mortality or readmission rates; and those with scores around the national average or better on measures of patient experiences and adherence to rec-ommended care processes for pneumonia, heart attack, heart failure, and surgery as reported on WhyNotTheBest.org. The selected hospitals also reflect a diversity of facilities, in terms of size and type of operating environment.
The authors gathered information through semistructured interviews (by telephone and through site visits) with key hospital leaders and staff knowledgeable about the hospital’s infection control methods and history, and through reviews of hospital data, reports, and other materials made available by the hospital or obtained through Internet searches.
This methodology has some limitations. First, it is based on self-reporting, with a mix of unaudited and audited data. There is variation in self-reported CLABSI data, which means the findings may overreport success. Second, other unmeasured factors may affect CLABSI rates. Third, the sample is small and it is inadvisable to gen-eralize to all hospitals based on such a small sample, or assume that hospitals in different circumstances have the capacity to adopt similar strategies. However, by synthesizing findings across the four hospitals and identifying common themes, challenges, innovations, and lessons, the authors offer other hospitals insights and options for reducing health care–associated infections.

eliMinating Central line infeCtionS and Spreading SuCCeSS at high-perforMing hoSpitalS: SyntheSiS report 15
about the authorS
Sharon Silow-Carroll, M.B.A., M.S.W., is a managing principal at Health Management Associates. She has more than 20 years of experience conducting research and analysis of local, state, and national health system reforms; strategies by hospitals to improve quality and patient-centered care; public–private partnerships to improve the performance of the health care system; and efforts to meet the needs of underserved populations. Prior to joining Health Management Associates, she was senior vice president at the Economic and Social Research Institute, where she directed and conducted policy analysis and authored reports and articles on a range of health care issues. Ms. Silow-Carroll earned a master of business administration degree at the Wharton School and a master of social work degree at the University of Pennsylvania.
Jennifer N. Edwards, Dr.P.H., M.H.S., is a managing principal with Health Management Associates’ New York City office. She has worked for 20 years as a researcher and policy analyst at the state and national levels to design, evaluate, and improve health care coverage programs for vulnerable populations. She worked for four years as senior program officer at The Commonwealth Fund, directing the State Innovations program and the Health in New York City program. Dr. Edwards has also worked in quality and patient safety at Memorial Sloan-Kettering Cancer Center, where she was instrumental in launching the hospital’s patient safety program. She earned a doctor of public health degree at the University of Michigan and a master of health science degree at Johns Hopkins University.
aCknowledgMentS
The authors thank Anne-Marie Audet, M.D., M.Sc., vice president for health systems improvement and effi-ciency at The Commonwealth Fund, for advice and guidance on the series, and the Fund’s communications team for assistance with editing and production.
They also thank the following individuals at the four case study sites who so generously shared their time, data, and insights about infection control efforts:
At Bronson Methodist Hospital: Cheryl Knapp, M.B.A., R.N., vice president of accreditations and quality standards; Gabriel Pedraza, M.D., adult critical care medical director; Carla Cook, R.N., B.S., nurse manager of the medical ICU; Richard Van Enk, Ph.D., director of infection prevention and epidemiology; and Wendy Douglas, B.S.N., R.N., VAST nurse.
At Englewood Hospital and Medical Center: Kathy Kaminsky, M.S., R.N., vice president, clinical effec-tiveness; Mary Curran, coordinator, clinical effectiveness; Lori Habersaat, GCM, quality specialist; Mary Ellen Walter, R.N., infection prevention coordinator; Sharon Roche, D.N.Sc., R.N., A.P.N., advanced practice nurse; Carmine Gianatiempo, M.D., director of critical care; and Aryeh Shander, M.D., chief of the department of anesthesiology, critical care, and hyperbaric medicine.
At Presbyterian Intercommunity Hospital: Judy Pugach, M.P.H., R.N., vice president of quality and risk management; and Helen Litvak, R.N., M.S.N., CIC infection preventionist.
At Southern Ohio Medical Center: Christine Aeh, R.N., director of patient safety, and Kathy Mullens, R.N., infection preventionist.
Editorial support was provided by Sarah Klein.

This study was based on publicly available information and self-reported data provided by the case study institution(s). The Commonwealth Fund is not an accreditor of health care organizations or systems, and the inclusion of an institution in the Fund’s case studies series is not an endorsement by the Fund for receipt of health care from the institution.
The aim of Commonwealth Fund–sponsored case studies of this type is to identify institutions that have achieved results indicating high performance in a particular area of interest, have undertaken innovations designed to reach higher performance, or exemplify attributes that can foster high performance. The studies are intended to enable other institutions to draw lessons from the studied institutions’ experience that will be helpful in their own efforts to become high performers. It is important to note, however, that even the best-performing organizations may fall short in some areas; doing well in one dimension of quality does not necessarily mean that the same level of quality will be achieved in other dimensions. Similarly, performance may vary from one year to the next. Thus, it is critical to adopt systematic approaches for improving quality and preventing harm to patients and staff.
Health Management Associates (HMA) is an independent health care research and consulting firm. In May 2010, HMA established a division, HMA Investment Services, to provide generalized information, analysis, and business consultation services to its clients, which principally include investment professionals. Neither HMA nor HMA Investment Services is a registered broker-dealer or investment adviser firm. Research and analysis prepared by HMA on behalf of The Commonwealth Fund is independent of and not influenced by personnel or clients of HMA Investment Services. In particular, the selection of subjects and content for HMA case studies published by The Commonwealth Fund is based solely on objective criteria and is in no way influenced by HMA Investment Services.





























