Embed Size (px)
Citation preview

INVITED REVIEW ABSTRACT: The cricopharyngeus (CP) is a striated muscle sphinctersituated at the pharyngoesophageal junction. The upper esophageal sphinc-ter is comprised of the striated CP muscle and nonmuscular components atthe level of the cricoid cartilage. This review describes the basic anatomyand physiology of the CP muscle, its central and peripheral relationship,methods of investigating it, and electrophysiological properties related todeglutition. The main function of the CP muscle is to control flow betweenthe pharynx and esophagus. The CP sphincter muscle is tonically contractedat rest and relaxes during swallowing, belching, and vomiting. Electromyo-graphy (EMG) of the CP sphincter muscle has been undertaken frequentlyin a variety of subhuman species with the aim of understanding deglutition,whereas it has seldom been reported in healthy human subjects and pa-tients. Increased knowledge of the physiology and anatomy of the humanCP sphincter muscle is not only important scientifically but is necessary foradvancing the diagnosis and treatment of oropharyngeal dysphagia, forwhich neurological causes are responsible in 80% of cases.
© 2002 Wiley Periodicals, Inc. Muscle Nerve 26: 729–739, 2002
ELECTROMYOGRAPHY OF HUMAN CRICOPHARYNGEALMUSCLE OF THE UPPER ESOPHAGEAL SPHINCTER
CUMHUR ERTEKIN, MD,1,2 and IBRAHIM AYDOGDU, MD 1,2
1 Department of Clinical Neurophysiology, Ege University, Medical School Hospital, Bornova, Izmir, Turkey2 Department of Neurology, Ege University, Medical School Hospital, Bornova, Izmir, Turkey
Accepted 29 July 2002
The cricopharyngeus (CP) is a striated musclesphincter situated at the pharyngoesophageal junc-tion. The upper esophageal sphincter (UES) is com-prised of the striated CP muscle and nonmuscularcomponents at the level of the cricoid cartilage. Themajor component of the UES is the CP muscle,which is attached to the lateral margins of the pos-terior aspect of the cricoid cartilage and encirclesthe lumen,19,47,48 though the inferior pharyngealconstrictor and striated muscles of the proximalesophagus may also contribute to the UES.4,48,71,76
The CP sphincter muscle is tonically active at restand relaxes during swallowing, belching, and vomit-
ing. Its main function is to control anterograde andretrograde flow of contents between the pharynxand esophagus.17,58,70,71,92
Several studies conducted on humans have indi-cated the importance of the CP muscle as part ofUES in deglutition, but these reports are mostlybased on data obtained by videofluoroscopy andmanometry.18,20,21,24,56,58,64,92,96 Following the impor-tant contribution of Doty and Bosma26 in 1956, elec-tromyography of the CP-sphincter muscle has beenstudied in a variety of subhuman species to under-stand deglutition.4,17,65,71,72,76,82,103 However, electro-myography (EMG) of the CP sphincter has seldombeen reported in healthy human subjects and pa-tients.29,41,54,95,99,101 Moreover, these human EMGstudies have mainly described the methodology orbasic aspects of the tonic EMG activity of the CPsphincter and its relaxation during swallowing.
CP MUSCLE FIBERS AND THEIR PERIPHERALINNERVATION
The CP muscle was first described by Valsalva in 1717(cited by Calcaterra et al.16). Its existence as a dis-crete muscle was the subject of controversy until thelast decades of the 20th century.16 Anatomically, the
Abbreviations: ALS, amyotrophic lateral sclerosis; CP, cricopharyngeus;CP-EMG, cricopharyngeal muscle electromyography; CPG, central patterngenerator; EMG, electromyography; NA, nucleus ambiguus; NTS, nucleustractus solitarius; PP, pharyngeal plexus; RLN, recurrent laryngeal nerve;SLN, superior laryngeal nerve; TMS, transcranial magnetic stimulation; UES,upper esophageal sphincterKey words: cricopharyngeal muscle, upper esophageal sphincter, degluti-tion, dysphagia, electromyographyCorrespondence to: C. Ertekin, Gonc Apt. Talatpasa, Bulvarı, No. 12 D.3,35220, Alsancak, Izmir, Turkey; e-mail: [email protected]; [email protected]
© 2002 Wiley Periodicals, Inc.
Cricopharyngeal Sphincter Muscle MUSCLE & NERVE December 2002 729

CP muscle is located at the pharyngoesophagealjunction and consists of the upper oblique (parsobliqua) and lower horizontal parts (pars fundifor-mis). The CP muscle attaches to the cricoid cartilageand forms a C-shaped muscular band (Fig. 1A). It ismost likely that the concentric needle electrode isinserted into the lower horizontal part of CP muscleduring the percutaneous approach. In fact, the term“cricopharyngeus” applies to the horizontal fibers ofCP; the oblique fibers (pars obliqua) of the crico-pharyngeal and thyroglossal muscles together arecalled the “inferior pharyngeal constrictor” by someauthors.16,47 Thus, although the pars obliqua andpars fundiformis are, by definition, cricopharyngealmuscles, radiologists and clinicians generally referonly to the pars fundiformis as the CP muscle.23,25,48
The vertical extent of the CP muscle (horizontalfibers) is approximately 0.7 cm.13 The width of theCP muscle varies from about 1 to 2 cm.31,80 The parsfundiformis of the CP muscle has no median ra-phe15,70 and forms a sling of muscle which blendwith the circular muscle layers of the proximalesophagus15 (Fig. 1A).
Compared to the limb striated muscles, the CPhas abundant connective tissue particularly made upof elastic elements and smaller diameter muscle fi-bers of about 10–40 �m.13,15,69 Such structural prop-erties as well as the network arrangement of musclefibers and connective tissue could account for thepassive elastic behavior of the CP muscle. In humanstudies, the predominant CP muscle fiber type isreported to be type I (slow-twitch) and highly oxida-tive. It also contains type II (fast-twitch) muscle fi-bers, which are relatively fewer and glycolytic.13,15The fiber type proportions and fiber sizes in CPmuscle do not vary significantly with age or gen-der. The composition of CP muscle, mostly type Iwith fewer type II fibers, correlates with the func-tions of sustained tonicity to prevent aerophagiaand occasional forceful contraction during deglu-tition.13,15 There are two other important featuresof the CP muscle. First, it may contain fusiformmuscle fibers which, rather than extendingthroughout the entire length of the muscle, insertinto a connective tissue framework.15 Second, mus-cle spindles are absent.13
The distribution and organization of the motorend-plate of the CP muscle have recently been inves-tigated.80 The horizontal portion of the CP musclehas a single motor end-plate band that is located 1cm distal from the insertional end of the muscle oneach side. In the center of the horizontal portion ofthe CP muscle, a number of tiny motor end-platesappear to be distributed randomly.80 The new datamay be important for the injection of botulinumtoxin into the CP muscle in some swallowing disor-ders.
Innervation of the CP muscle has been a subjectof much controversy. The following nerves havebeen proposed: (1) Most investigators describe aninnervation network of small-diameter nerve fibersconsisting of the pharyngeal plexus (PP) of the vagusnerve in humans.14,80,81,89 (2) Branches of the recur-rent laryngeal nerve (RLN) may innervate the CPmuscle.14,52,80,81,89,98 (3) The terminal external divi-sion of superior laryngeal nerve (SLN) may alsosupply the CP muscle,80,89 but Sasaki et al.89 did notfind any proof for such innervation. (4) Sympatheticmotor control of the CP muscle is controversial. Thepossible role of cervical sympathetic nerve fibers has
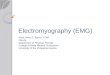
FIGURE 1. (A) EMG recording method for the CP sphincter(CP-EMG) and submental muscles (SM-EMG); their relations toadjacent structures are shown schematically. (B) EMG activitiesof the submental muscle (SM-EMG) and cricopharyngeal muscle(CP-EMG) while 3 ml water are swallowed. During rest, there wascontinuously high-frequency tonic EMG activity in the CP muscle(third trace). During swallowing, SM-EMG activity began first andthe tonic EMG activity of the CP muscle was switched off (pause)(first and second traces). Amplitude calibration: SM-EMG, 30 �V;CP-EMG, 30 and 50 �V, respectively. Time calibration: all traces,200 ms.
730 Cricopharyngeal Sphincter Muscle MUSCLE & NERVE December 2002

been discussed based on findings in animal stud-ies,67,82,98 but the absence of sympathetic innervationhas recently been shown in humans.89
Consensus is forming that the CP muscle has adual innervation by the PP of the vagus nerve andthe RLN.14,80,89 The RLN projects to the anteriormotor units located in the anterior segments of thehorizontal part of the muscle, whereas the PPprojects to the posterior motor units of the muscle.89
Experimentally, it appears that rapid, large-am-plitude CP electromyographic (EMG) responses areobtained by stimulation of the RLN, and another setof slower nerve fibers of different origin (probablysome PP nerve fibers) mediate the slower-rate, low-amplitude CP responses. Thus, the RLN may facili-tate a rapid closure of the proximal esophagus andrapid elevation and shortening of the pharynx,which allows the laryngeal area to be protected frominfiltration by the bolus.52
The CP muscle and its innervation are organizedas two separate muscles. Although there may be nowell-defined raphe in the CP, there is most likely aphysiological separation of the right and left CP.76The muscle fibers of CP are short and not organizedin a parallel fashion.13,15,69 Therefore, individual CPmuscle fibers do not cross the midline to any greatextent or length.76 Injection of horseradish peroxi-dase into the CP muscle or nerves supplying it in catsand rabbits have demonstrated projections primarilyto the ipsilateral nucleus ambiguus (NA),49,68 andbrainstem electrical stimulation primarily activatedthe ipsilateral CP in dogs.102
Thus, the CP muscle and its innervation are func-tionally organized into two separate muscles withindependent innervation in mammals. This must beconsidered when myotomy is to be performed orbotulinum toxin injected into the CP muscle for thetreatment of dysphagia.
CP MUSCLE MOTONEURONS INMEDULLA OBLONGATA
The motor neurons controlling the CP are foundprimarily within the semicompact and rostral com-pact portions of the NA, and innervation is mostly(�95%) ipsilateral.11,55,68,70,78,79 The CP motoneu-rons are topographically organized with the motorneurons to the other muscles of the pharynx andesophagus, although there is considerable over-lap.11,68,70 The neurons of the NA have extensivedendritic arborization to the adjacent reticular for-mation.2 Ultrastructural and physiological studies in-dicate that the synapses on these neurons are bothexcitatory and inhibitory.53
The motoneurons of the rostral NA have beenidentified by their intracellular activity in sheep dur-ing swallowing. Among these motoneurons, somehad hyperpolarization and depolarization with verylong latencies and durations. They projected to ei-ther the superior esophageal sphincter (i.e., CP mus-cle) or the cervical esophagus. These electrical se-quences were correlated with relaxation of theupper esophageal sphincter or cessation of tonicactivity, and followed an EMG burst during swallow-ing.105 This sequence of EMG activity of the CPsphincter is similar to that in humans.41 The clinicalelectrophysiology of oropharyngeal swallowing andthe EMG activity of the CP muscle indicate the im-portance of the sequential inhibitory and excitatoryactivities of motoneurons (Fig. 1B).
Experimental studies have identified two ana-tomical regions within the medulla oblongata con-cerned with swallowing activity: a dorsal region con-sisting of the neurons within and around the nucleusof the solitary tract (NTS), and a ventral regioncorresponding to the reticular formation surround-ing the NA.59,60,62,66 These two regions representedon both sides of the brain stem are interconnectedextensively so that either side can coordinate thepharyngeal and esophageal phases of swallow-ing.10,27,103,104 Their extensive connections and thereticular network are important for the performanceof oropharyngeal swallowing and certain other re-flex functions.
The anatomophysiological network mentionedabove has been designated the “central pattern gen-erator” of swallowing.78,79 When it is triggered, “se-quential muscle activity” begins in an orderly fashionfrom facial- and trigeminal-innervated muscles to theCP sphincter muscle and striated esophageal mus-cles. There are about 33 paired muscles that areinnervated from the 5 paired cranial motor nerves,i.e., trigeminal, facial, glossopharyngeal, vagus, andhypoglossal nerves.25 The CP motoneurons and theirinnervation in and around the NA are part of thisspecific network, and their activity changes with theswallowing events at the periphery. They may also becontrolled by the motor cortex and other supraspi-nal centers.
Normally, the sensory receptors in the oropha-ryngeal mucosa are involved in the initiation of vol-untary or reflex (spontaneous) swallowing. Theysend information about the size and content of thebolus to be swallowed to both the motor cortex andsuprasegmental centers, as well as to the premotorneurons of the NA and NTS.39,40
Cricopharyngeal Sphincter Muscle MUSCLE & NERVE December 2002 731

DESCENDING CONTROL OF THE CP MUSCLE
Three regions of the cerebral cortex appear to beimportant: the premotor cortex anterior to the mo-tor cortex (Brodmann’s area 6), the precentral mo-tor cortex (area 4 or M1), and the anterior insula.Thus, the inferior and posterior regions of the pri-mary motor cortex and the regions of the supple-mentary motor cortex must be intact for normalswallowing and CP sphincter muscle func-tion.22,74,78,79 Studies involving transcranial magneticstimulation (TMS) of the human motor cortex sug-gest that the lower precentral and posterior inferiorfrontal gyri induce contractions in the oral-phasemuscles, whereas the anterior inferior and middlefrontal gyri induce contractions in pharyngeal andesophageal striated muscles.6,50 The muscles in-volved in human swallowing function, including theproximal esophageal striated muscles, are repre-sented bilaterally in the motor cortex.7,8,50 Indeed,volitional swallowing in humans has multiregionalrepresentation especially within the sensorimotorcortex and cerebellum.51 Motor evoked potentialscan be elicited from the CP muscle by cortical mag-netic stimulation and by vagus nerve stimulationproximally at the suboccipital level. The central mo-tor delay suggests an oligosynaptic corticobulbarpathway to the motoneurons of the CP muscles (Fig.2). The topography of cortical stimulation suggeststhat the CP muscle is also bilaterally represented inthe motor cortex.42 Transcranial magnetic stimula-tion probably excites the corticobulbar fibers. Thetotal cortical effect on the CP sphincter is both ex-citatory and inhibitory, but the main function of thecerebral cortex in normal swallowing is to triggeroropharyngeal swallowing.33,36,38,42 Involvement ofthe inhibitory corticobulbar fibers results in disinhi-bition of the CP sphincter, as can be demonstratedelectrophysiologically.34,36,37 Subcortical regions in-cluding the limbic system, basal ganglia, upper brainstem, and cerebellum may have a role in oropharyn-geal swallowing and may, therefore, influence theCP sphincter EMG. However, precise anatomophysi-ological relationships remain to be clarified.
CP SPHINCTER EMG AT REST AND DURINGSWALLOWING
Recording Methods. There are two main ap-proaches to recording the CP muscle: the percuta-neous and intraluminal approaches. In the percuta-neous approach, a concentric needle electrode ispassed through the skin in a posterior and medialdirection at the level of, and just lateral to, the
cricoid cartilage. The point of insertion is about 1.5cm lateral to the palpable lateral border of the cri-coid cartilage (Fig. 3A).
The needle electrode should be inserted whilethe subject is in recumbent position, with the headtilted posteriorly, in order to prevent the rare possi-bility of arterial hypotension or syncope. After a fewminutes, the recording can be commenced. At anytime during this process, if cough occurs or thepatient experiences an unpleasant feeling or pain,the needle electrode should immediately be re-moved. The procedure has not caused any majorcomplications or complaints in our experience withover 150 normal subjects and patients. In a fewsubjects, a small subcutaneous hematoma occurred.
High-frequency, tonic EMG activity appears onthe oscilloscope screen and a continuous high-fre-quency sound is emitted from the loudspeaker, asthe needle electrode tip penetrates the CP muscle.During attempted swallowing, this tonic EMG activitydisappears for a short time (400–600 ms). Thispause in EMG activity during a swallow, and theincrease in tonic activity that often occurs prior toand always occurs following this pause, serves as themark for correct electrode entry into the CP mus-cle.37,38,41 The EMG signal can be conveniently re-corded or bandpass filtered (between 100 Hz and 10
FIGURE 2. Motor evoked potentials of the CP muscle obtainedfrom a normal subject. (A) Magnetic stimulation was applied overthe vertex around the Cz electrode position (cortical stimulation).(B) The parietooccipital skull region ipsilateral to the recordingsite was stimulated (peripheral stimulation). Note the differenttime base for (A) and (B). In each trace, two responses weresuperimposed. Amplitude calibration: upper trace, 100 �V; lowertrace, 1 mV. Time calibration: 5 and 2 ms, respectively. (FromErtekin et al.,42 by permission.)
732 Cricopharyngeal Sphincter Muscle MUSCLE & NERVE December 2002

kHz), rectified, integrated, and averaged during dy-namic swallowing studies (Fig. 3B). The needle tiprecords activity of the most lateral part of pars fun-diformis of the CP sphincter muscle. Sometimes, it isdifficult to reach the CP muscle, especially in obese,elderly, and short-necked persons. The depth of en-try of the concentric needle into the CP muscle isabout 2–4 cm from the skin in most people, but adeeper approach is sometimes necessary. The nee-dle tip can be introduced unintentionally into neigh-boring muscles, in which case the swallowing patternwith the EMG pause is not obtained. Sometimes the
laryngeal muscles are penetrated accidentally. In thiscase, the EMG activity is mainly increased by phona-tion or forced breathing.
A hook-wire electrode can also be used instead ofthe concentric needle electrode.86,87 Its positioningis more complicated, however, owing to two factors.First, it is more difficult to monitor the EMG associ-ated with placing the wire electrodes due to electri-cal noise and motion artifact. Second, the wire elec-trode position cannot be adjusted after initialplacement without unbending the hooks.86,87
An intraluminar approach to the CP muscle hasbeen mostly used in the past. Wire electrodes areintroduced with the aid of a specially designed in-strument or catheter through a rigid esophagoscopeof about 25 cm, and the instrument is then with-drawn, leaving the wires fixed in the CP muscles bytheir hooked ends. The wire electrodes can be intro-duced by an endoscopic procedure under generalanesthesia.101 Similar intraluminar approaches havebeen performed during oropharyngeal opera-tions.14,81,89
The pharyngeal constrictor muscles and crico-pharyngeus muscle have been investigated by bipo-lar suction electrodes. In this approach, a suctionelectrode applied to the posterior pharyngeal wall isheld in a constant, stable relationship with the un-derlying constrictor muscles. Topical anesthesia hasto be applied to the nasal and pharyngeal mucosa,and the bipolar suction electrodes are insertedthrough the nose, advanced to the pharynx, andbrought into contact with the mucosa using trans-oral forceps; suction is then applied with a syringeattached to the suction tube.83,84
Tonic and Phasic Activity of CP Sphincter. The CPsphincter muscle is tonically active during rest, and thiscontinuous activity ceases during a swallow in humansubjects (Figs. 1B and 3B). Numerous studies showingsuch findings have been performed in mam-mals,4,17,26,58,65,71 including humans.29,30,54,95,99,101 Inmost studies, the test subjects (either human or ani-mal) were maintained in a fixed posture by anesthesia,restraint, or verbal instruction, and this might accountfor the observed constant basal level of tonic CP activ-ity. The EMG activity of the CP and upper esophagealsphincter increased and decreased spontaneously, andcould be altered substantially either by arousal or bychanging posture.71 Thus, the CP muscle maintained acontinuous but varying basal tone, which depended onenvironmental conditions.
It can be assumed that the central nervous systemmechanisms generating sphincter tone adjust reflexlyto environmental stimuli and do not maintain a con-
FIGURE 3. (A) Application of the electrode positions for swallow-ing study. For the CP-EMG, the concentric needle electrode ispositioned in the CP muscle (needle in the left side). For record-ing submental EMG activity, surface electrodes are taped underthe chin. For recording the laryngeal movement, a piezoelectricmovement sensor is placed between the thyroid and cricothyroidcartilages at the midline. (B) Laryngeal sensor signals and con-ventional and integrated EMG activities of the cricopharyngealmuscle (CP-EMG) while swallowing 3 ml water. With the superiorrelocation of the larynx, tonic activity of the CP-EMG ceased andthe CP-EMG pause occurred. After the CP-EMG pause, bursts ofincreased EMG activity of the CP sphincter are clearly seen in theCP-EMG traces. First laryngeal sensor signal denotes upwardand later downward deflections of the larynx. Amplitude calibra-tion: CP-EMG, 50, 50, and 30 �V, respectively (amplitude oflaryngeal sensor signal is unimportant). Time calibration: alltraces, 200 ms.
Cricopharyngeal Sphincter Muscle MUSCLE & NERVE December 2002 733

stant output.48,63,71,93 Indeed, numerous reflexes con-tribute to the tonic activity of the CP muscle. Forinstance, bolus distension of the proximal esophaguscauses increased CP tonic activity mediated by vagalafferent fibers.17,32,45,77 Pharyngeal stimulation is foundto cause an increase in upper esophageal sphinctertone9,88 and cricopharyngeal muscle electromyo-graphic (CP-EMG) activity.70,77 These reflexes prob-ably help to close the esophagus during inspirationto prevent aerophagia or aspiration.70 UES pressureand tonic activity of the CP sphincter fluctuate withrespiration, but may be in or out of phase withinspiration and may be associated with contractionof the CP muscle.57,65,70,71 Some of the activity of theUES or CP muscle may be generated by variousreflexes and related to specific brainstem circuitry.70
Two groups of motor units exist in the human CPmuscle. Small motor units are continuously discharg-ing during rest, and larger motor units are recruitedjust before and after the CP-EMG pause during swal-lowing (Fig. 4). These EMG findings are consistent
with the histopathological findings in CP muscle oftwo groups of muscle fibers, i.e., type I oxidativefibers (the majority) and type II glycolytic musclefibers.13,15 Such histochemical and morphometriccharacteristics of the human CP muscle are clearlyadaptable to the physiological features of the twotypes of motor units, i.e., small motor units contin-uously discharging during rest and large motor unitsdischarging transiently just before and after degluti-tion.
During resting, the tonic EMG activity of CPmuscle is such that the motor unit potentials aresmall and range from 1–10 ms in duration (mean:4.9 ms) and between 50 and 120 �V in amplitude(Fig. 4A). They are bi- or triphasic and rarelypolyphasic. It is difficult to determine the dischargefrequency for a given motor unit due to technicaland physiological factors.
During wet or dry swallowing, two bursts of in-creased EMG activity are clearly observed just beforeand after the CP-EMG pause. The motor units in therebound burst are large biphasic or triphasic motorunit potentials with duration of 4–12 ms (mean: 7.4ms) and amplitudes that range within 80–1,900 �V(Fig. 4C). Similar large motor unit action potentialsmay also be recorded in the initial burst (Fig. 4B).
The foreburst and rebound burst accompanyingthe swallowing pause of the CP sphincter are pre-sumably related to the deglutition process but thereare no satisfactory explanations or studies on theseactivity bursts. We suggest that the foreburst is a kindof protective reflex strictly related to oropharyngealfunction and does not necessarily take part in thesequential muscle activity of deglutition, whereas therebound activity is an electrical event that is strictlybounded by the sequential muscle activity of thecentral pattern generator. The foreburst was re-corded in 69% of 39 normal subjects, in contrast tothe rebound burst which was recorded in all subjects(Table 1). Even in normal subjects in whom theforeburst is recorded during swallowing, a foreburstdoes not necessarily appear in each swallowing
FIGURE 4. The motor units potentials of the CP sphincter muscleduring resting tonic activity (A), foreburst activity (B), and re-bound burst activity (C). Note the increase in duration, amplitude,and frequency of the motor units during foreburst and reboundburst before and after the CP-EMG pause recorded from a win-dow as demonstrated in the uppermost trace. Amplitude calibra-tion: 200 �V. Time calibration: top trace, 200 ms; other traces, 8ms.
Table 1. Incidence of CP-EMG properties encountered in 39normal subjects during wet swallowing.
PropertiesNo. of cases
(%)
CP-EMG pause 39 (100)Rebound burst 39 (100)Foreburst 27 (69)Two stages of CP-EMG pause 14 (36)Forepause 7 (18)
CP-EMG, cricopharyngeal muscle electromyogram.
734 Cricopharyngeal Sphincter Muscle MUSCLE & NERVE December 2002

event. It is usually absent in semisolid or dry swallow-ing. Similar reflex responses are observed in theEMG of the laryngeal adductor muscles during swal-lowing as an oral-laryngeal reflex preceding the con-stant excitation of laryngeal adductors for closure ofthe larynx.38
During a swallow, tonic motoneurons supplyingthe CP muscle are first inhibited and the CP sphinc-ter is relaxed. Consequently, during the reboundburst, phasic larger motoneurons fire transiently toclose the sphincter as fast as possible after the pas-sage of the bolus, and the tonic motoneurons arere-excited. Although both tonic and phasic motorunits are under the control of the central patterngenerator (CPG), both are also influenced by sen-sory and cortical inputs. The corticobulbar systemprobably acts as a tonic inhibitor of the CP sphinctermotoneurons, as the CP-EMG pause is shortenedwith an unexpected burst of motor units within it,and prematurely closed, in some disorders with cor-ticobulbar involvement, such as amyotrophic lateralsclerosis and suprabulbar palsy with multiple lacunarinfarcts.34,36
Pause in CP Sphincter EMG Activity During Swallowing.
During wet and dry swallowing, the CP-EMG pausesometimes shows two stages: in the first part of thepause, the bioelectrical silence is obvious and poten-tials higher than 20 �V are never observed except formechanical artifacts due to the vertical motion ofdeglutition. This volume-conducted artifact can beeliminated with the low-pass filter in the EMG systemwhen necessary. In the later part of the pause, somesmall motor unit potentials exceeding 20 �V can beseen. This EMG activity eventually increases in am-plitude toward the onset of the rebound burst. Thesetwo stages can be termed the absolute and relativeCP-EMG pause (Fig. 5). The absolute period, whenvirtually no activity is encountered, occurs within thefirst 100–200 ms and covers about 40% of CP-EMGpause in wet swallowing. The relative period, whichfollows, constitutes over 50% of the total pause inwet swallowing. These two stages are recorded inonly about 36% of normal subjects (Table 1);complete silence during CP-EMG pause is recordedin most subjects. They have not been described be-fore. Some manometric studies have shown that dur-ing the relaxation period of the UES, immediatelybefore the arrival of the bolus, a negative (subatmo-spheric) pressure is generated in the pharyngoesoph-ageal segment during laryngeal elevation.20,26,46,58,75
In about 18% of normal subjects, an earlier sup-pression of tonic EMG activity, just before the initialburst of EMG activity in CP, was encountered during
swallowing (Table 1). This so-called forepause ischaracterized by a reduction in amplitude and fre-quency of tonic activity that always appears beforethe onset of submental muscle activity, which is thefirst and stable event for the swallowing, and alsobefore the onset of the upward deflection of thelarynx in the swallowing reflex.
Role of CP Sphincter EMG in Patients with Neurogenic
Dysphagia. After clinical examination, the evalua-tion of dysphagia may require videofluoroscopic,manometric, and endoscopic studies. These meth-ods display the “mechanical results of the end organfunction” of the oropharynx. They do not providefurther information about the striated muscles of theoropharynx, including the CP muscle, or about theprecise timing of activation among the differentmuscle groups involving in swallowing in response tothe central pattern generator of the brain stem.61,79Therefore, EMG methods have an important role inthe evaluation of neurogenic dysphagia.33,41
Swallowing abnormalities may results from le-sions involving sites anywhere along the pathwayfrom the cerebral cortex to the striated muscle of theoropharynx. Neurological disorders account for 75–80% of all patients with swallowing problems.91,97,100
“Hyperreflexic CP” is a type of EMG abnormalityof the CP sphincter mostly encountered in amyotro-phic lateral sclerosis (ALS),36 suprabulbar palsy with
FIGURE 5. Laryngeal sensor signals and EMG activities of thecricopharyngeal muscle (CP-EMG) during swallowing of 3 mlwater. Two stages of the CP-EMG pause (absolute and relative)are shown with conventional and integrated/averaged CP-EMGtraces. There was almost complete bioelectrical silence duringthe first part of the pause (absolute period), but in the later part ofthe pause (relative period), small motor unit potentials are seen.First laryngeal sensor signal denotes upward and later downwarddeflections of the larynx. Amplitude calibration: EMG traces, 50and 30 �V. Time calibration: all traces, 200 ms.
Cricopharyngeal Sphincter Muscle MUSCLE & NERVE December 2002 735

lacunar infarct,34 and craniocervical dystonia.37 Thefindings characterizing a hyperreflexic CP sphincterare shortening of the CP-EMG pause (�300 ms),premature closure before the descending movementof the larynx, and unexpected EMG bursts duringthe CP-EMG pause (Fig. 6). However, the motorneurons and the motor units of the CP muscle seemto be normal in most neuromuscular disorders in-cluding myasthenia gravis,43 polymyositis (in somepatients), ALS, and some lower cranial nerve disor-ders with dysphagia. The rarity of lower motor neu-ron involvement of the CP muscle may be specula-tively attributed to multiple innervation or relate toother, as yet unknown, factors.
Some myopathic changes in the motor unit po-tentials of the CP muscle, and shortening or length-ening of the CP-EMG pause, have been observed insome patients with polymyositis.33,37 Myopathic mo-tor unit potentials may also be encountered in theCP muscle in myotonic dystrophy, and the EMGpause during swallowing may be variable due tomyotonia or spasms.44 The striated muscle disorderscan be evaluated simply by noninvasive “single bolusanalysis”37,41,43 and “dysphagia limit” methods,35 un-less otherwise necessary.
More recently, it has been found that injectionsof botulinum toxin A into the hyperreflexic CP mus-cle can be a treatment of choice for dysphagic pa-tients.1,3,5,12,28,85,90 However, most patients were in-jected with the botulinum toxin by means ofendoscopic techniques under anesthesia. For theseinvasive methods, either EMG-guided injection un-der videofluoroscopy or CT-guided injections wereused.90,94 Blitzer and Brin12 used EMG-guided per-cutaneous injection of botulinum toxin into the CPmuscle. As the motor end-plate band is located 1 cmdistal from the insertional end of the muscle on eachside,80 percutaneous injections may, in fact, be betterfor administering this treatment. Moreover, it is dif-ficult to accurately place the injection during endos-copy and anesthesia, because the CP muscle is hid-den behind the cricoid cartilage,73 and anesthesiaand sleeping have a negative effect on the tonic andphasic activity of the CP muscle.54,70,71 Before apply-ing any treatment to the CP sphincter, includingmyotomy and botulinum toxin injection, the EMG ofthis muscle should be carefully evaluated togetherwith other aspects of the physiology of oropharyn-geal deglutition. Inaccurate injection may cause pa-ralysis of other muscles in the area, resulting in moresevere dysphagia.
This study was supported by a grant from the Turkish Scientificand Technological Research Council (TUBITAK) Project No.SBAG-1739. We are grateful for the cooperation of our coworkers,especially Murat Pehlivan, MD, Nur Yuceyar, MD, Nefati Kiylioglu,MD, Sultan Tarlaci, MD, and Yaprak Secil, MD. We also thankMrs. Sahire Erturan and Nilufer Ertekin-Taner, MD, PhD, whoreviewed the English text.
REFERENCES
1. Alberty J, Oelerich M, Ludwig K, Hartman S, Stoll W. Efficacyof botulinum toxin A for treatment of upper esophagealsphincter dysfunction. Laryngoscope 2000;110:1151–1156.
2. Altschuler AM, Bao X, Miselis RR. Dendritic architecture ofnucleus ambiguus motoneurons projecting to the upperalimentary tract in the rat. J Comp Neurol 1991;309:402–414.
3. Ashan SF, Meleca RJ, Dworkin JP. Botulinum toxin injectionof the cricopharyngeal muscle for the treatment of dyspha-gia. Otolaryngol Head Neck Surg 2000;122:691–695.
4. Asoh R, Goyal RK. Manometry and electromyography of theupper esophageal spincter in the opposum. Gastroenterol-ogy 1978;74:514–520.
5. Atkinson SI, Rees J. Botulinum toxin for cricopharyngealdysphagia: case report of CT-guided injection. J Otolarnyn-gol 1997;26:273–276.
6. Aziz Q, Rothwell JC, Hobson A, Alani S, Bancewicz J, Thomp-son DG. Esophageal myoelectric responses to magnetic stim-ulation of the human cortex and the extra-cranial vagusnerve. Am J Physiol 1994;267:G827–G835.
7. Aziz Q, Rothwell JC, Barlow J, Thompson DG. Modulation ofoesophageal responses to magnetoelectric stimulation of hu-man brain by swallowing and by vagal stimulation. Gastroen-terology 1995;109:1437–1445.
FIGURE 6. Laryngeal sensor signal and CP-EMGs recorded froman amyotrophic lateral sclerosis (ALS) patient with dysphagiaduring swallowing. The duration of the CP-EMG pause is shorterand CP-EMG pause ends prematurely before the larynx de-scends from its superior position [oblique arrow in (A)]. Theunexpected burst of motor unit action potentials (MUAP) duringthe swallowing pause of cricopharyngeal muscle is clearly seen[arrow in (B)]. [Averaged EMG trace is rectified and integrated in(A) . EMG trace is obtained from conventional EMG recordings in(B)]. First laryngeal sensor signal denotes upward and laterdownward deflections of the larynx. Amplitude calibration: CP-EMG traces, 30 and 50 �V, respectively. Time calibration: alltraces, 200 ms.
736 Cricopharyngeal Sphincter Muscle MUSCLE & NERVE December 2002

8. Aziz Q, Rothwell JC, Hamdy S, Barlow J, Thompson DG. Thetopographic representation of esophageal motor functionon the human cerebral cortex. Gastroenterology 1996;111:855–862.
9. Bardan E, Saesian K, Xie P, Ren J, Kern M, Dua K, Shaker R.Effect of pharyngeal stimulation on the motor function ofthe esophagus and its sphincter. Laryngoscope 1999;109:437–441.
10. Barrett RT, Bao X, Miselis RR, Altschuler AM. Brain stemlocalization of rodent esophageal premotor neurons re-vealed by transneural passage of pseudo-rabies virus. Gastro-enterology 1994;107:728–737.
11. Bieger D, Hopkins DA. Viscerotopic representation of theupper alimentary tract in the medulla oblongata in the rat:the nucleus ambiguus. J Comp Neurol 1987;262:546–562.
12. Blitzer A, Brin MF. Use of botulinum toxin for diagnosis andmanagement of cricopharyngeal achalasia. OtolaryngolHead Neck Surg 1997;116:328–330.
13. Bonington A, Mahon M, Whitmore I. A histological andhistochemical study of the cricopharyngeus muscle in man.J Anat 1988;156:27–37.
14. Brok HAJ, Copper MP, Stroeve RJ, Ongerboer de Visser BW,Venker-van Haagen AJ, Schouwenburg PF. Evidence for re-current laryngeal nerve contribution in motor innervation ofthe human cricopharyngeal muscle. Laryngoscope 1999;109:705–708.
15. Brownlow H, Whitmore I, Willan PLT. A quantitative studyof the histochemical and morphometric characteristics ofthe human cricopharyngeus muscle. J Anat 1989;166:67–75.
16. Calcaterra TC, Kandell BM, Ward PH. Dysphagia secondaryto cricophayngeal muscle disorders—surgical management.Arch Otolaryngol 1975;101:726–729.
17. Car A, Roman C. L’activite spontanee du sphincter oesoph-agien superieur chez le mouton. J Physiol (Paris) 1970;62:505–511.
18. Castell JA, Castell DO. Modern solid state computerizedmanometry of the pharyngo-esophageal segment. Dysphagia1993;8:270–275.
19. Cook IJ. Cricopharyngeal function and dysfunction. Dyspha-gia 1993;8:244–251.
20. Cook IJ, Dodds WJ, Dantas RO, Massey B, Kern MK, LangIM, BrasseurJG, Hogan WJ. Opening mechanism of the hu-man upper esophageal sphincter. Am J Physiol 1989;257:G748–G759.
21. Curtis DJ, Cruess DF, Dachman AH, Maso E. Timing in thenormal pharyngeal swallow: prospective selection and eval-uation of 16 normal asymptomatic patients. Invest Radiol1984;19:523–529.
22. Daniels SK, Foundas AL. The role of the insular cortex indysphagia. Dysphagia 1997;12:146–156.
23. Dantas RO, Kern MK, Massey BT, Dodds WJ, Kahrilas PJ,Brasseur JG, Cook IJ, Lang IM. Effect of swallowed bolusvariables on oral and pharyngeal phases of swallowing. Am JPhysiol 1990;258:G675–G681.
24. Dodds WJ, Hogan WJ, Lydon SB, Stewart ET, Steg JJ, Arn-dorfer RC. Quantitation of pharyngeal motor fuction innormal human subjects. J Appl Physiol 1975;39:692–696.
25. Donner MW, Bosma JF, Robertson DL. Anatomy and physi-ology of the pharynx. Gastrointest Radiol 1985;10:196–212.
26. Doty RW, Bosma JF. An electromyographic analysis of reflexdeglutition. J Neurophysiol 1956:19:44–60.
27. Doty RW, Richmond WH, Storey AT. Effect of medullarylesions on coordination of deglutition. Exp Neurol 1967;17:91–106.
28. Dunne J, Hayes M, Cameron D. Botulinum toxin A forcricopharyngeal dystonia. Lancet 1993;342:559.
29. Elidan J, Shochina M, Gonen B, Gay I. Electromyography ofthe inferior constrictor and cricopharyngeal muscles duringswallowing. Ann Otol Rhinol Laryngol 1990;99:466–469.
30. Elidan J, Scochina M, Gonen B, Gay I. Manometric andelectromyography of the pharyngeal muscles in patients withdysphagia. Arch Otolaryngol Head Neck Surg 1990;116:910–913.
31. Ellis FH. Upper esophageal spfincter in health and disease.Surg Clin North Am 1971;51:553–565.
32. Enzmann DR, Harell GS, Zboralske FF. Upper esophagealresponses to intraluminal distention in man. Gastroenterol-ogy 1977;72:1292–1298.
33. Ertekin C, Palmer JB. Physiology and electromyography ofswallowing and its disorders. In: Ambler Z, Nevsimalova S,Kadanka Z, Rossini PM, editors. Clinical neurophysiology atthe beginning of the 21st century. Amsterdam: Elsevier;2000. p148–154.
34. Ertekin C, Aydogdu I, Tarlaci S, Turman AB, Kiylioglu N.Mechanism of dysphagia in suprabulbar palsy with lacunarinfarct. Stroke 2000;31:1370–1376.
35. Ertekin C, Aydogdu I, Yuceyar N. Piecemeal deglutition anddysphagia limit in normal subjects and in patients with swal-lowing disorders. J Neurol Neurosurg Psychiatry 1996;61:491–496.
36. Ertekin C, Aydogdu I, Yuceyar N, Kiylioglu N, Tarlaci S,Uludag B. Pathological mechanisms of oropharyngeal dys-phagia in amyotrophic lateral sclerosis. Brain 2000;123:125–140.
37. Ertekin C, Aydogdu I, Yuceyar N, Tarlaci S, Kiylioglu N,Pehlivan M. Electrodiagnostic methods for neurogenic dys-phagia. Electroencephalogr Clin Neurophysiol 1998;109:331–340.
38. Ertekin C, Celik M, Secil Y, Tarlaci S, Kiylioglu N, AydogduI. The electromyographic behavior of the thyroarytenoidmuscle during swallowing. J Clin Gastroenterol 2000;30:274–280.
39. Ertekin C, Kıylıoglu N, Tarlaci S, Keskin A, Aydogdu I. Effectof mucosal anesthesia on oropharyngeal swallowing. Neuro-gastroenterol Motil 2000;12:567–572.
40. Ertekin C, Kıylıoglu N, Tarlacı S, Turman AB, Secil Y, Ay-dogdu I. Voluntary and reflex influences on the initiation ofswallowing reflex in man. Dysphagia 2001;16:40–47.
41. Ertekin C, Pehlivan M, Aydogdu I, Ertas M, Uludag B, CelebiG, Yuceyar N. An electrophysiological investigation of deglu-tition in man. Muscle Nerve 1995;18:1177–1186.
42. Ertekin C, Turman B, Tarlaci S, Celik M, Aydogdu I, Secil Y,Kiylioglu N. Cricopharyngeal sphincter muscle responses totranscranial magnetic stimulation in normal subjects and inpatients with dysphagia. Clin Neurophysiol 2001;112:86–94.
43. Ertekin C, Yuceyar N; Aydogdu I. Clinical and electrophysi-ological evaluation of dysphagia in myasthenia gravis. J Neu-rol Neurosurg Psychiatry 1998;65:848–856.
44. Ertekin C, Yuceyar N, Aydogdu I, Karasoy H. Electrophysio-logical evaluation of oropharyngeal swallowing in myotonicdystrophy. J Neurol Neurosurg Psychiatry 2001;70:363–371.
45. Freiman JM, El-Sharkey TY, Diamant NE. Effect of bilateralvagosympathetic nerve blockade on response of the dogupper esophageal sphincter (UES) to intraesophageal dis-tention and acid. Gastroenterology 1981;812:78–84.
46. Fyke FE, Code CF. Resting and deglutition pressures in thepharyngo-esophageal region. Gastroenterology 1955;29:24–34.
47. Goyal RK. Disorders of the cricopharyngeal muscle. Otolar-yngol Clin North Am 1984,17:115–130.
48. Goyal RK, Martin SB, Shapiro J, Spechler SJ. The role ofcricopharyngeus muscle in pharyngoesophageal disorders.Dysphagia 1993;8:252–258.
49. Grebt L, Barillot JC, Bianchi AL. Central distributions of theefferent and afferent components of the pharyngealbranches of the vagus and glossopharyngeal nerves: an HRPstudy in the cat. Exp Brain Res 1989;78:327–335.
50. Hamdy S, Aziz Q, Rothwell JC, Singh KD, Barlow J, HughesDG, Tallis RC,Thompson DG. The cortical topography ofhuman swallowing musculature in health and disease. NatMed 1996;2:1217–1224.
Cricopharyngeal Sphincter Muscle MUSCLE & NERVE December 2002 737

51. Hamdy S, Rothwell JC, David JB, Bailey D, Aziz Q, Thomp-son DG. Identification of the cerebral loci processing humanswallowing with H15O PET activation. J Neurophysiol 1999;81:1917–1926.
52. Hammond CS, Davenport PW, Hutchison A, Otto RA. Motorinnnervation of the cricopharyngeus muscle by the recur-rent laryngeal nerve. J Appl Physiol 1997;83:89–94.
53. Hayawaka T, Yajima Y, Zyo K. Ultrastructural characteriza-tion of pharyngeal and esophageal motoneurons in the nu-cleus ambiguus of the rat. J Comp Neurol 1996;370:135–146.
54. Hellemans J, Vantrappen G, Janssen J. Electromyogpaphy ofthe esophagus. In: Vantrappen G, Hellemans J, editors. Dis-orders of the esophagus. New York: Springer; 1974. p 270–285.
55. Hudson LC. The origins of innervation of the canine caudalpharyngeal muscles: an HRP study. Brain Res 1986;374:413–418.
56. Isberg A, Nilsson ME, Schiratzki H. The upper esophagealsphincter during normal deglutition. Acta Radiol Diagn1985;26:563–568.
57. Jacob P, Kahrilas PJ, Herzon McLaughin B. Determinants ofupper esophageal sphincter pressure in dogs. Am J Physiol1990,259:G245–G251.
58. Jacob P, Kahrilas PJ, Logeman JA, Shah V, Ha T. Upperesophageal sphincter opening and modulation during swal-lowing. Gastroenterology 1989;97:1469–1478.
59. Jean A. Brainstem organization of the swallowing network.Brain Behav Evol 1984;25:109–116.
60. Jean A. Control of the central swallowing program by inputsfrom the principal receptors. A review. J Auton Nerv Syst1986;10:225–233.
61. Jean A. Brainstem control of swallowing: neuronal networkand cellular mechanisms. Physiol Rev 2001;81:929–969.
62. Jean A, Car A. Inputs to swallowing medullary neuron’s fromthe peripheral afferent fibers and swallowing cortical area.Brain Res 1979;178:567–572.
63. Kahrilas PJ, Dodds WJ, Dent J, Haeberle B, Hogan WJ,Arndoorfer RC. Effect of sleep, spontaneous gastroesopha-geal reflux and a meal on upper esophageal sphincter pres-sure in normal human volunteers. Gastroenterology 1987;92:466–471.
64. Kahrilas PJ, Dodds WJ, Dent J, Logemann JA, Shaker R.Upper esophageal sphincter function during deglutition.Gastroenterology 1988;95:52–62.
65. Kawasaki M, Ogura JH, Takenovchi S. Neurophysiologicobservations of normal deglutition II: its relation to alliedphenomena. Laryngoscope 1964;74:1766–1780.
66. Kessler JP, Jean A. Identification of the medullary swallowingregions in the rat. Exp Brain Res 1985;57:256–263.
67. Kirchner JA. The motor activity of the cricopharyngeal mus-cle. Laryngoscope 1958;68:1119–1159.
68. Kitamura S, Ogata K, Nishiguchi T, Nagase Y, Shigenaga I.Location of motoneurons supplying the rabbit pharyngealconstrictor muscles and the peripheral course of their axons:a study using the retrograde HRP or fluorescent labelingtechnique. Anat Rec 1991;229:399–406.
69. Kristmundsdottir F, Mahon M, Froes MMQ, Cumming WJK.Histomorphometric and histopathological study of the hu-man cricopharyngeus muscle: in health and in motor neu-ron disease. Neuropathol Appl Neurobiol 1990;16:461–475.
70. Lang IM, Shaker R. Anatomy and physiology of the upperesophageal sphincter. Am J Med 1997;103:50S–55S.
71. Lang IM, Dantas RO, Cook IJ, Dodds WJ. Videoradio-graphic, manometric and electromyographic analysis of ca-nine upper esophageal sphincter. Am J Physiol 1991;260:G911–G919.
72. Levitt MN, Dedo HH, Ogura JH. The cricopharyngeus mus-cle, an electromyographic study in dog. Laryngoscope 1965;75:122–136.
73. Logemann JA. Evaluation and treatment of swallowing dis-orders, 2nd ed. Austin, TX: Pro-Ed Inc; 1998.
74. Martin RE, Sessle BJ. The role of the cerebral cortex inswallowing. Dysphagia 1993;8:195–202.
75. McConnel FMS, Cerenko D, Jackson RT, Guffin IN. Timingof major events of pharyngeal swallowing. Arch OtolaryngolHead Neck Surg 1988;114:1413–1418.
76. Medda BK, Lang IM, Dodds WJ, Christl M, Kern M, HoganWJ, Shaker R. Correlation of electrical and contractile activ-ities of the cricopharyngeus muscle in the cat. Am J Physiol1997;273:G470–G479.
77. Medda BK, Lang IM, Layman R, Dodds WJ, Hogan WJ,Shaker R. Characterization and quantification of pharyngo-UES contractile reflex in cats. Am J Physiol 1994;267:G972–G983.
78. Miller AJ. Deglutition. Physiol Rev 1982;62:129–184.79. Miller AJ. The neuroscientific principles of swallowing and
dysphagia. San Diego: Singular Publication Group; 1999.80. Mu L, Sanders I. The innervation of the human upper
esophageal sphincter. Dysphagia 1996;11:234–238.81. Mu L, Sanders I. Neuromuscular organisation of the human
upper esophageal sphincter. Ann Otol Rhinol Laryngol1998;107:370–377.
82. Murakami Y, Fukuda H, Kirchner JA. The cricopharyngeusmuscle, an electrophysiological and neuropharmacologicalstudy. Acta Otolaryngol 1972;311(Suppl):1–19.
83. Palmer JB. Electromyography of the muscles of oropharyn-geal swallowing. Basic concepts. Dysphagia 1989;3:192–198.
84. Palmer JB, Tanaka E, Siebens AA. Electromyography of thepharyngeal musculature: technical considerations. ArchPhys Med Rehabil 1989;70:283–287.
85. Pasricha PJ, Rai R, Ravich WJ, Hendrix TR, Kalloo AN.Botulinum toxin in achalasia: long term outcome and pre-dictors of response. Gastroenterology 1996;111:1410–1415.
86. Perlman AL. Electromyography and the study of oropharyn-geal swallowing. Dysphagia 1993;8:351–355.
87. Perlman AL, Luschei ES, Du Mond CE. Electrical activityfrom the superior pharyngeal constrictor during reflexiveand non-reflexive tasks. J Speech Hear Res 1989;32:749–754.
88. Ren J, Shaker R, Zamir Z, Dodds WJ, Hogan WJ, HoffmannRG. Effect of age and bolus variables on the coordination ofthe glottis and upper esophageal sphincter during swallow-ing. Am J Gastroenterol 1993;88:665–669.
89. Sasaki CT, Kim YH, Stevenson H, Czibulka A. Motor inner-vation of the human cricopharyngeus muscle. Ann OtolRhinol Laryngol 1999;108:1132–1139.
90. Schneider I, Thumfart W, Eckel HE. Treatment of dysfunc-tion of the cricopharyngeal muscle with botulinum toxin:introduction of new noninvasive method. Ann Otol RhinolLaryngol 1994;103:31–35.
91. Shaker R, Bardan E. Management of swallowing disorders.In: Corazziari E, editor. Neurogastroenterology. Berlin: deGruyter; 1996. p 243–275.
92. Shaker R, Dodds WJ, Dantas RO, Hogan WJ, Arndorfer RC.Coordination of deglutitive glottic closure with oropharyn-geal swallowing. Gastroenterology 1990;98:1478–1484.
93. Shaker R, Dodds WJ, Ren J, Hogan WJ, Arndorfer RC.Esophagoglottal closure reflex: a mechanism of airway pro-tection. Gastroenterology 1992;102:857–861
94. Shaw GY, Searl JP. Botulinum toxin treatment for cricopha-ryngeal dysfunction. Dysphagia 2001;16:161–167.
95. Shipp T, Deatsch WW, Robertson K. Pharyngoesophagealmuscle activity during swallowing in man. Laryngoscope1970;80:1–16.
96. Sokol EM, Heitmann P, Wolf BS, Cohen BR. Simultaneouscineoradiographic and manometric study of the pharynx,hypopharynx and cervical esophagus. Gastroenterology1966;51:960–974.
97. Staff D, Shaker R. Aging in the gastrointestinal tract. DisMon 2001;47:72–101.
98. Steinberg JL, Khane GJ, Fernandes CMG, Nel YP. Anatomyof the recurrent laryngeal nerve: a redescription. J LaryngolOtol 1986;100:919–927.
738 Cricopharyngeal Sphincter Muscle MUSCLE & NERVE December 2002

99. Tanaka E, Palmer J, Siebens A. Bipolar suction electrodes forpharyngeal electromyography. Dysphagia 1986;1:39–40.
100. Trate DM, Parkman HP, Fisher RS. Dysphagia. Evaluation,diagnosis, and treatment. Prim Care 1996;23:417–432.
101. Van Overbeek JJ, Wit HP, Paping RHL, Segenhout HM.Simultaneous manometry and electromyography in thepharyngoesophageal segment. Laryngoscope 1985;95:582–584.
102. Venker-van Haagen AJ, Barbas-Henry HA, Van den BromWE. CMAPs in pharyngeal and hyoid muscles evoked bynucleus solitarius stimulation in dogs. Brain Res Bull 1995;37:555–559.
103. Venker-van Haagen AJ, Hartman W, van den Brom WE,Wolvekamp WT.Continuous electromyographic recordingsof pharyngeal muscle activity in normal and previously de-nervated muscles in dogs. Am J Vet Res 1989;50:1725–1728.
104. Venker-van Haagen AJ, Hartman W, Wolvekamp WTC. Con-tributions of the glossopharyngeal nerve and the pharyngealbranch of the vagus nerve to the swallowing process in dogs.Am J Vet Res 1986;47:1300–1307.
105. Zoungrana OR, Amri M, Car A, Roman C. Intracellularactivity of motoneurons of the rostral nucleus ambiguusduring swallowing in sheep. J Neurophysiol 1997;77:909–922.
Cricopharyngeal Sphincter Muscle MUSCLE & NERVE December 2002 739