Embed Size (px)
Citation preview

Electroencephalography
doc. MUDr. Valja Kellerová, DrSc.
Department of Neurology

Principle of EEG:
• EEG examines the spontaneous electrical activity of the brain by means of scalp electrodes
• recording procedure: amplification
recording (20 minutes at least)
storage (on CD, DVD,
NAS, cloud …)

Electrode placement – the „ten-twenty“ electrode system

Principle of registration• EEG curve is registered/recalculated as the
difference of electric potentials between two electrodes (varying in the course of time)
• derivation = recording from a pair of electrodes (two electrodes are connected to a single amplifier, to one EEG channel)
– bipolar
– monopolar

Montages
• montage = a particular
electrode arrangement,
a number of different derivations is diplayed simultaneously
• commonly used and preset montages:– longitudinal
– transverse
– ( referential )
EEG reading
• Morphology
• Amplitude
• Frequency

EEG reading: morphology (wave shape)
• sharp waves• spikes = epileptiform patterns, • spike-and-wave complexes… they accompany epilepsy

EEG reading: amplitude
• voltage in microvolts• a peak-to-peak measurement• compared with the calibration signal• commonly 20 -100 μV (in normal EEG)
• amplitude changes may be pathological

EEG reading: frequency
• the rhythmic EEG activity is classified as:– delta - less than 4 Hz– theta – 4 to 8 Hz– alpha – 8 to 13 Hz– beta – more than 13 Hz

Normal rhythms• Alpha rhythm
– sinusoidal waves (8-13 Hz)
– maximal over the posterior head region (occipitally)
– occurs during wakefulness and relaxation
– best seen with the patient’s eyes closed
– blocked or attenuated with eye opening

Normal rhythms• Beta rhythm
– is not prominent
– has low amplitude – is best seen frontally– not affected by eye opening
• Theta rhythm– a small amount, of low
amplitude, frontally
– accompanies drowsiness
• Delta rhythm– is normal during deep sleep
– is normal in childhood– is abnormal in the other cases
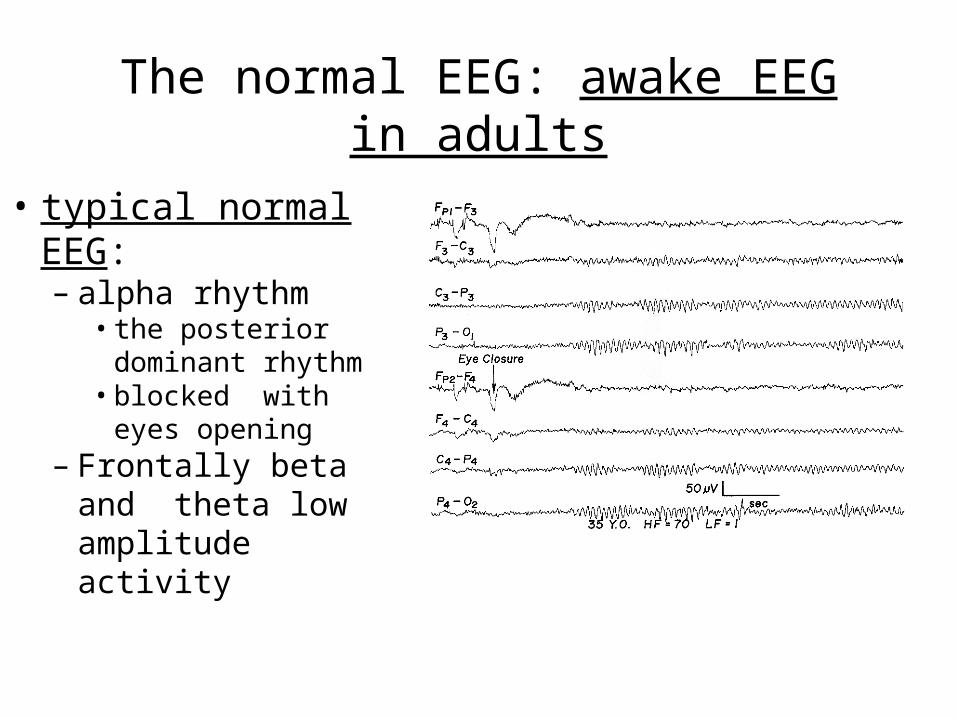
The normal EEG: awake EEG in adults
• typical normal EEG:– alpha rhythm
• the posterior dominant rhythm
• blocked with eyes opening
– Frontally beta and theta low amplitude activity

The normal EEG: awake EEG in adults
• low voltage EEG („atypical flat EEG“)– a variety of normal finding– 10% of normal healthy adults– no activity over 20 μV– various frequencies may be present– alpha rhythm may be absent

disappearance of the alpha rhythm
low voltage beta activity or flat recording
low voltage theta (5-6 Hz)
3-4 Hz (moderate amplitude)
paradoxical reaction to eye opening (alpha rhythm appears)
The normal EEG during drowsiness and NREM sleep
Drowsiness - somnolence

The normal EEG: EEG during drowsiness and sleep - NREM sleep
• Sleep stage 2:– slow waves 3-4 Hz continue
sleep spindles(12-14-16 Hz)
and K complexes (reaction to stimuli)

The normal EEG: EEG during drowsiness and sleep - NREM sleep
• Sleep stage 3: – slow waves of 2 Hz or less, of high amplitude
(20-50% of the recording time)
• Sleep stage 4:– slow activity of about 1 Hz (over 50%)

The normal EEG: EEG during drowsiness and sleep - REM sleep
• REM sleep (paradoxical sleep):– associated with dreaming– asynchronous low voltage waves of mixed
frequency– may resemble the pattern of stage 1

PolysomnographyFor reliable determination of REM stage polysomnography is necessary with recording also:
– rapid eye movements– heart rate and breathing– EMG of the mental muscles (postural) – tonic
activity disappears in the REM stage

Polysomnographyin NREM and REM sleep

Polysomnography in REM sleep (patient with narcolepsy)

Sleep cycles• Sleep cycles
– last about 80-120 minutes– NREM sleep lasts about 60-90 minutes– REM sleep lasts about 10-30 minutes (it is
longer in the morning)

Abnormal EEG patterns • abnormalities of the background rhythms
(areal differentiation, hemispheral organization…)
• abnormal sleep patterns – narcolepsy
• paroxysmal epileptiform abnormalities (generalized, focal…) - epilepsy
• abnormal slow activity (generalized, focal…) – structural cerebral lesions
• amplitude changes

Narcolepsy

Abnormal sleep patterns - narcolepsy
– short latency to sleep onset (less than 5 min)
– sleep onset REM periods
– multiple sleep latency test (MSLT):• gives a patient 5 opportunities to fall asleep during
the day
• at 2-hour intervals EEG is recorded and the patient is given 20 min to fall asleep
• if 2 or more sleep periods contain REM sleep, then a diagnosis of narcolepsy is highly likely

Abnormal EEG – amplitude changes:
• local - reduction of amplitude due to:– superficial lesions in the cortex, rare– change of material between cortex and
electrodes – subdural hematoma - flattening

Abnormal EEG – amplitude changes:
• generalized – in deep comaburst-suppression pattern or flat record

EEG in epilepsy
• interictal patterns – in intervals without seizures– epileptiform patterns – sharp waves, spikes,
spike-and-wave complexes– local, as a focus– or generalized
• ictal patterns – during seizure

Interictal patterns in epilepsy – localfocus:

Interictal patterns in epilepsy – generalized:
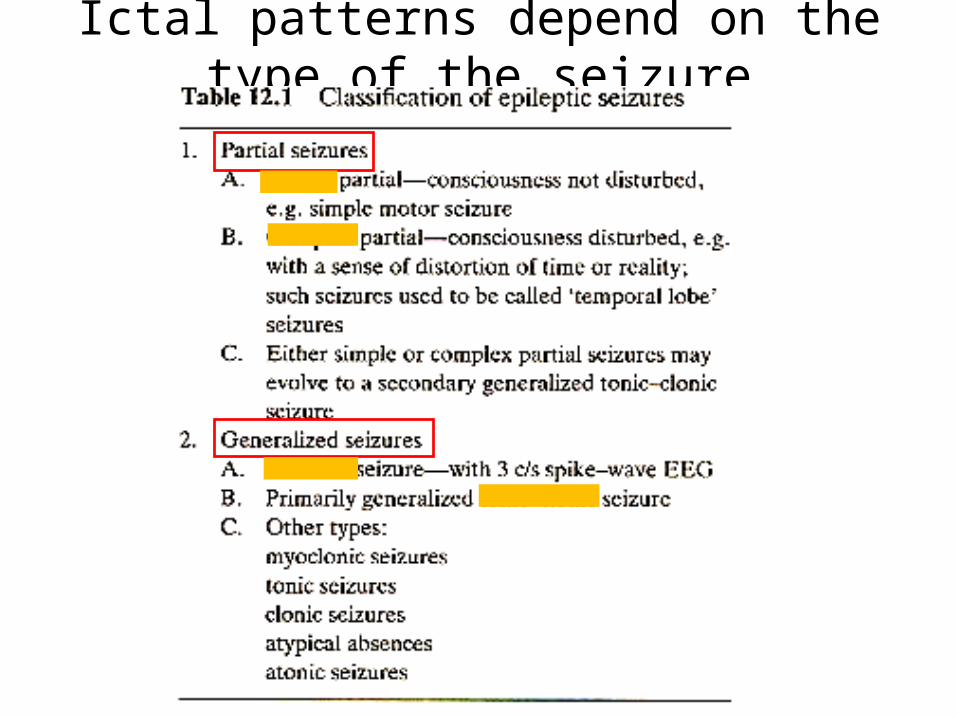
Ictal patterns depend on the type of the seizure

Simple partial seizures - consciousness is not impaired
- Jacksonian motor or somatosensory seizure

Simple partial seizures -single repetitive sharp waves

Complex partial seizurestemporal lobe seizure with automatisms

Complex partial seizures -sharp theta waves 6Hz – temporal region
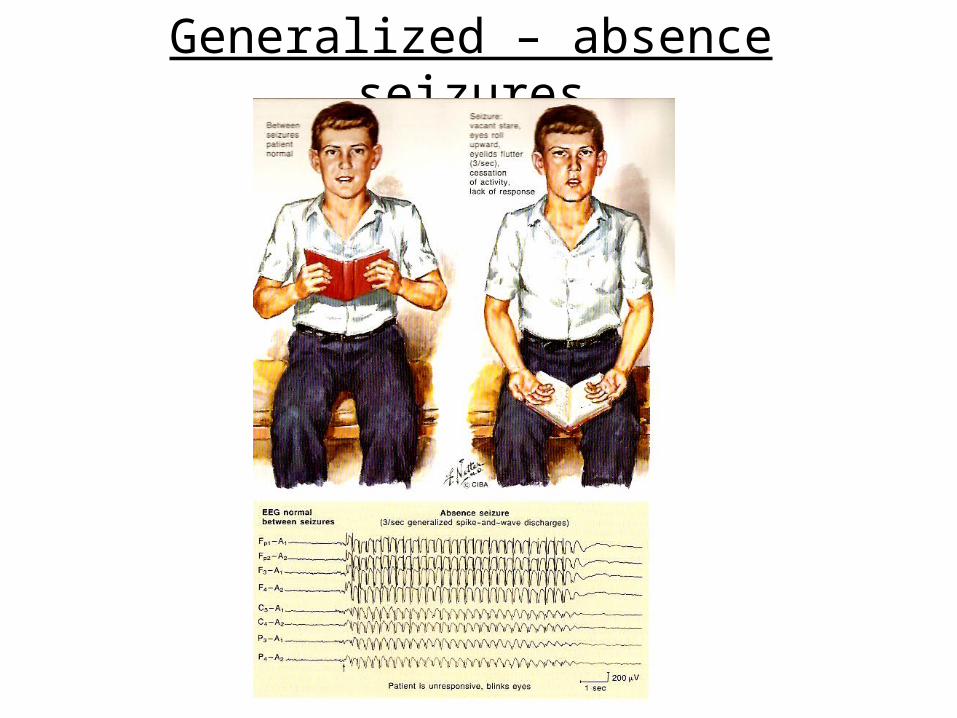
Generalized – absence seizures

Absence seizures – 3/sec generalized spike-and-wave discharges

Absence seizures

Generalized tonic-clonic seizures

Generalized tonic-clonic seizures• Tonic phase: generalized hypersynchronous 8-12Hz
sharp waves and muscle artifacts• clonic phase – generalized rhythmic spikes form groups,
followed by a slow wave• postictal coma – lower voltage arrhythmic activity,
attenuation and slowing or flat EEG

Generalized tonic-clonic seizure –tonic and clonic phase

Generalized tonic-clonic seizure –clonic and postictal phase

EEG in structural cerebral lesions
• Tumours
• Abscesses
• Contusions
• Strokes
cause mainly local slow waves (theta or delta), they form a focus of slow waves

EEG in structural cerebral lesions

Brain tumours
• supratentorial– focal slow waves (irregular, persistent delta)
– principles of localization of large tumours: “phase reversal”
• deep or infratentorial– episodes of synchronous slow waves theta or
delta

Phase reversal

Phase reversal

Activation procedures
• Hyperventilation– in all patients, 4 minutes– absence of any change is normal– abnormal responses include epileptiform
activity
• intermittent photic stimulation
• sleep recordings – after sleep deprivation

intermittent photic stimulation– rhythmic flashes, 1 - 30 Hz– normal response – photic driving, reproduction of the
rhythm - mostly frequencies of alpha, partially beta

intermittent photic stimulation– photic driving increases
• Hyperthyroidism
• tumours in the posterior fossa
• Migraine (fast beta)
– abnormal – photo convulsive response (epileptiform activity)

sleep recordings – after sleep deprivation
– drowsiness and light sleep (stages 1 and 2 of NREM sleep) accentuate epileptiform abnormalities
– all night sleep deprivation is required prior to taking the EEG

Easy, isn’t it ?





























