Embed Size (px)
Citation preview

2195
□ ORIGINAL ARTICLE □
Efficacy of Rikkunshito, a Traditional Japanese Medicine(Kampo), in Treating Functional Dyspepsia
Hiroaki Kusunoki 1, Ken Haruma 2, Jiro Hata 3, Manabu Ishii 2, Tomoari Kamada 2,
Naohito Yamashita 1, Keisuke Honda 1, Kazuhiko Inoue 1, Hiroshi Imamura 3,
Noriaki Manabe 3, Akiko Shiotani 2 and Tsukasa Tsunoda 1
Abstract
Background Rikkunshito, a traditional Japanese (Kampo) medicine, is widely prescribed as an oral prepa-
ration for the treatment of functional dyspepsia (FD). In our previous study, we reported that extracorporeal
ultrasonography (US) is a useful technique for the assessment of the gastric accommodation reflex (AR) and
duodenogastric motility. In this study, we examined the effects of Rikkunshito on the gastroduodenal function
in patients with FD.
Methods Sixteen FD patients (median age, 45 y) underwent US, before and after 14 days of treatment with
Rikkunshito (7.5 g b.d.). For assessment of the AR, a cross-sectional area of the proximal stomach was mea-
sured after incremental ingestion of a liquid meal up to 400-mL. The expansion rate was used as the parame-
ter to determine the AR. Then, the gastric emptying rate (GER), motility index (MI), and reflux index (RI)
were evaluated using previously reported methods.
Results Although no significant changes were observed in the total score of the Gastrointestinal Symptom
Rating Scale (GSRS), the scores of 3 of the 15 symptoms of GSRS decreased significantly after treatment
with Rikkunshito. The expansion rate of the proximal stomach was significantly greater after treatment with
Rikkunshito than before the treatment. Although the GER and MI increased significantly, no significant dif-
ferences in the RI were observed after treatment with Rikkunshito.
Conclusion These observations suggested that Rikkunshito may be beneficial for the treatment of FD pa-
tients with impaired AR and gastric motility. These results also suggested that Rikkunshito has a therapeutic
potential for FD and GERD.
Key words: Rikkunshito, gastric accommodation reflex, gastroduodenal motility, ultrasound, traditional Japa-
nese medicine (Kampo)
(Inter Med 49: 2195-2202, 2010)(DOI: 10.2169/internalmedicine.49.3803)
Introduction
Functional dyspepsia (FD) is defined as the presence of
gastrointestinal symptoms such as epigastric pain, epigastric
burning, postprandial fullness, and early satiation in the ab-
sence of any organic, systemic, or metabolic disease.
On the basis of the Rome III criteria (1), FD is subdi-
vided into 2 diagnostic categories: 1) meal-induced
postprandial distress syndrome (PDS), which is character-
ized by postprandial fullness and early satiation, and 2) epi-
gastric pain syndrome (EPS), which is characterized by epi-
gastric pain and burning. These categories were proposed
under the assumption that the 2 types of FD might arise
from different underlying pathophysiological mechanisms. It
has been suggested that impaired accommodation reflex
1Department of General Medicine, Kawasaki Medical School, Kurashiki, 2Division of Gastroenterology, Department of Internal Medicine,
Kawasaki Medical School, Kurashiki and 3Division of Endoscopy and Ultrasound, Department of Clinical Pathology and Laboratory Medicine,
Kawasaki Medical School, Kurashiki
Received for publication April 13, 2010; Accepted for publication July 14, 2010
Correspondence to Dr. Hiroaki Kusunoki, [email protected]

Inter Med 49: 2195-2202, 2010 DOI: 10.2169/internalmedicine.49.3803
2196
(AR) of the proximal stomach and delayed gastric emptying
may play major roles in the pathogenesis of the PDS sub-
group (2). According to previous reports, these functional
abnormalities are observed in 15% to 50% of all FD pa-
tients (3, 4). Therefore, assessment of both the gastric AR
and gastroduodenal motility is essential for understanding
the pathogenesis of FD.
Rikkunshito is an orally administered Japanese herbal
(Kampo) preparation that is widely prescribed for patients
showing various gastrointestinal symptoms such as gastroe-
sophageal reflux (5, 6), dyspeptic symptoms of post gastro-
intestinal surgery (7, 8), and chemotherapy-induced nau-
sea (9). Rikkunshito is composed of 8 constituents: Glycyr-
rhizae radix (4.7%), Zingiberis rhizoma (2.3%), Atractylodis
lanceae rhizoma (18.6%), Zizyphi fructus (9.3%), Aurantii
nobilis pericarpium (9.3%), Ginseng radix (18.6%), Pinelliae
tuber (18.6%), and Hoelen (18.6%). Several studies have
shown that many Japanese herbal medicines, including Rik-
kunshito, improve gastroduodenal motility-related disorders
and are therefore clinically efficacious against FD to some
extent (10-14). However, few studies have been reported on
the action mechanism of this medicine in humans (15); al-
though Rikkunshito has been demonstrated to improve the
impairment in the gastric AR in vitro (16), no clinical re-
ports have been published on the effects of Rikkunshito on
the gastric AR.
In our previous study, we reported that extracorporeal ul-
trasonography (US) is a useful modality for the assessment
of meal-induced gastric AR, gastric emptying rate (GER),
antral contractions, and duodenogastric reflux
(DGR) (17-22). The aim of this study was to determine the
clinical effects of Rikkunshito on gastric AR and gastroduo-
denal motility in FD patients by using US.
Subjects and Methods
Study Subjects
Sixteen FD patients (10 men and 6 women; age range,
28-78 y; median age, 45 y) were enrolled in this study. All
of the patients were diagnosed with FD according to the
Rome III criteria. None of them had a history of diabetes
mellitus and gastrointestinal surgery; they were not under
any medications that could affect gastric motility. Smoking
was prohibited on the day before and on both days of ultra-
sonographic examination. Candidates infected with Helico-bacter pylori were not excluded from the study. The proto-
col for this study was approved by the Ethics Committee of
Kawasaki Medical School, and all participants gave prior in-
formed consent.
Study Methods
Changes in gastrointestinal symptoms
The changes in the gastrointestinal symptoms were evalu-
ated on the basis of the Gastrointestinal Symptom Rating
Scale (GSRS), Japanese edition (23). The GSRS is com-
posed of 15 items, each rated according to severity on a
scale of 1 (absence of the symptom) to 7 (maximal intensity
of the symptom) (23); thus, higher GSRS scores indicate
more severe symptoms. We used the total score and the 15
gastrointestinal symptoms of GSRS for evaluating the dys-
peptic symptoms. The GSRS questionnaire was administered
twice to each patient (before and after treatment with Rik-
kunshito).
Assessment of AR
The patients were examined by US, before and after 14
days of treatment with Rikkunshito (TJ-43; Tsumura, Tokyo,
Japan) administered at a dose of 7.5 g b.d. The patients
were asked to fast overnight and before the US examination,
they were asked to consume incremental amounts of up to
400-mL of a liquid meal (consommé soup, 13 kcal/400-mL)
through a straw. Thereafter, the cross-sectional area of the
proximal stomach was measured for assessment of the gas-
tric AR with the subjects lying on a bed in the supine posi-
tion. In order to obtain the largest cross-sectional area of the
proximal stomach, an US probe was positioned and main-
tained in the intercostal space of the left axilla (Fig. 1) of
the patient, with the spleen as the landmark for this view
(Fig. 2) as described previously (20-22). The cross-sectional
area of the proximal stomach was estimated by tracing its
mucosal side using built-in calipers for 1-2 minutes after the
meal ingestion. The expansion rate in the cross-sectional
area measured before and after treatment with the drug was
expressed as follows: “[(area of each volume after ingestion
- area before ingestion) ÷ area before ingestion] ×100 (%).”
Assessment of gastroduodenal motility
After the assessment of gastric AR, the patients were
asked to sit on a chair, reclining slightly backwards, and the
GER, antral contractions, and DGR were evaluated by US,
as described previously (17-20, 22). The US probe was po-
sitioned vertically to simultaneously visualize the antrum,
superior mesenteric artery, and abdominal aorta.
The antral area was estimated by tracing the mucosal side
of the antrum with built-in caliper at 1 minute and 15 min-
utes after ingestion of the liquid meal. The GER was ex-
pressed as follows: “[(antral area at 1 minute - antral area at
15 minutes) ÷ antral area at 1 minute] ×100 (%).” The fre-
quency of antral contractions was defined as the number of
contractions per 3 minutes. The amplitude of the antral con-
tractions was calculated from the maximal reduction in the
antral area for each contraction as follows: “[(antral area at
the time of relaxation - antral area at the time of contrac-
tion) ÷ antral area at the time of relaxation] ×100 (%)”. The
motility index (MI) was expressed as the product of the fre-
quency of contractions and mean amplitude.
To evaluate the DGR by color Doppler US, we positioned
the US probe at the level of the transpyloric plane to simul-
taneously visualize the antrum, pylorus, and proximal duo-
denum. The color gain, high-pass filter, and angle between

Inter Med 49: 2195-2202, 2010 DOI: 10.2169/internalmedicine.49.3803
2197
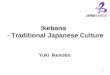
Figure 1. The position of the ultrasonography probe to obtain the largest cross-sectional area of the proximal stomach. The probe was placed in the intercostal space of the left axilla.
Figure 2. Changes in the US images of the largest cross-sectional area of the proximal stomach after incremental ingestion of up to 400-mL of a liquid meal. The incremental changes in the area of the proximal stomach positively corresponded to the intake volumes. The spleen was used as the marker for this view. The cross-sectional area of the proximal stomach was evaluated by marking the mucosal side with built-in calipers.
the US beam and the transpyloric flow were standardized
for all measurements. The frequency of DGR was defined as
the amount of DGR obtained at a distance “x” (measured in
cm) of the color signal from the pylorus. The reflux index
(RI) was expressed as follows: “frequency of DGR × mean
intensity of DGR.
All of the evaluations were performed by one researcher
(Kusunoki H). The equipment used was an SSA-770A US
system (Toshiba, Nasu, Japan) with a 3.75-MHz curved ar-
ray scanner.
Statistical analysis
The data are expressed as mean ± SE. The statistical sig-
nificance of differences between the 2 groups was assessed

Inter Med 49: 2195-2202, 2010 DOI: 10.2169/internalmedicine.49.3803
2198
Figure 3. Changes in the total score of GSRS. Although the total score of GSRS decreased after treatment with Rikkunshito, the differences were not statistically significant.
Table 1. Changes in the 15 Items of Gastrointestinal Symptoms of GSRS were Shown in the Table1. The Scores of Three Items of Gastrointestinal Symptoms (Abdominal Pains, Heartburn, and Abdominal Distension) of GSRS Decreased Significantly after Treatment with Rikkunshito.
using the Mann-Whitney’s test, the Wilcoxon test, or the
Student’s t-test. The difference was considered statistically
significant if p<0.05.
Results
Changes in gastrointestinal symptoms
Although the total score of GSRS decreased after treat-
ment with Rikkunshito, the differences were not statistically
significant (Fig. 3). However, the scores of 3 of the gastro-
intestinal symptoms of GSRS (abdominal pain, heartburn,
and abdominal distension) decreased significantly after treat-
ment with Rikkunshito (Table 1).
Assessment of AR
The expansion rate in the cross-sectional area of the
proximal stomach was significantly greater after treatment
with Rikkunshito than before the treatment (before treatment
vs. after treatment: after 100-mL ingestion, 2.20±0.28 vs.
3.27±0.45, p=0.034; after 200-mL ingestion, 3.69±0.57 vs.
6.51±1.39, p=0.007; after 300-mL ingestion, 5.13±0.97 vs.
9.08±2.06, p=0.017; and after 400-mL ingestion, 6.40±1.29)
vs. 11.29±2.48, p=0.017) (Fig. 4).
Assessment of gastroduodenal motility
Although the values of GER [before treatment vs. after
treatment: 57.9±5.7 vs. 72.3±5.4, p=0.010] and MI [7.93±
0.48 vs. 8.88±0.24, p=0.049] increased significantly after
Rikkunshito treatment, those of RI [18.8±3.1 vs. 15.3±3.0,
p=0.463] were not significantly different (Fig. 5). None of
the subjects had any adverse events that necessitated with-
drawal from the study.

Inter Med 49: 2195-2202, 2010 DOI: 10.2169/internalmedicine.49.3803
2199
Figure 4. The expansion rate in the cross-sectional area measured before and after treatment with Rikkunshito was expressed as“[(area of each volume after ingestion - area of each volume before ingestion) ÷ area before ingestion] × 100 (%).” The expansion rate in the cross-sectional area of the proximal stomach was significantly greater after treatment with Rikkunshito than be-fore the treatment
Figure 5. Changes in the gastric emptying rate (GER), motility index (MI), and reflux index (RI) before and after treatment with Rikkunshito. Although the values of GER and MI increased significantly after Rikkunshito treatment, those of RI were not significantly different.

Inter Med 49: 2195-2202, 2010 DOI: 10.2169/internalmedicine.49.3803
2200
Discussion
Traditional Japanese (Kampo) medicines are widely pre-
scribed in Japan for patients with various gastrointestinal
symptoms, and Rikkunshito is the most popular Kampo
medicine prescribed for the treatment of FD. Some clinical
studies have reported that Rikkunshito is efficacious in the
treatment of FD-related gastrointestinal (10-12, 14, 15) and
gastroesophageal reflux disease (GERD) symptoms (5, 6). In
the present study, we showed that the scores of 3 of the gas-
trointestinal symptoms of GSRS (abdominal pain, heartburn,
and abdominal distension) decreased significantly after treat-
ment with Rikkunshito. In this study, although we consid-
ered the symptoms individually, the present rating scale ap-
pears to be effective in assessing the degree of symptoms
and the changes before and after treatment. Our results were
consistent with those of previous studies, which suggested
that Rikkunshito may have a therapeutic potential for not
only FD patients with PDS but also FD patients with EPS
and GERD. All of the mechanisms underlying the effects of
Rikkunshito on these symptoms cannot be explained; how-
ever, improvement of AR, GER, and MI may contribute to
decreasing the GSRS score of 3 of the gastrointestinal
symptoms of GSRS. With regard to the effect of Rikkun-
shito on heartburn, Kawahara et al reported that Rikkunshito
reduces distal esophageal acid exposure by improving
esophageal acid clearance (6). However, since Rikkunshito
is composed of over 100 compounds, including 8 major
constituents, it is highly likely that this drug produces symp-
tomatic relief through an unknown prokinetic action. Addi-
tional mechanistic studies need to be performed in FD pa-
tients to conclusively determine the effects of Rikkunshito.
Previous studies have shown that Rikkunshito impairs the
adaptive AR in vitro (16); however, no reports have been
published on the clinical effects of Rikkunshito on AR. This
is the first clinical report showing that Rikkunshito enhanced
the meal-induced AR of the proximal stomach. In the pre-
sent study, we selected the cross-sectional area of the proxi-
mal stomach as a criterion for the assessment of gastric AR
by US (21, 22). The measurement of this criterion is simple
and easy. The efficacy of the previous methods that evalu-
ated the intragastric volume on the basis of the cross-
sectional area of the proximal stomach has been shown in
previous studies (21, 22). A previous study reported that
changes in the cross-sectional area of the proximal stomach
are significantly correlated with the changes in the gastric
volume caused by the ingestion of a liquid meal (21). Using
this method, we also reported that FD patients had impaired
gastric AR (21). Furthermore, Matsumoto et al (24) reported
that US and a pressure sensor can be used to assess the iso-
tonic expansion of the proximal stomach.
In the present study, all evaluations were performed by
the same researcher to prevent inter-observer variation. The
US probe was positioned and maintained in the same posi-
tion for all patients, and the expansion rate of the same area
was measured to assess the AR; this helped to prevent in-
consistencies in the results; however, the reproducibility of
the measurements was not adequately evaluated. In addition,
we selected and confirmed some landmarks to help maintain
the same view throughout the measurement (17-22). There-
fore, we believe that there were very few human errors of
measurement in this method.
Several devices such as the barostat and techniques such
as scintigraphy, single photon emission computed tomogra-
phy (SPECT), and magnetic resonance imaging have been
used to evaluate gastrointestinal functions (25-29) including
meal-induced gastric AR; however, these techniques often
have technical limitations and are too expensive or complex
for daily use. Hence, the use of the barostat is the standard
method for the assessment of AR in the proximal stomach
and has been used in several studies (4, 25, 30-33). How-
ever, this method is invasive and because the presence of
food in the stomach would interfere with the expansion of
the balloon of the barostat system, the value of the postpran-
dial gastric volume may be less than that recorded before
consuming the test meal (34). Similarly, the US method has
the same disadvantage as the barostat, i.e., it requires the pa-
tients to be in the supine position for partial distribution of
the liquid test meal in the proximal stomach. Therefore, the
US method also cannot be used to evaluate the AR with
normal gastric distribution of a liquid test meal. However,
we selected the US method for easy AR assessment.
Rikkunshito has reported improvement in delayed gastric
emptying in rats in vivo (35). However, there are few re-
ports discussing the clinical effects of Rikkunshito on gas-
troduodenal motility in humans (19). In a previous study by
Tatsuta and Ishii, 42 patients with FD were randomly di-
vided into the “Rikkunshito-treated” group and the
“Combizym-treated” group; they reported that Rikkunshito
enhances gastric emptying and provides significantly greater
relief from some symptoms than Combizym (11). In their
recent study, Kawahara et al demonstrated that administra-
tion of Rikkunshito results in symptomatic relief and im-
proves gastric emptying in patients with severe FD because
of delayed gastric emptying (6). In the present study, we
showed that Rikkunshito administration enhanced the meal-
induced AR of the proximal stomach, GER, and MI in pa-
tients with FD. Therefore, our results were consistent with
the reports of previous studies indicating that this drug has
an effect on gastric motility.
With regard to the role of Rikkunshito in the enhance-
ment of AR, GER, and MI, the precise mechanisms underly-
ing the effects of Rikkunshito on gastric AR and gastroduo-
denal motility are still unclear; however, the pharmacologi-
cal mechanisms and active ingredients of Rikkunshito have
been elucidated in part (16, 35). Factors associated with gas-
tric motility, such as gastric emptying and gastric AR, are
regulated by various effectors, including nitric oxide (NO),
5-hydroxytryptamine (5-HT), and its receptors. Studies have
shown that the prokinetic actions of Rikkunshito are medi-
ated by NO (16, 35, 36). Initially, the actions of Rikkun-

Inter Med 49: 2195-2202, 2010 DOI: 10.2169/internalmedicine.49.3803
2201
shito were thought to be mediated via NO production alone
because it contains L-arginine, a substrate of NO, in its
water fraction. Subsequently, analysis of the fractional ex-
tracts of Rikkunshito revealed that the methanol fraction
contained an even more potent promoter of gastric motility,
namely, hesperidin (35). It was reported that hesperidin is
not a substrate of NO because it does not belong to the
guanidine group (37) and that it actually decreases NO pro-
duction (38). Thus, Rikkunshito and hesperidin were be-
lieved to promote gastric motility through a mechanism
other than that mediated by NO. However, in a recent study,
Tominaga et al (39) reported that Rikkunshito has no effect
on dopamine-induced gastrointestinal motility. They also re-
ported that Rikkunshito has 5-HT3-antagonist effects on gas-
tric motility. Initially, we believed that the role of Rikkun-
shito in promoting gastric motility may be mediated by
ghrelin because Rikkunshito elevates the low plasma ghrelin
levels that are induced by cisplatin (40). Some subsequent
studies (41-43) revealed that the pharmacological actions of
Rikkunshito in promoting gastric motility may be associated
with ghrelin. Therefore, our results corroborate the evidence
obtained by previous studies showing that Rikkunshito has
an effect on gastric motility.
In the present study, although we confirmed the gastric
prokinetic actions of Rikkunshito by US evaluation, Rikkun-
shito did not show any significant effect on DGR. The DGR
occurs as a result of the reversal of the original pressure
gradient between the duodenum and the antrum. The mecha-
nism underlying this phenomenon is unclear; the DGR may
be related to a duodenal brake caused by early gastric emp-
tying. Thus, a decrease in DGR reflects the normalization of
gastrointestinal coordination.
In summary, this study showed that Rikkunshito enhanced
meal-induced gastric AR, GER, and MI in patients with FD
and that the scores of three of the gastrointestinal symptoms
of GSRS (abdominal pain, heartburn, and abdominal disten-
sion) decreased significantly after treatment with Rikkun-
shito. These observations suggested that Rikkunshito may be
beneficial for the treatment of FD patients with impaired AR
and gastric motility. These results also suggested that Rik-
kunshito has a therapeutic potential for FD (both PDS and
EPS) and GERD.
References
1. Tack J, Talley NJ, Camilleri M, et al. Functional gastrointestinal
disorders. Gastroenterology 130: 1466-1479, 2006.
2. Karamanolis G, Caenepeel P, Arts J, Tack J. Association of pre-
dominant symptom with clinical characteristics and pathophysi-
ological mechanisms in functional dyspepsia. Gastroenterology
130: 296-303, 2006.
3. Quartero AO, De Wit NJ, Lodder AC, Numans ME, Smout AJPM,
Hoes AW. Disturbed solid-phase gastric emptying in functional
dyspepsia. A meta-analysis. Dig Dis Sci 43: 2028-2033, 1998.
4. Van Den Elzen BDJ, Boeckxstaens GEE. A critical view on im-
paired accommodation as therapeutic target for functional dyspep-
sia. Aliment Pharmacol Ther 23: 1499-1510, 2006.
5. Kawahara H, Kubota A, Hasegawa T, et al. Effect of rikkunshito
on the clinical symptoms and esophageal acid exposure in chil-
dren with symptomatic gastroesophageal reflux. Pediatr Surg Int
23: 1001-1005, 2007.
6. Kawahara H, Mitani Y, Nomura M, et al. Impact of rikkunshito,
an herbal medicine, on delayed gastric emptying in profoundly
handicapped patients. Pediatr Surg Int 25: 987-990, 2009.
7. Yagi M, Homma S, Kubota M, et al. The herbal medicine
Rikkunshi-to stimulates and coordinates the gastric myoelectric
activity in post-operative dyspeptic children after gastrointestinal
surgery. Pediatr Surg Int 19: 760-765, 2004.
8. Tomono H, Ito Y, Watanabe T. Successful antiemetic treatment of
TSUMURA Rikkunshi-to extract granules for ethical use in addi-
tional to other antiemetic agents in neoadjuvant chemotherapy for
an advanced breast cancer patient. Gan To Kagaku Ryoho 33:
1129-1131, 2006.
9. Takahashi T, Endo S, Nakajima K, Souma Y, Nishida T. Effect of
Rikkunshito, a Chinese herbal medicine, on stasis in patients after
pylorus-preserving gastrectomy. World J Surg 33: 296-302, 2009.
10. Oka T, Tamagawa Y, Hayashida S, Kaneda Y, Kodama N, Tsuji S.
Rikkunshito attenuates adverse gastrointestinal symptoms induced
by fluvoxamine. Biopsychosoc Med 1: 21, 2007.
11. Tatsuta A, Ishii H. Effect of treatment with Lin-Jun-Zi-Tang (TJ-
43) on gastric emptying and gastrointestinal symptoms in dyspep-
tic patients. Aliment Pharmacol Ther 7: 459-462, 1993.
12. Terasawa K. Evidence-based reconstruction of Kampo medicine
part-III-how should Kampo be evaluated? eCAM 1: 219-222,
2004.
13. Oyachi N, Takano K, Hasuda N, Arai H, Koshizuka K, Matsu-
moto M. Effect of Rikkunshi-to on infantile hypertrophic pyloric
stenosis, refractory to atropine. Pediatr Int 50: 581-583, 2008.
14. Oikawa T, Ito G, Hoshino T, Koyama H, Hanawa T.
Hangekobokuto (Banxia-houpo-tang), a Kampo medicine that
treats functional dyspepsia. eCAM 6: 375-378, 2009.
15. Suzuki H, Inadomi JM, Hibi T. Japanese herbal medicine in func-
tional gastrointestinal disorders. Neurogastroenterol Motil 21: 688-
696, 2009.
16. Hayakawa K, Arakawa T, Kase Y, et al. Liu-Jun-Zi-Tang, a
Kampo medicine, promotes adaptive relaxation in isolated guinea
pig stomachs. Drugs Exp Clin Rev 25: 211-218, 1999.
17. Fujimura J, Haruma K, Hata J, Yamanaka H, Sumii K, Kajiyama
G. Quantitation of duodenogastric reflux and antral motility by
color Doppler ultrasonography. Scand J Gastroenterol 29: 897-
902, 1994.
18. Okamoto E, Haruma K, Hata J, Tani H, Sumii K, Kajiyama G.
Effects of octoreotide, a somatostatin analogue, on gastric function
evaluated by real-time ultrasonography. Aliment Pharmacol Ther
11: 177-184, 1997.
19. Kusunoki H, Haruma K, Hata J, et al. Real-time ultrasonographic
assessment of antroduodenal motility after ingestion of solid and
liquid meals by patients with functional dyspepsia. J Gastroenterol
Hepatol 15: 1022-1027, 2000.
20. Kusunoki H, Haruma K, Hata J, et al. Influence of Helicobacterpylori infection on gastrointestinal motility of dyspeptic patients
―Real-time ultrasonographic study―. Gastroenterology 130(Suppl 2): A433, 2006.
21. Hara M, Hata J, Haruma K, et al. Impaired fundic accommodation
seen in functional dyspepsia. Gut 51 (Suppl III): A188, 2002.
22. Kusunoki H, Haruma K, Hata J, et al. Efficacy of mosapride cit-
rate in proximal gastric accommodation and gastrointestinal motil-
ity in healthy volunteers. A double-blind placebo-controlled ultra-
sonographic study. J Gastroenterol 2010 in press.
23. Hongo M, Fukuhara S, Green J. Shoukaki-ryoiki ni okeru QOL
―nihongo ban GSRS niyoru QOL hyouka―. Shindan to Chiryo
87: 731-736, 1999 (in Japanese).
24. Matsumoto Y, Ito M, Tsuge M, et al. Ecabet sodium induces neu-
ronal nitric oxide synthase-derived nitric oxide synthesis and gas-
tric adaptive relaxation in the human stomach. J Gastroenterol 44:

Inter Med 49: 2195-2202, 2010 DOI: 10.2169/internalmedicine.49.3803
2202
1118-1124, 2009.
25. Tack J, Piessevaux H, Coulie B, Caenepeel P, Janssens J. Role of
impaired gastric accommodation to a meal in functional dyspepsia.
Gastroenterology 115: 1346-1352, 1998.
26. Bouras EP, Delgado-Aros S, Camilleri M, et al. SPECT imaging
of the stomach: comparison with barostat, and effects of sex, age,
body mass index, and fundoplication. Gut 51: 781-786, 2002.
27. Kim DY, Dolgado-Aros S, Camilleri M, et al. Noninvasive mea-
surement of gastric accommodation in patients with idiopathic
nonulcer dyspepsia. Am J Gastroenterol 96: 3099-3105, 2001.
28. Van Den, Elzen BDJ, Bennink RJ, Wieringa RE, Tytgat GNJ,
Boeckxstaens GEE. Fundic accommodation assessed by SPECT
scanning comparison with the gastric barostat. Gut 52: 1548-1554,
2003.
29. Jian R, Ducrot F, Ruskone A, et al. Symptomatic, radionuclide
and therapeutic assessment of chronic idiopathic dyspepsia: A
double-blind placebo-controlled evaluation of cisapride. Dig Dis
Sci 34: 657-664, 1989.
30. Tack J, Broeckaert D, Coulie B, Janssens J. The influence of
cisapride on gastric tone and the perception of gastric distension.
Am J Physiol Gastrointest Liver Physiol 286: G278-G284, 2004.
31. Tack J, Vos R, Janssens J, Salter J, Jauffret S, Vandeplassche G.
Influence of tegaserod on proximal gastric tone and on the percep-
tion of gastric distension. Aliment Pharmacol Ther 18: 1031-1037,
2003.
32. Caldarella MP, Azpiroz F, Malagerada JR. Antro-fundic dysfunc-
tions in functional dyspepsia. Gastroenterology 124: 1220-1229,
2003.
33. Lee KJ, Vos R, Janssens J, Tack J. Influence of duodenal acidifi-
cation on the sensorimotor function of the proximal stomach in
humans. Am J Physiol Gastrointest Liver Physiol 286: G278-
G284, 2004.
34. Tutuian R, Vos R, Karamanolis G, Tack J. An audit of technical
pitfalls of gastric barostat testing in dyspepsia. Neurogastroenterol
Motil 20: 113-118, 2008.
35. Kido T, Nakai Y, Kase Y, et al. Effects of rikkinshi-to, a tradi-
tional Japanese medicine, on the delay of gastric emptying in-
duced by NG-nitro-L-arginine. J Pharmacol Sci 98: 161-167, 2005.
36. Desai KM, Zembowicz A, Sessa WC, Vane JR. Nitroxergic nerves
mediate vagally induced relaxation in the isolated stomach of the
guinea pig. Proc Natl Acad Sci USA 88: 11490-11494, 1991.
37. Galati MM, Monforte MT, Kirjavainen S, Forestieri AM, Trovato
A. Biological effects of hesperidin, a citrus flavonoid (note 1):
anti-inflammatory and analgesic activity. Farmaco 49: 709-712,
1994.
38. Sakata K, Hirose Y, Qiao Z, Tanaka T, Mori H. Inhibition of in-
ducible isoforms of cyclooxygenase and nitric oxide synthase by
flavonoid hesperidin in mouse macrophage cell line. Cancer Lett
199: 139-145, 2003.
39. Tominaga K, Kido T, Ochi M, et al. The traditional Japanese
medicine rikkunshito promotes gastric emptying via the antagonis-
tic action of the 5-HT3 receptor pathway in rat. eCAM: Oct 27: 1-
8, 2009 [Epub ahead of print].
40. Takeda H, Sadakane C, Hattori T, et al. Rikkunshito, an herbal
medcine, suppresses cisplatin-indiced anorexia in rats via 5-HT2
receptor antagonism. Gastroenterology 134: 2004-2013, 2008.
41. Takeda H, Muto S, Hattori T, et al. Rikkunshito ameliorates the
aging-associated decrease in ghrelin receptor reactivity via phos-
phodiesterase III inhibiton. Endocrinology 151: 244-252, 2010.
42. Matsumura T, Arai M, Yonemitsu Y, et al. The traditional Japanese
medicine Rikkunshito increases the plasma level of ghrelin in hu-
man and mice. J Gastroenterol 45: 300-307, 2010.
43. Yakabi K, Kurosawa S, Tamai M, et al. Rikkunshito and 5-HT2C
receptor antagonist improve cisplatin-induced anorexia via hypo-
thalamic ghrelin interaction. Regul Pept 161: 97-105, 2010.
Ⓒ 2010 The Japanese Society of Internal Medicine
http://www.naika.or.jp/imindex.html