Embed Size (px)
Citation preview

Effects of the Manual Lymph Drainage on
Cardiac Autonomic Tone, Lymphedema,
and Quality of Life
Sungjoong Kim
The Graduate School
Yonsei University
Department of Rehabilitation Therapy

Effects of the Manual Lymph Drainage on
Cardiac Autonomic Tone, Lymphedema,
and Quality of Life
A Dissertation
Submitted to the Department of Rehabilitation Therapy
and the Graduate School of Yonsei University
in partial fulfillment of the
requirements for the degree of
Doctor of Philosophy
Sungjoong Kim
June 2008

This certifies that the dissertation of Sungjoong Kim
is approved.
Thesis Supervisor: Ohyun Kwon
Chunghwi Yi
Sanghyun Cho
Hyeseon Jeon
Sunghyun You
The Graduate School
Yonsei University
June 2008

Acknowledgements
This dissertation involved a series of stages towards its completion.
Without the support from many caring people it would not have been possible.
First of all, I thank my God for giving me the courage to purse my dreams, the
strength to endure the difficulties, and the sensitive to acknowledge my
blessings.
I would like to begin by saying how indebted, grateful, and appreciative I
am of my supervisor Professor Ohyun Kwon, who accepted me to study in the
doctorate course and has been a wonderful advisor and mentor. I would not
have been able to complete this dissertation without his thoughtful advice and
support. I am very grateful to Professor Chunghwi Yi for providing this topic,
and sincere advice to improve the quality of this study. I wish to acknowledge
Professor Sanghyun Cho who taught me the right way to get the scientific
method for systemic studies and to be a good scholar, Professor Hyeseon Jeon,
who gave me the warm encouragement and support whenever I was in trouble
and Professor Sunghyun You for always helping expand my knowledge and
complete this dissertation. I also thank Professor Boin Chung, Professor Minye
Jung, and Professor Eunyoung Yoo for providing encouragement.

Furthermore, this dissertation would not have been completed without the
love and support of my family. I cannot fully articulate in words the deep sense
of love I continue to receive from my parents, parents-in-law, and brother. I
dedicate this to them. I especially would like to thank my two daughters,
Sooah and Goeun for being my inspiration and for their patience and
confidence. I sent my heart felt appreciation to grandmother-in-law who took
care of my children for a long time.
Finally, my special gratitude goes to my wife Jungmyo, Shim for giving
me spiritual and moral support in every endeavor. She made sacrifices so that I
could pursue this vision. She was a constant source of encouragement. Thank
you.

- i -
Table of Contents
List of Figures ·····························································································ⅳ
List of Tables ······························································································ⅴ
Abstract ·······································································································ⅵ
ChapterⅠ ········································································································1
Introduction ·······························································································1
Chapter Ⅱ ·······································································································3
Effects of Manual Lymph Drainage on Cardiac Autonomic Tone in
Healthy Subjects (Experiment 1) ······························································3
Introduction ·······························································································3
Method ······································································································6
1. Subjects ·····························································································6
2. Experimental Protocol ·······································································7
3. MLD Procedure ·················································································9
4. ECG Recording and Analysis ·························································10
5. Measuring the PPT ··········································································12
6. Statistical Analysis ··········································································13
Results ·····································································································14
1. Descriptive Characteristics ·····························································14
2. ECG Measure ··················································································16

- ii -
3. PPT Measure ···················································································18
Discussion ·······························································································19
Conclusion ·······························································································23
Chapter Ⅲ ···································································································24
The Long-Term Effects of Manual Lymph Drainage-Based
Complex Decongestive Physical Therapy on Edema and the
Quality of Life in Breast Cancer Patients With Unilateral
Lymphedema (Experiment 2) ··································································24
Introduction ·····························································································24
Method ····································································································28
1. Subjects ···························································································28
2. Experimental Protocol ·····································································30
3. Edema Measurement and Analysis ·················································32
4. Statistical Analysis ··········································································34
Results ·····································································································35
1. Descriptive Characteristics ·····························································35
2. PCEV ·······························································································36
3. Measurement of QOL ······································································38
4. Relationship Between PCEV and QOL ··········································42
Discussion ·······························································································44
Conclusion ·······························································································49
Chapter Ⅳ ···································································································50

- iii -
Summary and Conclusion ·······································································50
References ···································································································51
Abstract in Korean ······················································································64

- iv -
List of Figures
Figure 1. Experimental 1 procedure for the determination of
manual lymph drainage effects on the heart rate
variability and pressure pain threshold ·········································· 8
Figure 2. Pictures before and after treatment ··············································· 37
Figure 3. Mean quality of life scores at baseline, 1 month, and
6 months in the physical functioning, social functioning,
role-physical, and role-emotional domains ·································· 40
Figure 4. Mean quality of life scores at baseline, 1 month, and
6 months in the mental health, vitality, bodily pain,
and general health domains ·························································· 41

- v -
List of Tables
Table 1. Homogeneity test for general characteristics and time-
and frequency-domain parameters of the subjects at baseline ······15
Table 2. Postintervention time-and frequency-domain results in
the experimental and control groups ·············································17
Table 3. Baseline, 1 month, and 6 months quality of life values
assessing functional status and well-being attributes of
patients with unilateral arm lymphedema ·····································39
Table 4. Pearson’s correlations between the percentage excess
volume and quality of life ·····························································43

- vi -
ABSTRACT
Effects of the Manual Lymph Drainage on Cardiac
Autonomic Tone, Lymphedema, and Quality of Life
Sungjoong Kim
Dept. of Rehabilitation Therapy
(Physical Therapy Major)
The Graduate School
Yonsei University
The purpose of this study was to investigate the effects of manual lymph
drainage (MLD) on the cardiac autonomic tone and the long-term physical and
psychological conditions in patients with breast cancer unilateral arm
lymphedema. The study was divided into two experiments. Experiment 1 was
done to investigate the effects of MLD on the cardiac autonomic tone. Thirty-
two healthy male subjects with no drug intake, musculoskeletal disorders,

- vii -
infection, pain, or history of treatment for thrombosis were randomly assigned
to experimental (MLD) and control (rest) group. MLD was applied with a
comfortable pressure for 40 minutes on the neck and abdomen in the
experimental group and the rest was allowed for 40 minutes for the control
group. Autonomic function was determined by time and frequency domain
analysis of heart rate variability (HRV). Data of HRV were recorded with
bipolar electrocardiography (ECG) using standard limb lead. The pressure pain
threshold (PPT) was quantitatively measured using a pressure algometer.
Unpaired t-tests were used to compare the cardiac autonomic tone and the PPT
between experimental and control group. Heart rate variability differed
significantly between the experimental and control group (p<0.05), but the
PPT in the upper trapezius muscle did not (p>0.05). These findings indicate
that the application of MLD was effective in reducing the activity of the
sympathetic nervous system. Experiment 2 was done to ascertain whether
MLD-based complex decongestive physiotherapy (CDP) for upper arm
lymphedema results in long-term changes in edema and quality of life (QOL),
using the SF-36 questionnaire and to determine the whether the treatment-
induced change in the percentage excess volume (PCEV) is correlated with
any changes in QOL. Fifty-three breast cancer patients who had unilateral
lymphedema were treated with MLD-based CDP. PECV and QOL was

- viii -
recorded before and 1 month after MLD-based CDP, and at a 6 months follow-
up visit. One-way analysis of variance (ANOVA) with repeated measures was
used to detect any significant effect of MLD-based CDP on the lymphedema
and QOL. Pearson’s correlation was calculated to examine the relationships
between PCEV and QOL. PCEV in breast cancer patients with lymphedema
was decreased significantly (p<0.05) at 1 month after MLD-based CDP, but it
increased significantly (p<0.05) at 6 months. The QOL scores at 1 and 6
months after MLD-based CDP were significantly higher than the baseline
scores, indicating an improvement in the QOL. Significant changes were also
evident in the single domains of physical functioning, role-physical, mental
health, and general health. The change in PCEV was associated with the
changes in physical functioning, vitality, bodily pain, and general health at 1
and 6 months after MLD-based CDP (p<0.05). Therefore, this study suggests
that QOL significantly improved with upper-arm lymphedema during the
maintenance phase, which was correlated with the reduction in limb volume.

- ix -
Key Words: Cardiac autonomic tone, Complex decongestive physiotherapy,
Lymphedema, Manual lymph drainage, Quality of life.

- 1 -
Chapter ⅠⅠⅠⅠ
Introduction
Manual lymph drainage (MLD), which was developed by a physical
therapist (Dr. Vodder), is a type of skin massage involving a range of
specialized hand movements designed to increase lymph flow and reabsorption
without increasing filtration (Kasseroller 1998; Wittlinger, and Wittlinger
1998). Gentle skin massage is thought to cause superficial lymphatic
contractions, thereby increasing lymph drainage. MLD generally forms the
main part of an intensive treatment regime (Chikly 2001).
The actual techniques of MLD are well documented and firmly established
as a preferred first-line treatment throughout Europe, North America, and
Australia. MLD is commonly prescribed by physicians, who recognize that the
removal of excess fluid expedites the healing process, and can be used in as
many as 60 different indications (Pollot 2001).
Numerous observational ‘before and after’ case studies and case series
published over many years have demonstrated that MLD is effective at
reducing the size of edematous limbs (Boris, Weindorf, and Lasinski 1997;
Foldi, and Foldi 1993; Ko et al. 1998; Olszewski 1991; Sitzia, and Sobrido

- 2 -
1997). MLD can be beneficial in the treatment of both lymphedema and
various other ailments. However, very few reported studies have actually
investigated the various effects of MLD on the body. Despite the increasing
popularity and availability of MLD, most studies into its efficacy have focused
on the physical reduction of edema, and hence the other effects of MLD
remain to be demonstrated.
The purposes of the present study were to elucidate the immediate effects of
MLD on the autonomic nervous system (ANS) in healthy subjects (experiment
1), and the long-term volumetric reductions in unilateral arm lymphedema and
the changes in the quality of life (QOL) after a intensive treatment course of
MLD-based complex decongestive physiotherapy (CDP) (experiment 2).
We hypothesized that in experiment 1 the MLD would (1) change the time-
and frequency-domain parameters of heart-rate variability, (2) decrease the
activities of the ANS and thereby affect the cardiac autonomic tone, and (3)
immediately increase the pressure pain threshold, and that in experiment 2 the
MLD-based CDP would (4) decrease edema and improve the QOL in the
maintenance phase and (5) reveal in a negative correlation between the QOL
and edema.

- 3 -
Chapter ⅡⅡⅡⅡ
Effects of Manual Lymph Drainage on Cardiac
Autonomic Tone in Healthy Subjects
(Experiment 1)
Introduction
Lymphedema is defined as a swelling of the extremity caused by insufficient
lymph drainage. There are two kinds of lymphedema, primary and secondary.
Primary lymphedema results from defects in the lymphatic system and is often
occurred at birth. Secondary can be associated with surgery, trauma, infection,
inflammation, cancer, and radiation (Brennan, DePompolo, and Garden 1996;
Olszewski 1991; Smeltzer, Stickler, and Schirger 1985). Although the exact
pathogenesis of lymphedema is often unclear, in most cases, it is caused by a
failure of the lymph pump (Mortimer 1998).
Lymphedema is not rare and troublesome complication in various medical
conditions such as cancer, trauma and infection. The deformity in body shape
can not be disguised with an ordinary dress; physically uncomfortable activity

- 4 -
and limbs disability are associated with expansion of edema and recurrent
episodes of cellulitis. Because of theses physical symptoms and its nonfetal
nature, patients may experience distress throughout life (Petrek, Pressman, and
Smith 2000). In this situation the sympathetic nervous system arousal is never
“turned off”, which makes the individual more vulnerable to infection (Selye
1978).
The methods for the treatment are debulking or reduction surgery, drug
therapy, MLD-based CDP, compression garments, pneumatic pump, mercury
compression, mesotherapy, ultrasound, elevation, and microwave and laser
therapies (Brennan, and Weitz 1992; Bunce et al. 1994; Cartier, Guilhem, and
Andrieu 1985). The best one of them is MLD-based CDP, which especially
includes MLD (Kasseroller 1998), even in the most advanced stages of
lymphostatic edema. Because it is a gentle, effective, cost-effective, safe, non-
invasive and reliable method that shows good long term results in both primary
and secondary lymphedema (Foldi, and Foldi 1993; Kasseroller 1998;
Olszewski 1991; Wittlinger, and Wittlinger 1998).
MLD affects the treatment of edema and acts on the body in various ways
(Chikly 2001), especially a calming effects on the sympathetic hyperactivity
that results from daily stress, the environment, and other factors (Wittlinger,
and Wittlinger 1998). This means that the appropriate application of MLD to

- 5 -
patients makes them calmer and more relaxed, with MLD having a tonic effect
on the smooth muscle of blood and lymph vessels that possess numerous nerve
endings with connections to the ANS (Foldi, and Foldi 1993; Kasseroller
1998; Weissleder, and Schuchhardt 2001; Wittlinger, and Wittlinger 1998).
That is, MLD is one of the therapies useful for treating lymphedema patients
with stress that result from autonomic-function imbalance. However, no
previous study has investigated the impact of MLD on ANS.
In recent years, noninvasive and sensitive indirect techniques have used
HRV as a marker of changes in the activity of the ANS (Kay 1987; Pagani, and
Malliani 2000; Stein 1994; Zefferino et al. 2003; Zhong et al. 2006). Analysis
of HRV can be used to identify cardiac autonomic disturbances (Kleiger et al.
1987; Pagani et al. 1988) and assess changes in sympathovagal tone in various
psychological (Carney et al. 1995) and emotional (McCraty et al. 1995;
Rechlin et al. 1994) states.
We are not aware of any reports on the effects of MLD on ANS using power
spectral analysis (PSA). In this study we investigated the effects of MLD on
the cardiac autonomic tone and evaluated the PPT as an index of psychological
outcomes of the treatment.

- 6 -
Method
1. Subjects
The sample comprised 32 normal, healthy male volunteers of Young-Dong
University, Republic of Korea. The participants were randomly assigned to an
experimental group (17 subjects) and a control group (15 subjects).
Participants were screened for inclusion/exclusion criteria. The inclusion
criteria were (1) normal skin with no preexisting skin conditions, (2) giving
informed consent, and (3) agreeing to adhere strictly to instructions. The
exclusion criteria included (1) history of treatment for thrombosis, (2)
compromised skin, such as irritation, excessive dryness, known presence of
eczema or psoriasis, or visible adverse condition (rash or infection), and (3)
taking any prescription drugs known to affect the cardiovascular system and
pain relief.

- 7 -
2. Experimental Protocol
Subjects were allowed to rest comfortably for at least 5 minutes prior to the
baseline recording procedure. Brief psychological stress (Kuriyama et al. 2005)
was induced to change the sympathetic activity by performing a serial
subtraction task (100 minus 7) for 2 minutes. Electrocardiography (ECG) was
recorded for 5 minutes, and PPT data were acquired prior to performing MLD.
Subjects in the experimental group received MLD to the neck and abdomen for
40 minutes, while the subjects in the control group relaxed by lying quietly for
the same time period. Data acquisition and MLD took place in a quiet
temperature-controlled environment (22~24℃). Conversation, phone calls,
and noise that could increase the activity of the SNS were minimized, and the
subject’s body was covered with a soft and thin sheet so as to avoid discomfort
from body exposure. ECG and PPT data were acquired immediately following
MLD in the experimental group and in the control group (Figure 1).

- 8 -
Figure 1. Experimental 1 procedure for the determination of manual lymph
drainage (MLD) effects on the heart rate variability and pressure
pain threshold (PPT).

- 9 -
3. MLD Procedure
Subjects were required to undress for MLD. Following baseline recordings,
they remained supine on the massage table. In order to maintain consistency,
an MLD therapist certified by Dr. Vodder’s school and physical therapist with
10 years of experience in the treatment of lymphedema performed MLD by
applying the same standardized procedures to the neck and abdomen. MLD
procedure, which took 40 minutes, employed the technique as described by Dr.
Vodder. The technique was applied in the areas of the neck and abdomen.
MLD procedure used in this study can be found in detail in the Textbook of Dr.
Vodder's Manual Lymph Drainage (Wittlinger, and Wittlinger 1998).
- 10 -
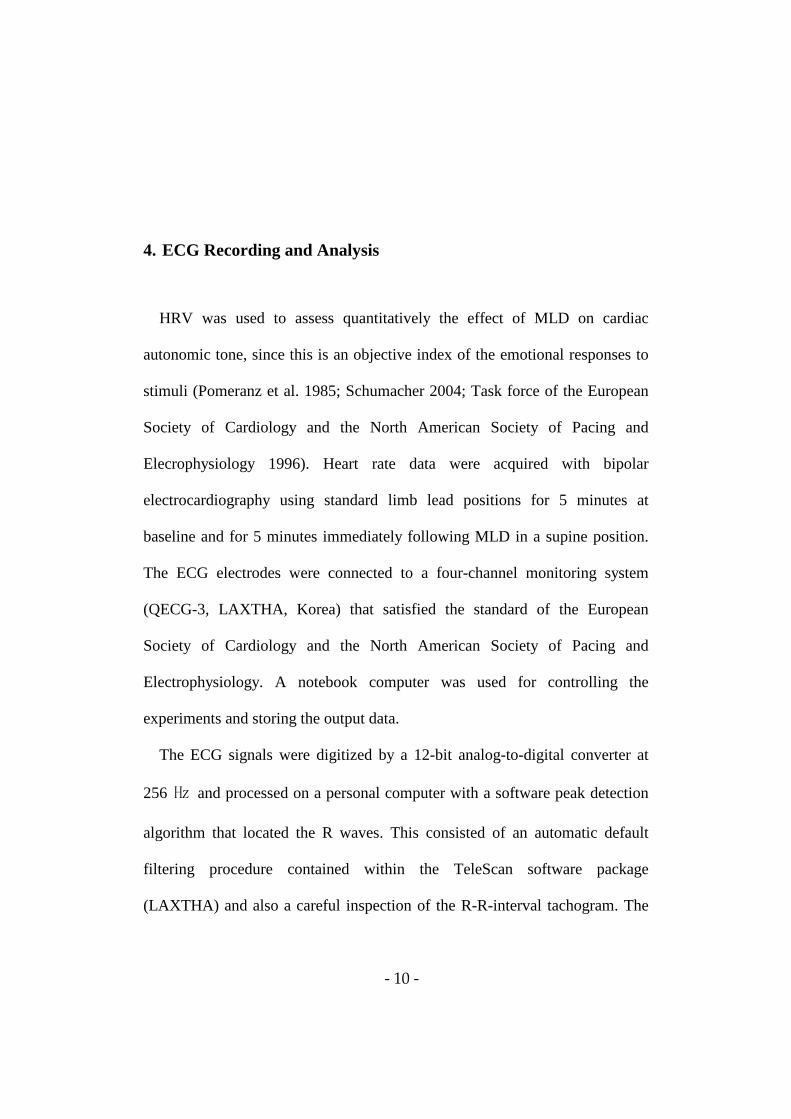
4. ECG Recording and Analysis
HRV was used to assess quantitatively the effect of MLD on cardiac
autonomic tone, since this is an objective index of the emotional responses to
stimuli (Pomeranz et al. 1985; Schumacher 2004; Task force of the European
Society of Cardiology and the North American Society of Pacing and
Elecrophysiology 1996). Heart rate data were acquired with bipolar
electrocardiography using standard limb lead positions for 5 minutes at
baseline and for 5 minutes immediately following MLD in a supine position.
The ECG electrodes were connected to a four-channel monitoring system
(QECG-3, LAXTHA, Korea) that satisfied the standard of the European
Society of Cardiology and the North American Society of Pacing and
Electrophysiology. A notebook computer was used for controlling the
experiments and storing the output data.
The ECG signals were digitized by a 12-bit analog-to-digital converter at
256 ㎐ and processed on a personal computer with a software peak detection
algorithm that located the R waves. This consisted of an automatic default
filtering procedure contained within the TeleScan software package
(LAXTHA) and also a careful inspection of the R-R-interval tachogram. The

- 11 -
tachogram was visually scanned to ensure the complete removal of abnormal
data.
The assessed time-domain indices were the mean heart rate, R-R interval,
the standard deviation of normal-to-normal cardiac interbeat (R-R) intervals
(SDNN), the root mean square of successive differences (RMSSD), and
pNN50%, and the frequency-domain indices were the total power, low
frequency (LF) power, high frequency (HF) power and the LF/HF ratio. Data
were computed off-line using TeleScan software.

- 12 -
5. Measuring the PPT
A pressure algometer was used (Algometer Commander, JTECH Medical,
USA) to determine the changes in muscle tension associated with changes in
ANS. Before the measurements, the subjects were asked to relax in a chair in
an upright position as the investigator explained the procedure to them. To
determine a baseline value, the investigator applied pressure to the upper
trapezius muscle on the dominant side which has received considerable
attention in clinical fields due to the high prevalence of work-related shoulder
and neck disorders (Madeleine et al. 2002; Maeda 1977; Schnoz, Laubli, and
Krueger 2000) until the subject experienced that the sensation of pressure
changed to pain. The pressure was increased at a constant rate of
approximately 0.5 kg/s. The recording was stopped immediately when the
subject reported the sensation change. The entire procedure was repeated three
times, with the mean value calculated for each muscle. Following MLD being
performed for 40 minutes, the PPT of the upper trapezius muscle was
immediately reassessed in the same manner as described above.

- 13 -
6. Statistical Analysis
Descriptive data are expressed here as mean and standard deviation (SD)
values. Testing of all variables using the one-sample Kolmogorov-Smirnov
test revealed that they were normally distributed. An unpaired t-test was used
to test for homogeneity and to compare the experimental group and control
groups for differences in HRV. The collected data were analyzed using
standard statistics software (SPSS ver. 12.0), and a probability of p<0.05 was
considered statistically significant.

- 14 -
Results
1. Descriptive Characteristics
The general characteristics and the time- and frequency-domain parameters
in the study of MLD on the cardiac tone did not differ statistically between the
two groups at baseline (p>0.05) (Table 1).

- 15 -
Table 1. Homogeneity test (mean ±SD) for general characteristics and time-
and frequency-domain parameters of the subjects at baseline
Variable Experimental
group (n1=17)
Control group
(n2=15) t p
Age (years) 21.16±1.24 20.95±1.37 0.46 0.65
Height (cm) 176.10±2.80 175.99±2.43 0.11 0.91
Weight (kg) 73.78±4.61 74.51±3.96 –0.48 0.63
Pressure Pain Threshold (kg) 9.97±2.01 10.15±1.62 –0.27 0.79
Time-domain parameters
Heart rate (beats/minute) 72.71±1.39 72.77±2.03 –0.11 0.91
R-R interval (ms) 834.29±40.69 827.75±17.58 0.58 0.57
Standard deviation of
interbeat intervals (ms) 62.30±2.77 60.50±4.65 1.35 0.19
Root mean square of
successive differences (ms) 38.97±1.43 37.47±9.35 0.65 0.52
pNN50 (%) 5.94±0.50 5.93±0.88 0.06 0.95
Frequency-domain
parameters
Total power (ms2) 2912.59±344.63 2824.20±317.44 0.75 0.45
Low frequency power (ms2) 1512.94±157.52 1555.87±136.91 –0.82 0.42
High frequency power (ms2) 633.47±162.60 656.53±173.61 –0.39 0.70
Low frequency to high
frequency ratio 2.81±0.39 3.01±0.51 –1.32 0.19

- 16 -
2. ECG Measures
The postintervention R-R interval, SDNN, RMSSD, and pNN50 (%) value
were significantly higher in the experimental group than in the control group
(Table 2) (p<0.05). Moreover, the heart rate was significantly reduced in the
experimental group, as indicated by an increase in the average R-R-interval
length (p<0.05). The postintervention total power and LF/HF ratio differed
significantly between the groups (p<0.05), with the latter being significantly
lower in the experimental group.

- 17 -
Table 2. Postintervention time- and frequency-domain results in the
experimental and control groups
Variables Experimental
group (n1=17)
Control group
(n2=15) t p
Time-domain parameters
Heart rate (beats/minute) 68.39±2.11* 71.15±1.45 4.24 0.00
R-R interval (ms) 879.88±51.41 830.35±42.07 2.96 0.01
Standard deviation of interbeat intervals (ms)
70.72±7.52 65.02±4.74 2.53 0.02
Root mean square of successive differences (ms)
50.58±6.31 38.77±10.90 3.81 0.00
pNN50 (%) 7.54±1.27 5.93±0.98 3.98 0.00 Frequency-domain
parameters
Total power (ms2) 3771.47±538.37 3168.07±443.94 3.43 0.00
Low frequency power (ms2) 1844.00±279.50 1817.20±300.77 0.26 0.79
High frequency power (ms2) 1459.18±258.74 1268.73±222.43 2.22 0.03
Low frequency to high frequency ratio
1.28±0.17 1.46±0.28 –2.28 0.03
*mean ±SD.
- 18 -
3. PPT Measures
Pain threshold responses to treatment were assessed as changes in muscle
tension as a result of changes to the ANS according to pressure algometer
results. The mean (±SD) PPT were 11.14±2.32 kg for the experimental group
and 10.18±1.72 kg for the control group. There were no significant differences
between the groups after intervention (p>0.05).

- 19 -
Discussion
This is the first study to examine the effects of MLD using HRV analysis to
measure cardiac autonomic tone in healthy college students. It has been
reported that physical and psychological stress can change HRV; heart rate
being reduced and stabilized during relaxation or proper stimulation (Haker,
Egekvist, and Bjerring 2000). We found that R-R interval, SDNN, RMSSD,
and pNN50 (%) value in time domain were higher in the experimental group,
and heart rate and the LF/HF ratio were lower following MLD application. The
results of the study suggest that MLD for 40 minutes is highly effective in
increasing HRV and cardiac parasympathetic activity in normal subjects. Lee
et al. (2004) have demonstrated that physical and psychological stresses can
reduce the heart rate during experimental measurements. Delaney et al. (2002)
reported a significant increase in HF power following trigger-point massage.
Haker, Egekvist, and Bjerring (2000) also reported that a significant decrease
in the heart rate frequency and increase in the HF component of HRV at the
end of the post-stimulation period by acupuncture. Possibly, these explain the
relaxation, calmness and reduced feelings of distress commonly experienced

- 20 -
by the patients with the increase in PNS activity (Benson, Beary, and Carol
1974).
Not only has massage such as MLD to be used in this study recently become
popular as part of the conservative treatment, but it also received nonobjective
support for reducing pain and alleviating stress, depression, and anxiety in the
context of various physical and psychiatric disorders. The PSA of HRV has
been used as a sensitive index of autonomic nervous activity that provides
quantitative information on autonomic control mechanisms (Malliani et al.
1991; Pagani et al. 1986; Pomeranz et al. 1985; Task force of the European
Society of Cardiology and the North American Society of Pacing and
Elecrophysiology 1996). There are two approaches to measurement of HRV:
analysis in the time (Kleiger et al. 1992) or in the frequency domain (Malliani
et al. 1991; Malliani, Lombardi, and Pagani 1994). These measures are based
on the analysis of interbeat intervals of normal beats. Time domain based on
interbeat intervals includes SDNN, RMSSD and pNN 50 (%). Frequency
domain includes total power, HF, LF and the LF/HF ratio (Malliani et al. 1991;
Schumacher 2004; Stein et al. 1994). HF component of HRV visualize the
component of parasympathetic activity on HRV (between 0.15 and 0.4 Hz),
and LF component of HRV may be considered as a marker sympathetic
activity associated with components around 0.1 Hz on HRV (Benson, Beary,

- 21 -
and Carol 1974; Kay 1987; Stein et al. 1994; Sztajzel 2004). The lower LF/HF
ratios measured in experimental group suggests that vagal drive is increased
when compared to control sessions (p<0.05), this results suggests a shift
toward cardiac parasympathetic activity. MLD may be able to decrease
sympathetic responses and increase parasympathetic responses in the
neuromuscular system (sympathicolytic action).
By stimulating parasympathetic tone, MLD can cause relaxation, antispastic,
and antalgic effects. Light rhythmic stimulation such as MLD of the skin
nonnociceptive receptors may have a pain-inhibiting effect (Pagani et al. 1988).
In the gate control theory of pain, Wall, and Melzack (1994) explain how
nonnoxious sensory stimulation can help to reduce the intensity of pain.
Many clinical applications of the pressure algometer have been documented,
including evaluation (Fischer 1988) and identification of trigger points, and
evaluation of pain sensitivity (Fischer 1987). The PPT of a muscle is the
pressure level at which the patient reports that the feeling of pressure changes
into a painful sensation (Fischer 1987). Autonomic nerves extend to all parts
of the skin; blood vessels, lymphatic vessels, and soft connective tissue ground
substance. Inputs from the special senses acting via the limbic system and
hypothalamus have an effect on the responses of the ANS (Ebner 1985;
Wittlinger, and Wittlinger 1998). Although the PPT was not differed

- 22 -
significantly between the experimental and the control group, there was
increased in pain threshold in the experimental group following MLD from
9.97±2.01 kg to 11.14±2.32 kg.
The present results indicate that sensory stimulation during MLD is
associated with change of various components in the time and frequency
domain of HRV reflecting changed from the sympathetic activity to
parasympathetic activity.
MLD seemed to make the experimental group more comfortable than the
control group. Light, soft, and rhythmical massage can reduce stress in
experimental group, thereby improving their psychological state. These
relaxation factors reduced the HR and stabilized the sympathetic nervous
system, with a corresponding decrease in LF/HF in experimental group
compare to control group. Our study reveals that MLD reduces negative
psychological factors, such as stress, depression, anxiety, compared to the rest.
These effects may induce stabilization of the SNS and cardiac autonomic tone.
Under correct physical therapist’s instruction, MLD could be taught to the
caregivers of lymphedema patients for reducing the physical problems that are
caused by the physical and psychological harmful stress and decreasing the
lymphedema by stimulating the lymphangiomotoricity.

- 23 -
Conclusion
The data presented here suggest that MLD is highly effective in increasing
HRV and cardiac parasympathetic activity in normal subjects, as demonstrated
in the time domain by a decrease in heart rate and increases in SDNN and
RMSSD, and in the frequency domain by an increase in the total power and a
decrease in the LF/HF ratio. These results suggest that MLD could help reduce
stress and improve autonomic function by increasing HRV and
parasympathetic activity. Further study is needed to identify the effects of
MLD on the edema.

- 24 -
Chapter ⅢⅢⅢⅢ
The Long-Term Effects of Manual Lymph Drainage -
Based Complex Decongestive Physical Therapy on
Edema and the Quality of Life in Breast Cancer
Patients With Unilateral Lymphedema
(Experiment 2)
Introduction
The incidence of breast cancer continues to rise in South Korea (Kim 2005).
However, improvements to disease management have led to a well-publicized
recent decline in breast cancer deaths (Peto et al. 2000) and a concomitant
greater emphasis on the side effects of treatment (Pain, Vowler, and
Purushotham 2003). Breast-cancer-related lymphedema due to impaired
lymphatic drainage from the arm secondary to axillary surgery and/or
radiotherapy is one of the common side effects, occurring in 12~28% of cases
(Clark, Sitzia, and Harlow 2005; Meric et al. 2002). Lymphedema is a chronic

- 25 -
condition because it is not possible to reverse the damage responsible for the
swelling. Affected patients have an unsightly, uncomfortable arm that is prone
to repeated episodes of infections, with the rare – but potentially fatal –
complications of secondary lymphangiosarcoma (Foldi 1998). Several physical
and emotional factors are related to lymphedema (MacWayne, and Heiney
2005; Passik, and McDonald 1998), including increased weight of the
edematous limb with restricted motion aggravated by fibrosis and joint
contracture, and altered sensitivity and embarrassment during social
interactions (Didem et al. 2005; Liao et al. 2004).
The main aim of treatment is not cure but to reduce the limb size, usually
via MLD, skin care, remedial exercise, compression garments, pneumatic
pump, mercury compression, elevation, and microwave and laser therapies
(Brennan, and Weitz 1992; Bunce et al. 1994; Cartier, Guilhem, and Andrieu
1985). Treatment involving combined therapies was developed in Europe in
the 1930s and was introduced to South Korea in the 1990s (Kim 2002). One
such treatment, MLD-based CDP is now recognized as an effective
nonsurgical technique for managing lymphedema, and is recommended by the
International Society of Lymphology (Lymphology Executive Committee
1995). Most studies into upper-arm lymphedema have focused on the physical
aspects using volumetric measurements of the limb as the primary tool (Sitzia,

- 26 -
Stanton, and Badger 1997). Since patients with lymphedema experience a wide
range of psychological and physical difficulties, including depression,
embarrassment, resentment, poor body image, impaired limb movement,
impaired physical mobility, and pain (Sitzia, and Sobrido 1997), they would
probably benefit from treatment being assessed using a broader clinical
approach based on the QOL (Pereira de Godoy et al. 2002). Evaluating the
QOL is becoming an increasingly important issue in breast cancer patients
with lymphedema, and the emotional, social, psychological, and sexual effects
of breast cancer treatment have been studied (Ganz 1997; Lee 1997; Moyer
1997).
The SF-36 (Medical Outcome Study 36–Short Form) is a potentially useful
instrument used for evaluating the QOL in cancer patients with lymphedema
(Jager, Doller, and Roth 2006; McKenzie, and Kalda 2003; Pereira de Godoy
et al. 2002; Velanovich, and Szymanski 1999). The SF-36 is potentially useful
instrument to evaluate the QOL and its reliability and validity are well
established (Ware, Kosinski, and Gandek 2004). This measure contains eight
subscales relevant to the health of the individual: physical functioning (PF),
role-physical (RP), role-emotional (RE), mental health (MH), bodily pain (BP),
general health (GH), vitality (VT), and social functioning (SF). The responses
to the SF-36 are transformed into the concepts to provide a scale from zero

- 27 -
(worst possible score) to 100 (i.e., the optimal level of health in that domain)
(Ware, Kosinski, and Gandek 2004). Though a great deal of research has
aimed at understanding the QOL of breast cancer patients with lymphedema,
such interventional studies with MLD-based CDP have generally been
undertaken in small number of patients (Moffatt et al. 2003; Pereira de Godoy
et al. 2002; Sitzia, and Sobrido 1997; Weiss, and Spray 2002), typically less
than 50 in subjects, using nonvalidated QOL tools (McKenzie, and Kalda
2003), or have used a combination of patients with arm and leg edema (Pereira
de Godoy et al. 2002; Sitzia, and Sobrido 1997; Weiss, and Spray 2002). Also,
few papers have reported follow-up assessments of arm lymphedema and QOL
after MLD-based CDP.
The purpose of this study was to ascertain the long-term physical and
psychological impacts of MLD-based CDP treatment for arm lymphedema,
and to determine whether limb volume changes resulting from of MLD-based
CDP treatment are associated with changes in the QOL.

- 28 -
Method
1. Subjects
Data were collected from breast cancer patients who had experienced
lymphedema and who had been referred by a physician for lymphedema
treatment to three outpatient physical therapy clinics in South Korea from
March 1, 2003, through October 30, 2005. The inclusion criteria were as
follows: (1) being female, (2) aged at least 19 years, (3) no known neurological
disorder that would interfere with completion of the measures, (4) able to
complete a questionnaire, (5) no history of treatment for other types of cancer,
(6) no known untreated or unstable medical conditions, (7) no edema in lower
limbs, (8) completed adjuvant chemotherapy, radiation, and surgical treatments
for breast cancer at least 3 months and a most 5 years previously, (9)
agreement to fully receive decongestive treatment five times per week, and
(10) unilateral upper-arm lymphedema. Seventy-eight patients met all of these
eligibility criteria, of which seven refused to participate and three were
excluded since they had active disease and/or were receiving treatment for
recurrent cancer. Five patients did not visit the clinic during the follow-up

- 29 -
period, one patient died, nine patients refused to complete the SF-36 and
volume measurements in follow-up assessments (five patients became too ill
or physically or mentally tired to respond, and four patients declined to
participate due to their personal reasons). The total number of subjects who
successfully complete this study was 53 (N=53, 67.9%).

- 30 -
2. Experimental Protocol
Informed consent was obtained before performing a clinical examination
and documenting general characteristics. Each patient received of MLD-based
CDP treatment, which consisted of a “decongestive phase” that lasted 2–4
weeks, during which the patients received treatment daily. The patients then
followed a “maintenance phase” of self-care for the rest of their lives. The
decongestive phase programs consisted of MLD, compression bandaging,
remedial exercise, and skin care, with each MLD session lasting 45~60
minutes. Treatments were performed by physical therapists certified in
Vodder’s technique of MLD who had at least 5 years of experience of treating
lymphedema. A low-pH skin lotion (Eucerin, Beiersdorf, Norwalk, CT) was
applied prior to bandaging the limb using padding (Artiflex, Beiersdorf) and
low-stretch bandages (Rosidal K, Lohmann, Neuwied, Germany). The protocol
also included teaching the patients to perform self-edema-control activities
(e.g., self-administered MLD, exercise, self-applied bandages or compression
bandage, and skin care) that were to be continued at home in the maintenance
phase. Patients were issued with compression garments as a final component
of the treatment. The protocol in the maintenance phase consisted of wearing
compression bandages or hosiery at all times, a daily session of self-

- 31 -
administered MLD, skin care, and an exercise program. The use of daytime
bandages on at least three days per week was recommended during the
maintenance phase. During the maintenance phase, follow-up visits were
scheduled at 1 month and 6 months after treatment.

- 32 -
3. Edema Measurement and Analysis
A trained physical therapist measured the arm circumference at six locations
(hand, wrist, forearm, elbow, and two locations on the upper arm) using a tape
measure along the lateral aspect in each upper arm (Kim, Yang, and Yi 2000)
before treatment (baseline) and at 1 and 6 months after treatment.
Lymphedema volume was calculated using the truncated cone formula:
volume=H(C2+Cc+c2)/12π, where H=height, C=circumference of the top of
the cone, and c=circumference of the base of the cone (Boris, Weindorf, and
Lasinski 1997; Ko et al. 1998; Weiss, and Spray 2002). This method
demonstrated excellent inter- and intraexaminar reproducibility in comparison
to water displacement, which is considered the gold standard (Galland et al.
2002; Megens et al. 2001).
Each segment was measured three times, and the average reduction in arm
circumference was calculated by the following formula with the unaffected
limb used as a normal control for the affected limb (percentage excess volume;
PCEV): PCEV = [(affected volume – unaffected volume)/unaffected volume]
× 100.
Patients also completed the SF-36 questionnaire (Korean version,
QualityMetric Incorporated, Lincoln, RI) at the initial visit and 1 month after

- 33 -
completion of the decongestive phase, and then at 6 months after treatment in
the clinic.

- 34 -
4. Statistical Analysis
Descriptive data are expressed here as mean and SD values. Testing of all
variables using the one-sample Kolmogorov-Smirnov test revealed that they
were normally distributed. One-way analysis of variance (ANOVA) with
repeated measures was used to detect significant effects of MLD-based CDP
on the lymphedema and QOL. All was three time points: baseline, one-month
post-treatment and 6 months post-treatment. In the event of significant values
of F in the ANOVA, the Bonferroni’s correction test of critical differences was
used to detect significant differences between means. Pearson’s correlation
coefficients were calculated to examine the relationships between the PCEV
and QOL. The collected data were analyzed using standard statistics software
(SPSS ver. 12.0), and a probability of p<0.05 was considered statistically
significant.

- 35 -
Results
1. Descriptive Characteristics
The fifty-three patients in the study of MLD-based CDP on the lymphedema
and QOL were aged 51.0±6.7 years, and their body mass index was 19.0~30.7
(23.9±3.3) kg/m2. Forty-six patients (86.7%) were educated to at least high
school level, and 28 patients (52.8%) were not currently working. The majority
(92.4%) of patients reported a high or moderate economic status, and 44
patients (83.0%) were married. Thirty-four patients (64.2%) had received both
surgery and radiotherapy for cancer, with the length of time since
surgery/radiotherapy being 0.3~4.7 (2.5±1.5) years.

- 36 -
2. PCEV
The PCEV differences between the abnormal and normal arms at baseline, 1
month, and 6 months after treatment were 49.28±21.98%, 28.66±11.29%, and
41.64±17.31%, respectively. The PCEV was higher at baseline than at 1 and 6
months, and was higher at 6 months than at 1 month. However, it generally
decreased significantly during the decongestive and maintenance phases
(p<0.05). Figure 2 is an example of edema reduction in upper lymphedema
after MLD-based CDP.

- 37 -
Figure 2. Pictures before and after treatment. A, lymphedema after
mastectomy before manual lymph drainage - based complex
decongestive physiotherapy. B, The same patient after 1 month of
treatment.

- 38 -
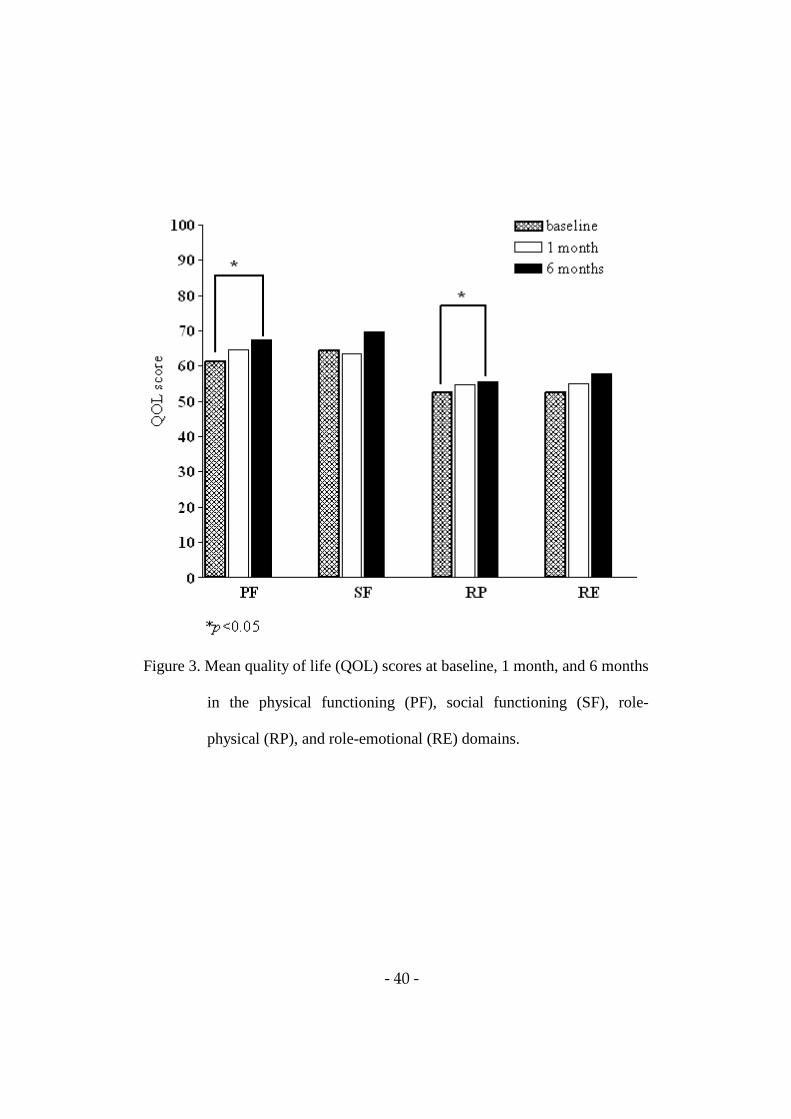
3. Measurement of QOL
Table 3 presents the mean scores of all domains of the SF-36 for the patients.
The scores for the PF (p=0.004), RP (p=0.001), MH (p=0.004), and GH
(p=0.020) domains differed significantly among baseline, 1 month, and 6
months after treatment. Figures 3 and 4 illustrate the differences between the
mean scores after post-hoc test. The scores in the PF, RP, and GH domains
were significantly higher at 6 months after treatment than at baseline,
indicating an improved QOL in these domains at 6 months after treatment. The
score in the MH domain was significantly higher at 1 month after treatment
than at baseline.

- 39 -
Table 3. Baseline, 1 month, and 6 months quality of life values assessing
functional status and well-being attributes of patients with unilateral
arm lymphedema
Baseline 1 month 6 months p
Functional status
Physical functioning 61.25±16.10* 64.68±15.87 67.30±13.51 0.004
Social functioning 64.30±21.83 63.54±18.26 69.59±16.98 0.098
Role-physical 52.34±16.97 54.76±17.18 55.55±14.73 0.001
Role-emotional 52.53±24.90 55.10±16.41 57.81±17.76 0.184
Well-being
Mental health 54.11±16.84 59.47±20.09 58.79±14.79 0.004
Vitality 57.83±18.31 59.53±20.02 59.86±17.70 0.250
Bodily pain 61.28±22.00 63.13±23.53 66.20±22.63 0.782
General health 64.36±16.76 66.85±16.52 71.91±19.29 0.020
* mean ±SD.
- 40 -
Figure 3. Mean quality of life (QOL) scores at baseline, 1 month, and 6 months
in the physical functioning (PF), social functioning (SF), role-
physical (RP), and role-emotional (RE) domains.

- 41 -
Figure 4. Mean quality of life (QOL) scores at baseline, 1 month, and 6 months
in the mental health (MH), vitality (VT), bodily pain (BP), and
general health (GH) domains.
- 42 -
4. Relationship Between PCEV and QOL
The PCEV of edema was negatively correlated with SF-36 subscales (Table
4), including functioning at baseline (r=–0.55, p<0.01), 1 month after
treatment (r=0.46, p<0.01), and 6 months after treatment (r=–0.50, p<0.01),
VT at 1 month (r=–0.27, p<0.05) and 6 months after treatment (r=–0.42,
p<0.05), BP at 1 month (r=–0.28, p<0.015) and 6 months after treatment (r=–
0.51, p<0.01), and GH at 1 month (r=–0.30, p<0.05) and 6 months after
treatment (r=–0.55, p<0.01).

- 43 -
Table 4. Pearson’s correlations between the percentage excess volume and
quality of life
Before (baseline) 1 month 6 months
Functional status
Physical functioning –0.55** –0.46** –0.50**
Social functioning –0.18 –0.25 –0.18
Role-physical –0.19 –0.10 –0.16
Role-emotional –0.26 –0.15 –0.11
Well-being
Mental health –0.22 –0.23 –0.50
Vitality –0.15 –0.27* –0.42*
Bodily pain –0.19 –0.28* –0.51**
General health –0.19 –0.30* –0.55** *p<0.05; ** p<0.01.

- 44 -
Discussion
Lymphedema can be viewed as a QOL issue due to the difficulties in causes
in functioning at work or at home, altered body image, low self-esteem,
difficulty dressing, and a loss of interest in social activities (Carter 1997; Sitzia,
and Sobrido 1997; Wood, Tobin, and Mortimor 1995). This study was
undertaken to examine whether the QOL at long-term follow-up was improved
in breast cancer patients with lymphedema following MLD-based CDP, and
whether limb volume changes were associated with any detected changes in
the QOL.
During the decongestive phase, we noted that the PCEV decreased from
49.29±21.98% at baseline to 28.66±11.29% at 1 month after treatment. The
percentage reduction in the lymphedema volume has varied from 20% to 80%
in previously published series, but these have employed diverse calculation
formulas (e.g., in terms of the perimeter measures used and different intervals
between the two measures) (Boris, Weindorf, and Lasinski 1994; Casley-Smith,
and Casley-Smith 1992; Foldi, Foldi, and Clodius 1989; Ko et al. 1998). There
was a small increase in the lymphedema volume during the maintenance phase.
Boris, Weindorf, and Lasinski (1997) reported that the maintenance of reduced

- 45 -
lymphedema volume depend on the compliance. Foldi, Foldi, and Clodius
(1989) found in a 3-year follow-up that more than 50% of the patients
maintained the initial reduction in lymphedema obtained after the decongestive
phase.
We found that the self-reported PF, RP, MH, and GH scores were
significantly changed by MLD-based CDP treatment. Sitzia, and Sobrido
(1997) reported similar improvements in the QOL of patients following MLD
with multilayered bandaging or simple massage with multilayered bandaging.
Based on the Nottingham Health Profile Part 1 (NHP-1), they reported that
patients had the greatest improvement in physical attributes. They also
concluded that the NHP-1 was useful in assessing physical aspects of the QOL,
but less helpful with regard to psychological and emotional attributes. In
contrast, we found that using the SF-36 resulted in the detection of significant
changes in physical, functional, and psychosocial posttreatment measures.
Weiss, and Spray (2002) also reported the MLD-based CDP improved the
QOL of patients with peripheral lymphedema due to various causes. The trend
toward increases in PF scores in the study participants supports the theory that
MLD-based CDP is beneficial for women with secondary lymphedema after
breast cancer treatment. Subjects expressed greater confidence in using their
affected arm for activities of daily living, and some mentioned that they were

- 46 -
again able to lift objects with the affected arm after the decongestive phase.
This may explain the trend toward increased RP, MH, and GH scores, in as
much as the subjects were less aware of their disease, were confident that
MLD-based CDP prevents the edema from increasing, and therefore felt
healthier overall. Although the lymphedema volume was increased at 6 months,
the data showed trends toward increases in almost all domains of the SF-36. A
recent similar study (Mondry, Riffenburgh, and Johnstone 2004) investigated
the long-term effects of MLD-based CDP in 20 patients with breast-cancer-
related lymphedema, and found similar results for QOL: there was no
significant change in QOL immediately after treatment, but QOL scores had
consistently increased by 6 months. These observations suggest that MLD-
based CDP programs improve the QOL .
The study reported here differs from previous evaluations (Pereira de Godoy
et al. 2002; Weiss, and Spray 2002) of changes in the QOL in lymphedema
patients following MLD-based CDP, in that it included only breast cancer
patients with lymphedema and reported follow-up assessments of QOL after
MLD-based CDP. In contrast, the studies of Pereira de Godoy et al. (2002) and
Weiss, and Spray (2002) involved patients with multiple diseases (and only a
small number of breast cancer patients with lymphedema) and reported only
short-term results.

- 47 -
Despite MLD-based CDP inducing significant edema volume reductions,
the results from this study did not support an association between limb volume
reduction and scores in any of the domains of the SF-36 except for the PF
score at baseline, an association between limb volume reduction and scores
that is supported by Mondry, Riffenburgh, and Johnstone (2004), Sitzia,
Stanton, and Badger (1997), and Weiss, and Spray (2002). But the significant
correlations at 1 and 6 months after treatment (i.e., in the maintenance phase)
support an association with PF, VT, BP, and GH. The lack of association
suggests that a reduction in the edema volume is only partly responsible for an
improvement in the QOL. It is therefore reasonable to postulate that education
programs for edema control influence the association between limb volume
reduction and the QOL. These data highlight the importance of broadening
care to treat these patients beyond the physical aspect of lymphedema, and they
also suggest that more-effective treatment of the physical condition increases
the likelihood of the emotional and social statuses also improving. Nonetheless,
a multidisciplinary approach is desirable for optimizing the QOL of a patient
with lymphedema.
The main strengths of our study were to deal only with patients with
lymphedema after breast cancer. The treatment was homogeneous and
provided by physiotherapists who specialized in lymphology. The intensive

- 48 -
treatment program allowed education, giving advice about avoiding infection
such as cellulitis, and learning self-bandaging and self-administered MLD.
However, the limitations of this study mean that its results must be interpreted
cautiously. These included the absence of a nontreatment control group, which
meant that the effects of MLD-based CDP on the QOL could not be
distinguished from the effects of simply participating in a clinical research
study. Moreover, the extent to which improvements in edema volume and the
QOL are attributable to poor internal validity factors such as measurement
errors, testing effects, and statistical regression could not be determined.
Twenty-five (32.0%) of the original sample of 78 patients were missed during
follow-up, of whom 9 withdrew due to recurrent cancer, death, illness, or
fatigue, and the others did not complete the study due to poor motivation. We
consider this to be an acceptable attrition rate for a sample of mostly older
women who had received treatment for breast cancer. In such populations the
persuasive power of the researchers may be very important to ensuring active
participation by patients. Although the loss to follow-up might have introduced
bias, our findings suggest that the MLD-based CDP program induced
lymphedema management that had a substantial impact on the QOL.

- 49 -
Conclusion
The data presented here suggest that MLD-based CDP reduce the
lymphedema in breast cancer patients with unilateral lymphedema. PF, RP,
MH, and GH scores in the maintenance phase were significantly higher than
the pre-treatment scores and QOL correlated with the reduction in limb
volume in the domain of PF, VT, BP, and GH. The findings reported here
emphasize the effect of MLD-based CDP to reduce the edema and the need to
evaluate the long-term QOL in patients with lymphedema, and not merely to
measure the limb volume. Further studies are needed to compare the effects of
different modalities of treatment on the QOL of patients with various
characteristics and clinical symptoms.

- 50 -
Chapter ⅣⅣⅣⅣ
Summary and Conclusion
MLD can increase parasympathetic activity and decrease sympathetic
activity through stabilization of the autonomic system. Therefore, it can reduce
the physical problems that are caused by the physical and psychological
harmful stress and decrease the lymphedema by stimulating the contraction of
lymphatic vessels whose activities are regulated by the ANS.

- 51 -
References
Benson H, Beary JF, and Carol MP. The relaxation response. Psychiatry. 1974;37(1):
37-46.
Boris M, Weindorf S, Lasinski B, and Boris G. Lymphedema reduction by
noninvasive complex lymphedema therapy. Oncology. 1994;8(9): 95-106.
Boris M, Weindorf S, and Lasinski S. Persistence of lymphedema reduction after
non-invasive complex lymphedema therapy. Oncology. 1997;11(1):99-114.
Brennan MJ, DePompolo RW, and Garden FH. Focused review: Postmastectomy
lymphedema. Arch Phys Med Rehabil. 1996;77(3 Suppl):S74-S80.
Brennan MJ, and Weitz J. Lymphedema 30 years after radical mastectomy. Am J
Phys Med Rehabil. 1992;71(1):12-14.
Bunce IH, Mirolo BR, Hennessy JM, Ward LC, and Jones LC. Post-mastectomy
lymphoedema treatment and measurement. Med J Aust. 1994;161(2):125-128.

- 52 -
Carney RM, Saunders RD, Freedland KE, Stein P, Rich MW, and Jaffe AS.
Association of depression with reduced heart rate variability in coronary artery
disease. Am J Cardiol. 1995;76(8):562-564.
Carter BJ. Women’s experiences of lymphedema. Oncol Nurs Forum.
1997;24(5):875-882.
Cartier CJ, Guilhem JR, and Andrieu RC. Lymphedema treatment using hydrostatic
pressure of mercury. Prog Lymphol. 1985;10:173-175.
Casley-Smith JR, and Casley-Smith JR. Modern treatment of lymphoedema. I.
Complex physical therapy: the first 200 Australian limbs. Australas J Dermatol.
1992;33(2): 61-68.
Chikly B. Theory of Practice of Lymph Drainage Therapy, 1st ed. Arizona :
International Health & Healing Inc. 2001.
Clark B, Sitzia J, and Harlow W. Incidence and risk of arm oedema following
treatment for breast cancer: a three-year follow-up study. QJM. 2005;98(5): 343-
348.

- 53 -
Delaney JP, Leong KS, Watkins A, and Brodie D. The short-term effects of
myofascial trigger point massage therapy on cardiac autonomic tone in healthy
subjects. J Adv Nurs. 2002;37(4):364-371.
Didem K, Ufuk YS, Serdar S, and Zumre A. The comparison of two different
physiotherapy methods in treatment of lymphedema after breast surgery. Breast
Cancer Res Treat. 2005;93(1):49-54.
Ebner M. Connective Tissue Manipulation: Theory and Therapeutic Application, 3rd
ed. Florida : Krieger Pub Co. 1985.
Fischer AA. Pressure algometry over normal muscles. Standard values, validity, and
reproducibility of pressure threshold. Pain. 1987;30(1):115-126.
Fischer AA. Documentation of myofascial trigger points. Arch Phys Med Rehabil.
1988;69(4):286-291.
Foldi E. Treatment of lymphedema and patient rehabilitation. Anticancer Res.
1998;18(3C):2211-2212.
Foldi M, and Foldi E. Lymphoedema: Methods of Treatment and Control, 1st ed.
Australia : Lymphoedema Association of Victoria Inc. 1993.

- 54 -
Foldi E, Foldi M, and Clodius L. The lymphedema chaos: a lancet. Ann Plast Surg.
1989;22(6):505-515.
Galland C, Auvert JF, Flahault A, and Vayssairat M. Why and how post-mastectomy
edema should be quantified in patients with breast cancer. Breast Cancer Res
Treat. 2002;75(1):87-89.
Ganz PA. Sexual functioning after breast cancer: a conceptual framework for future
studies. Ann Oncol. 1997;8(2):105-107.
Harker E, Egekvist H, and Bjerring P. Effect of sensory stimulation (acupuncture) on
sympathetic and parasympathetic activities in healthy subjects. J Auton Nerv Syst.
2000;79(1):52-59.
Jager G, Doller W, and Roth R. Quality-of-life and body image impairments in
patients with lymphedema. Lymphology. 2006;39(4):193-200.
Kasseroller RG. The Vodder School: the Vodder method. Cancer.1998;83(12
Suppl):2840-2842.

- 55 -
Kay SM. Modern Spectral Estimation: Theory and Application, 1st ed. NJ : Prentice-
Hall Englewood Cliffs. 1987.
Kim GT. Cancer incidence in Korea 1999-2001, Seoul : Ministry of Health and
Welfare. 2005.
Kim SJ. Lymphedema, 1st ed. Seoul : Jungdam Media Publishing Co. 2002.
Kim SJ, Yang HS, and Yi CH. Intertester and Intratester Reliability of Tape
Measurement on Lower Extremities. J Korean Acad Univ Trainde Phys
Therapists. 2000;7(1):38-45.
Kleiger RE, Miller JP, Bigger JT Jr, and Moss AJ. Decreased heart rate variability
and its association with increased mortality after acute myocardial infarction. Am
J Cardiol. 1987;59(4):256-262.
Kleiger RE, Stein PK, Bosner MS, and Rottman JN. Time domain measurement of
heart rate variability. Cardiol Clin. 1992;10(3):487-498.
Ko DS, Lerner R, Klose G, and Cosimi AB. Effective treatment of lymphedema of
the extremities. Arch Surg. 1998;133(4):452-458.

- 56 -
Kuriyama H, Watanabe S, Nakaya T, Shigemori I, Kita M, Yoshida N, Masaki D,
Tadai T, Ozasa K, Fukui K, and Imanishi J. Immunological and Psychological
Benefits of Aromatherapy Massage. Evid Based Complement Alternat Med.
2005;2(2):179-184.
Lee CO. Quality of life and breast cancer survivors. Psychosocial and treatment
issues. Cancer Pract. 1997;5(5):309-316.
Lee MS, Kim HJ, Song J, Park KW, and Moon SR. Effects of multifunctional fabrics
on cardiac autonomic tone and psychological state. Int J Neurosci.
2004;114(8):923-931.
Liao SF, Huang MS, Li SH, Chen IR, Wei TS, Kuo SJ, Chen St, and Hsu JC.
Complex decongestive physiotherapy for patients with chronic cancer-associated
lymphedema. J Formos Med Assoc. 2004;103(5):344-348.
Lymphology Executive Committee. The diagnosis and treatment of peripheral
lymphedema. Consensus document of the International Society of Lymphology
Executive Committee. Lymphology. 1995;28(3):113-117.
MacWayne J, and Heiney SP. Psychologic and social sequelae of secondary
lymphedema: a review. Cancer. 2005;104 (3):457-466.

- 57 -
Madeleine P, Farina D, Merletti R, and Arendt-Nielsen L. Upper trapezius muscle
mechanomyographic and electromyographic activity in humans during low force
fatigue and non-fatiguing contractions. Eur J Appl Physiol. 2002;87(4-5):327-336.
Maeda K. Occupational cervicobrachial disorder and its causative factors. J Hum
Ergol.1977;6(2):193-202.
Malliani A, Lombardi F, and Pagani M. Power spectrum analysis of heart rate
variability: a tool to explore neural regulatory mechanism. Br Heart J. 1994;71(1):
1-2.
Malliani A, Pagani M, Lombardi F, and Cerutti S. Cardiovascular neural regulation
explored in the frequency domain. Circulation. 1991;84(2):482-492.
McCraty R, Atkinson M, Tiller WA, Rein G, and Watkins AD. The effects of
emotions on short-term power spectrum analysis of heart rate variability. Am J
Cardiol. 1995;76(14):1089-1093.
McKenzie DC, and Kalda AL. Effect of upper extremity exercise on secondary
lymphedema in breast cancer patients: a pilot study. J Clin Oncol.
2003;21(3):463-466.

- 58 -
Megens AM, Harris SR, Kim-Sing C, and McKenzie DC. Measurement of upper
extremity volume in women after axillary dissection for breast cancer. Arch Phys
Med Rehabil. 2001;82(12):1639-1644.
Meric F, Buchholz TA, Mirza NQ, Vlastos G, Ames FC, Ross MI, Pollock RE,
Singletary SE, Feig BW, Kuerer HM, Newman LA, Perkins GH, Strom EA,
McNeese MD, Hortobagyi GN, and Hunt KK. Long-term complications
associated with breast-conservation surgery and radiotherapy. Ann Surg Oncol.
2002;9(6):543-549.
Moffatt CJ, Franks PJ, Doherty DC, Williams AF, Badger C, Jeffs E, Bosanquet N,
and Mortimer PS. Lymphoedema: an underestimated health problem. QJM.
2003;96(10):731-738.
Mondry TE, Riffenburgh RH, and Johnstone PA. Prospective trial of complete
decongestive therapy for upper extremity lymphedema after breast cancer therapy.
Cancer J. 2004;10(1):42-48.
Mortimer PS. The pathophysiology of lymphedema. Cancer. 1998;83(12
Suppl):2798-2802.

- 59 -
Moyer A. Psychosocial outcomes of breast-conserving surgery versus mastectomy: a
meta-analytic review. Health Psychol. 1997;16(3):284-298.
Olszewski WL. Lymph Stasis: Pathophysiology, Diagnosis and Treatment, 1st ed.
Florida : CRC Press. 1991.
Pagani M, Lombardi F, Guzzetti S, Rimoldi O, Furlan R, Pizzinelli P, Sandrone G,
Malfatto G, Dell'Orto S, and Piccaluga E, Turiel M, Baselli G, Cerutti S, and
Malliani A. Power spectral analysis of heart rate and arterial pressure variabilities
as a marker of symphatho-vagal interaction in man and conscious dog. Circ
Res.1986;59(2):178-193.
Pagani M, Malfatto G, Pierini S, Casati R, Masu AM, Poli M, Guzzetti S, Lombardi
F, Cerutti S, and Malliani A. Spectral analysis of heart rate variability in the
assessment of autonomic diabetic neuropathy. J Auton Nerv Syst. 1988;23(2):143-
153.
Pagani M, and Malliani A. Interpreting oscillations of muscle sympathetic nerve
activity and heart rate variability. J Hypertens. 2000;18(12):1709-1719.

- 60 -
Pain SJ, Vowler SL, and Purushotham AD. Is physical function a more appropriate
measure than volume excess in the assessment of breast cancer-related
lymphoedema (BCRL)? Eur J Cancer. 2003;39(15):2168-2172.
Passik SD, and McDonald MV. Psychosocial aspects of upper extremity lymphedema
in women treated for breast carcinoma. Cancer. 1998;83(12 Suppl Am):2817-
2820.
Pereira de Godoy JM, Braile DM, de Fatima Godoy M, and Longo O Jr. Quality of
life and peripheral lymphedema. Lymphology. 2002;35(2):72-75.
Peto R, Boreham J, Clarke M, Davies C, and Beral V. UK and USA breast cancer
deaths down 25% in year 2000 at ages 20-69 years. Lancet. 2000;355(9217):1822.
Petrek JA, Pressman PI, and Smith RA. Lymphedema: Current Issues in research and
management. CA Cancer J Clin. 2000;50(5):292-307.
Pollot PJ. Lymphedema , Finding the Holistic Approach, 1st ed. NY. 2001.
Pomeranz B, Macaulay RJ, Caudill MA, Kutz I, Adam D, Gordon D, Kilborn KM,
Barqer AC, Shannon DC, and Cohen RJ. Assessment of autonomic function in
humans by heart rate spectral analysis. Am J Physiol.1985;248(1 Pt 2):H151-H153.

- 61 -
Rechlin T, Weis M, Spitzer A, and Kaschka WP. Are affective disorders associated
with alterations of heart rate variability? J Affect Disord. 1994;32(4):271-275.
Schnoz M, Laubli T, and Krueger H. Co-activation of the trapezius and upper arm
muscle with finger tapping at different rates and trunk postures. Eur J Appl
Physiol. 2000;83(2-3):207-214.
Schumacher A. Linear and nonlinear approaches to the analysis of R-R interval
variability. Bio Res Nurs. 2004;5(3):211-221.
Selye H. The Stress of Life, 2nd ed. New York : McGraw-Hill. 1978. Sitzia J, and Sobrido L. Measurement of health-related quality of life of patients
receiving conservative treatment for limb lymphoedema using Nottingham Health
Profile. Qua Life Res. 1997;6(5):373-384.
Sitzia J, Stanton AW, and Badger C. A review of outcome indicators in the treatment
of chronic limb oedema. Clin Rehabil. 1997;11(3):181-191.
Smeltzer DM, Stickler GB, and Schirger A. Primary lymphedema in children and
adolescents: A follow-up study and review. Pediatrics. 1985;76(2):206-218.

- 62 -
Stein PK, Bosner MS, Kleiger RE, and Conger BM. Heart rate variability: A measure
of cardiac autonomic tone. Am Heart J. 1994;127(5):1376-1381.
Sztajzel J. Heart rate variability: a noninvasive electrocardiographic method to
measure the autonomic nervous system. Swiss Med Wkly. 2004;134(35-36):514-
522.
Task Force of the European Society of Cardiology and the North American Society
of Pacing and Electrophysiology. Heart rate variability: Standards of measurement,
physiological interpretation, and clinical use. Circulation. 1996;93(5):1043-1065.
Velanovich V, and Szymanski W. Quality of life of breast cancer patients with
lymphedema. Am J Surg. 1999;177(3):184-187.
Wall PD, and Melzack R. Textbook of Pain, 3rd ed. Edinburgh : Churchill
Livingstone. 1994.
Ware JE, Kosinski M, Gandek B. SF-36 Health Survey: Manual & interpretation
guide, 1st ed. Lincoln : QualityMetric Incorporated. 2004.
Weiss JM, and Spray BJ. The effect of complete decongestive therapy on the quality
of life of patients with peripheral lymphedema. Lymphology. 2002;35(2):46-58.

- 63 -
Weissleder H, and Schuchhardt C. Lymphedeam: Diagnosis and Therapy, 3rd ed.
Koln : Viavital Verlag GmbH. 2001.
Wittlinger H, and Wittlinger G. Textbook of Dr. Vodder's manual lymph drainage,
6th ed. Heidelberg : Karl F. Haug Publishers. 1998.
Woods M, Tobin M, and Mortimor P. The psychosocial morbidity of breast cancer
with lymphoedema. Cancer Nurs. 1995;18(6);467-471.
Zefferino R, L'Abbate N, Facciorusso A, Potenza A, Lasalvia M, Nuzzaco A, Di
Biase M, and Ambrosi L. Assessment of heart rate variability (HRV) as a stress
index in an emergency team of urban police. G Ital Med Lav Ergon. 2003;25(3
Suppl):167-169.
Zhong Y, Jan KM, Ju KH, and Chon KH. Quantifying cardiac sympathetic and
parasympathetic nervous activities using principal dynamic modes analysis of
heart rate variability. Am J Physiol Heart Circ Physiol. 2006;291(3):H1475-
H1483.

- 64 -
국문 요약
MLD 가가가가 심장심장심장심장 자율신경자율신경자율신경자율신경 긴장도긴장도긴장도긴장도, 림프부종림프부종림프부종림프부종, 그리고그리고그리고그리고
삶의삶의삶의삶의 질에질에질에질에 미치는미치는미치는미치는 영향영향영향영향
연세대학교 대학원
재활학과(물리치료학 전공)
김 성 중
본 연구의 목적은 MLD 가 심장 자율신경 긴장도와 편측 상지
림프부종이 있는 유방암 환자의 장기적 신체적, 정신적 상태에 미치는
영향을 알아보는 것이었다. 연구는 두 단계로 나뉘어 실시되었다. 연구
1 은 MLD 가 심장 자율신경 긴장도에 미치는 영향을 조사하는 것이었다.
약 복용, 근골격계 질환, 감염, 통증, 또는 혈전 치료에 대한 병력이 없는
32 명의 건강한 성인 남자를 무작위로 실험(MLD)군과 대조(휴식)군에
무작위로 할당하였다. 실험군에는 MLD 를 40 분 동안 목과 복부에 편안한
압력으로 적용하였고 대조군은 40 분간 안정을 취하도록 하였다. 자율신경

- 65 -
기능을 심박수 변이도의 시간과 주기 영역 분석을 이용하여 측정하였으며
자료는 표준 사지유도법을 이용하여 심전도로 기록 되었다. 압통역치는
통각측정기를 이용하여 정량적으로 측정하였다. 실험군과 대조군의 심장
자율신경 긴장과 압통역치를 비교하기 위해 독립 t 검정을 사용하였다.
심박수 변이도는 실험군과 대조군에서 통계적으로 유의한 차이를
보였으나(p<0.05), 상부 승모근에서의 압통 역치는 유의한 차이를 보이지
않았다 (p>0.05). 이런 결과는 MLD 적용이 자율신경계 활동성을
감소시키는데 효과가 있다는 것을 의미한다. 연구 2 는 MLD-기반 복합적
부종 감소 물리치료가 상지 림프부종에 장기적으로 부종과 SF-36
설문지를 이용한 삶의 질 평가에 어떠한 영향이 있는지를 알아보고
치료로 인한 부종 과용적률의 변화와 삶의 질 변화가 어떤 상관성이
있는지를 알아보았다. 53 명의 편측 림프부종을 가지고 있는 유방암
환자에게 MLD-기반 복합적 부종 감소 물리치료를 실시하였다. 부종
과용적률과 삶의 질을 치료 전, 치료 후 1 달, 그리고 6 개월 후에
측정하였다. MLD-기반 복합적 부종 감소 물리치료가 림프부종과 삶의
질에 어떤 유의한 효과가 있는지를 반복 측정된 일요인 분산분석으로
알아보았고 부종 과용적률과 삶의 질과의 상관성은 피어슨 상관계수를
이용하였다. 림프부종이 있는 유방암 환자의 부종 과용적률은 치료 한달
후에는 유의하게 감소하였으나 (p<0.05) 6 개월 후에는 유의하게

- 66 -
증가하였다 (p<0.05). 삶의 질 점수는 치료 시작 전보다 치료 후 한달
그리고 6 개월 후에 유의하게 향상되어 삶의 질이 개선되었음을 알 수
있었다. 신체적 기능, 신체적 역할, 정신 건강, 그리고 일반적 건강의 개별
영역에서 유의한 변화를 보였다. 부종 과용적률의 변화는 치료 후 한 달과
6 개월 후에서 신체적 기능, 활력, 신체 통증, 그리고 일반적 건강과
상관관계가 있는 것으로 나타났다. 결국, 본 연구는 상지 림프부종이 있는
환자의 부종 유지기 동안에 체지 용적 감소와 상관관계가 있는 삶의 질이
MLD-기반의 치료를 통해 개선이 되었다는 것을 보여 주었다.

- 67 -
핵심되는 말: 림프부종, 복합적 부종감소 물리치료, 삶의 질, 심장
자율신경 긴장도, MLD.