Embed Size (px)
Citation preview

Effects of Percutaneous Transluminal Coronary Angioplasty: lntracoronary Thrombolysis with Urokinase in
Acute Myocardial Infarction
MASAO YASUNO, MD, YOSHIHIKO SAITO, MD, MORIHARU ISHIDA, MD,
KATSUHIRO SUZUKI, MD, SHIGFKI ENDO, MD, and MASAAKI TAKAHASHI, MD
Coronary angiography and percutaneous translu- minal coronary angk@asty (PTCA) were performed in 32 patients with evolving acute myocardial in- farction. Cf the 25 patients with complete occlusion of an infarct-related coronary artery, in 18 (72%) the occluded vessel was successfully opened by an intracoronary infusion of urokinase. With a small dose of urokinase the successful recanallzatton was achieved in only 25%; with a larger dose it was achieved in 94 % . After PTCA, all patients received glucose-insulin-potassium solution for 76 hours. Repeat angiography 42 days later showed a patent coronary artery tn 12 (group A) of 18 patients with
successful PTCA. In group A, left ventricular ejection fraction increased from 51 f 13% to 72 f 10% (p <O.Ol) and regional wall shortening from 4.5 f 9.5% to 29 f 19% (p <O.Ol). In contrast, these variables did not change signtficantty in patients with unsuccessful PTCA or late reocclusion of an in- farct-related vessel (group 6). These data suggest that successful PTCA with sustained patency of an infarct-related coronary artery has a beneficial ef- fect on the salvage of the jeopardized myocardium, and glucose-insulin-potassium therapy may enhance the beneficial effect of PTCA.
(Am J Cardiol 1984;53:1217-1220)
Since the initial reports of Rentrop et all and Ganz et a1,2 percutaneous transluminal coronary angioplasty (PTCA) during the acute phase of evolving myocardial infarction (MI) has been rapidly accepted as 1 of the most important therapeutic methods of protecting myocardial tissue and reducing overall mortality. Sev- eral studies3-lo have reported a significant, although slight, improvement of the left ventricular (LV) func- tion by this therapy. In these reports, streptokinase alone or streptokinase in combination with human plasmin is used as the thrombolytic agent. In Japan, PTCA has been performed with the use of urokinase, and overall success rate of coronary recanalization is reported to be 65%. With a small dose of urokinase (<240,000 units), thrombolysis was achieved in only 28%; at a higher dose (240,000 to 480,000 units), it was achieved in 60% and in 79% (>480,000 unit&l1 How- ever, there are no reports of the beneficial effects of PTCA with the use of urokinase on LV function. This
From the Division of Internal Medicine, Shiruoka Rosai Hospital, Hamamatsu City, Japan. Manuscript received Dctober 3, 1983; revised manuscript received January 20, 1984, accepted January 23, 1984.
Address for reprints: Mesa0 Yasuno, MD, Division of internal Medi- cine, Shizuoka Rosai Hospital, 25 Shogen-cho, Hamamatsu City 430, Japan.
study evaluates the beneficial effects of intracoronary application of urokinase on LV function.
Methods
Patients: The study patients consisted of 32 consecutive patients with MI who were admitted to the Shizuoka Rosai Hospital between January 1981 and June 1983 and who re- ceived PTCA within an average of 3.9 hours (range 1.5 to 8) after the onset of symptoms. Twenty-two were men and 10 were women, mean age 58 years (range 40 to 83). All patients had chest pain typical of MI that persisted for 30 minutes or longer and electrocardiographic evidence of ST-segment de- viation in 2 or more leads. Serum CK values were measured on admission and every 4 hours thereafter, and the typical ascent and subsequent descent pattern was demonstrated in all cases. Patients with symptoms for more than 8 hours before entry into the coronary care unit were excluded from this study.
Protocol: Angiography was performed using the trans- femoral approach. After hemodynamic values were measured, left ventriculography was performed in the 30° right anterior oblique projection using 40 ml of 76% Urografine. Selective coronary angiography was performed in multiple views after ventriculography to identify the infarct-related vessel. After visualizing the occlusion, 0.5 mg of nitroglycerin was slowly injected into the occluded artery to rule out coronary artery spasm as a cause of the acute occlusion. If no change in the
1217

1218 INTRACORONARY THROMBOLYSIS WITH UROKINASE
angiographic appearance of the vessel was noted, urokinase was continuously infused selectively into the occluded vessel at a rate of 24,000 unitslmin. Coronary angiography was re- peated routinely at lo-minute intervals during the infusion of urokinase. In the first 10 patients, PTCA was stopped if the occluded coronary artery could not be recanalized after infusion of 240,000 units of urokinase; in the latter 22 patients, the urokinase infusion was extended up to 960,000 units.
Subsequent treatment: After PTCA was completed, all patients received aspirin (300 mg/day), calcium antagonists (nifedipine, 20 mg, or diltiazem, 60 mg orally every 6 hours), and heparin (5,000 units subcutaneously every 8 to 12 hours). All patients were further treated with glucose-insulin-potas- sium (GIK) solution, which contained 313 g of glucose, 40 units of regular insulin, and 60 mEq of potassium per liter of water at 67 ml/hour for 76 hours. During this treatment, blood sugar levels were measured every 4 hours and subcutaneous injec- tion of regular insulin was added when they were over 200 mg/dl. Although our GIK protocol is somewhat different in the concentration and infusion rate from those in established reports, 12,13 we have found in more than 200 MI patients that accidental hyperkalemia, hyper- or hypoglycemia, and volume overloading are minimal during this protocol. Plasma free fatty acid levels were elevated on admission (mean 0.94 f 0.46 mmol/liter [* standard deviation]) and decreased significantly during GIK infusion (0.37 f 0.30 mmolfliter, p < 0.001).
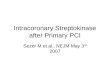
Left ventricular function: Coronary and LV angiography were repeated before hospital discharge 42 days (range 30 to 56) after the admission. Ventricular volumes were calculated by the formula of Sandler and Dodge.14 Local wall motion of the infarcted area was calculated as shown in Figure 1.
Statistical methods: All values are expressed as mean f standard deviation. Evaluations were done by the use of paired and unpaired t tests and a p value <0.05 was considered statistically significant.
Results
Of the 32 patients with MI, 7 had subtotal occlusion of an infarct-related coronary artery with good distal flow. After urokinase infusion, there was no apparent improvement of the coronary arterial stenosis in these 7 patients; thus, they were excluded from further study. In the remaining 25 patients, the complete occlusion of
FIGURE 1. A reference system for ventricular wall motion analysis, consisting of 36 radial hemiaxes converging toward the long-axis midpoint, forming a 10” angle between 2 adjacent axes. Local wall shortening was calculated on hemiaxes 10 to 20 for anterior wall in- farction and on hemiaxes 24 to 31 for inferior wall infarction.
an infarct-related vessel was identified, and intracoro- nary application of urokinase recanalized the occluded vessel in 18 patients (72%). With a small dose of uroki- nase (1240,000 units), recanalization was achieved in only 2 of the first 8 patients (25%); with a larger dose it was achieved in 16 of the last 17 patients. The mean dose of urokinase required to recanalize the occluded vessel was 530,000 units (range 240,000 to 960,000). Follow-up coronary angiography 42 days later showed that 12 of 18 patients with successful PTCA sustained the patency of an infarct-related coronary artery (group A), whereas 6 patients showed reocclusion (group B). In 7 patients, PTCA failed (group C) (Fig. 2).
Complications: Two patients had ventricular fi- brillation during the procedure of PTCA before ad- ministration of GIK. Defibrillation reestablished nor- mal sinus rhythm in both patients. Except for 4 cases of minor hematoma at the puncture site, no bleeding complications were observed.
Left ventricular function: Asynergy of lateral wall MI caused by the circumflex arterial occlusion is diffi- cult to assess by ventriculography in the right anterior oblique projection; therefore, only anterior or inferior MI was assessed. Regarding 11 patients with anterior or inferior wall MI in group A and 10 patients in groups B and C, LV ejection fraction (EF) and local wall shortening on admission and discharge are shown in Table I. In group A, EF increased from 51 f 13% to 72 f 10% (p <O.Ol), and local wall shortening increased from 4.5 f 9.5% to 29 f 19% (p <O.Ol). In contrast, in groups B and C, neither EF nor local wall shortening showed significant increases. This tendency was more marked in patients with anterior wall MI (Table II). A representative case in group A is shown in Figure 3. Cases of the inferior wall MI were few (4 in group A and 3 in groups B and C); thus, no statistical analysis was performed.
Discussion
In Europe and the United States, PTCA has been performed by the use of streptokinase alone or strep- tokinase in combination with human plasmin in pa- tients with MI, and successful recanalization of the occluded coronary artery was reported in approximately
Patent
~(G%lp*n)
L Subtotal Occlusion
N=7
(Group C)
FIGURE 2. Results of coronary angiography (CAG) in 32 patients with acute myocardial infarction. PTCA = percutaneous transluminal cor- onary angioplasty.

May 1, 1984 THE AMERICAN JOURNAL OF CARDIOLOGY Volume 53 1219
TABLE I Comparison of Admfsslon and Discharge Ejection Fraction and’ Local Wall Shortening in Anterior or inferior Wall Infarction ~___ ..___. _ -. -.~~ _ .--.-. -- - -----------
Ejection Fraction ( %I : ILocal Wall Shortening (76)
Group Admission Discharge p Value Admiss:cn Discharge p Value __. -__.-
Group A(n = 11) 51 f 13 72f 10 <O.Ol 4.5 f 9.5 29.3 f 19.0 <O.Ol
Groups B and C (n = 10) 41 f 13 41 f 10 NS 3.3 f 6..3 2 1 f 6.2 NS
p Value NS <O.Ol NS <O.Ol _ ___~ ~___ _____ __...____-____ .__ ~._____
NS = not significant.
TABLE II Comparison of Admission and Discharge Ejection Fraction and Local Wall Shortening in Anterior Wall Infarction ___-___--- .__. Ejection Fraction (%) Local Walt Shortening (%)
-- _______ .--
GrOUD Admission Discharoe D Value Admission Discharge p Value
Group A (n = 7) 44 f 8 74f 11 <O.Ol 0.6 f 8.3 36.9 f 20.0 <O.Ol $cu,up,” and C (n = 7) 40f 14 41 f9 NS 1.5 f 5.8 --0.5 f 2.6 NS
NS co.01 NS <O.Ol
NS = not significant.
80% of the patients. In the present study, the overall success rate of recanalization was 72% (18 of 25 patients) with use of urokinase. With a small dose of urokinase (1240,000 units), the successful recanalization was achieved in only 25%, while it was achieved in 94% (16 of 17 patients) who received a larger dose of urokinase. These results are comparable to those achieved with use of streptokinase. Although both streptokinase and urokinase can activate the fibrinolytic system, they do so by different mechanisms.15 Streptokinase is an in- direct activator, converting plasminogen to plasmin by way of a proactivator-activator mechanism. One of the major problems with streptokinase is that it is a foreign protein and, therefore, antigenic. Antibodies to strep- tococci are present in almost everyone in various amounts, depending on the nature of previous strep- tococcal infections. Urokinase, in contrast, is a direct activator. It can initiate fibrinolysis without forming an
activator complex. Because it is a protein secreted by the human kidney, it is also nonantigenic. It can be administered to all patients without concern for neu- tralizing antibodies; the problem of pyrogenicity is re- lated simply to the purity of the preparationi In fact, even without administration of corticosteroid or anti- histamines before urokinase treatment, no allergic re- action probably related to urokinase was observed in our study. In the acute period of MI, in which the general hemodynamic condition of the patient is unstable, urokinase, which is free of allergic reaction, may be used without worry.
Left ventricular function: Improvement in LV contractile function was observed in group A and was documented by significant augmentation of the global EF and local wall shortening of the infarct area in the ventriculogram. However, contractile function showed no recovery in either groups B and C. These data have
FIGURE 3. Left ventriculograms from a 52-year-old man who received intra- ccronary tfrcrnbolysis 2 hours after the onset of symptoms. A, left ventriculo- gram on admission showing anteroap- ical atdnesia (top, enddiitole; bottom, end-systole). B, arrow indicates total proximal occlusion of the left anterior descending ccmnary artery (top). After 480.000 units of urokinase (UK), re- canalization was achieved (bottom). C, the anteroapical akinesia disappeared 42 days after recanalization.

1220 INTRACORONARY THROMBOLYSIS WITH UROKINASE
confirmed reports that PTCA contributed to salvage of jeopardized myocardium in MI. However, the extent of improvement in LV function was minor in previous studies, and many studies reported less than 10% im- provement in global EF.7-10J6-18 Why more marked improvement in LV function was documented in our study is unclear, but.may be attributed to the difference in methods of PTCA between the present study. First, we performed repeat ventriculography later (42 -days after admission) than previous studies. Theroux et ali9 observed late return of segmental function several weeks after coronary reperfusion after a 2-hour period of oc- clusion in conscious dog, and suggested that substantial periods may be required to assess the ultimate effect of therapeutic interventions..Thus, in previous studies, the extent of improvement of LV function may have been underestimated. Second, the possibility that the dif- ference between urokinase and streptokinase influenced LV function cannot be.excluded. Further studies on this point are required, because the thrombolytic agent with fewer side effects, such as allergic reaction, might be advantageous for the jeopardized myocardium. Third, GIK solution was administered in our study. The hy- pothetical mechanisms of GIK on ischemic myocardium include reduction of circulating free fatty acid, which has been shown to be toxic to ischemic myocardium; increased utilization of glucose for energy production; stabilization of the altered membrane; and improve- ment in coronary perfusion.12J3 If these effects of GIK are true, recanalization of the occluded coronary artery by PTCA will make better diffusion of GIK solution into jeopardized myocardium and a synergistic effect af PTCA and, GIK on the jeopardized myocardium in MI is possible. Experimental as well as randomized studies of a large number of patients are required to justify the above-mentioned hypothesis.
In conclusion, urokinase can be used safely as a thrombolytic agent to recanalize the occluded coronary artery in MI. Its beneficial effect on LV function may be superior to that of streptokinase. Future research must assess PTCA in combination with other proposed interventions such as GIK, myocardium-protect- ing drugs, and intraaortic counterpulsation in an at- tempt to further reduce the extent of injury in patients with MI.
References
I. Rentrop P, Blanke H, Karsch KR, Kaiser H, K&terlng H, Leltz K. Selective intracoronary thrombolysis in acute myocardial infarction and unstable angina pectoris. Circulation 1981;63:307-317.
2. Ganz W, Buchbinder N, Marcus H, hlondkar A, Maddahl J, Charuzi Y, O’Connor L, Shell W, Fishbein MC, Kass R, Miyamoto ?, Swan HJC. In- tracoronary thrombolysis in evolving myocardial infarctlon. Am Heart J 1981;101:4-13.
3. Mathey DG, Kuck KH, Tllsner V, Krebber HJ, Blelfeld W. Nonsurgical coronary artery recanalization in acute transmural myocardial infarction. Circulation 1981;83:489-497.
4. Reduto LA, Smalling RW, Freund GC, Gould KL. lntracoronary infusion of streptokinase in patients with acute myocardial infarction: effects of re- perfusion on left ventricular performance. Am J Cardiol 1981;48:403-
5.
6.
7.
8.
9.
10.
II.
12.
13.
14.
409. Cowley MJ, Hastlllo A, Vetrovec GW, Hess ML. Effects of intracoronary streptokinase in acute myocardial infarction. Am Heart J 1981;102: 1149-1158. Lee G, Amsterdam EA, Low R, Joye JA, Kimchl A, LIeMarIa AN, Mason DT. Efficacy of percutaneous transluminal coronary recanalization utilizing streptokinase thrombolysis in patients with acute myocardial infarction. Am Heart J 1981;102:1159-1167. Rentrop P, Blanke H, Karsch KR, Rutsch W, Schartl M, Merx W, D&r R, Mathey D, Kuck K. Changes in left ventricular function after intracoronary streotokinase infusion in clinically evolvino mvocardial infarction. Am Heart J 1981;102:1188-1193. . - - Rentrop KP, Blanke Ii, Karsch KR. Effects of nonsurgical coronary re- perfusim on the left ventricle in human subjects compared with conventional treatment: study of 18 patients with acute myocardial infarction treated with intracoronary infusion of streptokinase. Am J Cardiol 1982;49:1-8. Weinstein J. Treatment of mvocardial infarction with intracoronary strep- tokinase: efficacy and safety data from 209 United States cases in the Hoechst-Roussel registry. Am Heart J 1982;104:894-898. Smallktg RW, Fuentes F, Frti GC, Reduto LA, Wanta-Mattews M, Gaeta JM. Walker W. Sterllno R. Gould KL. Beneficial effects of intracoronary thrombolysis up to eight&i hovs after onset of pain in evolving myocardial infarction. Am Heart J 1982;104:912-920. Research Committee on Coronary Thrombolysis. Treatment of acute myocardial infarction with intracoronary urokinase infusion: preliminary results of 242 cases from 15 medical centers in Japan (abstr). Jpn Circ J 1983;47:900. Mantle JA, Rogers WJ, Smlth LR, McDaniel HO, Papapietro SE, Russell RO Jr, Rackley CE. Clinical effects of glucose-insulin-potassium on left ventricular function in acute myocardiil infarctii: results from a randomized clinical trial. Am Heart J 1981;102:313-324. Rackley CE, Russell RO Jr, Rogers WJ, Mantle JA, McDaniel HO, Papa- pieho SE. Clinical experience with glucose-insulin-potassium therapy tn acute myocardial infarction. Am Heart J 1981;102:1038-1049. Sandler H, Dodge HT. The use of single plane angiocardiograms for the calculation of left ventricular volume in man. Am Heart J 1968;75:325- 334.
15. Sharma GVRK. Cella 0. Parisi AF. Sasahara AA. Thrombolvtic theraov. N Engl J Mad 1982;306:i268-1276.
.
16. Reduto LA, Freund GC, Gaeta JM, Smalllng RW, Lewls B, Gould KL. Coronary artery reperfusion in acute myocardial infarction: beneficial effects of intracoronarv streotckinase on left ventricular salvage and performance. Am Heart J 1981;1d2:1168-1177.
17. Schwarz F, Schuler G, Katus H, Mehmel HC, Olshausen K, Hofmann M, Herrmann HJ, Ktibler W. lntracoronary thrombolysis in acute myocardial infarction: correlations among serum enzyme, scintigraphic and hemody- namic findings. Am J Cardiol 1982;52:32-38.
18. Timmis GC, Gangadharan V, Hauser AM, Ramos RG, Westveer DC, Gordon S. lntracoronary streptokinase in clinical practice. Am Heart J 1982;104:925-938.
19. Theroux P, Ross J Jr, Franklln D, Kemper WS, Sasayama S. Coronary arterial repark&n. III. early and late effects on regional myocardlal function and dimensions in conscious dogs. Am J Cardiol 1976;38:599-805.