Embed Size (px)
Citation preview

235
Effects of Indomethacin on rCBF During and After FocalCerebral Ischemia in the Cat
SHUKU SHIGENO, M . D . , * EMANUEL FRITSCHKA, M . D . , t
TAKU SHIGENO, M . D - . t t AND MARIO BROCK, M . D . I t
SUMMARY The effect of indomethacin on rCBF was studied in cats anesthetized with Nembutal eitherunder resting conditions or with temporary middle cerebral artery (MCA) occlusion. RCBF was measuredby the microsphere method. In control animals (n = 3), indomethacin (4 mg/kg, i.v.) significantly reducedrCBF by about 25% in both cortex (from 44 ± 6 to 32 ± 3 ml/100 g/min, p < 0.001) and white matter (from36 ± 4 to 26 ± 2 ml/100 g/min, p < 0.001). After MCA occlusion rCBF was markedly decreased in thesylvian region ipsilateral to occlusion (ischemic core) (from 38 ± 4 to 14 ± 2 ml/100 g/min in cortex, 4animals). Although pretreatment with indomethacin (4 mg/kg) (4 animals) 30 min prior to occhision did notalter rCBF during ischemia, a marked enhancement of reactive hyperemia was observed in the ischemiccore immediately upon reperfusion following 2 h occlusion (54 ± 1 1 untreated vs 95 ± 13 treated, p <0.05). In the delayed postischemic period, namely 2 h after ^circulation, rCBF still remained to be higher inthe animals treated with indomethacin (40 ± 6 untreated vs 96 ± 9 treated, p < 0.001). Such an effect ofindomethacin for ameliorating postischemic blood flow in both the immediate and delayed period was lessprominent in the adjacent area (penumbra) ipsilateral to occlusion. In the contralateral hemisphere,indomethacin caused slight reduction in rCBF during ischemia. An altered relationship between the actionsof PGI2 and TXA2 has been proposed to occur at the blood-endothelium interface during reperfusion afterischemia in which a disproportionate synthesis of TXA2 might be suppressed by indomethacin, whereasindomethacin dominantly suppresses PGI2 synthesis under normal conditions.
Stroke Vol 16, No 2, 1985
AN ALTERED RELATIONSHIP between the actionsof several prostaglandins (PGs) such as prostacyclin(PGIj) and thromboxane A2 (TXA2) may occur inpathological situations, whereas a balanced interactionis maintained under normal conditions. In addition tothe general agreement that PGI2 is produced in vascularendothelia, and TXA2 in platelets,1 there is increasingevidence that TXA2 synthesis can also occur in thevascular endothelium,2"9 where a dominant but oppos-ing role of PGI2 with respect to TXA2 has been docu-mented. Thus previous results which have shown adecrease in basal cerebral blood flow with indometha-cin treatment10"18 might be indicative of preferentialsuppression of PGI2 synthesis at the vascular endothe-lia, although indomethacin is thought to inhibit moreor less all the products of cyclooxygenase.19
In cerebral ischemia, a significant accumulation ofcyclooxygenase products is known to occur, particu-larly when the ischemia is either transient20"22 or in-complete.22"24 Although the pathogenetic role of accu-mulation of PGs in cerebral ischemia remains unclear,the improvement shown in cerebral microcirculationwith indomethacin treatment following global cerebralischemia suggests a reversal of roles: a relative domi-nance in TXA2 level during this pathological situa-tion.2326 Accordingly the present study was aimed atexploring whether the above relationship can be al-
From the Department of Radiology, Tokyo Women's Medical Col-lege, 10 Kawadacho, Shinjuku-ku, Tokyo 160, Japan,* and the Depart-ments of Internal Medicine,t and Neurosurgery.t Klinikum SteglitzderFreien Universitaet Berlin Hindenburgdamm 30, 1000 Berlin, 45,F.R.G.
This paper was presented in part at the Xlth International Symposiumon Cerebral Blood Flow & Metabolism.
Address correspondence to: Taku Shigeno, M.D., Department ofNeurosurgery, University of Tokyo, 7-3-1 Hongo, Bunkyo-ku, Tokyo113, Japan.
Received June 22, 1983; revision #2 accepted September 5, 1984.
tered by treatment with indomethacin in cats with focalcerebral ischemia.
Material and methodsAdult mongrel cats weighing 3 to 4 kg were anesthe-
tized with Nembutal® (30 mg/kg), paralyzed withFlaxedil®, and artificially ventilated with nitrous ox-ide/oxygen gas mixture via a cuffed endotracheal tube.Following catheterization to one femoral vein and twofemoral arteries, one of the arterial catheters beingintroduced to the left cardiac ventricle, the animal wasfastened on the stereotaxic frame in a sphinx like posi-tion. Systemic blood pressure and cardiac ventricularpressure were continuously monitored. Arterial bloodgases were intermittently determined and maintainedwithin normal limits throughout the experiment. Rec-tal temperature was continuously measured and keptbetween 36° and 38° C by an electrically heated blan-ket. Regional cerebral blood flow (rCBF) was meas-ured by the microsphere method, using microspheres15 /Am in diameter and labelled with scandium-46,strontium-85, cerium-141 and iodine-125. Preparationof the microspheres and calculation of rCBF valueshave been described in detail elsewhere.27
In three animals rCBF was determined in a restingstate before and 30 min after intravenous injection of 4mg/kg of indomethacin (Sigma0). The solution of in-domethacin was prepared just prior to the experimentby dissolving 20 mg of indomethacin in 10 ml of a0.5% sodium bicarbonate solution followed by addi-tion of 10 ml of a phosphate buffer (Na 149.2, K 4.2,Cl 139.6, Phosphate 8.2 mM/L), thus yielding a 1 mg/ml solution. The pH value was 7.45 ± 0.01 and theappropriate volume was delivered by an infusion pump(Braun0) over 10 min. After the experiment, braintissues weighing 100 to 200 mg were rapidly dissectedfrom 9 regions of the cortex and subjacent white matter
by guest on May 26, 2018
http://stroke.ahajournals.org/D
ownloaded from
236 STROKE VOL 16, No 2, MARCH-APRIL 1985
in the cerebral hemisphere and the wet weight wasdetermined after storing tissues in preweighed tightly-sealed test tubes. A paired comparison by Student's t-test was made using the rCBF values against tissue wetweight before and after treatment.
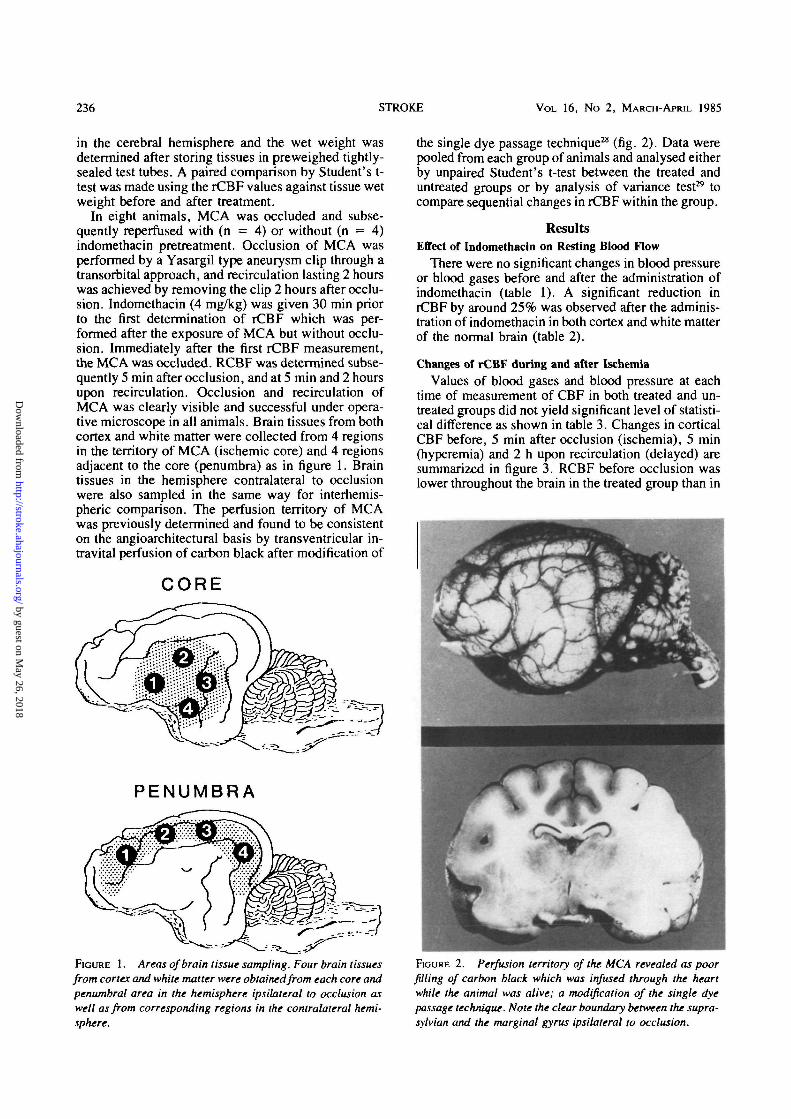
In eight animals, MCA was occluded and subse-quently reperfused with (n = 4) or without (n = 4)indomethacin pretreatment. Occlusion of MCA wasperformed by a Yasargil type aneurysm clip through atransorbital approach, and recirculation lasting 2 hourswas achieved by removing the clip 2 hours after occlu-sion. Indomethacin (4 mg/kg) was given 30 min priorto the first determination of rCBF which was per-formed after the exposure of MCA but without occlu-sion. Immediately after the first rCBF measurement,the MCA was occluded. RCBF was determined subse-quently 5 min after occlusion, and at 5 min and 2 hoursupon recirculation. Occlusion and recirculation ofMCA was clearly visible and successful under opera-tive microscope in all animals. Brain tissues from bothcortex and white matter were collected from 4 regionsin the territory of MCA (ischemic core) and 4 regionsadjacent to the core (penumbra) as in figure 1. Braintissues in the hemisphere contralateral to occlusionwere also sampled in the same way for interhemis-pheric comparison. The perfusion territory of MCAwas previously determined and found to be consistenton the angioarchitectural basis by transventricular in-travital perfusion of carbon black after modification of
CORE
PENUMBRA
FIGURE 1. Areas of brain tissue sampling. Four brain tissuesfrom cortex and white matter were obtained from each core andpenumbral area in the hemisphere ipsilateral to occlusion aswell as from corresponding regions in the contralateral hemi-sphere.
the single dye passage technique28 (fig. 2). Data werepooled from each group of animals and analysed eitherby unpaired Student's t-test between the treated anduntreated groups or by analysis of variance test29 tocompare sequential changes in rCBF within the group.
ResultsEffect of Indomethacin on Resting Blood Flow
There were no significant changes in blood pressureor blood gases before and after the administration ofindomethacin (table 1). A significant reduction inrCBF by around 25% was observed after the adminis-tration of indomethacin in both cortex and white matterof the normal brain (table 2).
Changes of rCBF during and after IschemiaValues of blood gases and blood pressure at each
time of measurement of CBF in both treated and un-treated groups did not yield significant level of statisti-cal difference as shown in table 3. Changes in corticalCBF before, 5 min after occlusion (ischemia), 5 min(hyperemia) and 2 h upon recirculation (delayed) aresummarized in figure 3. RCBF before occlusion waslower throughout the brain in the treated group than in
FIGURE 2. Perfusion territory of the MCA revealed as poorfilling of carbon black which was infused through the heartwhile the animal was alive; a modification of the single dyepassage technique. Note the clear boundary between the supra-sylvian and the marginal gyms ipsilateral to occlusion.
by guest on May 26, 2018
http://stroke.ahajournals.org/D
ownloaded from

EFFECTS OF INDOMETHACIN ON rCBF IN CAT/Shigeno et al 237
TABLE 1 Physiological Variables Before and After IndomethacinTreatment
Before After
TABLE 3 Physiological Variables before, 5 min after MCA Oc-clusion (ischemia), 5 min (hyperemia) and 2 h (delayed) uponRecirculation with or without Indomethacin Treatment
MABP (mm Hg)
PO2 (mm Hg)
PCO2 (mm Hg)
PH
140 ±6112±5
31 ±2
7.36 + 0.04
133±9112 + 5
31 ±2
7.40 ±0.03
Values are mean + SEM. MABP = mean arterial blood pressure.There is no statistical significance in all parameters before and afterindomethacin treatment.
the untreated group, again showing the effect of indo-methacin in decreasing CBF under resting conditions.However, in the core region ipsilateral to occlusion,the pre-occlusion values were lower than in other re-gions in both groups which might have been caused bysome operative insult in exposing the MCA. Or, sincethe flow value was calculated against tissue wet weightand the tissues in the ischemic core developed massivewater increase in this study, the CBF values in the corecould be lower than those in the other regions withoutincrease in water content. In the untreated group, amarked flow reduction in the core was followed byimmediate hyperemia exceeding the contralateral flowupon recirculation and returned toward the pre-occlu-sion value 2 h later. In the penumbra the reduction inrCBF during ishemia and subsequent hyperemia wereless marked. In the contralateral hemisphere, sequen-tial values of rCBF during occlusion and upon recircu-lation stayed unchanged in the corresponding regionsto core and penumbra, although there was tendency ofslight reduction in rCBF in the area corresponding tocore.
By contrast in the animals treated with indometha-cin, striking and sustained increases in CBF were ob-served in the ipsilateral ischemic core in both the im-mediate and delayed period upon recirculation. Thedecrease in rCBF during ischemia in the core did notdiffer significantly irrespective of the indomethacintreatment. In the penumbral region ipsilateral to occlu-sion, such an effect for enhancing hyperemia was lessmarked. Contralaterally, indomethacin only displayedan effect of slight reduction in rCBF throughout theischemia and recirculation period without developingany hyperemic stage.
CBF changes in the white matter were similar tothose in the cortex (fig. 4), where a significant andsustained increase of flow in the ischemic core follow-ing indomethacin treatment was also observed in thepostischemic period. Occlusion and recirculation ofMCA did not influence contralateral flow, where indo-methacin had no effect, either.
TABLE
Cortex
White
2 Effect
matter
of Indomethacin (4 mglkg)
Before
44 + 6
36 + 4
on Resting rCBFAfter
Indomethacin
32 ±3*
26 ±2*
MABP
PO2
PCO2
pH
MABP
PO2
PCO2
pH
Nc
Before
130 + 7
99±5
33 ±3
7.41 ±0.03
) treatment (n
Ischemia
138±5
104±7
32±2
7.40±0.03
= 4)
Hyperemia
138±6
105 ±5
3O±2
7.39 ±0.03
Indomethacin treatment (n = 4)
Before
121±11
95 ±5
35 ±2
7.36±0.02
Ischemia
123 ±9
106 ±5
35 ±3
7.33±0.02
Hyperemia
128+10
106 ±4
32±1
7.37±0.01
Delayed
123±13
98±4
32±1
7.38±0.03
Delayed
143 ±5
101 ±4
31±1
7.37±0.02
Values are mean ± (SEKl-(ml/100 g/min) obtained from 27 braintissue samples in 3 cats. *sig. (p < 0.001) by paired t-test.
Values are mean ± PEM. MABP = mean arterial blood pressure.No statistical significance was obtained either within or betweengroups.
DiscussionSince the effect of indomethacin on resting CBF was
first reported by Pickard et al,10 there have been anumber of reports which have shown CBF reductionby indomethacin in both normal and hypercapnic situa-tions." '8 In accordance with those reports, the presentstudy in cats under barbiturate anesthesia showed adecrease in resting CBF. However, others have showna total lack of effect on CBF.30"32 As to the microspheremethod, Busija & Heistad32 did not observe any effectof indomethacin, while other workers"18 observedCBF reduction. Explanation for these conflicting re-sults is difficult but might have been caused by differ-ences in the methods employed for CBF measurement,animal species or anesthetics.
Gaudet & Levine20 first reported a marked accumu-lation of PGs upon reperfusion following global cere-bral ischemia in the gerbil. The PGs which accumulat-ed in the postischemic period were PGD2, PGF 2 Q ,
PGE2 and to a lesser degree TXB2 and 6-keto-PGFlo.Pretreatment with indomethacin almost completely in-hibited this accumulation.21 Thereafter similar resultson the massive accumulation of PGs in cerebral isch-emia were also obtained.l5'22> 23 Using reversible globalischemia in the rat, Shohami et al22 reported an accu-mulation of PGE2, 6-keto-Fla and TXB2 during ische-mia and upon reperfusion. Of interest to note was afurther accumulation of TXB2 upon reperfusion,whereas other PGs tended to be decreased. Pretreat-ment with indomethacin (4 mg/kg) prior to the induc-tion of ischemia ameliorated the increases of thesePGs, particularly of TXB2 after recirculation.
The biosynthesis of prostaglandins is primarily de-termined by substrate availability as long as the mini-mum level of tissue oxygen is maintained.33 Kagstrdmet al34 assumed that high concentrations of arachidonicacid which accumulated during the ischemic peri-od35' 36 might trigger a burst of PG synthesis as soon asthe tissue is reoxygenated. For the activity of cycloox-ygenase, however, the presence of endoperoxides is
by guest on May 26, 2018
http://stroke.ahajournals.org/D
ownloaded from

238 STROKE VOL 16, No 2, MARCH-APRIL 1985
paradoxically required.33'37 It may also be assumedthat hydroperoxides formed in the lipoxygenase path-way (HPETEs) which is probably involved in cerebralischemia38"40 take part in the elucidation of clyclooxy-genase activity. Once these hydroperoxides are formedand further converted to hydroxyacids by peroxydases,the active oxygen liberated concomitantly in this proc-ess is known to suppress the synthesis of PGI2 but notTXA2,4142 leading to imbalance between these oppos-ing vasoactive substances in pathological situations.
The effect of indomethacin in ameliorating impairedpostischemic reperfusion was first documented by Fur-low and Hallenbeck.25 Pretreatment with indomethacin4 mg/kg one hour prior to ischemia improved the de-layed hypoperfusion.26 In the present study we coulddemonstrate that indomethacin increased postischemicflow either in the immediate period upon reperfusionor in the delayed period. The reactive hyperemia wasmuch more enhanced and the flow still remained to behigher in the delayed period than in the untreated con-trols. Although the degree of interaction between PGI2
CORTEX
Core Penumbra
Ipsilateral
I.
Contralateral dFIGURE 3. Changes in rCBF in the cortex ipsilateral or con-tralateral to MCA occlusion with (closed bars) or without indo-methacin treatment (open bars). RCBF was measured before, 5min after MCA occlusion (ischemia), 5 min (hyperemia) and 2 h(delayed) upon reperfusion. Note a marked increase in bloodflow upon reperfusion in the ischemic core of animals treatedwith indomethacin (upper left). Asterisks indicate statisticalsignificance between untreated and treated groups by Student'st-test at each time of CBF measurement f*p < 0.05, **p <0.01, ***p < 0.001). Circles on the top of the bars indicatestatistical significance between changes in rCBF during andafter MCA occlusion as compared to the pre-occlusion flow byScheffe test in each treated or untreated group (°p<0.05,°°p<0.01).
WHITE MATTER
Core Penumbra
Ipsilateral
Contralateral
I tt I I I
FIGURE 4. Changes in rCBF in the white matter ipsilateral orcontralateral to MCA occlusion with (closed bar) or without(open bar) indomethacin treatment. RCBF was measured be-fore, 5 min after MCA occlusion (ischemia), 5 min (hyperemia)and 2 h (delayed) upon reperfusion. Note also a marked in-crease in blood flow upon reperfusion in the ischemic core of thetreated animals as observed in the cortex (upper left). Asterisksindicate statistical significance between untreated and treatedgroups by Student's t-test at each time of CBF measurement (*p< 0.05, **p < 0.01, ***p < 0.001). Circles on the top of thebars indicate statistical significance between changes in CBFduring and after MCA occlusion as compared to the pre-occlu-sion value by Scheffe test in each treated and untreated groupf°p < 0.05, °°p < 0.01).
and TXA2 might be different in the immediate anddelayed period after recirculation, a major contributionwould seem to be the relative dominance of TXA2
synthesis throughout the re-oxygenation period. Thefinding that such changes were most prominent in thecore of ischemia indicates that re-oxygenation processpropagates from this region but not from the peripheryof ischemia. This enhanced postischemic blood flowby indomethacin was not a result from a difference inthe level of ischemic flow, because indomethacin didnot change this even in the presence of premorbidreduction of CBF. No such patterns as ischemia andhyperemia were noted in the contralateral hemisphereexcept for the effect of indomethacin in reducing bloodflow as observed in normal conditions. Recently, Kag-strom et al34 also demonstrated that indomethacin en-hanced immediate reflow upon recirculation. Theyconcluded that TXA2 restricted the hyperemia. As tosuch an inversed effect of indomethacin on rCBF inhealth and disease, Okabe et al17 has shown decrease in
by guest on May 26, 2018
http://stroke.ahajournals.org/D
ownloaded from

EFFECTS OF INDOMETHACIN ON rCBF IN CAVShigeno et al 239
CBF in normal subjects, but increase in patients withrecent stroke.
It has been generally agreed that TXA2 and PGI2
interact at the blood-endothelium interface, with thesite of synthesis being in the platelets for the formerand vascular endothelia in the latter.1 Recently, how-ever, evidence of the production of TXA2 in vascularendothelia has arisen which suggests that the ratio ofPGI2 synthesis to that of TXA2 is greater under normalconditions.2"9 Therefore the effect of indomethacin fordecreasing resting CBF can be understood as a resultfrom a greater suppression of PGI2 synthesis. By con-trast, following cerebral ischemia disproportionatesynthesis of TXA2 might occur, at least as judged bythe amelioration of postischemic flow in the presentstudy. As stated previously, arachidonic acid accumu-lated during the ischemic period is involved in thesubsequent cascades after incorporation of oxygen ei-ther for cyclooxygenase reaction or for lipoxygenasereaction. Since the prostacyclin synthetase is selective-ly inhibited by peroxidase-derived products, possiblyoxygen radicals in both pathways,4142 disproportion-ate synthesis of TXA2 is readily suspected. However,evidence for this hypothesis is still indirect on accountof the rather non-specific inhibition of all prostaglan-din synthesis by indomethacin, or the possibility thatindomethacin may not be a pure cyclooxygenase in-hibitor.43 The recent discoveries of more specificthromboxane antagonist, either of synthetase44 or ofreceptor45 may be of value in order to clarify themechanisms involved. In this regard, the resolution ofexperimental vasospasms by a TXA2 synthetase inhibi-tor46 also suggests a disproportionate synthesis ofTXA2 in pathological situations.
In summary, although there is strong evidence ofdisproportionate synthesis of TXA2 in cerebral isch-emia, the significance of PGs in the postischemic path-ophysiology such as edema formation and ischemicbrain damage remains unclear. Furthermore, whetherthe augmented reactive hyperemia caused by indo-methacin is of actual benifit to neuronal recovery isopen to question.
AcknowledgmentsThe authors are particularly grateful to Mr. John Sharkey for prepar-
ing the manuscript. We also thank the staff of the Medical Illustration ofthe Institute of Neurological Sciences, University of Glasgow for theirexcellent photographic work.
References1. Moncada S, Flower RJ, Vane JR: Prostaglandins, prostacyclin and
thromboxane A2. In Goodman Oilman A, Goodman LS, Gilman A(eds) Goodman and Gilman's The Pharmacological Basis forTherapeutics. 6th ed. New York-Toronto-London, MacMillan, pp668-681, 1980
2. Hagen AA, White RP, Robertson JT: Synthesis of prostaglandinsand thromboxane B2 by cerebral arteries. Stroke 10: 306-309,1979
3. Maurer P, Moskowitz MA, Levine L, Melamed E: The synthesis ofprostaglandins by bovine cerebral microvessels. Prostaglandinsand Medicine 4: 153-161, 1980
4. Salzman PM, Salmon JA, Moncada S: Prostacyclin and thrombox-ane A2 synthesis by rabbit pulmonary artery. J Pharmacol Exp Ther215: 240-247, 1980
5. Ingerman-Wojenski D, Silver MJ, Smith JB, Macarak E: Bovineendothelial cells in culture produce thromboxane as well as prosta-cyclin. J Clin Invest 67: 1292-1296, 1981
6. Geese A, Ottlecz A, Meze Z, Telegdy G, Joo F, Dux E, Karnu-shina I: Prostacyclin and prostaglandin synthesis in isolated braincapillaries. Prostaglandins 23: 287-297, 1982
7. Goldsmith JC, Needelman SW: A comparative study of thrombox-ane and prostacyclin release from ex vivo and cultured bovinevascular endothelium. Prostaglandins 24: 173-178, 1982
8. Alhenc-Gelas F, Tsai SJ, Callahan KS, Campbell WB, JohnsonAR: Stimulation of prostaglandin formation by vasoactive media-tors in cultured human endothelial cells. Prostaglandins 24: 723-742, 1982
9. Neri Semeri GG, Abbate R, Gensini GF, Panetta A, Casolo GC,Carini M: TXA2 production by human arteries and veins. Prosta-glandins 25: 753-766, 1983
10. Pickard JD, MacKenzie ET: Inhibition of prostaglandin synthesisand the response of baboon cerebral circulation to carbon dioxide.Nature 245: 187-188, 1973
11. Bill A: Effects of indomethacin on regional blood flow in consciousrabbits — a microsphere study. Acta Physiol Scand 105: 437-442,1979
12. Sakabe T, Siesjo BK: The effect of indomethacin on the blood flow— metabolism couple in the brain under normal, hypercapnic andhypoxic conditions. Acta Physiol Scand 107: 283-284, 1979
13. Dahlgren N, Nilsson B, Sakabe T, Siesjo BK: The effect of indo-methacin on cerebral blood flow and oxygen consumption in the ratat normal and increased carbon dioxide tensions. Acta PhysiolScand 111: 475-485, 1981
14. Dahlgren N, Siesjo BK: Effects of indomethacin on cerebral bloodflow and oxygen consumption in barbiturate-anesthetized normo-capnic and hypercapnic rats. J Cereb Blood Flow Metabol 1: 109—115, 1981
15. Crockard A, lannotti F, Ladds G: Cerebrovascular effects of pros-taglandin inhibitors in the gerbil. J Cereb Blood Flow Metabol 2:67-72, 1982
16. McCulloch J, Kelly PAT, Grome JJ, Pickard JD: Local cerebralcirculatory and metabolic effects of indomethacin. Am J Physiol243: H416-H423, 1982
17. Okabe T, Meyer JS, Amano T, Okayasu H, Mortel K: Prostaglan-din inhibition and cerebrovascular hemodynamics in normal andischemic human brain. J Cereb Blood flow Metabol 3: 115-121,1983
18. QuintanaA, RaczkaE, GiraltMT, Quintana MA: Effects of aspirinand indomethacin on cerebral circulation in the conscious rat: Evi-dence for a physiological role of endogenous prostaglandins. Pros-taglandins 25: 549-556, 1983
19. Abdel-Halim MS, SjoquistB, AnggardE: Inhibition of prostaglan-din synthesis in rat brain. Acta Pharmacol Toxicol 43: 266-272,1978
20. Gaudet RJ, Levine L: Transient cerebral ischemia and brain pros-taglandins. Biochem Biophys Res Comm 86: 893-901, 1979
21. Gaudet RJ, Alam I, Levine L: Accumulation of cycloocygenaseproducts of arachidonic acid metabolism in gerbil brain duringreperfusion after bilateral common carotid artery occlusion. J Neur-ochem 35: 653-658, 1980
22. Schohami E, Rosenthal J, Lavy S: The effect of incomplete cere-bral ischemia on prostaglandin levels in rat brain. Stroke 13: 494-499, 1982
23. Gaudet RJ, Levine L: Effect of unilateral common carotid arteryocclusion on levels of prostaglandins D2, F 2 Q and 6-keto-prosta-glandin F ] a in gerbil brain. Stroke 11: 648-652, 1980
24. Crockard HA, Bhakoo KK, Lascelles PT: Regional prostaglandinlevels in cerebral ischemia. J Neurochem 38: 1311-1314, 1982
25. Furlow TW Jr, Hallenbeck JM: Indomethacin prevents impairedperfusion of dog's brain after global ischemia. Stroke 9: 591-594,1978
26. Hallenbeck JM, Furlow TW Jr: Prostaglandin I2 and indomethacinprevent impairement of post-ischemic brain reperfusion in the dog.Stroke 10: 629-637, 1979
27. Shigeno T, Fritschka E, Brock M, Schramm J, Shigeno S, Cervos-Navarro J: Cerebral edema following experimental subarachnoidhemorrhage. Stroke 13: 368-379, 1982
28. Weber R, Furuse M, Brock M, Dietz H: The single dye passage. A
by guest on May 26, 2018
http://stroke.ahajournals.org/D
ownloaded from

240 STROKE V O L 16, No 2, MARCH-APRIL 1985
new technique for the study of cerebral blood flow distributions.StrokeS: 247-251, 1974
29. Scheffe H: The Analysis of Variance. New York, John Wiley &Sons, 1959
30. Wei EP, Ellis EF, Kontos HA: Role of prostaglandins in pialarteriolar response to CO2 and hypoxia. Am J Physiol 238: H226-H230, 1980
31. Cuypers J, Cuevas A, Duisberg R: Effect of indomethacin on CO2-induced hyperaemia (CO2-response) in the rabbit brain. Neurochir-urgia21: 62-66, 1978
32. Busija DW, Heistad DD: Effects of indomethacin on cerebral bloodflow during hypercapnia in cats. Am J Physiol 244: H519-H524,1983
33. Lands WEM: The biosynthesis and metabolism of prostaglandins.Ann Rev Physiol 41: 633-652, 1979
34. Kagstrom E, Smith M-L, Wallstedt L, Siesjo BK: Cyclo-oxygen-ase inhibition by indomethacin and recirculation following cerebralischemia. Acta Physiol Scand 118: 193-201, 1983
35. Yoshida S, Inoh S, Asano T, Sano K, Kubota M, Shimazaki H,Ueta N: Effect of transient ischemia on free fatty acids and phos-pholipids in the gerbil brain. J Neurosurgery 53: 323-331, 1980
36. Rehncrona S, Westerberg B, Akesson B, Siesjo BK: Brain corticalfatty acids and phospholipids during and following complete andsevere incomplete ischemia. J Neurochem 38: 84-93, 1982
37. Kulmacz RJ, Lands WEM: Requirements for hydroperoxide by thecycloocygenase and peroxidase activities of prostaglandih H syn-thase. Prostaglandins 25: 531-540, 1983
38. Sautebin L, Spagnuolo C, Galli C, Galli G: A mass fragmento-graphic procedure for the simultaneous determination of HETE and
1978in the central nervous system. Prostaglandins 16: 985-988,
39. Spagnoulo C, Sautebin L, Galli G, Racagni G, Galli C, Mazzari S,Finesso M: PGF^, thromboxane B2 and HETE levels in gerbilbrain cortex after ligation of common carotid arteries and decapita-tion. Prostaglandins 18: 53-61, 1979
40. Asano T, Gotoh O, Koide T, Takakura K: Ischemic brain edemafollowing occlusion of the middle cerebral artery in the rat. II:Alteration of the eicosanoid synthesis profile of the brain microves-sels. Stroke (in press)
41. Ham EA, Egan RW, Soderman DD, GalePH, Kuehl FA Jr: Peroxi-dase-dependent deactivation of prostacyclin synthetase. J BiolChem254: 2191-2194, 1979
42. Kuehl FA, James JL, Ham EA, Egan RW, Dougherty HW: Inflam-mation: The role of peroxidase-derived products. Adv Prostaglan-din Thromboxane Res 6: 77-86, 1980
43. Wieloch T, Hougaard K: Cyclooxygenase inhibitors and the regu-lation for cerebral blood flow. J Cereb Blood Flow Metabol 3:S291-S292, 1983
44. Parry MJ, Randall MJ, Hawkeswood E, Cross PE, Dickinson RP:Enhanced production of prostacyclin in blood after treatment withthromboxane synthetase inhibitor, UK-38,485. In Proceedings ofBritish Pharmacological Society, Glasgow, 53, 1982
45. Kennedy I, Coleman RA, Humphrey PPA, Levy GP, Lumley P:Studies on the characterization of prostanoid receptors: A proposedclassification. Prostaglandins 24: 667-689, 1982
46. Sasaki T, Wakai S, Asano T, Takakura K, Sano K: Prevention ofcerebral vasospasm after SAH with a thromboxane synthetase in-hibitor, OKY-1581. J Neurosurgy 57: 74-82, 1982
by guest on May 26, 2018
http://stroke.ahajournals.org/D
ownloaded from

S Shigeno, E Fritschka, T Shigeno and M BrockEffects of indomethacin on rCBF during and after focal cerebral ischemia in the cat.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1985 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.16.2.235
1985;16:235-240Stroke.
http://stroke.ahajournals.org/content/16/2/235World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 26, 2018
http://stroke.ahajournals.org/D
ownloaded from







![Indomethacin Capsules, USP 25 mgdiuretics, ACE inhibitors, or angiotensin receptor blockers (ARBs)] [see Precautions; Drug Interactions]. Avoid the use of indomethacin capsules in](https://img.dokumen.tips/doc/110x75/5f723d43e581ab752c2e347b/indomethacin-capsules-usp-25-mg-diuretics-ace-inhibitors-or-angiotensin-receptor.jpg)





















