Embed Size (px)
Citation preview

Effects of Heart Rate on Coronary Flow and Cardiac Oxygen Consumption
D. LAURENT, C. BOLENE-WILLIAMS, F. L. WILLIAMS AND L. N. KATZ
From tJde Cardiovascular Department, Medical Research Institute, ikficlzael Reese Hospital, Chicago, Illinois
ABSTRACT The effects of electrically-induced heart rate (up to 300 beats/min.) on
coronary flow and cardiac oxygen consumption has been studied in an open- chested intact preparation. A significant correlation between heart rate, coronary flow and cardiac oxygen consumption has been found at each level of cardiac work. Coronary flow and cardiac oxygen consumption increase with a rise in heart rate and seem to approach a limit at extremely rapid heart rates. Nomograms relating heart rate, work and oxygen consumption of the heart have been constructed. From these it is seen that heart rate is an im- portant factor in determining the myocardial oxygen consumption; this is true at each level of cardiac work. The significance of these findings have been discussed relative to the unanesthetized animal. Under conditions of excessive heart rate or cardiac load which presumably lead to unusually high energy requirements, a radical departure from the expected ‘normal’ values was found in coronary flow, coronary A-V oxygen difference and cardiac oxygen consumption. This confirms the presence of ‘spontaneous’ change pre- viously described by us. Its meaning and significance is discussed. Under these conditions of ‘spontaneous’ change coronary flow was increased, oxy- gen consumption decreased and coronary venous oxygen was raised as the coronary A-V oxygen difference declined. This ‘spontaneous’ change shifted the relationship of coronary flow to oxygen consumption. Furthermore, it led to a rise in coronary flow despite an elevation in coronary venous oxygen. It would seem that at this time the energy metabolism of the heart must change in that less oxygen is extracted from the blood despite an increase in its availability. The heart may therefore operate anaerobically in part or may make use of other hydrogen acceptors in the blood. The fact that this kind of metabolism may last as long as an hour or more, excludes the or- dinary type of ‘oxygen debt.’
T HE INFLUENCE of arterial blood pressure and cardiac output on coronary flow and cardiac gaseous metabolism, and the
interrelation between the latter two, have been studied recently in this department (1-3). The present study deals with the cha nges in coro- nary flow and cardiac oxygen consumption induced by changes in heart rate. No clear relationship of coronary flow to heart rate has emerged from the literature. This may be a result of the differences in physiological prepa- rations employed to measure coronary flow (4-6) and th e different methods used to obtain cardiac rate variations (7-1 I). In the heart- lung preparation oxygen consumption (I 2)
Received for publication December 5, 1955.
increases as heart rate is increased, and its in- crement tremely
is less at extremely low rates (13, 14).
high In a
than more
at ex- intact
preparation, Wegria (IS) has recently shown that electrically induced auricular tachycardia results in an increased coronary flow and cardiac oxygen consumption, while the cardiac work and efficiency is decreased.
The present study also employed a rela- tively intact preparation and the experiment was designed to determine the effects of heart rate over a wide range of work loads. Adjust- ments in cardiac output and blood pressure were predetermined and carefully controlled to keep them constant while the heart rate changes were produced. This was done in order
355
by 10.220.33.6 on Septem
ber 18, 2017http://ajplegacy.physiology.org/
Dow
nloaded from

356 LAURENT, BOLENE-WILLIAMS, WILLIAMS AND KATZ
CC/MN/l00 G HW g 140 -J
24
ci
g 22
2
5 0 20
0” 0 I8
RATE (BEATS/MINI
120 I40 160 I80 200
FIG. I. Graph showing relationships between coronary flow and heart rate (zapper curve), and between total oxygen consumption and heart rate (Zower curve).
to study the effect of heart rate on cardiac metabolism independently of these two deter- minants of work load.
METHODS
Ten mongrel dogs, ranging in weight from 13.0-17.7 kg, anesthetized with sodium pentobarbital (30 mg/kg) were used in these experiments. The coronary flow was measured by the method previously described (16, 3)
and expressed in cc/min/Ioo gm of heart weight (HW). Variations in heart rate were induced by sino-auricular or auricular stimulation. Platinum wire electrodes attached to a curved hemostat were used. After making a small slit in the pericardium these electrodes were clamped with slight tension to the area of junction between the superior vena cava and the right auricle.
The characteristics of the artificial pacemaker1 were such that a square-wave impulse of 2o-msec. duration could be delivered at any desired frequency. The voltages and milliamperages as delivered varied from &IO and 1-2, respectively, but were kept constant during each experiment. In one experiment a stimulat- ing needle electrode was inserted into the upper part of the interventricular septum and an indifferent needle electrode was inserted into the hind leg of the animal; however, the results of the stimulation were similar and the data of this experiment were used.
Pressures and electrocardiograms were recorded on a Sanborn twin-viso direct writer. Aortic blood pressures were obtained with a catheter inserted into the carotid artery. In some instances left ventricular pressure
l Artificial pacemaker was designed and constructed by Mr. M. Tausig of the Dept. of Developmental Engineering, Michael Reese Hospital. Details of the pacemaker are being published in the J. Lab. & Clin. Med.
curves were obtained with a catheter inserted into the ventricle by way of the left auricular appendage. In order to closely approximate the normal resistance of the pulmonary tree, a variable Starling resistance was introduced between the outflow of the right ventricle and the coronary flowmeter, which by itself offers little resistance to flow. This pressure was recorded with a needle inserted into the inflow arm of the flowmeter and designated as ‘pulmonary arterial pressure.’ Ordinary limb and aV limb leads were recorded and used to check the induced heart rates. The dog was kept in a steady state with regard to heart rate, arterial pressures and coronary flow for 10-15 minutes before simultaneous arterial and coronary venous blood sam- ples were drawn from the carotid artery and the inflow arm of the coronary flowmeter, respectively. Constant and regular auricular rates were obtained in all but three instances; one of these exhibited auricular fibrilla- tion (average ventricular rate rro/min.) while the other two showed occasional isolated auricular premature systoles.
The level of anesthesia and the circulating blood temperature were kept constant in each experiment. Artificial respiration, using a gas mixture of 95% oxy-
gen and 5% carbon dioxide, was carried out by tracheal intubation. Blood gases were determined by the method of Van Slyke and Neil1 (I 7) and the myo- cardial oxygen consumption was calculated in volume percentage per 100 gm HW, the latter determined directly. Oxygen capacity was determined on every third sample. The work of the heart was calculated in kilogram meters per hour per IOO gm. HW, the oxygen work equivalent in liters per hour per IOO gm HW, and its ‘efficiency,’ the ratio of work done/oxygen consumed, by methods previously described (18). Work was calcu- lated as the sum of the work of each ventricle. Kinetic work was neglected because of its insignificant magni- tude.
The hematocrits in these experiments were within the normal range in all animals and did not vary by more than 10% in any given experiment. The arterial 02 saturations rarely fell below 9070, and when it did the corresponding data were discarded.
In each experiment two, and sometimes three, levels of cardiac output were used, varying between 800 and 1600 cc/min. The cardiac output was ad- justed by altering the speed of the pump delivering blood through the lungs to the left heart. The aortic pressure was kept constant in each experiment by adjusting a clamp regulating the degree of constriction of the aorta. The mean blood pressure range in the different experiments was between 52 and 108 mm Hg. The ‘pulmonary arterial pressure’ was kept within a relatively narrow range in each experiment byadjust- ing the Starling-resistance. The range in all but two of the experiments was between 5 and 25 mm Hg; in the two exceptions it varied between 25 and 40
mm Hg. In this way, the variations of calculated values of total work for any stated work level were within %&.
Effect -of Electrical Stimulatior . A true pulsus alternans, accompanied by a left ventricular but not by an electrical alternans, was often seen when the heart was beating at rates of 200 beats/min. or more.
by 10.220.33.6 on Septem
ber 18, 2017http://ajplegacy.physiology.org/
Dow
nloaded from

CORONARY FLOW, CARDIAC OXYGEN CONSUMPTION AND HEART RATE xc7
This alternans was often transitory and varied in degree even at the same rate of stimulation. Our experiments do not support the concept that the alternation is necessarily a sign of heart failure and necessarily associated with an increase in the venous return or end-diastolic pressure (or volume) above a critical level, because: a) this alternans was transitory and reversible; b) there was no evidence of a rise in the left ventricular end-diastolic pressure when alternans occurred; c) the same pattern of cardiac oxygen con- sumption change with heart rate occurred in the presence of alternation as in its absence. However since the calculations of work are based on electrically integrated pressures, small differences in ‘efficiency’ might have been overlooked.
Several experiments were carried out to test the effect of electrical stimulation per se on coronary flow and cardiac oxygen consumption. In two experiments the electrically induced heart rate (197 and 205 beats/ min., respectively) was maintained for at least 30 minutes, while cardiac output and systemic and ‘pulmonary arterial’ pressures were kept constant. It was found that during this period, coronary flow did not vary and coronary A-V oxygen differences checked within I vol. 70. This would indicate that electrical stimulation of the heart per se does not lead either to progressive coronary vasomotor changes or to pro- gressive changes in cardiac oxygen consumption.
The coronary flow was seen to change immediately when the rate of cardiac stimulation was altered at constant work levels, and it reverted to its previous value immediately when the heart rate returned to its previous level. The speed with which the coronary flow, and presumably the cardiac oxygen consumption, changed precludes any lasting effect of the previous rate of stimulation.
When electrical stimulation was utilized to obtain a heart rate identical with the dog’s own basal rate (with- out stimulation) no change in coronary flow occurred. Unfortunately these comparisons were possible only at rates below 150 beats/min. Therefore, this generaliza- tion has not been demonstrated for higher heart rates. However, a comparison of oxygen consumption utiliza- tion values in animals with electrically driven hearts at a rate below ISO beats/min. with those observed in other dogs setting their own pace revealed no significant differences; this is in accord with a report by others
(4.
RESULTS
Heart Rate, Coronary Flow and Myocardial Oxygen Consumption. The present experi- ments, incorporating 60 observations at heart rates between 77 and 310 beats/min., showed a definite relationship between heart rate and coronary flow, and between heart rate and myocardial oxygen consumption. Figure I illus- trates a single experiment at a relatively con- stant work level (61-67 kg m/hr/roo gm NW). Curzjes A and B are, respectively, the plots of coronary flow and oxygen consumption against heart rate. It can be seen that the slope of both
OO~YIN/l000 HW 30 -
I I RATE (BEATSLMIN)
I
76 100 I60 200 260 300
FIG. 2. Nomogram of cardiac isowork lines relating total myocardial oxygen consumption to heart rate. The heavy line represents experimental points with work level of 50 kg m/hr/roo gm HW; the cardiac oxygen consumption values from one experiment at this work level are plotted on the nomogram and are found to lie close (I a) to those that would be predicted.
curves decreased at extremely rapid heart rates. When treated statistically the 60 experi- mental observations of the three variables- heart rate, cardiac oxygen consumption and coronary flow- show a significant correlation2 regardless of the work load.
Despite wide variations in heart rate and work, the arteriovenous oxygen difference fluctuated within a narrow range. Thus, the increment of oxygen extraction by the myo- cardium was determined primarily by an increase in coronary flow rather than by an increase in coronary A-V oxygen difference.
Heart Rate, Cardiac Work and Myocardial Oxygen Consumption. At a given heart rate, the cardiac oxygen consumption and the coro- nary flow increased as the work level increased. The variation in work used in these experi- ments ranged from 25-130 kg m/hr/Ioo gm HW, a range wider than previously reported by us (3). These variations in heart work in- volved change in both cardiac output and blood pressure. This does not preclude differ-
2 Regression equations showing are best expressed logarithmically :
these relationships
log 02 = 0.306 + 0.420 log R (Y = 0.611)
log CF = 1.035 + 0.483 log R (r = 0.546)
where 02 = oxygen consumption cc/100 gm HW/min.; R = heart rate beats/min.; CF = coronary flow cc/100
gm HW/min. Both coefficients (Y) are statistically significant.
by 10.220.33.6 on Septem
ber 18, 2017http://ajplegacy.physiology.org/
Dow
nloaded from

358 LAURENT, BOLENE-WILLIAMS, WILLIAMS AND KATZ
CC/MIN/lOO 6 HW
consumption at high work levels than at low ones, but the percent of the oxygen consump- tion increment remains the same. For example, at a work level of 20 kg m/hr/roo gm HW an increase in rate from 75 to 300 beats/min. leads to an increase in oxygen consumption from 8.5 to 18 cc/100 gm HW, which repre- sents a rise of 112% [(IS - 8.5)/8.5 X 1001;
the same increment of heart rate at a work level of 60 kg m,/hr/Ioo gm HW results in a greater increase in oxygen consumption (i.e. I 1.5-24 cc/100 gm HW), but this rise repre-
WORK KOM/HR 1 L I fi. - * 1" sents 108% [(24 - II.~)/II.S X 1031. 30 40 50 60 70 80 90 100 110 120 130 The similarity of percent increase (33 %) in
FIG. 3. Nomogram of isorate lines relating total myocardial oxygen consumption to cardiac work (the latter is in kg m/hr/roo gm. HW). Cardiac oxygen consumption values of two experiments are plotted on the nomogram and are found to lie close (I a) to those that would be predicted.
ences in the amount of oxygen consumption when the work increase due to change in cardiac output was compared with that due to change in arterial pressure (cf. 2).
By using the 60 above-mentioned experi- mental points, two nomograms have been constructed.3
The nomogram of figure 2 (isowork curves) shows that with an increase in work more oxygen was extracted at the fast heart rates than at the slow ones, but the percentage increase of oxygen extracted for a given incre- ment of work was the same at all heart rates. For example, the cardiac oxygen consumption increases from 8.5 to 11.5 cc/100 gm HW with an increase in work from 20 to 60 kg m/hr/Ioo gm HW when the rate is kept at 75 beats/min., and represents a rise of 35% [(II.~ - 8.5)/ 8.5 X 1001; the same increment of work results in a much greater increase in the oxygen con- sumption (i.e. 18-24 cc/100 gm HW) when the heart rate is 300 beats/min., but this still rep- resents a rise of 33% [(24 - 18)/18 X no].
The nomogram of figure 3 (isorate curves) shows that a given increase in heart rate results in a greater increase in cardiac oxygen
3 These regression
nomograms equation:
were derived from the following
log 02 = 0.267 log IV + 0.544 1ogR - 0.441 (r = 0.813)
where W = work kg m/hr/Ioo gm HW. The standard error of estimate equals 1.4 cc of oxygen consumption and the coefficient of multiple correlation is statistically quite significant.
cardiac oxygen consumption when the work is tripled at a low rate (75 beats/min.) or at a high rate (300 beats/min.) is striking. When this is compared to the percentage increase (110%) bt o ained when the rate is increased fourfold at a low work level or a high work level, the greater cardiac oxygen requirement for work done at a higher rate level is empha- sized.
Heart Rate, Efficiency and Work. As noted in previous experiments with this preparation (3) the ‘efficiencies’ were low. However, the values change sufficiently under the conditions of these experiments to permit certain conclu- sions. Figure 4 is a plot of ‘efficiency’ against heart rate in one isowork experiment. Effi- ciency declines and approaches a level asymp- totically as the heart rate increases to about 200 beats/min. The highest efficiencies, in con- firmation of earlier experiments (2, IS), were found at the highest work levels.
Heart Rate and Stroke-Oxygen Consump- tion. Figure 5 illustrates a single experiment in which the total work was kept constant. The stroke-oxygen consumption-the oxygen con- sumed by the heart per stroke-is seen to decrease rapidly when the heart rate increases. The plots of stroke-oxygen consumption against heart rate exhibited the same trend in each experiment, approaching a level asymp- totically as the heart rate increases to about 250 beats/min.
Coronary Flow and Total Oxygen Consump- tion. There was a good correlation4 between coronary flow and oxygen consumption. This
4 This general follows :
relationship can be expressed
log CF = 1.161 + 0.774 02 (Y = 0.600).
by 10.220.33.6 on Septem
ber 18, 2017http://ajplegacy.physiology.org/
Dow
nloaded from

CORONARY FLOW, CARDIAC OXYGEN CONSUMPTION AND HEART RATE 359
correlation is valid beyond the physiological heart rates and work levels; but the closer the heart rate and work levels are to physiological conditions, the better is the correlation.
DISCUSSION
Oxygen Consumption Alterations With Heart Rate Changes. The results clearly demonstrate-at least under these experimen- tal conditions- that oxygen utilization of the heart, as well as the coronary flow, are closely regulated by the conditions of performance of the heart. Cardiac work and heart rate are the most obvious factors in this regard. The effect of each of these was investigated separately in these experiments as far as blood supply and oxygen utilization (and presumably oxygen requirements) of cardiac muscle are concerned.
The heart rate per se was shown to have an effect upon the oxygen extraction by the heart muscle, in confirmation of other reports (12-14). No matter how this relationship is expressed, either as the increment of total oxygen consumption at the fast heart rates, the decrement of stroke-oxygen consumption in tachycardia, or the lower ‘efficiency’ of the fast beating heart, the phenomenon cannot be explained entirely on the basis of the change in stroke-work, or of alteration in the relative durations of systole and diastole, at the differ- ent heart rates.
The stroke-oxygen consumption of the heart is not solely a function of the stroke-work. If this were the case, then each beat having the same stroke-work would consume the same quantity of oxygen regardless of the heart rate. That this relationship does not hold is seen clearly from figure 4. At a heart rate of 300 beats/min., cardiac work of 80 kg m/hr/Ioo gm HW, and stroke-work of 0.0044, the oxygen consumed per beat per IOO gm HW is equal to 25.0
300 or 0.08 cc; and at a heart rate of 75,
cardiac work of 20 kg m/hr/Ioo gm HW, and the same stroke-work, the stroke-oxygen con-
Q+ sumption is equal to? or 0.1 I cc. Thus, with
the same stroke-work different stroke-oxygen consumption occurs.
If the major part of energy utilization takes place during diastole as has been postulated recently (20), then stroke-oxygen consumption
3' s 2!
W
3
k W
21 I
RATE (BEATS/ MN) 1 I
200 250
FIG.
cardiac 4. Graph showing relationship between per cent ‘efficiency’ and heart rate.
should be a function of diastolic duration at constant cardiac work. At a heart rate of 150
beats/min. the total period of diastole per minute is 33 seconds, while at a rate of 300 beats/min. it is 36 seconds (21), an increase of 3 seconds (or approximately IO%). Yet our experiments have demonstrated that cardiac oxygen consumption increase about 50% be- tween 150 and 300 beats/min. The wide dif- ference between expected and observed incre- ments of oxygen consumption emphasize the unlikelihood of a cause and effect relationship between duration of diastole and cardiac oxy- gen utilization.
The greater work/oxygen consumption ratio at slow heart rates can not be based upon a simple mechanical concept. It would appear instead that heart rate acceleration augments the energy metabolism of the heart without the manifestation of the extra energy as output- or pressure-work. The interrelation- ship between work, heart rate and oxygen consumption can be more clearly understood on the assumption that the heart rate effect per se acts independently of the effect of heart work upon the cardiac oxygen consumption. Thus, the percentage rise in cardiac oxygen consumption for a given increment of heart work was unchanged at four widely different heart rates. Furthermore, the percentage rises in cardiac oxygen consumption for a given increment of heart rate was identical at differ- ent levels of cardiac work. Such an independ- ence between the cardiac oxygen utilization induced by change in heart rate and that in- duced by change in work, is in keeping with the possibility that heart rate and cardiac work compete for the oxygen.
One of the most important physiological adjustments in trained athletes is the ability to perform a greatly augmented amount of
by 10.220.33.6 on Septem
ber 18, 2017http://ajplegacy.physiology.org/
Dow
nloaded from

360 LAURENT, BOLENE-WILLIAMS, WILLIAMS AND KATZ
‘0.07 1 HR (BEATS&IN) 4 1 4 I50
FIG. 5. Graph showing relationship between cardiac stroke-oxygen consumption and heart rate.
body work without much increment in heart rate. This adjustment, on the basis of our results, may depend in part on the decreased energy requirements of the heart in doing this intense work at the slower heart rates main- tained by athletes. Indeed some of the dele- terious effects of sustained tachycardias may be explained in terms of the metabolic cost of performing heart work at excessive heart rates. The same type of relationship between oxygen consumption, heart rate and cardiac work, found in our experiments, may exist in the normal animal, as well as under certain abnor- mal conditions in man, as for example in paroxysmal auricular tachycardia. It seems unlikely that the degree of reduction in cardiac output and blood pressure occurring in parox- ysmal auricular tachycardia (I 5, 2 2) will decrease cardiac work sufficiently to offset the energy cost of increased heart rate.
Coronary Flow With Heart Rate Changes. Dynamic factors have been suggested as an explanation for augmented coronary flow dur- ing tachycardia. Wiggers concluded that the increased coronary flow when heart rate in- creased was not due to increased massaging of the coronary vessels (21). Gregg could not relate the increase in coronary flow with increase heart rate to changes in the relative duration of diastole and systole (23). Alteration in coronary vasomotor tone could be considered in view of the possible interference of the auto- nomic nervous system in order to explain the coronary flow changes immediately following the change in heart rate. However, this is not likely since the same coronary dilatation fol- lows acceleration of the heart induced either
spontaneously (24)) by direct electrical pacing (9-1 I, IS), or in recovery from central vagal stimulation (14). Furthermore, the good corre- lation found in these experiments between cardiac oxygen consumption and coronary flow within and outside the physiological range, requires an explanation which relates the vascular tone of the coronary bed with the cardiac metabolism (3, 23). Increased heart rate, like increased cardiac work, requires coro- nary vasodilatation to meet the augmented oxygen needs of the heart muscle.
There appears to be a maximum capacity for oxygen uptake on the part of the myocar- dium under ‘normal’ conditions. When the needs for oxygen surpasses that supplied by the existing rate of blood flow through the myocardium, an increase in blood flow results. This increase in coronary flow seems to have a physiological limit as evidenced by the small increment observed at extremely rapid heart rates. When the limit of normal physiological adjustment of cardiac oxygen consumption to oxygen availability is surpassed as with an increasing load or an extremely high heart rate, then the mechanism by which the myocardium obtains its oxygen may change qualitatively. This we have previously described as ‘span- taneous’ change (I, 2).
‘Spontaneous’ Change. In some experi- ments of the present series we were able to observe a phenomenon to which we have referred in previous work (I) as ‘spontaneous’ change in coronary flow. This phenomenon consists of: a) an abnormal increase in coronary flow, and b) a concomitant arterialization of coronary venous blood, of such a degree that it is readily seen visually on observing the coronary flowmeter measuring the coronary venous blood flow. In addition it has been previously reported (2) that under these condi- tions cardiac oxygen consumption declines even if work increases. All this we have con- firmed in the present study.
In our present studies, the blood gaseous determinations showed, in every case, a strik- ing increase in venous oxygen content associ- ated with a marked decrement in the coronary A-V oxygen difference. No clear pattern of change of the respiratory quotient of the heart was seen under such conditions. The cardiac oxygen consumption for a given cardiac work
by 10.220.33.6 on Septem
ber 18, 2017http://ajplegacy.physiology.org/
Dow
nloaded from

CORONARY FLOW, CARDIAC OXYGEN CONSUMPTION AND HEART RATE 361
TABLE I. SUMMARY OF THE FACTORS INVOLVED IN THE ‘SPONTANEOUS’ CHANGE
Duration of Stimulation
Total > IWO/o
I-- Exp. 3, sample 8
2 hr. 1 45 min.
Exp. 4, sample 6 I hr. ) 45 min. 79
30 min. C.O. rise 850-1200
St. >207
failed
I32 [2451
114 [2071
150
I33 bs 21
I33 b5 21
83 [ 79 1 3
I72 c 37 2 1
I94 [24Il
Sample 8 2 hr. 45 min. 77 As above
Exp. 5, sample 7 I hr. 30 min. Ao. const.
St. >252
failed
Sample I2 2 hr. 60 min. 32 St. >252
failed
St. >I79 failed
Ao. const.
4.8 (1s 03)
7-I (10.0)
9-s (154)
16.7
(19-Q
150 (102)
150 (127)
178 (137)
I77 (93)
148 (94)
150 (65)
176 (128)
290 (1%)
Exp. 6, sample 7 2 hr. 50 min. 31 End
50 min.
Exp. 7, sample 12 I hr. 70 min. 91 End
40 min.
Exp. 8, sample 7 I hr. I hr. Ao. const. 77 P
40 min. 15 min.
St. > . . . failed = stimulation unsuccessful when rate is over . . . beats/min.; Ao. Const. = aortic constric- tion which increased aortic pressure over 5 mm Hg; C.O. = cardiac output (the figures following C.O. are the values expressed in cc/min.); HR = heart rate; W = work; (A-V) 02 diff. = coronary A-V oxygen difference; 02 cons. = oxygen consumption; CF = coronary flow; T = transient, P = permanent; End = experiment termi- nated; HW = heart weight.
5.6 (16.0)
16.2
(20.0)
C.O. rise 1200-1500
Parameters
HR, beats/min.
W kg m/hr/Ioo gm
HW
59
42
(A-V)02
diff*+vol* 0
8.3 (15 -9)
02 cons., CF cc/hr/Ioo cc/min/Ioo gm HW gm HW
Type of ‘spontaneous’
change
12.5
(15 -3)
T
11.0
(12.3)
16.5
(IS l 5)
P
8-9 (12 -9)
15.8
(17.7)
P
6.2
(15 l 3)
11.1
(14 l 2)
T
8.0
(13.8)
11.9
(13 l o>
P
The numbers written in the column ‘Duration of Stimulation- > 150%' indicate the time elapsed from the onset of a rate > 15oa/~ of the dog’s natural basic heart rate to the occurrence of the ‘spontaneous’ change. ‘Pa- rameters’ represent the physiological conditions (work and rate) at the onset of the ‘spontaneous’ change, when the first sample is drawn and ‘Data’ represent the 02 and CF values in the same period. The heart rate figures in brackets below the other figures indicate the heart rate values prior to the first sampling of the period of ‘spon- taneous’ change. The figures in parentheses below the other figures represent the theoretical values derived from the nomograms at the experimental conditions of work and rate for the sample and from the correlation between 02 cons. and CF. In exp. 4, sample 8 is also included in order to show the accentuation of the phenomenon in- itiated with sample 6.
Data
load and heart rate were much reduced in oxygen consumption, as shown by the nomo- comparison with periods not displaying these grams. combination of changes. The conditions in This ‘spontaneous’ change was sometimes which these so-called ‘spontaneous’ changes transient (cf. exp. 3 and T), in which case the were seen are summarized in table I. An at- coronary flow gradually decreased to the ex- tempt has been made to evaluate the factors petted ‘normal’ value. In these cases, however, that could be responsible for them, and a no oxygen data was obtained during recovery. comparison was made between the actually More often the ‘spontaneous’ change persisted observed and expected values of coronary flow, for over an hour, or until the experiment was coronary A-V oxygen differences and cardiac terminated. In these latter cases we were able
by 10.220.33.6 on Septem
ber 18, 2017http://ajplegacy.physiology.org/
Dow
nloaded from

362 LAURENT, BOLENE-WILLIAMS, WILLIAMS AND KATZ
cc/MIN/loo G HW 200 7
g ---- ----s W=77KgM
Ei ,f-
-5 r’-
,2- /-
I50
5
is
’ W=52KgM
100 -
RATE (BEATS/ Ml N) I. I I I I 1
100 I20 140 160 I80 200 220
FIG. 6. Graphs showing relationship between coro- nary flow and heart rate, and between cardiac oxygen consumption and heart rate, before (solid Zincs) and after (dashed lines) the occurrence of ‘spontaneous’ change. In this case the ‘spontaneous’ change was initiated by increasing the cardiac output, and thereby increasing work from 52 to 77 kg m/hr/roo gm HW, at a rate of 207 beats/min.
to study the effects of change in work and heart rate.
Figure 6 illustrates the variations of coro- nary flow and oxygen consumption observed under isowork conditions when heart rate was changed, both before and after the appearance of this ‘spontaneous’ change. The same quali- tative relationships were obtained in both conditions. Thus, an increase in coronary flow and cardiac oxygen consumption was obtained during the ‘spontaneous’ change when heart rate was increased. However, the position of the isowork curves was shifted downward compared to the ‘normal’ state, and the usual relationship between cardiac oxygen consump- tion and coronary flow no longer held. The degree of ‘spontaneous’ change was so variable in the same animal and between animals that no quantitation of the degree of the shift could be established.
Twenty-seven samples were taken under conditions of ‘spontaneous’ change, and all but four fell below the expected values of car- diac oxygen consumption of the nomograms.
In one experiment (e@. 5) the ‘spontaneous’ change persisted for I hour and 50 minutes, and nine determinations were made at three different levels of work. In this experiment coronary A-V oxygen differences under normal conditions were 18 zt I vol. %, while during the ‘spontaneous’ change the difference became I I =t 2 vol. %, and finally 7 =l= 1.5 vol. %. The coronary flow values did not follow the same stepwise progressive deviation, and although consistently high, they varied from sample to sample. The cardiac oxygen consumption, by and large, showed the same shifting pattern as the coronary flow.
No single factor or group of factors were consistently implicated as the stimulus for the ‘spontaneous’ change. Various factors which may have been contributory (table I) are briefly considered: a) in every case, ‘spontane- ous’ change was observed to occur when elec- trically induced heart rates were greater than 150% of the dog’s own basic heart rate. While the phenomenon did not always occur at such extremely high heart rates, it seemed to appear more frequently when the excessive rate lasted more than 30 minutes. Even at lower rates, electrical stimulation lasting more than I hour also seemed to be contributory. b) In four instances, ‘spontaneous’ change occurred when an unsuccessful attempt was made to obtain a rapid ventricular regular rate with electrical stimulation. In fact the ‘spontaneous’ change persisted even when the ventricular rate was slowed and after the electrical stimulation was discontinued. c) More than one factor may have been operating simultaneously. In two instances, the change could have been trig- gered by an increment of work imposed by increasing cardiac output to a level $ higher than that previously existing. In two instances, the change could have been aided by an in- duced increase in aortic resistance, even though the resulting increase in work was not large. However, alternans was not necessarily associ- ated with the ‘spontaneous’ change.
In any discussion of ‘spontaneous’ change it is necessary to integrate the findings of this laboratory relating work, coronary flow and oxygen consumption with reference to the ‘normal’ state. The data presented in this report extends the correlation of coronary flow
rate to oxygen consumption to include a con-
by 10.220.33.6 on Septem
ber 18, 2017http://ajplegacy.physiology.org/
Dow
nloaded from
CORONARY FLOW, CARDIAC OXYGEN CONSUMPTION AND HEART RATE 363
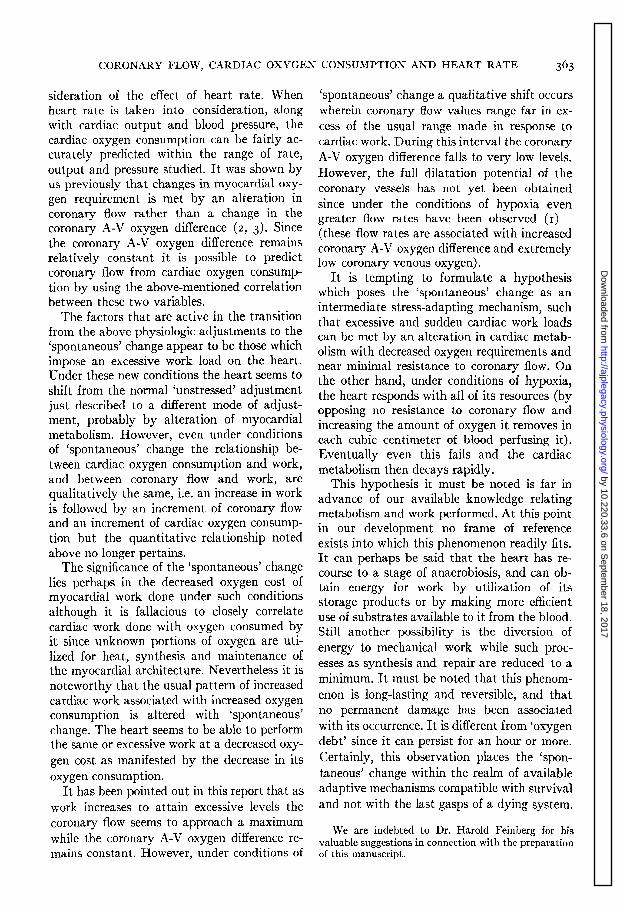
sideration of the effect of heart rate. When heart rate is taken into consideration, along with cardiac output and blood pressure, the cardiac oxygen consumption can be fairly ac- curately predicted within the range of rate, output and pressure studied. It was shown by us previously that changes in myocardial oxy- gen requirement is met by an alteration in coronary flow rather than a change in the coronary A-V oxygen difference (2, 3). Since the coronary A-V oxygen difference remains relatively constant it is possible to predict coronary flow from cardiac oxygen consump- tion by using the above-mentioned correlation between these two variables.
The factors that are active in the transition from the above physiologic adjustments to the ‘spontaneous’ change appear to be those which impose an excessive work load on the heart. Under these new conditions the heart seems to shift from the normal ‘unstressed’ adjustment just described to a different mode of adjust- ment, probably by alteration of myocardial metabolism. However, even under conditions of ‘spontaneous’ change the relationship be- tween cardiac oxygen consumption and work, and between coronary flow and work, are qualitatively the same, i.e. an increase in work is followed by an increment of coronary flow and an increment of cardiac oxygen consump- tion but the quantitative relationship noted above no longer pertains.
The significance of the ‘spontaneous’ change lies perhaps in the decreased oxygen cost of myocardial work done under such conditions although it is fallacious to closely correlate cardiac work done with oxygen consumed by it since unknown portions of oxygen are uti- lized for heat, synthesis and maintenance of the myocardial architecture. Nevertheless it is noteworthy that the usual pattern of increased cardiac work associated with increased oxygen consumption is altered with ‘spontaneous’ change. The heart seems to be able to perform the same or excessive work at a decreased oxy- gen cost as manifested by the decrease in its oxygen consumption.
It has been pointed out in this report that as work increases to attain excessive levels the coronary flow seems to approach a maximum while the coronary A-V oxygen difference re- mains constant. However, under conditions of
‘spontaneous’ change a qualitative shift occurs wherein coronary flow values range far in ex- cess of the usual range made in response to cardiac work. During this interval the coronary A-V oxygen difference falls to very low levels. However, the full dilatatio n poten .tial of the coronary vessels has not yet been obt.ained since under the conditions of hypoxia even greater flow rates have been observed (I)-
(these flow rates are associated with increased coronary A-V oxygen difference and extremely low coronary venous oxygen).
It is tempting to formulate a hypothesis which poses the ‘spontaneous’ change as an intermediate stress-adapting mechanism, such that excessive and sudden cardiac work loads can be met by an alteration in cardiac metab- olism with decreased oxygen requirements and near minimal resistance to coronary flow. On the other hand, under conditions of hypoxia, the heart responds with all of its resources (by opposing no resistance to coronary flow and increasing the amount of oxygen it removes in each cubic centimeter of blood perfusing it). Eventually even this fails and the cardiac metabolism then decays rapidly.
This hypothesis it must be noted is far in advance of our available knowledge relating metabolism and work performed. At this point in our development no frame of reference exists into which this phenomenon readily fits. It can perhaps be said that the heart has re- course to a stage of anaerobiosis, and can ob- tain energy for work by utilization of its storage products or by making more efficient use of substrates available to it from the blood. Still another possibility is the diversion of energy to mechanical work while such proc- esses as synthesis and repair are reduced to a minimum. It must be noted that this phenom- enon is long-lasting and reversible, and that no permanent damage has been associated with its occurrence. It is different from ‘oxygen debt’ since it can persist for an hour or more. Certainly, this observation places the ‘spon- taneous’ change within the realm of available adaptive mechanisms compatible with survival and not with the last gasps of a dying system.
We are indebted to Dr. Harold Feinberg for his valuable suggestions in connection with the preparation of this manuscript.
by 10.220.33.6 on Septem
ber 18, 2017http://ajplegacy.physiology.org/
Dow
nloaded from

364 LAURENT, BOLENE-WILLIAMS, WILLIAMS AND KATZ
REFERENCES
I. KATZ, A. M.,L. N. KATZ AND F. L. WILLIAMS. A,m. J. Physiol. So: 393, 1955.
2. KATZ, L. N., A. M. KATZ AND F. I,. WILLIAMS. Am. J. Physiol. 181: 539, 1955.
3. ALELLA, A., F. L. WILLIAMS, C. BOLENE-WILLIAMS AND L. N. KATZ. Am. J. Plzysiol. 183:57cr, IC)SS.
4. ANREP, G. V. AND H. HA~~SLER. J. Physiol. 67: 299,
19290 5. ANREP, G. V. AND B. KING. J. Physiol. 64: 341,
1927-28.
6. ANREP, G. V. AND H. N. SEGALL. Heart 13: 239, 1926.
7. NAKAGAWA, T. J. Physiol. 56: 340, 1922.
8. NAMMOUDA, M. AND B. KINOSITA. J. Physiol. 61; 615, 1926.
9. MILLER, G. H., F. M. SMITIF AND V. C. GRABER. Am. Heart J. 2: 479, 1927.
IO. HAUSNER, E., H. E. ESSEX, J. F. HERRICK AND E. G. BALDES. Am. J. Pltysiol. 131: 43, 1940-41.
I I. WEGRIA, R. AND R. P. KEATING. III Interamerican Cardiolog. Congress, Am. Heart J. 3 7 : 685, 1949.
12. COHN, A. E. AND J. M. STEELE. Am. J. Physiol.
113: 654, 1935.
13. KIESE, M. AND R. S. GARAN. Arch. exper. Pa,t/z. u. Pharmakol. 188: 226, 1938.
14. STARLING, E. H. AND M. B. VISSCIIER. J. Physiol. 62: 1926-27. 243,
15. WEGRIA, R., H. H. WANG AXD W. GLAVIAND. Absts. Am. Sot. Clin. Inv., May, 1955, Atlantic City, N. J.
16. RODBARD, S., G. K. GRAHAM AND F. WILLIAMS. J. Appl. Physiol. 6: 31 I, 1953.
17. VAN SLYKE, D. D. AND J. M. NEILL. J. Biol. Chem. 61: 523, 1924.
18. KATZ, L. N. AND M. MENDLOWITZ. Am. J.PhysioZ. 122: 262, 1938.
19. EVANS, C. L. AND Y. MATSUCE;A. J. Physiol. 49:
378, 19x4---Is* 20. HILL, D. K. J. Physiol. 98: 207, 1940.
21. WIGGERS, C. J. Circulatory Dynamics. New York:
Grune & Stratton, 1953.
22. STEWART, H. J. AND J. H. CRAWFORD. J. Clin. In- vestigation 3: 449, 1926.
23. GREGG, D. E. Coronary Circulation in Health and Disease. Philadelphia: Lea, 1950.
24. ECKENHOFF, J. E. Am. J. Physiol. 148: 582, 1947.
by 10.220.33.6 on Septem
ber 18, 2017http://ajplegacy.physiology.org/
Dow
nloaded from