Embed Size (px)
Citation preview

E
Ei
Ta
b
c
a
ARRA
KBCMMCR
1
rtodiatu
i
Hf
0d
Resuscitation 83 (2012) 1391– 1396
Contents lists available at SciVerse ScienceDirect
Resuscitation
jo u rn al hom epage : www.elsev ier .com/ locate / resusc i ta t ion
xperimental paper
ffects of bone marrow mesenchymal stem cells in a rat model of myocardialnfarction�
ong Wanga,b, Shijie Suna,c, Zhi Wana, Max Harry Weila,c, Wanchun Tanga,b,c,∗
Weil Institute of Critical Care Medicine, Rancho Mirage, CA, USADepartment of Emergency Medicine, The Second Affiliated Hospital of Sun Yat-sen University, Guangzhou, ChinaThe Keck School of Medicine of the University of Southern California, Los Angeles, CA, USA
r t i c l e i n f o
rticle history:eceived 11 July 2011eceived in revised form 15 February 2012ccepted 21 February 2012
eywords:one marrow mesenchymal stem cellsardiomyocytesyocardial infarctionyocardial function
ontractilityat
a b s t r a c t
Aim: Infusion of bone marrow mesenchymal stem cells (MSCs) improves myocardial function followingmyocardial infarction (MI). The mechanisms, however, remain controversial. This study was to investigatechanges of MSCs in vivo after administration into myocardial infarcted rats. Our hypothesis was that MSCsmight differentiate into contractile myocytes and improve myocardial function in vivo.Methods: MI was induced in 21 Sprague–Dawley rats by ligation of the left anterior descending artery.One week after ligation, 18 rats were randomized to receive MSCs labeled with PKH26 in a phosphatebuffer solution (PBS) by direct injection into the infarcted myocardium. The remaining 3 rats received PBSalone as placebo. An additional 3 non-ligated rats served as a normal group to obtain normal myocytes.Results: Every week for 6 weeks, hearts from 3 rats injected with MSCs were harvested to observe sin-gle cardiomyocytes. Although each week numerous round MSCs were found in the hearts of animalstreated with MSCs, beating cardiomyocyte-like cells labeled with PKH26 were observed at the sixthweek. The contractility of cardiomyocyte-like cells was the same to that of the unlabeled contractile
native cardiomyocytes at the sixth week and that of the normal group (10.71 ± 1.59 vs. 11.09 ± 3.42 vs.11.21 ± 2.16, p > 0.05). The contractility of cardiomyocyte-like cells was greater than cells both from thefirst week (10.71 ± 1.59 vs. 7.37 ± 3.47, p < 0.01) and the second week (10.71 ± 1.59 vs. 8.08 ± 3.11, p < 0.05)which was associated with significantly increased ejection fraction.Conclusions: MSCs can differentiate into beating cardiomyocytes in a rat model of MI and improve myocar-dial function.. Introduction
Mesenchymal stem cell transplantation provides a potentialegenerative therapy for the heart damaged by myocardial infarc-ion (MI).1 Our group previously demonstrated that transplantationf bone marrow mesenchymal stem cells (MSCs) improved myocar-ial function and the results of cardiopulmonary resuscitation
n a rat model of MI.2,3 These results agreed with other animalnd clinical studies.4–6 However, the underlying mechanisms of
he transplanted mesenchymal stem cells for treating MI remainnclear.� A Spanish translated version of the abstract of this article appears as Appendixn the final online version at doi:10.1016/j.resuscitation.2012.02.033.∗ Corresponding author at: Weil Institute of Critical Care Medicine, 35100 Bobope Drive, Rancho Mirage, CA 92270, USA. Tel.: +1 760 778 4911;
ax: +1 760 778 3468.E-mail address: [email protected] (W. Tang).
300-9572/$ – see front matter © 2012 Published by Elsevier Ireland Ltd.oi:10.1016/j.resuscitation.2012.02.033
© 2012 Published by Elsevier Ireland Ltd.
Earlier studies indicated that MSCs might have the capability ofreplacing dead cardiomyocytes,6 inducing revascularization of theinjured region,7,8 reorganizing damaged extracellular matrix,9,10
releasing soluble factors11,12 and therefore preventing delete-rious pathological remodeling after MI.13 Among the potentialmechanisms of myocardial function improvement, there is alsothe most controversial possibility that MSCs might be able todifferentiate into contractile cardiomyocytes and replace deadcardiomyocytes.14,15
Previous studies observed cardiomyocyte markers (e.g., Desmin,�-Actin, cTnI) on the surface of MSCs in myocardial bioptic tissueby utilizing immunohistochemistry to confirm the morphologicaldifferentiation of MSCs in vivo, but they did not convincingly ver-ify that the contractility of cardiomyocyte-like cells differentiatedfrom MSCs.6 Morphological differentiation of MSCs (morphologi-cal) and contractile differentiation of MSCs (functional) in vivo are
quite different.6,16 Many studies have confirmed that MSCs coulddifferentiate into beating cardiomyocyte-like cells in vitro.17,18Until this study, no scientist had confirmed that MSCs could differ-entiate into beating cardiomyocyte-like cells in vivo. The different

1 tation
eeaoidcoomtdodtac
2
cfAa0Io
2
piwtawdaoaLnc
npwtladcac
2M
ltc
392 T. Wang et al. / Resusci
nvironments of in vitro and in vivo effect the direction of differ-ntiation of MSCs. With the recent advances in cellular isolationnd culture techniques, direct measurement of the mechanicsf isolated ventricular myocytes is becoming an increasinglymportant technique in cardiac physiology.19 Video-based edge-etection technique (IonOptixTM, Milton, MA) which measureshanges in cardiomyocyte length during isotonic contractions, isne of the most commonly used approaches in studies of cardiomy-cyte contractility.20 In the current study, we isolated ventricularyocytes from infarcted rat hearts at varying time points after MSC
reatment. With this way, we were able to monitor and recordifferent contractile cardiomyocytes, including native cardiomy-cytes and cardiomyocyte-like cells differentiated from MSCs atifferent time points. The aim of our study was to observe differen-iation of MSCs from the first week to the sixth week after injectionnd to confirm the capability of MSCs to differentiate into beatingardiomyocytes in vivo and improve myocardial function.
. Methods
All animals received humane care in compliance with the Prin-iples of Laboratory Animal Care formulated by the National Societyor Medical Research and the Guide for the Care and Use of Laboratorynimals prepared by the Institute of Laboratory Animal Resourcesnd published by the National Institutes of Health (NIH publication-309-05337-3, Revised 1996). The protocol was approved by thenstitutional Animal Care and Use Committee of the Weil Institutef Critical Care Medicine.
.1. Myocardial infarction model
The animal model of MI was utilized as we have describedreviously.2,3 Twenty-one male Sprague–Dawley rats weigh-
ng 350–450 g were fasted overnight except for free access toater. The animals were anesthetized by intraperitoneal injec-
ion of pentobarbital (45 mg/kg). Additional doses (10 mg/kg) weredministered at intervals of 1 h to maintain anesthesia. The tracheaas orally intubated with a 14 g cannula mounted on a blunt nee-le with a 145◦ angled tip and animals were ventilated with roomir at a tidal volume of 0.65 mL/100 g of body weight at a frequencyf 100 breaths/min. End-tidal PCO2 (PETCO2) was measured with
side-stream infrared CO2 analyzer (model 200, Instrumentationaboratories, Lexington, MA) interposed between the tracheal can-ula and the respirator. The electrocardiogram (ECG) lead II wasontinuously monitored.
After baseline measurements of myocardial function using aoninvasive transthoracic echocardiograph, a thoracotomy waserformed via the fourth left intercostal space. The pericardiumas incised and the left atrial appendage was elevated to expose
he left anterior descending coronary artery (LAD). The LAD wasigated using a 5/0 nylon suture. The chest was then closed around
soft tube which had been inserted into the chest cavity to with-raw accumulated air and/or blood. Successful LAD occlusion wasonfirmed by the elevation of the ST segment.2,3 The animals werellowed to recover from anesthesia and were then returned to theirages.
.2. Isolation, expansion, culture, identification and labeling ofSCs
Allogeneic MSCs were isolated, characterized, cultured, andabeled as we have described previously.2,3 MSCs were expandedo passage 3 before infusion into recipient animals. At this time,ultures were 95% homogenous for rat MSCs.
83 (2012) 1391– 1396
2.3. MSCs transplantation
One week after surgical intervention, the animals were anes-thetized; the trachea was orally intubated and PETCO2 wasmonitored as previously described.2,3 Myocardial function wasassessed by echocardiographic ejection fraction (EF). Thoracotomywas then performed as previously described. Eighteen animalswere randomized to receive 5 × 106 MSCs labeled with PKH26in a phosphate buffer solution (PBS) by direct injection into theinfarcted myocardium. The 3 remaining animals received PBS aloneas a placebo (control group). The animals were allowed to recoverfrom anesthesia prior to being returned to their cages.
2.4. Isolation procedure of rat ventricular myocytes
Each week for 6 weeks following the MSC injection, the heartsfrom 3 rats were harvested for the purpose of observing single car-diomyocytes. On the sixth week after injection, the hearts from the3 animals treated with PBS only, were harvested and examined asa placebo group. An additional 3 rats were not ligated such as to actas a normal group to obtain normal myocytes.
Animals were intraperitoneally injected with heparin(1000 U/kg) 20 min prior to the anesthetization. The animalswere then anesthetized and the trachea was orally intubatedas previously described, and PETCO2 was monitored. Once theanimal was anesthetized, a thoracotomy was performed and therib cage was opened. The ascending aorta was then cannulatedafter stopping the heart beat with ice-cold saline, and the heartwas rapidly harvested and hooked up to a Langendorff perfusionapparatus (Kontes Glass Co., Vineland, NJ), modified by our groupas previously described.21 Once the heart was successfully can-nulated, it was perfused for 5 min at a rate of 11 mL/min withKrebs-Henseleit bicarbonate (KHB) buffer solution containing inmM: 118 NaCl, 4.7 KCl, 1.25 CaCl2, 1.2 MgSO4, 1.2 KH2PO4, 25NaHCO3, 10 N-[2-hydro-ethyl]-piperazine-N′-[2-ethanesulfonicacid] (HEPES) and 11.1 glucose, equilibrated with 5% CO2–95% O2,at 37 ◦C.
The heart was subsequently perfused with a Ca2+-free KHBbuffer for 3 min until cessation of spontaneous beating. The per-fusion was then continued for 15–20 min with Ca2+-free KHBcontaining 223 U/mL collagenase type II (Worthington BiochemicalCorp., Freehold, NJ). The ventricles were then rapidly harvested andfinely minced in Ca2+-free KHB buffer with 2% bovine serum albu-min plus 0.02 mg/mL trypsin (Mediatech, Hendon, VA) at a pH of 7.4,at 37 ◦C. The resulting suspension was filtered through a 300 �mnylon mesh and subsequently separated from the collagenase-trypsin solution by centrifugation at 600 rpm for 60 s. The depositwas re-suspended in sterile, filtered, Ca2+-free KHB supplementedwith 2% bovine serum albumin, and 10 �M CaCl2. The suspensionwas settled for 10 min on the basis that living cells precipitatequickly, whereas dead cells tend to float in the sedimentationbuffer. After removing the supernatant, the sediment was re-suspended in 10 mL sedimentation buffer with the addition of25 �M CaCl2. The sedimentation and re-suspension cycle was thenrepeated twice with 50 �M and 75 �M CaCl2, respectively. Afteranother 10 min of sedimentation, the sediment was re-suspendedin 50 mL normal culture medium. The suspension was transferredinto the culture dishes pre-coated by laminin. One h after sedi-mentation at 37 ◦C, the dead cells in the supernatant were gentlyremoved and fresh culture medium was added.22
2.5. Measurements
Prior to ligation, a blinded investigator measured myocardialfunction including left ventricular (LV) EF, left ventricular enddiastolic volume (LVEDV) and left ventricular end systolic volume
tation 83 (2012) 1391– 1396 1393
(HmtwLmm
wsaSews
lo(fiqte
2
vbfMr
3
dg(tvoifi
wSf“
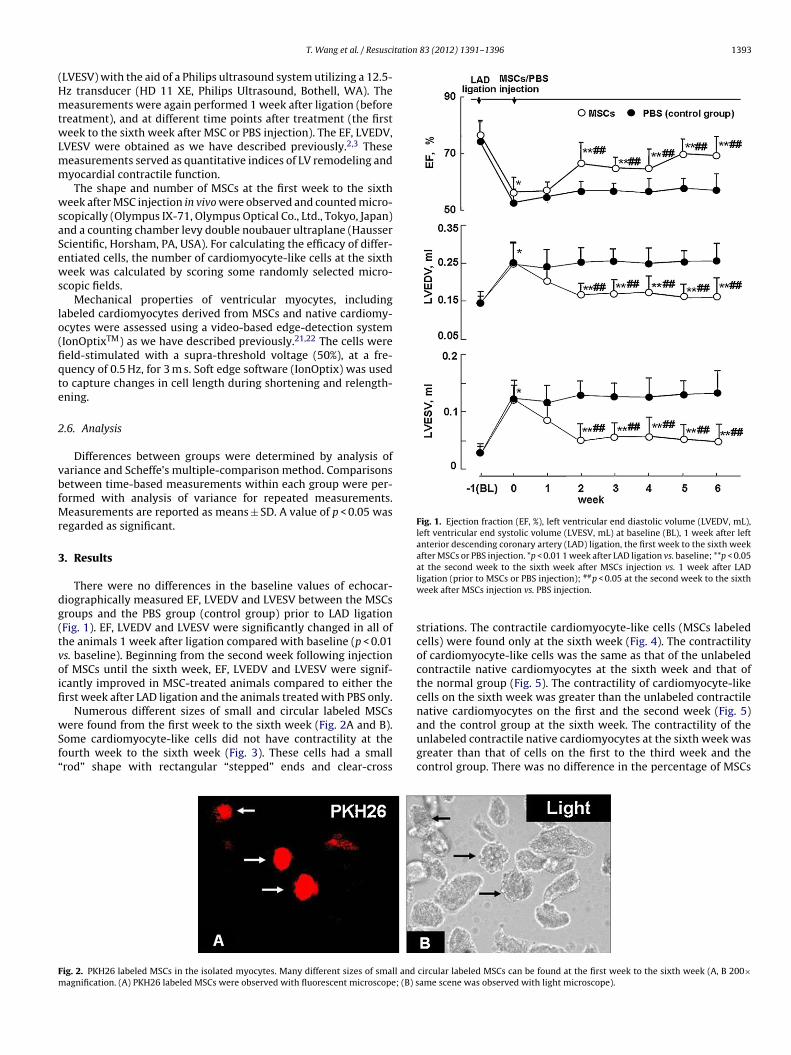
Fig. 1. Ejection fraction (EF, %), left ventricular end diastolic volume (LVEDV, mL),left ventricular end systolic volume (LVESV, mL) at baseline (BL), 1 week after leftanterior descending coronary artery (LAD) ligation, the first week to the sixth weekafter MSCs or PBS injection. *p < 0.01 1 week after LAD ligation vs. baseline; **p < 0.05at the second week to the sixth week after MSCs injection vs. 1 week after LAD
Fm
T. Wang et al. / Resusci
LVESV) with the aid of a Philips ultrasound system utilizing a 12.5-z transducer (HD 11 XE, Philips Ultrasound, Bothell, WA). Theeasurements were again performed 1 week after ligation (before
reatment), and at different time points after treatment (the firsteek to the sixth week after MSC or PBS injection). The EF, LVEDV,
VESV were obtained as we have described previously.2,3 Theseeasurements served as quantitative indices of LV remodeling andyocardial contractile function.The shape and number of MSCs at the first week to the sixth
eek after MSC injection in vivo were observed and counted micro-copically (Olympus IX-71, Olympus Optical Co., Ltd., Tokyo, Japan)nd a counting chamber levy double noubauer ultraplane (Haussercientific, Horsham, PA, USA). For calculating the efficacy of differ-ntiated cells, the number of cardiomyocyte-like cells at the sixtheek was calculated by scoring some randomly selected micro-
copic fields.Mechanical properties of ventricular myocytes, including
abeled cardiomyocytes derived from MSCs and native cardiomy-cytes were assessed using a video-based edge-detection systemIonOptixTM) as we have described previously.21,22 The cells wereeld-stimulated with a supra-threshold voltage (50%), at a fre-uency of 0.5 Hz, for 3 m s. Soft edge software (IonOptix) was usedo capture changes in cell length during shortening and relength-ning.
.6. Analysis
Differences between groups were determined by analysis ofariance and Scheffe’s multiple-comparison method. Comparisonsetween time-based measurements within each group were per-ormed with analysis of variance for repeated measurements.
easurements are reported as means ± SD. A value of p < 0.05 wasegarded as significant.
. Results
There were no differences in the baseline values of echocar-iographically measured EF, LVEDV and LVESV between the MSCsroups and the PBS group (control group) prior to LAD ligationFig. 1). EF, LVEDV and LVESV were significantly changed in all ofhe animals 1 week after ligation compared with baseline (p < 0.01s. baseline). Beginning from the second week following injectionf MSCs until the sixth week, EF, LVEDV and LVESV were signif-cantly improved in MSC-treated animals compared to either therst week after LAD ligation and the animals treated with PBS only.
Numerous different sizes of small and circular labeled MSCs
ere found from the first week to the sixth week (Fig. 2A and B).ome cardiomyocyte-like cells did not have contractility at theourth week to the sixth week (Fig. 3). These cells had a smallrod” shape with rectangular “stepped” ends and clear-cross
ig. 2. PKH26 labeled MSCs in the isolated myocytes. Many different sizes of small and
agnification. (A) PKH26 labeled MSCs were observed with fluorescent microscope; (B) s
ligation (prior to MSCs or PBS injection); ##p < 0.05 at the second week to the sixthweek after MSCs injection vs. PBS injection.
striations. The contractile cardiomyocyte-like cells (MSCs labeledcells) were found only at the sixth week (Fig. 4). The contractilityof cardiomyocyte-like cells was the same as that of the unlabeledcontractile native cardiomyocytes at the sixth week and that ofthe normal group (Fig. 5). The contractility of cardiomyocyte-likecells on the sixth week was greater than the unlabeled contractilenative cardiomyocytes on the first and the second week (Fig. 5)
and the control group at the sixth week. The contractility of theunlabeled contractile native cardiomyocytes at the sixth week wasgreater than that of cells on the first to the third week and thecontrol group. There was no difference in the percentage of MSCscircular labeled MSCs can be found at the first week to the sixth week (A, B 200×ame scene was observed with light microscope).

1394 T. Wang et al. / Resuscitation 83 (2012) 1391– 1396
Fig. 3. Labeled small cardiomyocyte-like MSCs in the isolated myocytes. A few numbers of small cardiomyocyte-like cells can be found at the fourth week to the sixth week.They had small “rod” shapes with rectangular “stepped” ends and clear cross-striation, but had no contractility (A, B 200× magnification. (A) Small cardiomyocyte-like cellwas observed with fluorescent microscope; (B) same scene was observed with light microscope).
F e cellc or (A,l ardio
opwsc
Feclfmc*c*cfvvct
ig. 4. Beating myocytes differentiated from MSCs. Normal sized cardiomyocyte-likells differentiated from MSCs can beat rhythmically when stimulated by stimulatabeled MSCs were observed with fluorescent microscope, b: the unlabeled native c
btained from the first week to the sixth week. There was a small
ercentage of MSCs differentiated into cardiomyocyte-like cellsith contractile properties at the sixth week (please see the onlineupplementary data, video 1 and video 2). The percent of thoseells was (8.8 ± 3.0)%.
ig. 5. Myocytes contractility (%). 90 cells were measured each week (30 cells forach rat). Values are means ± SD; unlabeled native cells means the native myocardialells obtained from the first week to the sixth week after MSCs treatment. MSCsabeled cells means the cardiomyocyte-like cells differentiated from MSCs obtainedrom the digested heart at 6 weeks after MSCs treatment. Normal cells means the
yocardial cells obtained from the normal heart. Control cells means the myocardialells obtained from the digested heart at 6 weeks after PBS treatment (control group)p < 0.01 unlabeled native cells obtained from the fifth week vs. unlabeled nativeells obtained from the first week and control cells obtained from control group;*p < 0.01 unlabeled native cells obtained from the sixth week vs. unlabeled nativeells obtained from the first week and the second week and control cells obtainedrom control group; †p < 0.05 unlabeled native cells obtained from the sixth weeks. unlabeled native cells obtained from the third week; #p < 0.01 MSCs labeled cellss. unlabeled native cells obtained from first week and control cells obtained fromontrol group; ‡p < 0.05 MSCs labeled cells vs. unlabeled native cells obtained fromhe second week.
s differentiated from MSCs can be found at the sixth week. The cardiomyocyte-like B 200× magnification. (A) a: Cardiomyocyte-like cells differentiated from PKH26myocytes; (B) same scene was observed with light microscope).
4. Discussion
The present study is the first one to confirm that MSCs can dif-ferentiate into beating cardiomyocytes in vivo at the sixth weekafter direct injection into the heart, and that the contractile effectsderived from MSCs are comparable to those of the native myocytes.
Animal and clinical studies have suggested that the trans-plantation of MSCs after MI might improve cardiac functionand minimize the ventricular remodeling by regenerating themyocardium itself.2,3,23 The differentiation of MSCs into cardiomy-ocytes is one of the most likely underlying mechanisms in vivo, butit has never been proven.
Evidence showed that MSCs expressed cardiomyocyte markersin vitro when cultured in the presence of the DNA demethy-lating agent 5-azacytidine.17,18,24 These cells form myotube-likestructures, began to beat spontaneously after 2 weeks, andbeat synchronously after 3 weeks.24 Studies in vivo revealed byhistopathology and immunohistochemistry that MSCs in heartsexpressed myocyte specific proteins, including desmin, cTnI and�-sarcomeric actin.6,25,26
Even though morphological resemblance and myocyte specificproteins were validated, the differentiation of MSCs into contrac-tile myocytes in vivo would not have been securely verified. It iscontroversial that MSCs can differentiate into beating cardiomy-ocytes in a MI model in vivo. The Feygin group’s study indicatedthat MSCs did not provide a structural contribution to the dam-aged heart and that the observed beneficial effects likely resultedfrom paracrine repair mechanisms.27 Many other studies havesupported the paracrine repair mechanism of MSCs in treatingMI.12,28,29 Mills et al. reported that MSCs enhanced electrical via-
bility in a rat model of MI by the gap junction formation betweenMSCs and native myocytes.30 Song and his group’s study foundthat poor to moderate survival benefits of MSC-implanted ratswere caused by incomplete electromechanical integration induced
tation
bimeuc
bt(vItMsfsblMituottbtcmpbiasmmtrcofttwimototroTtatftme
slti
1
1
1
1
1
1
T. Wang et al. / Resusci
y tissue heterogeneity between myocytes and engrafted MSCsn the infarcted myocardium, and cardiomyocytes from phorbol
yristate acetate-activated mesenchymal stem cells could restorelectromechanical function in infarcted rat hearts.31 Nevertheless,ntil now, no published study has directly confirmed that MSCsould differentiate into beating cardiomyocytes in vivo.
The development of cultured cardiac myocytes methodologyrings tremendous innovation to the observation of the charac-eristics of a single cardiomyocyte.19 Using special instrumentsIonOptixTM) and digestive methods (collagenase II), our group har-ested and cultured contractile myocytes from isolated hearts.21,22
n the present study, small and circular labeled MSCs were foundhroughout the 6 weeks after MSC injection, which suggested that
SCs remained viable in the myocardial microenvironment. Somemall cardiomyocyte-like cells did not show contractility from theourth week to the sixth week and these cells were small “rod”haped with rectangular “stepped” ends and clear cross-striation,ut had no contractility. At the sixth week, the cardiomyocyte-like
abeled cells were observed to be beating which confirmed thatSCs obtained the capability of contraction over 6 weeks of grow-
ng in vivo. The beat-to-beat shortening/relengthening changes ofhe cells differentiated from MSCs were the same as those of thenlabeled beating myocytes obtained from the same heart and thatf the myocytes obtained from the normal group, which confirmedhat the contractile effects derived from MSCs were comparable tohose of the native myocytes and normal myocytes. A small num-er of cardiomyocyte-like cells derived from MSCs were found inhis study, the probable reason was that we obtained the activeardiomyocytes with digestive methods (collagenase II), and thisethod may, in part, damage or kill active cardiomyocytes. The
resent study therefore proved that MSCs could differentiate intoeating cardiomyocytes, which might replace dead myocytes in an
schemic zone, dynamically integrating with the native myocytes,nd improving myocardial function. In order to exclude the pos-ibility of PKH26-labeled contractile cells fused with residentyocytes, in the next study we will use confocal laser scanningicroscope or electron microscope to prove the differentiation of
he cells. Although cardiomyocytes differentiated from MSCs mayeplace dead myocytes, we are not sure these cells can electrome-hanical integrate with native myocytes very well. This is not thenly mechanism for MSC transplantation to improve myocardialunction. However, there may be some mechanisms other than con-ractile cardiomyocyte differentiation of MSCs that contribute tohe improvement of myocardial function. In our current study, 2eeks after MSC injection, better myocardial function was found
n the treated group,2,3 which indicated that the benefit of MSCs toyocardial function occurred earlier than the beating cardiomy-
cytes differentiated from MSCs at the sixth week. It is conceivablehat MSCs may benefit native myocytes through some pathwaysther than the contractile developments of themselves. Poten-ial paracrine effects of transplanted MSCs may play an importantole in improving the contractility of unlabeled native cardiomy-cytes and myocardial function from the second week.11,12,32–34
ransplanted MSCs may produce several different growth fac-ors, cytokines, chemokines and other proteins, including somenti-apoptotic factors by MSCs,35,36 which may increase the con-ractility of unlabeled native myocytes and improve myocardialunction.26,37 MSCs may induce revascularization7,8 and reorganizehe extracellular matrix,9,10 and may also contribute to improved
yocardial function. Further investigation is needed to reveal thexact mechanisms underlying the findings mentioned above.
The optimal time for MSC transplantation in rats with MI is
till unclear. Jiang et al. study indicated that one week after LADigation was an optimal time for MSC transplantation.38 At thisime point scar formation has not occurred and the inflammations reduced, which should facilitate integration of transplanted cells1
83 (2012) 1391– 1396 1395
and functional recovery.39 In our present study, we chose 1 weekpost-LAD ligation as the optimal time for MSC transplantation.
5. Conclusion
The current study has confirmed that MSCs can differentiate intobeating cardiomyocytes in vivo at the sixth week after direct injec-tion of MSCs into the heart, and the contractile effects derived fromMSCs are comparable to those of the myocytes obtained from anormal group.
Conflicts of interest
The authors report no conflicts of interest.
Acknowledgements
This study was supported in part by Mrs. Marilyn and Mr. JerryBlue, GDSF (no.: 8151008901000119), Rancho Mirage, CA.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, inthe online version, at doi:10.1016/j.resuscitation.2012.02.033.
References
1. Wen Z, Zheng S, Zhou C, Wang J, Wang T. Repair mechanisms of bonemarrow mesenchymal stem cells in myocardial infarction. J Cell Mol Med2011;15:1032–43.
2. Wang T, Tang W, Sun S, Ristagno G, Huang Z, Weil MH. Intravenous infusion ofbone marrow mesenchymal stem cells improves myocardial function in a ratmodel of myocardial ischemia. Crit Care Med 2007;35:2587–93.
3. Wang T, Tang W, Sun S, Ristagno G, Xu T, Weil MH. Improved outcomes ofcardiopulmonary resuscitation in rats with myocardial infarction treated withallogenic bone marrow mesenchymal stem cells. Crit Care Med 2009;37:833–9.
4. Zuo S, Jones WK, Li H, et al. Paracrine effect of Wnt11-overexpressing mesenchy-mal stem cells on ischemic injury. Stem Cells Dev 2011 [Epub ahead of print, June1].
5. Wolf D, Reinhard A, Seckinger A, Katus HA, Kuecherer H, Hansen A. Dose-dependent effects of intravenous allogenic mesenchymal stem cells in theinfarcted porcine heart. Stem Cells Dev 2009;18:321–9.
6. Dai W, Hale SL, Martin BJ, et al. Allogeneic mesenchymal stem cell transplanta-tion in postinfarcted rat myocardium: short- and long-term effects. Circulation2005;112:214–23.
7. Tang J, Xie Q, Pan G, Wang J, Wang M. Mesenchymal stem cells participate inangiogenesis and improve heart function in rat model of myocardial ischemiawith reperfusion. Eur J Cardiothorac Surg 2006;30:353–61.
8. Huang NF, Lam A, Fang Q, Sievers RE, Li S, Lee RJ. Bone marrow-derived mes-enchymal stem cells in fibrin augment angiogenesis in the chronically infarctedmyocardium. Regen Med 2009;4:527–38.
9. Vela DC, Silva GV, Assad JA, et al. Histopathological study of healing afterallogenic mesenchymal stem cell delivery in myocardial infarction in dogs. JHistochem Cytochem 2009;57:167–76.
0. Wang CC, Chen CH, Lin WW, et al. Direct intramyocardial injection of mes-enchymal stem cell sheet fragments improves cardiac functions after infarction.Cardiovasc Res 2008;77:515–24.
1. Sassoli C, Pini A, Mazzanti B, et al. Mesenchymal stromal cells affect cardiomy-ocyte growth through juxtacrine Notch-1/Jagged1 signaling and paracrinemechanisms: clues for cardiac regeneration. J Mol Cell Cardiol 2011 [Epub aheadof print, June 13].
2. Kim JK, Brown DA, Zuk PA, et al. The role of cytoprotective cytokines in cardiacischemia/reperfusion injury. J Surg Res 2008;148:164–71.
3. Liu XH, Bai CG, Xu ZY, et al. Therapeutic potential of angiogenin modified mes-enchymal stem cells: angiogenin improves mesenchymal stem cells survivalunder hypoxia and enhances vasculogenesis in myocardial infarction. MicrovascRes 2008;76:23–30.
4. Chang SA, Lee EJ, Kang HJ, et al. Impact of myocardial infarct proteins and oscil-lating pressure on the differentiation of mesenchymal stem cells: effect of acutemyocardial infarction on stem cell differentiation. Stem Cells 2008;26:1901–12.
5. Wang XJ, Li QP. The roles of mesenchymal stem cells (MSCs) therapy in ischemic
heart diseases. Biochem Biophys Res Commun 2007;359:189–93.6. Hahn JY, Cho HJ, Kang HJ, et al. Pre-treatment of mesenchymal stem cells with acombination of growth factors enhances gap junction formation, cytoprotectiveeffect on cardiomyocytes, and therapeutic efficacy for myocardial infarction. JAm Coll Cardiol 2008;51:933–43.

1 tation
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
396 T. Wang et al. / Resusci
7. Tokcaer-Keskin Z, Akar AR, Ayaloglu-Butun F, et al. Timing of induction of car-diomyocyte differentiation for in vitro cultured mesenchymal stem cells: aperspective for emergencies. Can J Physiol Pharmacol 2009;87:143–50.
8. Wang T, Xu Z, Jiang W, et al. Cell-to-cell contact induces mesenchymal stemcell to differentiate into cardiomyocyte and smooth muscle cell. Int J Cardiol2006;109:74–81.
9. Ren J, Wold LE. Measurement of cardiac mechanical function in isolated ventric-ular myocytes from rats and mice by computerized video-based imaging. BiolProced Online 2001;3:43–53.
0. Lu J, Zang WJ, Yu XJ, Jia B, Chorvatova A, Sun L. Effects of postconditioning ofadenosine and acetylcholine on the ischemic isolated rat ventricular myocytes.Eur J Pharmacol 2006;549:133–9.
1. Ristagno G, Wang T, Tang W, Sun S, Castillo C, Weil MH. High-energy defibrilla-tion impairs myocyte contractility and intracellular calcium dynamics. Crit CareMed 2008;36:S422–8.
2. Tsai MS, Sun S, Tang W, Ristagno G, Chen WJ, Weil MH. Free radicalsmediate postshock contractile impairment in cardiomyocytes. Crit Care Med2008;36:3213–9.
3. Amado LC, Schuleri KH, Saliaris AP, et al. Multimodality noninvasive imagingdemonstrates in vivo cardiac regeneration after mesenchymal stem cell therapy.J Am Coll Cardiol 2006;48:2116–24.
4. Makino S, Fukuda K, Miyoshi S, et al. Cardiomyocytes can be generated frommarrow stromal cells in vitro. J Clin Invest 1999;103:697–705.
5. Yang J, Zhou W, Zheng W, et al. Effects of myocardial transplantation of marrowmesenchymal stem cells transfected with vascular endothelial growth factor forthe improvement of heart function and angiogenesis after myocardial infarction.Cardiology 2007;107:17–29.
6. Jiang W, Ma A, Wang T, et al. Homing and differentiation of mesenchymal stem
cells delivered intravenously to ischemic myocardium in vivo: a time-seriesstudy. Pflügers Arch 2006;453:43–52.7. Feygin J, Mansoor A, Eckman P, Swingen C, Zhang J. Functional and bioenergeticmodulations in the infarct border zone following autologous mesenchymal stemcell transplantation. Am J Physiol Heart Circ Physiol 2007;293:H1772–80.
3
83 (2012) 1391– 1396
8. Haider HKh, Idris NM, Jiang S, Idris NM, Ashraf M. IGF-1-overexpressingmesenchymal stem cells accelerate bone marrow stem cell mobilization viaparacrine activation of SDF-1alpha/CXCR4 signaling to promote myocardialrepair. Circ Res 2008;103:1300–8.
9. Mishra PK. Bone marrow-derived mesenchymal stem cells for treatment of heartfailure: is it all paracrine actions and immunomodulation? J Cardiovasc Med(Hagerstown) 2008;9:122–8.
0. Mills WR, Mal N, Kiedrowski MJ, et al. Stem cell therapy enhances electricalviability in myocardial infarction. J Mol Cell Cardiol 2007;42:304–14.
1. Song H, Hwang HJ, Chang W, et al. Cardiomyocytes from phorbol myristateacetate-activated mesenchymal stem cells restore electromechanical functionin infarcted rat hearts. Proc Natl Acad Sci USA 2011;108:296–301.
2. Crisostomo PR, Wang M, Markel TA, et al. Stem cell mechanisms and paracrineeffects: potential in cardiac surgery. Shock 2007;28:375–83.
3. Schuleri KH, Boyle AJ, Hare JM. Mesenchymal stem cells for cardiac regenerativetherapy. Handb Exp Pharmacol 2007;180:195–218.
4. Ladage D, Brixius K, Steingen C, et al. Mesenchymal stem cells induce endothelialactivation via paracine mechanisms. Endothelium 2007;14:53–63.
5. Perin EC. The use of stem cell therapy for cardiovascular disease. Tex Heart InstJ 2005;32:390–2.
6. Ye NS, Chen J, Luo GA, Zhang RL, Zhao YF, Wang YM. Proteomic profiling of ratbone marrow mesenchymal stem cells induced by 5-azacytidine. Stem Cells Dev2006;15:665–76.
7. Kinnaird T, Stabile E, Burnett MS, et al. Marrow-derived stromal cells expressgenes encoding a broad spectrum of arteriogenic cytokines and promotein vitro and in vivo arteriogenesis through paracrine mechanisms. Circ Res2004;94:678–85.
8. Jiang CY, Gui C, He AN, et al. Optimal time for mesenchymal stem cell trans-
plantation in rats with myocardial infarction. J Zhejiang Univ Sci B 2008;9:630–7.9. Hu X, Wang J, Chen J, et al. Optimal temporal delivery of bone marrow mes-enchymal stem cells in rats with myocardial infarction. Eur J Cardiothorac Surg2007;31:438–43.







![Bone Marrow Mesenchymal Stem Cells Inhibit ......Bone Marrow Mesenchymal Stem Cells Inhibit ... and TLR4 response to acute otitis through activation of NF-𝜅B [15], we hypothesized](https://img.dokumen.tips/doc/110x75/60a8bcfbd0a1141ee6336b62/bone-marrow-mesenchymal-stem-cells-inhibit-bone-marrow-mesenchymal-stem.jpg)





















