Embed Size (px)
Citation preview
Veterinary Surgery, 21, 3, 195-200, 1992
Effects of Arytenoid Abduction and Modified Castellated Laryngofissure on the Rima Glottidis in Canine Cadavers
SCOTT LOZIER, DVM, and ERIC POPE, DVM, MS, Diplomate ACVS
The percentages of change in cross-sectional area and dorsoventral height of the rima glottidis were measured after seven types of laryngoplasty in 30 postmortem canine specimens. The mean increases in area after each procedure were, in decreasing order, bilateral cricoarytenoid disarticulation with interarytenoid sesamoid band transection before placement of arytenoid abduction sutures 350% f 42%, bilateral placement of arytenoid abduction sutures 318% f 40%, bilateral cricothyroid disarticulation before placement of arytenoid abduction sutures 255% f 51%, modified castellated laryngofissure 244% f 30%, unilateral cricoarytenoid dis- articulation with interarytenoid sesamoid band transection before placement of an arytenoid abduction suture 161% f 25%, unilateral placement of an arytenoid abduction suture 151% f 24% and unilateral cricothyroid disarticulation before placement of an arytenoid abduction suture 108% f 25%. Bilateral cricoarytenoid disarticulation with interarytenoid sesamoid band transection before placement of arytenoid abduction sutures resulted in a significantly greater increase in rima glottidis area than modified castellated laryngofissure and all unilateral ar- ytenoid abduction techniques. Modified castellated laryngofissure resulted in a significantly greater increase than unilateral placement of an arytenoid abduction suture and cricothyroid disarticulation before placement of an arytenoid abduction suture. Bilateral disarticulation of the cricothyroid joint before placement of arytenoid abduction sutures resulted in significant collapse of the dorsoventral height of the rima glottidis.
UMEROUS SURGICAL PROCEDURES have been de- N scribed to enlarge the rima glottidis in dogs with la- ryngeal paralysis, but comparisons of these techniques are
Abduction ofthe arytenoid cartilage with sutures that mimic the action of the cricoarytenoideus dorsalis muscle and modified castellated laryngofissure are popular surgical treatments for laryngeal paraly~is.~.~,~ When per- forming laryngoplasty, disarticulation of the cricothyroid joint is advised to increase surgical exposure.2 Division of the interarytenoid sesamoid band and disarticulation of the cricoarytenoid joints has been recommended to enhance enlargement of the rima glottidis.* A simple ar- ytenoid abduction without disarticulation or band division has also been recommended.6 The relative effect of these surgical procedures on the size of the rima glottidis has not been determined. In this study, we compare the per- centage increase in rima glottidis area after seven types of laryngoplasty in normal postmortem specimens.
Materials and Methods
Immediately after euthanasia, the tongue, larynx, and proximal esophagus and trachea of 30 mixed-breed dogs
were removed en bloc from animals that had been used in laboratory teaching exercises. The specimens were rinsed with saline, placed in a saline bath, and refrigerated overnight. They were warmed to room temperature and extraneous tissue was removed before use. Each esophagus was incised dorsally to expose the laryngeal aditus and rima glottidis. All larynges appeared to be functionally and anatomically normal.
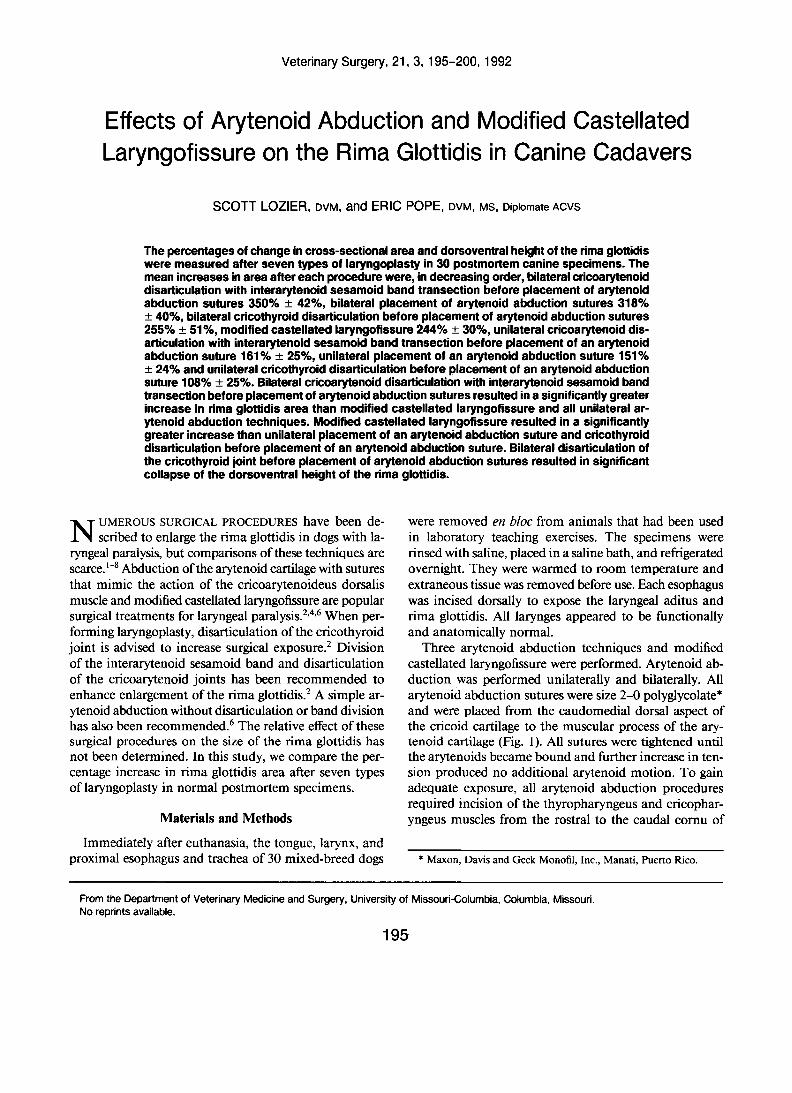
Three arytenoid abduction techniques and modified castellated laryngofissure were performed. Arytenoid ab- duction was performed unilaterally and bilaterally. All arytenoid abduction sutures were size 2-0 polyglycolate* and were placed from the caudomedial dorsal aspect of the cricoid cartilage to the muscular process of the ary- tenoid cartilage (Fig. 1). All sutures were tightened until the arytenoids became bound and further increase in ten- sion produced no additional arytenoid motion. To gain adequate exposure, all arytenoid abduction procedures required incision of the thyropharyngeus and cricophar- yngeus muscles from the rostral to the caudal cornu of
* Maxon, Davis and Geck Monofil, Inc., Manati, herto Rico.
From the Department of Veterinary Medicine and Surgery, University of Missouri-Columbia, Columbia, Missouri. No reprints available.
195
196 ARYTENOID ABDUCTION AND CASTELLATED LARYNGOFISSURE
W HA
A 0
Fig. 1. Canine laryngeal cartilages. (A) Lateral view. (B) Thyroid cartilage removed. Placement of an arytenoid abduction suture. AR = arytenoid cartilage; TH = thyroid cartilage; CR = cricoid cartilage; CAD = cricoarytenoideus dorsalis muscle; ISB = interarytenoid sesamoid band; CT = cricothyroid joint; CA = cricoarytenoid joint; EP = epiglottis; HA = hyoid apparatus.
the thyroid cartilage. Sharp and blunt dissection on the medial aspect of the thyroid cartilage allowed medial re- traction of the esophagus. This approach provided ex- posure of the cranial two-thirds of the cricoarytenoideus dorsalis muscle and the prominence of the muscular pro- cess of the arytenoid cartilage, and access to the cricothy- roid joint.
Simple arytenoid abduction suture placement was per- formed on 10 specimens as previously described, with no disarticulation or transection of the interarytenoid sesa- moid band.6 The abduction suture was guided through the cricoid cartilage by palpation. The muscular process of the arytenoid cartilage was visible. Proper suture place- ment was assured by appropriate motion of the arytenoid cartilage when tension was placed on the suture.
The second arytenoid abduction technique was per- formed on the same specimens. Immediately after doc- umenting results of simple placement of arytenoid ab- duction sutures, the sutures were removed. The cricothy- roid joint was disarticulated with Mayo scissors, and the sutures were replaced in the same fashion as in the first technique. These results were recorded as cricothyroid disarticulation before placement of arytenoid abduction sutures.
The third arytenoid abduction technique was per- formed on 10 new specimens. In this procedure, the cri- coarytenoid joint was disarticulated and the interarytenoid sesamoid band was transected before placement of ary- tenoid abduction sutures. The attachment of the crico- arytenoideus dorsalis muscle to the muscular process of the arytenoid cartilage and the underlying joint capsule were incised with Mayo scissors. The articular surfaces of the cricoarytenoid joint were visible. The ventral esoph-
ageal mucosa was carefully elevated to dorsal midline to expose the interarytenoid sesamoid band, which was sev- ered with Metzenbaum scissors. The cricothyroid joint was not disarticulated as in the original description.2 The abduction suture was placed through the mid-base of the triangular articular surface of the muscular process of the arytenoid cartilage.
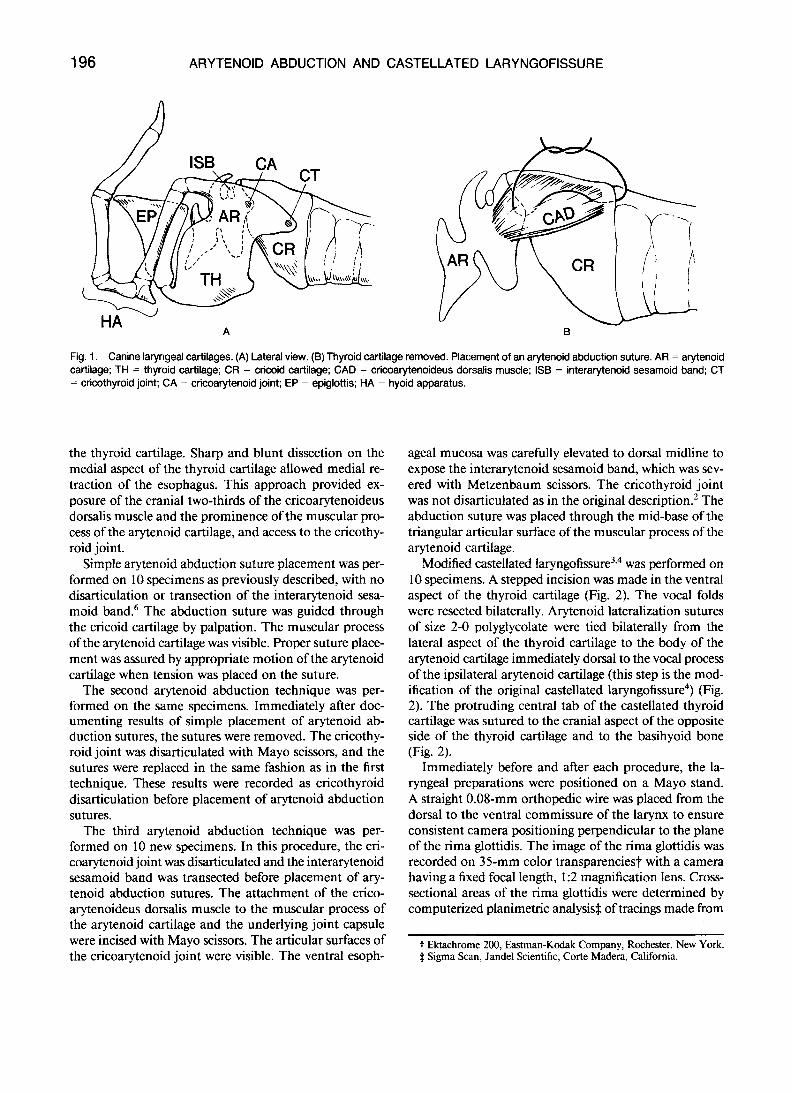
Modified Castellated laryngofi~sure~,~ was performed on 10 specimens. A stepped incision was made in the ventral aspect of the thyroid cartilage (Fig. 2). The vocal folds were resected bilaterally. Arytenoid lateralization sutures of size 2-0 polyglycolate were tied bilaterally from the lateral aspect of the thyroid cartilage to the body of the arytenoid cartilage immediately dorsal to the vocal process of the ipsilateral arytenoid cartilage (this step is the mod- ification of the original castellated laryngofi~sure~) (Fig. 2). The protruding central tab of the castellated thyroid cartilage was sutured to the cranial aspect of the opposite side of the thyroid cartilage and to the basihyoid bone (Fig. 2).
Immediately before and after each procedure, the la- ryngeal preparations were positioned on a Mayo stand. A straight 0.08-mm orthopedic wire was placed from the dorsal to the ventral commissure of the larynx to ensure consistent camera positioning perpendicular to the plane of the rima glottidis. The image of the rima glottidis was recorded on 35-mm color transparencies? with a camera having a fixed focal length, 1 :2 magnification lens. Cross- sectional areas of the rima glottidis were determined by computerized planimetric analysis3 of tracings made from
t Ektachrome 200, Eastman-Kodak Company, Rochester, New York. 4 Sigma Scan, Jandel Scientific, Corte Madera, California.
LOZIER AND POPE 197
\\ A / I 1
’ HA
TH
CR
I
B
Fig. 2. Modified castellated laryngofissure. (A) Stepped incision (bro- ken line) in the ventral aspect of the thyroid cartilage. (6) Ventral aspect of larynx after castellated laryngofissure. (C) Lateral aspect of larynx with arytenoid lateralization suture (modification of original castellated laryngofissure). AR = arytenoid cartilage; Cr = cricoid cartilage; HA = hyoid apparatus; TH = thyroid cartilage.
consistently magnified projections of the transparencies. The midline height of the rima glottidis was measured manually from the same tracings. The percentage change in surface area and dorsoventral height of the rima glottidis after each procedure was calculated. The data were grouped by surgical technique and compared statistically. Friedman’s and Wilcoxon’s signed rank tests were used to compare surface area data from dependent surgical techniques. Wilcoxon’s rank sum test was used to compare surface area data from unmatched surgical techniques. Wilcoxon’s signed rank test was used to determine if the changes in rima glottidis height were significantly different from zero. Statistical significance was accepted at p < .05.
Results
Bilateral simple placement of arytenoid abduction su- tures resulted in a mean increase. of 318% f 40% in the rima glottidis surface area, which was significantly greater than that of all unilateral arytenoid abduction techniques (Table 1 ). Bilateral cricothyroid disarticulation before placement of arytenoid abduction sutures resulted in a mean increase of 255% 4 5 1 % in the rima glottidis surface area, which was significantly greater than that of unilateral simple arytenoid abduction and unilateral cricothyroid disarticulation before placement of the arytenoid abduc-
TABLE 1. Percentage Increases (i SEM) in Surface Area of the Canine Rima Glottidis after Laryngoplasty
Technique Unilateral Bilateral
151 f 24 318 & 40’ AA CT/AA 108 f 25 255 f 51t CA/SB/AA 161 t 2 5 350 k 42$ MCL 244 ? 30t
AA = Simple arytenoid abduction. CT/AA = Cricoarytenoid joint disarticulation before arytenoid ab-
CA/SB/AA = Cricoarytenoid joint disarticulation and transection of
MCL = Modified castellated laryngofissure. Significantly higher than all unilateral techniques (p < .05)
t Significantly higher than unilateral AA and CT/AA (p < .05) * Significantly higher than MCL and all unilateral techniques (p < .05)
duction.
interarytenoid sesamoid band before arytenoid abduction.
tion suture. Bilateral cricoarytenoid disarticulation with interarytenoid sesamoid band transection before place- ment of arytenoid abduction sutures resulted in a mean increase of 350% k 42% in the rima glottidis surface area, which was significantly greater than that of modified cas- tellated laryngofissure and all unilateral arytenoid abduc- tion techniques. Modified castellated laryngofissure re- sulted in a mean increase of 244% * 30% in the rima glottidis surface area, which was significantly greater than that of unilateral simple arytenoid abduction and unilat- eral cricothyroid disarticulation before placement of the arytenoid abduction suture. All other compared changes in the rima glottidis were not significant.
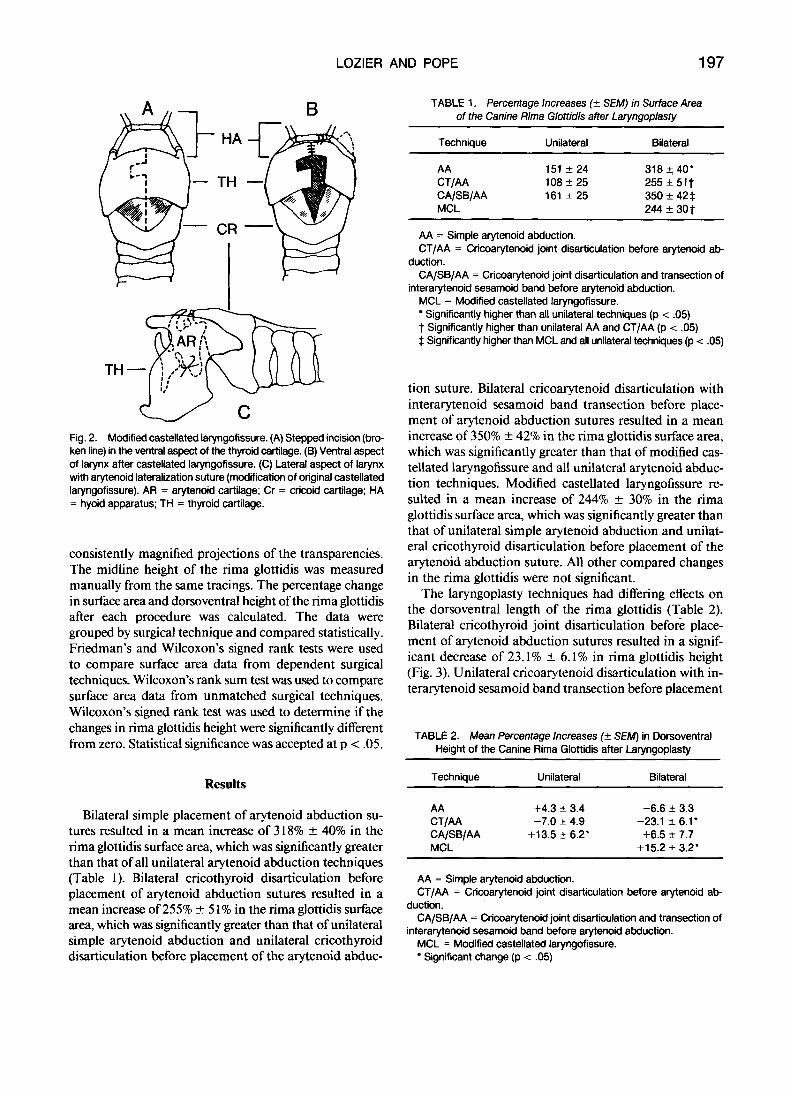
The laryngoplasty techniques had differing effects on the dorsoventral length of the rima glottidis (Table 2). Bilateral cricothyroid joint disarticulation before place- ment of arytenoid abduction sutures resulted in a signif- icant decrease of 23.1% f 6.1% in rima glottidis height (Fig. 3). Unilateral cricoarytenoid disarticulation with in- terarytenoid sesamoid band transection before placement
TABLE 2. Mean Percentage Increases (f SEM) in Dorsoventral Height of the Canine Rima Glottidis after Laryngoplasty
Bilateral Technique Unilateral
AA +4.3 * 3.4 -6.6 f 3.3 CT/AA -7.0 f 4.9 -23.1 ? 6.1’ CA/SB/AA +13.5 2 6.2’ +6.5 ? 7.7 MCL +15.2 f 3.2’
AA = Simple arytenoid abduction. CT/AA = Cricoarytenoid joint disarticulation before arytenoid ab-
CA/SB/AA = Cricoarytenoid joint disarticulation and transection of
MCL = Modified castellated laryngofissure. Significant change (p < .05)
duction.
interarytenoid sesamoid band before arytenoid abduction.

198 ARYTENOID ABDUCTION AND CASTELLATED LARYNGOFISSURE
Fig. 3. Postoperative appearance of laryngeal aditus after arytenoid abduction. (A) Bilateral simple arytenoid abduction. (B) Bilateral cricothyroid disarticulation performed before placement of arytenoid abduction sutures. There is dorsoventral flattening of the rima glottidis.
of the arytenoid abduction sutures resulted in a significant increase of 13.5% 2 6.2% in rima glottidis height. Modified castellated laryngofissure resulted in a significant increase of 15.2% k 3.2% in rima glottidis height. All other changes in rima glottidis height were not significant.
Subjectively, the modified castellated laryngofissure re- sulted in more distortion of the larynx and rima glottidis than arytenoid abduction. In five of the 10 specimens, the long axis of the rima glottidis and epiglottis became grossly malaligned (Fig. 4). Unilateral arytenoid abduction caused slight asymmetry of the rima glottidis, and bilateral abduction resulted in symmetric enlargement.
The modified castellated laryngofissure and cricoary- tenoid disarticulation with interarytenoid sesamoid band transection before placement of the arytenoid abduction sutures were more technically difficult than the other ar- ytenoid abduction procedures. Although the procedures were not timed, it took more time to perform them than other procedures.
Fig. 4. Laryngeal aditus after modified castellated laryngofissure. Five of ten specimens were distorted similarly.
Discussion
The cricoid and thyroid cartilages are overlapping half shells that form the dorsal and ventral aspects, respectively, of the short tubular larynx. Dorsal-ventral ovemding is prevented by firm bilateral attachment of the cartilages at the cricothyroid joint. The arytenoid cartilages are at- tached to the thyroid cartilage cranioventrally by the ven- tricular and vocal ligaments.' They project dorsally, cra- nial to the cricoid cartilage, to form a major portion of the adjustable opening to the larynx, the rima glottidis. In the resting state, this opening is a vertically oriented, elongated channel. When abducted, the arytenoid carti- lages are drawn dorsolaterally and louvered open. They move in an arc defined by the position and shape of the articular surface and the vector forces placed on them. The arytenoid cartilages are adjoined dorsally by the se- samoid band: which contains the interarytenoid cartilage, the sesamoid cartilage, and the ventricularis muscle.' This attachment makes the rima glottidis a structurally com- plete circuit and prevents totally independent motion of the arytenoid cartilages. Opposing outward forces applied by the cricoarytenoideus dorsalis muscles at the dorso- lateral aspects of the rima glottidis increase inward tension at the dorsal and ventral poles. As long as the tubular shape of the larynx is maintained by the appropriate cri- cothyroid cartilage relationship, the shape of the rima glottidis becomes more circular as the arytenoids abduct, and the rima glottidis surface area is optimized.
Small animal arytenoid lateralization techniques have evolved by borrowing an equine surgical technique in which a suture is placed from the origin to the insertion of the crioarytenoideus dorsalis muscle.2~6~10 In an attempt to clarify discussion, we have elected to call this an ary- tenoid abduction suture. In other arytenoid lateralization techniques, sutures are placed from the arytenoid carti- lages to various positions on the thyroid cartilage. 'A ' ','*

LOZIER AND POPE 199
Those sutures apply a more lateral force to the arytenoid cartilage that is less physiologic than the abduction arc effected by the cricoarytenoid abduction suture: Tech- niques using arytenoid-to-thyroid lateralization sutures were not included in this study because of a limited supply of fresh cadaver specimens.
Bilateral arytenoid abduction techniques resulted in a larger glottic lumen than modified castellated laryngofis- sure. This was consistent with recent findings that tidal- breathing, flow-volume loop parameters, partial pressure of inspired oxygen, and clinical results were better in dogs undergoing bilateral arytenoid abduction techniques than modified castellated laryngofissure.8 In the modified cas- tellated laryngofissure, the rima glottidis was enlarged di- rectly and indirectly. The castellation in the thyroid car- tilage stented the thyroid cartilage open, and resection of the vocal folds directly increased the rima glottidis size. The vocal processes of the arytenoid cartilage were drawn laterally and secured to, but limited by, the thyroid car- tilage. The vocal process is not part of the rima glottidis, but the corniculate and cuneiform processes of the ary- tenoids are indirectly drawn laterally with the vocal pro- cesses. Modified castellated laryngofissure provided en- largement of the subglottic laryngeal lumen, but it was not as effective in enlarging the rima glottidis as bilateral cricoarytenoid disarticulation with transection of the in- terarytenoid sesamoid band before placement of arytenoid abduction sutures. Modified castellated laryngofissure re- sulted in a significantly greater percentage increase in the rima glottidis than unilateral arytenoid abduction with or without cricothyroid disarticulation before suture place- ment. In this study, modified castellated laryngofissure did not result in a significantly larger rima glottidis than unilateral cricoarytenoid disarticulation with transection of the interarytenoid sesamoid band before placement of arytenoid abduction sutures (p = -07). It is possible that a larger sample size might have resulted in statistical sig- nificance at the -05 level.
The laryngeal distortion created by castellated laryn- gofissure seemed to result from the cranial transposition of the protruding central tab on the ventral aspect of the thyroid cartilage. Performing this procedure as described3 resulted in a 33% cranial shift of one side of the thyroid cartilage. That side of the base of the epiglottis was forced craniad, the tip of the epiglottis was forced craniad, and the tip of the epiglottis deviated away from the midline.
Of the arytenoid abduction techniques studied, cri- coarytenoid disarticulation with interarytenoid sesamoid band transection before placement of arytenoid abduction sutures resulted in the greatest enlargement of the rima glottidis. When the interarytenoid sesamoid band was severed, dorsolateral movement of the arytenoid cartilages caused larger increases in the height and surface area of the rima glottidis than other techniques. Incising the soft tissues surrounding the cricoarytenoid joint might allow
additional motion of the arytenoid cartilage. Disarticu- lation of the cricoarytenoid joint and transection of the interarytenoid sesamoid band were not studied separately, and further study is needed to determine the relative per- centage that each procedure contributes to the overall en- largement increase of the rirna glottidis.
Disarticulation of the cricothyroid joint disrupts the lateral support of the larynx. The lateral walls of the larynx can no longer withstand a tendency to buckle when out- ward tension is applied to the rima glottidis by arytenoid abduction sutures. The rima glottidis collapses dorsoven- trally as a result of flattening and overriding of the cricoid and thyroid cartilage half shells.
The decrease in height of the rima glottidis is minor with unilateral cricothyroid disarticulation before place- ment of the arytenoid abduction suture, but it may be- come extreme when performed bilaterally. The rima glot- tidis becomes a horizontally oriented elongated orifice with a decreased surface area (Fig. 3). Surgical exposure for arytenoid abduction is adequate without cricothyroid disarticulation. Although visualization of the caudodorsal aspect of the cricoid cartilage is not permitted without disarticulation, palpation assists accurate needle place- ment.
The results of this study might seem to suggest a relative value of one technique over another. However, the degree of clinical improvement in animals with laryngeal paral- ysis has not been proven to be proportional to the post- operative size of the rima glottidis. Intuitively, the size of the rima glottidis during maximal inspiratory effort is a reasonable surgical goal. Unfortunately, the percentage increase of the rima glottidis during maximum inspiratory effort in normal dogs is unknown. Furthermore, this study was performed on young to middle-aged healthy dogs without signs of laryngeal paralysis. It is possible that a different outcome would result if these procedures were performed on older dogs with brittle cartilage and some degree of soft-tissue fibrosis. Other factors must also be considered, including the potential of each technique to cause complications, the type of surgical approach and amount time required, the strength and status of the lar- ynx, and functional occupation of the dog.
Aspiration pneumonia is a frequent clinical sign and postoperative complication of laryngeal paralysis, and it
phagia, coughing, and gagging are common in the im- mediate postoperative period and are reported long term after many types of laryngopla~ty.'.~.~,'~-~~ In normal an- imals, aspiration is prevented by closure of the rima glot- tidis by the arytenoid cartilage and vocal fold adductors and by coverage of the rima glottidis by the epiglottis dur- ing swal10wing.l~ Animals with experimentally created laryngeal paralysis have an apparently normal swallowing mechanism after partial laryngectomy18 but a relatively high incidence of aspiration. I 4 , l 7 Modified castellated lar-
may be a significant factor in the progno~is.~*~~'~- '* D YS-

ARYTENOID ABDUCTION AND CASTELLATED LARYNGOFISSURE
yngofissure or arytenoid lateralization may cause distor- tion of the laryngeal aditus or interference with the swal- lowing mechanism, resulting in poor coverage by the epi- glottis and predisposing to aspiration. In one study, two of 12 dogs developed aspiration pneumonia after modified castellated laryngofissure: In the present study, modified castellated laryngofissure frequently resulted in enough laryngeal distortion that congruent apposition of the epi- glottis and the laryngeal aditus during swallowing would have been unlikely. Bilateral arytenoid abduction per- formed with sutures placed under maximal tension may cause supraphysiologic enlargement of the rima glottidis and increase the hazard of aspiration. More aspiration complications were noted with bilateral simple arytenoid abduction than with unilateral simple arytenoid abduc- tion.6 Other investigators suggest that only animals with preoperative signs of aspiration have aspiration tendencies after unilateral arytenoid abduction or laterali~ation.~,'~ Future studies are needed to detect aspiration accurately and determine the relative causal potential of these tech- niques.
The surgical approach for unilateral abduction is quick, requires one incision, and allows for further widening of the rima glottidis later by operating on the opposite side. Simultaneous bilateral arytenoid abduction is more dif- ficult to perform through one incision and may require two incisions and increased operating time. Disarticula- tion of the cricoarytenoid joint can be performed quickly and' easily. This provides visibility of the articular surface of the arytenoid cartilage and aids correct suture place- ment. Transection of the interarytenoid band is technically more difficult and time consuming. This procedure also may increase the risk of penetrating the laryngopharyngeal muco!sx6
Thyroid cartilage castellation and lateralization of the vocal processes of the arytenoid cartilages result in en- largement of the rima glottidis and the subglottic laryngeal lumen. In clinical cases, we inspect the larynx before la- ryngeal surgery and have not observed subglottic luminal compromise in cases of idiopathic laryngeal paralysis. Modified castellated laryngofissure is suggested when subglottic luminal compromise is present (e.g., traumatic fibrosis). In our hands, modified castellated laryngofissure is technically more demanding, more time consuming, and more traumatic than the arytenoid abduction tech- niques.
Older dogs frequently have brittle, calcified laryngeal cartilages. If arytenoid abduction sutures break the car- tilage of the muscular process even after predrilling with
a K-wire, modified castellated laryngofissure can be used as a second attempt. In such animals, the thyroid cartilage may also be brittle and castellation may fail. Partial ary- tenoidectomy may occasionally be required when other techniques fail.
References
I. Harvey CE. Partial laryngectomy in the dog: 11: Immediate increase in glottic area obtained compared with other laryngeal procedures. Vet Surg 1983; 12:192-196.
2. Lahue TR. Treatment of laryngeal paralysis in dogs by unilateral cricoarytenoid laryngoplasty. J Am Anim Hosp Assoc 1989;25: 3 17-324.
3. Gourley IM, Paul H, Gregory C. Castellated laryngofissure and vocal fold resection for the treatment of laryngeal paralysis in the dog. J Am Vet Med Assoc 1983; 182:1084-1086.
4. Smith MM, Gourley IM, Kurpershoek CJ, Amis TC. Evaluation of a modified castellated laryngofissure for alleviation of upper airway obstruction in dogs with laryngeal paralysis. J Am Vet Med Assoc
5 . Rosin E, Greenwood K. Bilateral arytenoid lateralization for laryngeal paralysis in the dog. J Am Vet Med Assoc 1982; 1805 15-5 18.
6. Payne JT, Martin RA, Rigg DL. Abductor muscle prosthesis for correction of laryngeal paralysis in 10 dogs and one cat. J Am Anim Hosp Assoc 199026:599-604.
7. Hedlund CS, Tangner CH, Montgomery DL, Hobson HP. A pro- cedure for tracheostomy and its effects on tracheal mucosa. Vet Surg 1982; 1 1: 13-1 7.
8. Burbidge HM. An evaluation of the effectiveness of castellated lar- yngofissure and bilateral arytenoid lateralisation for the relief of laryngeal paralysis in dogs. Vet Surg 1990 19:60. Abstract.
9. Evans HE, Christensen GC. Miller's Anatomy ojthe Dog. Philadel- phia: WB Saunders, 19793 18-526.
10. Marks D, Mackay-Smith MP, Cushing LS, Leslie JA. Use of a pros- thetic device for surgical correction of laryngeal hemiplegia in horses. J Am Vet Med Assoc 1970; 157:157-163.
1 1. Lane JG. ENT and Oral Surgery of the Dog and Cat: A Veferinary Practitioner Handbook. Bristol: John Wright and Sons, Ltd., 1982: 114.
12. Harvey CE, Venker-van Haagan A. Surgical management of pha- ryngeal and laryngeal airway obstruction on the dog. Vet Clin North Am 1975;5:515-534.
3. Greenfield CL. Canine laryngeal paralysis. Compend Cont Educ Pract Vet 1987:9;1011-1020.
4. Harvey CE. Treatment of laryngeal paralysis by partial laryngectomy. J Am Anim Hosp Assoc 1982; 18:551-562.
5 . White RAS. Unilateral lateralization: an assessment of technique and long term results in 62 dogs with laryngeal paralysis. J Small Anim Pract 1989;30:543-549.
16. Lane JG. Diseases and surgery of the larynx. Proceedings 53rd Annu Sci Meet Am Anim Hosp Assoc 1986;620-623.
17. Ross JT, Matthiesen DT, Noone KE, Scavelli TA. Complications and long-term results after partial laryngectomy for the treatment of idiopathic laryngeal paralysis in 45 dogs. Vet Surg 1991;20:
18. Harvey CE. Partial laryngectomy in the dog: I : healing and swal-
1986; 11:1279-1283.
169- 173.
lowing function in normal dogs. Vet Surg 1983;12:192-196.





























