Embed Size (px)
Citation preview

Original Article
EFFECTIVENESS OF THERAPEUTIC PLASMA EXCHANGE IN MYASTHENIA GRAVIS
R N Makroo*, V Raina**, A Kohli***, V Suri*** and P Kumar+
*Director, **Senior Consultant, Department of Transfusion Medicine, ***Senior Consultant, Department of Neurology,+Registrar, Department of Transfusion Medicine, Indraprastha Apollo Hospitals, Sarita Vihar, New Delhi 110 076, India.
Correspondence to: Dr. R N Makroo, Director, Department of Transfusion Medicine, Indraprastha Apollo Hospitals,Sarita Vihar, New Delhi 110 076, India.
Background: Myasthenia gravis is the most common primary disorder of neuromuscular transmission,caused by an acquired immunological abnormality. The patients have a weakness of muscles which cansometimes be life threatening. Treatment modalities include administration of anti- cholinesterase drugs,corticosteroids, immunosuppression drugs, thymectomy, therapeutic plasma exchange and intra venousimmunoglobulin (IVIg) and permutation and combination of all these therapies. Aim & Objective: Weconducted a retrospective study in Myasthenia gravis patients to find and compare the effectiveness of IVIgtreatment vis-à-vis therapeutic plasma exchange, at our hospital. Material & Methods: A total of 60 patients(35 males and 25 females) with a diagnosis of Myasthenia gravis, admitted between 1st January2000 to 31stDecember 2006 were retrospectively analyzed. Nineteen patients were treated by doing Therapeutic PlasmaExchange (TPE) of approximately 1-1.5 times the patient’s plasma volume on Haemonetics cell separator(MCS / MCS 3p) using FFP 80% & Normal Saline 20% as replacement fluid. All the patients had central line inplace for doing the procedure. The case files of all these patients were scrutinized and the treatment modalitieswere compared. The duration of illness, clinical features, need for assisted / mechanical ventilation, hospitalstay, number of therapeutic plasma exchanges performed were analyzed. Results: Twenty four of the 60Myasthenic patients (40%) improved clinically on anti-cholinesterase drugs alone. The other 36 patients (60%)underwent thymectomy followed by medications (anti-cholinesterase & cortico-steroids). Twelve of thesepatients improved their muscle power, recovered clinically and were discharged. Six of the remaining 24patients (average age 45.6 yrs.) were readmitted with myasthenic crisis or impending myasthenic crisis & wereput on TPE as next treatment modality and all 6 responded to treatment. Eighteen patients were given IVIgtherapy after they showed non-responsiveness to steroids & or immuno-suppressant drugs. Five of thesewere of younger age group (average age of 23.6 yrs) & recovered completely with IVIg treatment. Thirteenpatients did not show substantial improvement & had to be supplemented with TPE. Ten of these patientsresponded to treatment (average age of 46.1 yrs) while 3 succumbed to the disease process.Conclusion: TPE is a better option as the next line of treatment modality in older patients not responsive tothymectomy & medications. IVIg is the preferred line of treatment in the younger myasthenic patientsunresponsive to thymectomy and medications. TPE resulted in less hospital stay and thus decrease in overallexpense in treatment.
Key words: Myasthenia gravis (MG), Therapeutic Plasma Exchange(TPE), IntravenousImmunoglobulins(IVIg)
INTRODUCTION
MYASTHENIA Gravis (MG) is the most common primarydisorder of neuromuscular transmission. What was once arelatively obscure condition of interest primarily toneurologists is the best characterized and understoodautoimmune disease. A wide range of potentially effectivetreatments are available, many of which have implicationfor the treatment of other autoimmune disorders [1]. It is anacquired autoimmune disease with antibodies against thenicotinic acetylcholine receptor (AChR) at theneuromuscular junction [2]. The hallmark of myastheniagravis is muscle weakness that increases during periods ofactivity and improves after periods of rest. Certain musclessuch as those that control eye and eyelid movement, facial
expression, chewing, talking, and swallowing are often,but not always, involved. The muscles that controlbreathing and neck and limb movements may also beaffected. Treatment modalities include administration ofanti-cholinesterase drugs, corticosteroids, immuno-suppression drugs, thymectomy, therapeutic plasmaexchange and intra venous immunoglobulin (IVIg) andpermutation and combination of all these therapies.
MATERIAL AND METHODS
A total of 60 patients (35 males & 25 females) wereadmitted with a diagnosis of myasthenia gravis atIndraprastha Apollo Hospitals between 1st January 2000 to31st December 2006.We retrospectively analyzed the case
Apollo Medicine, Vol. 5, No. 2, June 2008 118

Original Article
119 Apollo Medicine, Vol. 5, No. 2, June 2008
records of all these patients. Nineteen patients were treatedby doing TPE of approximately 1-1.5 times the patient’splasma volume on Haemonetics cell separator (MCS + /MCS 3p) using FFP 80% & Normal Saline 20% asreplacement fluid. All the patients had central line in placefor doing the procedure. The case files of all these patientswere scrutinized and the treatment modalities werecompared. The duration of illness, clinical features, needfor assisted / mechanical ventilation, hospital stay, numberof therapeutic plasma exchange performed were analyzed.The patients were categorized as per the Myasthenia Gravisfoundation of America (MGFA) classification into variousclasses (as at the time of admission). Twenty four patientsfalling in MGFA class IV and class V (severe myastheniaand myasthenia crisis), received either IVIg or plasmaexchange or a combination of both.
RESULT
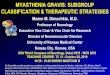
Twenty four of the 60 patients (40%) had improvedclinically on anti-cholinesterase drugs alone and did notrequire IVIg or therapeutic plasma exchange. The other 36patients (60%) underwent thymectomy followed bymedications (anti-cholinesterase & cortico-steroids).Twelve of these patients had significant improvement intheir muscle weakness & improved their power afterthymectomy and medications. No significant improvementoccurred in the other 24 patients. Six of the remaining 24patients (average age 45.6 yrs.) were readmitted withmyasthenic crisis or impending myasthenic crisis & wereput on TPE as next treatment modality and all 6 respondedto treatment. The average age of these 6 patients was 45.6years (youngest 22 yrs to oldest 60 yrs) & the earliestremission was noticed within 5 days of starting TPE. Theseimproved clinically and their average hospital stay was 7.1days after starting TPE. Eighteen patients were given IVIgtherapy after they showed non-responsiveness to steroids &or immuno-suppressant drugs. Five of these 18 patientsresponded well to treatment. Their average age was 23.6 yrs(youngest 7 yrs to oldest 49 yrs) & average hospital staywas 12.6 days of starting IVIg. Thirteen patients whoinitially received intravenous immunoglobulin (IVIg)following failure of response to medication andthymectomy had to be augmented with TPE as IVIg therapyalone was not effective in them. Three of these patients stilldid not improve in spite of extensive TPE and IVIg. Theaverage hospital stay of these 3 patients was 147.33 days.These patients died during their hospital stay. The hospitalstay of these three patients was 77 days, 137days, and 228days. Ten patients who had partial and or minimal benefitson IVIg once supplemented with TPE did show response.The average number of days for achieving a significantimprovement in power in these patients was 19.7 days. Theaverage age of these ten patients who required both IVIg
and TPE was 46.1 years (32 yrs to 65 yrs) (Fig. 1).
DISCUSSION
The present study was conducted with the objective toanalyze the treatment based distribution of cases ofmyasthenia gravis, encountered in our hospital from 2000to 2006 with reference to age, sex, IVIg, TPE,Thymectomy, and average hospital stay. Very few studieson the various treatment modalities have been carried outboth in India and abroad. The mean age of myastheniapatients in our study was 40 yrs (7 yrs to 68 yrs).
Therapeutic Plasma Exchange was effective in all agegroups. Patients of younger age group responded more toIVIg. As age advances, the probability of supplementingIVIg with TPE increased. The time to achieve clinicalimprovement with TPE was 7.1 days as compared to IVIg,which was 12.6 days. In patients whom IVIg was noteffective, the hospital stay as well as the cost of treatmentwent up. In contrast Murthy & colleagues found that inpatients with myasthenic crisis, both therapeutic options,TPE and IVIg, are equally effective in diseasestabilization[3].
Skeie et al 2006 recommended anticholinesterase drugsto be the first line to be given in the management of MG. PEis recommended as a short term treatment in MG speciallyin severe cases to induce remission and in preparation forsurgery. IVIg and PE are equally effective for the treatmentof myasthenia gravis exacerbations [4]. Yeh et al in 1999found daily plasmapheresis to be more effective in thetreatment of patients with advanced Myasthenia gravis [5].Howard recommended that IVIg appears to have a role asan acute treatment intervention in rapidly progressiveweakness or as a chronic maintenance therapy when allother treatment modalities have failed. Its response issimilar to but slower than the response of TPE [6].
CONCLUSION
TPE is a better option as the next line of treatmentmodality in older patients not responsive to thymectomy &medications. IVIg is the preferred line of treatment in theyounger myasthenic patients unresponsive to thymectomyand medications. TPE resulted in less hospital stay anddecrease in overall expense in treatment.
REFERENCE
1. James F Howard. Myasthenia gravis foundation ofAmerica, Myasthenia gravis-A Summary.11 Nov1997.
2. Kalb B, Matell G, Pirskanen R. Epidemiology ofMyasthenia Gravis: A Population Based Study inStockholm Sweden, Neuroepidemiology 2002; 21(5):221-225.

Apollo Medicine, Vol. 5, No. 2, June 2008 120
Original Article
3. Murthy JM, Meena AK Chowdary GV, Naryanan JT.Myasthenia crisis: Clinical features, complications andmortality. Neurology India. 2005; 53(1): 37-40.
4. Skeie GO, Apostolski S, Evoli A, Gilhus NE, Hart IK,Harms L, et al. Guidelines for treatment of autoimmuneneuromuscular transmission disorders. Europ. J.Neurology. 2006; 13(7): 691-699.
5. Yeh J-H. Compare the efficacy of different protocolsof plasmapheresis in the treatment of myastheniagravis. Acta Neurologica Scandinavica1999; 3 (3): 147-151.
6. Howard Jr JF. Intravenous immunoglobulins for thetreatment of acquired myasthenia gravis. Neurology. 51.(6) S30-S36.
60 Hospitalized MyastheniaGravis / Crisis Patients
Anti-cholinesterase drugs
24 patients improved clinically 36 patients did not improve
Thymectomy + medications
24 patients did not improve 12 patients showed clinicalimprovement & discharged
6 patients received only TPE 18 patients instituted IVIg therapy(Impending myasthenic crisis) (After non-responsiveness to steroids/immuno-suppressants)
All 6 patients recovered
5 patients recovered with only 13 patients did not showIVIg therapy substantial improvement
13 patients given TPE in addition to IVIg
10 patients recovered 3 patients had a fatal prognosis
Fig.1. An analysis of various treatment modalities received with their prognosis Myasthenia gravis patients.