-
part of
29ISSN 1758-190710.2217/DMT.13.62 © 2014 Future Medicine Ltd
Diabetes Manage. (2014) 4(1), 29–48Diabetes Manage.
Summary Aim: Medication adherence is associated with improved
outcomes in diabetes. Interventions have been established to help
improve medication adherence; however, the most effective
interventions in patients with Type 2 diabetes remain unclear.
The goal of this study was to distinguish whether interventions
were effective and identify areas for future research. Methods:
Medline was searched for articles published between January 2000
and May 2013, and a reproducible strategy was used. Study
eligibility criteria
1Center for Health Disparities Research, Medical University of
South Carolina, Charleston, SC, USA 2Division of General Internal
Medicine & Geriatrics, Department of Medicine, Medical
University of South Carolina, Charleston, SC, USA 3Center for
Disease Prevention & Health Interventions for Diverse
Populations, Charleston VA, REAP, Ralph H Johnson VAMC,
Charleston, SC, USA
*Author for correspondence: Tel.: +1 843 876 2969; Fax: +1 843
876 1201; [email protected]
Medication adherence is an important element in diabetes
management, but may not be solely responsible for achieving
glycemic control.
Three critical components of any intervention are education,
skills training and problem-solving. Most of the interventions in
this review focused on education rather than the other components.
Based on this finding, more research is needed to identify
effective interventions for improving medication adherence in
Type 2 diabetes. Interventions targeting diabetes
self-management are needed and must be developed.
One-on-one counseling was the method used in many of the
randomized controlled trials reviewed, and was found to be
effective.
Interventions led by pharmacists demonstrated the most
statistically significant results. Although small in number,
interventions using other types of facilitators such as nurse
educators, community health workers and certified diabetes
educators were also effective.
Uniform definitions for medication adherence must be
constructed.
Interventions should be simple and tailored to patients’
individual needs to increase the likelihood of effectiveness and
improved outcomes.
Clinical outcomes may not adequately reflect medication
adherence.
Benefits of medication adherence must continue to be
reinforced.
Prac
tice
Poi
nts
Effective interventions to improve medication adherence in
Type 2 diabetes: a systematic review
Review
Joni L Strom Williams1,2, Rebekah J Walker1,3, Brittany L
Smalls1,2, Jennifer A Campbell1,2 & Leonard E Egede*1,2,3
-
Diabetes Manage. (2014) 4(1) future science group30
review Williams, Walker, Smalls, Campbell & Egede
Medication adherence is one of several behaviors vital to
diabetes self-management and clinical outcomes. The variables
believed to contribute to adherence behaviors include treatment and
disease characteristics, intra- and inter-personal factors, and
environmental characteristics [1]. Patients, providers and health
systems, in addi-tion to the treatment plan itself, may contribute
to the success of adherence [2,3].
Adherence has been associated with better glycemic control,
fewer diabetes-related com-plications, reduced hospitalizations,
reduced healthcare costs, and lower all-cause mortality [4–8].
Despite the known benefits of medica-tion adherence in patients
with Type 2 dia-betes mellitus (T2DM), adherence rates vary, with
patients taking between 36 and 93%
of prescribed recommended doses [4]. Addi-tionally, national
clinical practice guidelines emphasize the need for composite
control of blood glucose, blood pressure and choles-terol to
improve glycemic control and reduce adverse outcomes, but only 43,
29 and 52% of patients with T2DM have controlled blood sugar (HbA1c
≥7%), blood pressure (systolic blood pressure
-
Interventions to improve medication adherence in Type 2
diabetes review
future science group www.futuremedicine.com 31
Given the complex assignment of role responsibility in
medication adherence and the variety of methods used to determine
adherence to medication regimens, we aimed to identify
interventions targeted at improving medication adherence and
T2DM-related clinical outcomes in adults. The goal of this
systematic review was to distinguish whether interventions were
effective and identify areas for future research.
Methods information sources, eligibility criteria
& searchA reproducible strategy was used to identify
interventions addressing medication adherence in patients with
T2DM. Studies were identified by searching Medline on 23 May 2013
for arti-cles published in the English language between 2000 and
2013. The search terms were based on the Cochrane Metabolic and
Endocrine Dis-order Group search strategy for T2DM [13] and the
Cochrane search strategy for medication compliance/adherence [14].
Some search terms in the Cochrane strategies were not used based on
the goals of this review. The search strategy is given in
Box 1.
Study selection & data collectionEligibility assessment was
performed by four independent authors (JLS Williams, RJ Walker, BL
Smalls and JA Campbell) in a standardized manner and disagreements
were resolved by the fifth author (LE Egede). The process used to
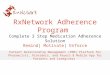
identify eligible citations is shown in Figure 1. Titles and
abstracts were reviewed using a stan-dardized checklist. Abstracts
were eliminated if
they did not investigate a T2DM patient popu-lation, measure
medication adherence/compli-ance as an outcome or describe an
intervention. Interventions included randomized controlled trials
(RCTs) and quasiexperimental studies, with and without a control
arm.
Data collected from the eligible articles are shown in Tables
1–4. For each study, data were extracted on the number of
participants, sam-ple population, duration of intervention,
set-ting of intervention, study design and type of control
(Table 1). An outcome table for medica-tion adherence was
created to include the mean baseline medication adherence score,
mean change (or baseline and postintervention if not reported) and
statistical significance (Table 2). Table 2 also reports
the method used to mea-sure medication adherence, categorized as
phar-macy claims, electronic monitoring, pill count, self-report or
serum/blood levels. If the article measured HbA1c, it was included
in Table 3, which provides mean baseline HbA1c, mean change
(or baseline and postintervention if not reported) and statistical
significance. Each article was analyzed for relevant intervention
characteristics, including whether it was cul-turally tailored,
educational or skills focused, device driven (i.e., mobile phone,
computers with internet access or landline telephone) and/or
personnel administered (i.e., commu-nity health worker [CHW] or
pharmacist) (Table 4). A narrative review was performed as the
heterogeneous measures used to determine medication adherence
precluded conducting a meta-ana lysis. Although risks of bias
exist, articles were not excluded due to the limited
148,990 articles identi�edfor diabetes
228,716 articles identi�edfor compliance/adherence
311,657 articles identi�edfor intervention
922 articles screened afterduplicates were removed
56 full articles reviewed
27 eligible studies includedin the systematic review
Eliminated 866 ineligibleabstracts
Eliminated 29 ineligiblearticles
Figure 1. Process for eligible article selection.
-
Diabetes Manage. (2014) 4(1) future science group32
review Williams, Walker, Smalls, Campbell & EgedeTa
ble
1. S
tudi
es m
eeti
ng in
clus
ion
crite
ria.
Stud
y (y
ear)
Pati
ents
(n)
Sam
ple
popu
lati
onD
urat
ion
Sett
ing
inte
rven
tion
des
crip
tion
Stud
y de
sign
Type
of c
ontr
olRe
f.
Al M
azro
ui
et al.
(200
9)24
0A
dults
with
T2D
M12
mon
ths
Mili
tary
hos
pita
l ou
tpat
ient
clin
ic
in th
e U
nite
d A
rab
Emira
tes
Patie
nts
rece
ived
edu
catio
n ab
out t
heir
illne
ss
from
a re
sear
ch p
harm
acis
t tha
t inc
lude
d co
mpl
icat
ions
, pro
per m
edic
atio
n do
sage
and
st
orag
e, a
s w
ell a
s a
heal
thy
lifes
tyle
RCT
Stan
dard
pr
ovid
er c
are
and
nonc
onta
ct
cont
rol g
roup
[15]
Aro
ra et a
l. (2
012)
23
Adu
lts w
ith T
2DM
3 w
eeks
Emer
genc
y de
part
men
t at L
os
Ang
eles
Cou
nty
Hos
pita
l (CA
, USA
)
Part
icip
ants
rece
ived
dai
ly te
xt m
essa
ges
with
he
alth
info
rmat
ion
incl
udin
g kn
owle
dge,
he
alth
y ea
ting,
exe
rcis
e, s
elf-
effica
cy a
nd
med
icat
ion
adhe
renc
e
Pre–
post
-tes
t N
one
[16]
Baba
mot
o et al.
(200
9)31
8H
ispa
nic/
Latin
os n
ewly
di
agno
sed
with
T2D
M6
mon
ths
Inne
r-ci
ty fa
mily
he
alth
cen
ter i
n Lo
s A
ngel
es (C
A, U
SA)
Dia
bete
s ed
ucat
ion
and
mon
itorin
g se
rvic
es
inco
rpor
atin
g pa
rtic
ipan
t pre
fere
nces
usi
ng
CHW
s or
CM
s
Pre–
post
-tes
t St
anda
rd
prov
ider
car
e an
d no
ncon
tact
co
ntro
l gro
up
[17]
Bogn
er et a
l. (2
010)
58A
fric
an–A
mer
ican
adu
lts
aged
50+
yea
rs w
ith
HbA
1c >
7 an
d di
agno
sis
of
depr
essi
on
4 w
eeks
Com
mun
ity-
base
d pr
imar
y ca
re p
ract
ice
in P
hila
delp
hia
(PA
, U
SA)
An
inte
grat
ed C
M w
orke
d w
ith p
atie
nt
and
prov
ider
to p
rovi
de e
duca
tion
abou
t de
pres
sion
and
dia
bete
s
RCT
Usu
al c
are
[18]
Bogn
er et a
l. (2
012)
180
Indi
vidu
als
with
T2D
M
≥30
year
s w
ith d
iagn
osis
of
dep
ress
ion
2-w
eek
run-
in,
3 m
onth
s
Prim
ary
care
pra
ctic
es
in P
hila
delp
hia
(PA
, U
SA)
Run-
in p
hase
and
inte
rven
tion
phas
e. In
tegr
ated
CM
wor
ked
with
pat
ient
and
pro
vide
r to
prov
ide
educ
atio
n ab
out d
epre
ssio
n an
d T2
DM
RCT
Usu
al c
are
[19]
Bren
nan
et al.
(201
2)In
terv
entio
n:
5123
Cont
rol:
24,1
24
Empl
oyee
s with
T2D
M
wor
king
in a
hea
vy
indu
stry
com
pany
in
the
mid
wes
t whe
re
CVS
Care
mar
k w
as th
e ph
arm
acy
bene
fit m
anag
er
18 m
onth
s12
CVS
reta
il ph
arm
acie
s in
no
rthw
est I
ndia
na
(USA
)
Ther
e w
ere
two
inte
rven
tion
grou
ps (r
etai
l an
d ph
arm
acy
bene
fit m
anag
emen
t)
and
four
inte
rven
tion
prog
ram
s: g
ener
al
info
rmat
ion;
initi
atio
n of
ACE
inhi
bito
rs a
nd/o
r st
atin
s; ad
here
nce
enfo
rcem
ent;
and
first
-fill
coun
selin
g
Pros
pect
ive
coho
rtU
sual
car
e[20]
Cast
illo et al.
(201
0)70
enr
olle
d an
d 47
co
mpl
eted
pr
e–po
st-
test
dat
a
His
pani
c/La
tino
resi
dent
s w
ith T
2DM
10 w
eeks
Com
mun
ity
self-
care
(n
oncl
inic
al) c
ente
rsCH
Ws
cond
ucte
d 2-
h T2
DM
edu
catio
n se
ssio
ns
addr
essi
ng s
elf-
man
agem
ent
Pre–
post
-tes
t de
sign
N/A
[21]
Chan
et a
l. (2
011)
105
Adu
lts w
ith a
t le
ast 5
dru
gs a
nd
HbA
1c ≥
8
9 m
onth
sPu
blic
hos
pita
l in
Hon
g Ko
ngSt
ruct
ured
pha
rmac
ist c
are
prog
ram
pro
vidi
ng
15–3
0 m
in w
ith p
harm
acis
t bef
ore
each
ph
ysic
ian
visi
t
RCT
Usu
al c
are
[22]
Farm
er et a
l. (2
012)
211
Indi
vidu
als
with
T2D
M
and
HbA
1c v
alue
≥7.
5%,
and
pres
crib
ed a
t lea
st
one
gluc
ose-
low
erin
g or
al
med
icat
ion
12 w
eeks
13 p
rimar
y ca
re
prac
tices
in
Oxf
ords
hire
, Bu
ckin
gham
shire
, Su
ffolk
, Ess
ex a
nd
Hun
tingd
onsh
ire
(UK)
Patie
nts
wer
e as
ked
ques
tions
abo
ut th
eir
belie
fs re
gard
ing
taki
ng m
edic
atio
n re
gula
rly,
posi
tive
beha
vior
s w
ere
rein
forc
ed a
nd
prob
lem
-sol
ving
was
use
d fo
r neg
ativ
e be
liefs
. Pat
ient
s w
ere
aske
d to
writ
e th
e ex
act
circ
umst
ance
s in
whi
ch th
ey w
ould
take
thei
r m
edic
atio
n
RCT
Usu
al c
are
[23]
BGSM
: Blo
od g
luco
se m
onito
ring;
CH
W: C
omm
unit
y he
alth
wor
ker;
CM
: Cas
e m
anag
er; D
MSM
: Dia
bet
es m
ellit
us s
elf-
man
agem
ent;
N/A
: Not
app
licab
le; R
CT:
Ran
dom
ized
con
trol
led
tria
l; T1
DM
: Typ
e 1
diab
etes
mel
litus
; T2
DM
: Typ
e 2
diab
etes
mel
litus
; TO
FHLA
: Tes
t of F
unct
iona
l Hea
lth L
itera
cy in
Adu
lts.
-
Interventions to improve medication adherence in Type 2
diabetes review
future science group www.futuremedicine.com 33
Tabl
e 1.
Stu
dies
mee
ting
incl
usio
n cr
iteri
a (c
ont.)
.
Stud
y (y
ear)
Pati
ents
(n)
Sam
ple
popu
lati
onD
urat
ion
Sett
ing
inte
rven
tion
des
crip
tion
Stud
y de
sign
Type
of c
ontr
olRe
f.
Gia
lam
as
et al.
(200
9)Re
crui
ted:
49
68D
ata
anal
yzed
: 43
81
Indi
vidu
als
with
T1D
M o
r T2
DM
with
hyp
erlip
idem
ia
or re
quiri
ng a
ntic
oagu
lant
th
erap
y
2 ye
ars
53 A
ustr
alia
n ge
nera
l pr
actic
es in
urb
an,
rura
l and
rem
ote
area
s
Bloo
d an
d ur
ine
sam
ples
test
ed u
sing
po
int-
of-c
are
devi
ces
with
in th
eir g
ener
al
prac
tices
RCT
Usu
al c
are:
bl
ood
test
ed
by u
sual
pa
thol
ogy
labo
rato
ry
[24]
Gla
sgow
et al.
(201
0)46
3H
eter
ogen
eous
sam
ple
of
adul
ts w
ith T
2DM
4 m
onth
s5
prim
ary
care
cl
inic
s w
ithin
Ka
iser
Per
man
ente
Co
lora
do (C
O, U
SA)
Inte
rnet
-bas
ed D
MSM
pro
gram
RCT
Enha
nced
usu
al
care
[25]
Gla
sgow
et al.
(201
2)46
3A
dults
age
d 25
–75
year
s w
ith a
BM
I of ≥
25 a
nd
biw
eekl
y ac
cess
to th
e in
tern
et
12 m
onth
sPr
imar
y cl
inic
s w
ithin
Ka
iser
Per
man
ente
Co
lora
do (C
O, U
SA)
Inte
rnet
-bas
ed, c
ompu
ter-
assi
sted
DM
SM
com
pare
d w
ith c
ompu
ter-
base
d pr
ogra
m w
ith
soci
al s
uppo
rt
Prag
mat
ic
RCT
Enha
nced
usu
al
care
: com
pute
r-ba
sed
risk
appr
aisa
l
[26]
Gra
nt et a
l. (2
003)
232
Indi
vidu
als w
ith T
2DM
who
ha
d un
derg
one
labo
rato
ry
test
ing
in th
e pr
eced
ing
year
and
had
vis
ited
the
clin
ic 6
mon
ths p
rece
ding
th
e st
udy
3 m
onth
sA
cade
mic
-affi
liate
d co
mm
unit
y he
alth
ce
nter
Phar
mac
ist a
dmin
iste
red
deta
iled
ques
tionn
aire
s, p
rovi
ded
tailo
red
educ
atio
n re
gard
ing
med
icat
ion
use
and
help
with
ap
poin
tmen
t ref
erra
l
Pros
pect
ive
RCT
Usu
al c
are
[27]
Jara
b et al.
(201
2)17
1A
dults
with
T2D
M
atte
ndin
g an
out
patie
nt
diab
etes
clin
ic
6 m
onth
sRo
yal M
edic
al
Serv
ices
Hos
pita
l (J
orda
n)
A c
linic
al p
harm
acis
t-le
d ph
arm
aceu
tical
car
e pr
ogra
m d
eliv
ered
ant
idia
betic
ther
apy
and
adju
nct t
hera
py to
pat
ient
s
RCT
Usu
al c
are
[28]
Kim
et a
l. (2
006)
45In
divi
dual
s ag
ed ≥
30 y
ears
w
ith in
tern
et a
t hom
e12
wee
ksU
rban
are
a in
Sou
th
Kore
aU
sed
onlin
e si
te to
ent
er a
nd m
onito
r blo
od
gluc
ose
leve
ls a
nd d
rug
info
rmat
ion,
with
su
ppor
t fro
m a
nur
se th
roug
h w
eekl
y SM
S m
essa
ges
Qua
si-
expe
rimen
tal,
1 gr
oup,
pr
e–po
st-t
est
N/A
[29]
Kras
s et al.
(200
5)18
8D
iagn
osed
with
T2D
M,
taki
ng >
3 m
edic
atio
ns,
aged
18–
85 y
ears
, abl
e to
co
mpl
ete
ques
tionn
aire
s
9 m
onth
sRe
gion
s of
New
So
uth
Wal
es
(Aus
tral
ia)
Patie
nts
wer
e gi
ven
inst
ruct
ions
on
BGSM
us
ing
Med
iSen
se; d
iabe
tes
hist
ory,
info
rmat
ion
on q
ualit
y of
life
, med
icat
ion
adhe
renc
e,
clin
ical
dat
a an
d m
edic
atio
n hi
stor
y w
ere
used
to
dev
elop
pat
ient
pro
toco
ls; i
nter
vent
ion
stra
tegi
es in
clud
ed B
GSM
leve
ls, e
duca
tion
abou
t the
dis
ease
and
med
icat
ions
, adh
eren
ce
devi
ces,
rem
inde
rs, a
nd re
gula
r fol
low
-up
Para
llel
grou
p,
repe
ated
m
easu
re
desi
gn
Usu
al c
are
[30]
Neg
aran
deh
et al.
(201
3)13
5A
dults
dia
gnos
ed fo
r >6
mon
ths
with
low
lit
erac
y (T
OFH
LA ≤
59)
6 w
eeks
Dia
bete
s cl
inic
in
Kurd
ista
nTw
o ed
ucat
iona
l str
ateg
ies
(teac
h ba
ck a
nd
pict
oria
l im
age)
usi
ng th
e sa
me
educ
atio
nal
cont
ent
RCT
Usu
al d
iabe
tes
educ
atio
n[31]
BGSM
: Blo
od g
luco
se m
onito
ring;
CH
W: C
omm
unit
y he
alth
wor
ker;
CM
: Cas
e m
anag
er; D
MSM
: Dia
bet
es m
ellit
us s
elf-
man
agem
ent;
N/A
: Not
app
licab
le; R
CT:
Ran
dom
ized
con
trol
led
tria
l; T1
DM
: Typ
e 1
diab
etes
mel
litus
; T2
DM
: Typ
e 2
diab
etes
mel
litus
; TO
FHLA
: Tes
t of F
unct
iona
l Hea
lth L
itera
cy in
Adu
lts.
-
Diabetes Manage. (2014) 4(1) future science group34
review Williams, Walker, Smalls, Campbell & EgedeTa
ble
1. S
tudi
es m
eeti
ng in
clus
ion
crite
ria
(con
t.).
Stud
y (y
ear)
Pati
ents
(n)
Sam
ple
popu
lati
onD
urat
ion
Sett
ing
inte
rven
tion
des
crip
tion
Stud
y de
sign
Type
of c
ontr
olRe
f.
Ode
gard
et al.
(200
5)77
Adu
lts w
ith T
2DM
ta
king
at l
east
one
ora
l T2
DM
med
icat
ion
and
HbA
1c ≥
9%
12 m
onth
sN
onpr
ofit m
edic
al
clin
ics i
n gr
eate
r Se
attle
are
a (W
A,
USA
)
Phar
mac
ist i
nter
vent
ion
with
a d
evel
oped
T2
DM
car
e pl
an a
nd p
harm
acis
t–pa
tient
/ph
arm
acis
t–pr
ovid
er c
omm
unic
atio
n on
pa
tient
pro
gres
s
RCT
Usu
al c
are
[32]
Ode
gard
et al.
(201
2)26
5Pa
tient
s with
T2D
M ta
king
or
al T
2DM
med
icat
ions
and
la
te fo
r refi
lls b
y ≥6
day
s
18 m
onth
sFo
ur c
omm
unit
y ch
ain
phar
mac
ies
in
Seat
tle (W
A, U
SA)
Tele
phon
e-in
itiat
ed a
dher
ence
sup
port
by
phar
mac
ists
follo
win
g m
isse
d re
fill a
lert
s fr
om
com
pute
r
RCT
Usu
al c
are
[33]
Ruba
k et al.
(201
1)80
Indi
vidu
als
aged
40
–69
year
s w
ith T
2DM
12 m
onth
sD
enm
ark
Effec
t of m
otiv
atio
nal i
nter
view
trai
ning
on
gene
ral p
ract
ition
ers
and
qual
ity
of c
are
mea
sure
s in
pat
ient
s w
ith T
2DM
RCT
Stan
dard
car
e [34]
Tan et al.
(201
1)16
4A
dults
with
poo
rly
cont
rolle
d T2
DM
12 w
eeks
Mal
aysi
aBr
ief s
truc
ture
d di
abet
es e
duca
tion
prog
ram
ba
sed
on s
elf-
effica
cySi
ngle
-bl
inde
d RC
TSt
anda
rd c
are
[35]
Thie
baud
et al.
(200
8)25
98A
dults
that
did
not
opt
out
of
car
e m
anag
emen
t2
year
sFl
orid
a M
edic
aid
bene
ficia
ries
(FL,
USA
)
Tele
phon
e ed
ucat
ion
of M
edic
aid
bene
ficia
ries
on c
hron
ic d
isea
ses
and
incr
easi
ng
self-
man
agem
ent a
bilit
ies
Coho
rtM
atch
ed
mod
erat
e-to
-hig
h ris
k be
nefic
iarie
s w
ith d
iabe
tes
[36]
Thoo
len
et al.
(200
8)22
7In
divi
dual
s ag
ed
50–7
0 ye
ars
and
rece
ivin
g tr
eatm
ent
12 w
eeks
The
Net
herla
nds
Gro
up m
eetin
gs to
teac
h ne
cess
ary
skill
s to
an
ticip
ate
and
deal
with
pot
entia
l bar
riers
to
goal
mai
nten
ance
thro
ugh
proa
ctiv
e co
ping
RCT
Broc
hure
on
diab
etes
sel
f-m
anag
emen
t
[37]
Verv
loet
et al.
(201
1)10
4A
dults
usi
ng m
edic
atio
n fo
r at l
east
1 y
ear w
ith lo
w
adhe
renc
e
6 m
onth
sD
utch
pha
rmac
ies
(The
Net
herla
nds)
Two
inte
rven
tion
grou
ps w
ith e
lect
roni
c di
spen
sers
; one
gro
up re
ceiv
ed a
SM
S re
min
der
if th
ey h
ad n
ot o
pene
d th
eir d
ispe
nser
RCT
No
use
of S
MS
with
ele
ctro
nic
mon
itorin
g
[38]
Wak
efiel
d et al.
(201
2)30
2A
dults
with
T2D
M a
nd
hype
rten
sion
trea
ted
by
a Ve
tera
ns A
ffairs
prim
ary
care
pro
vide
r
12 m
onth
sIo
wa
City
Vet
eran
s A
ffairs
Med
ical
Ce
nter
(IA
, USA
)
Patie
nts
in th
e in
terv
entio
n gr
oup
ente
red
bloo
d pr
essu
re a
nd b
lood
glu
cose
mea
sure
s in
to a
hom
e te
lehe
alth
dev
ice
and
rece
ived
ed
ucat
iona
l fee
dbac
k
RCT
Usu
al c
are
[39]
Wol
ever
et al.
(201
0)56
Div
erse
sam
ple
of a
dults
w
ith T
2DM
6 m
onth
sCo
mm
unit
y se
rvic
ed
by D
uke
Uni
vers
ity
Scho
ol o
f Med
icin
e (N
C, U
SA)
14 3
0-m
in in
tegr
ativ
e co
achi
ng s
essi
ons
by
tele
phon
e Pr
e–po
st-t
est
Usu
al c
are
[40]
Zolfa
ghar
i et al.
(201
2)77
Recr
uite
d fr
om th
e Ira
nian
D
iabe
tes
Ass
ocia
tion,
ag
ed 1
8–65
yea
rs, m
ust
have
tele
phon
e ac
cess
in
thei
r hom
es a
nd h
ave
a m
obile
pho
ne, m
ust b
e on
ly u
sing
ora
l med
icat
ion
6 m
onth
sTe
hran
Uni
vers
ity
of M
edic
al S
cien
ce
(Iran
)
The
SMS
grou
p re
ceiv
ed 6
mes
sage
s/w
eek
rega
rdin
g ex
erci
se, t
akin
g T2
DM
med
icat
ion,
di
et, B
GSM
and
str
ess m
anag
emen
t. Th
e te
leph
one
grou
p in
volv
ed sc
hedu
ling
appo
intm
ents
, cou
nsel
ing
abou
t the
nat
ure
of th
e di
seas
e, ri
sk fa
ctor
s, im
port
ance
of
mai
ntai
ning
nor
mal
blo
od g
luco
se le
vels
, die
t, ex
erci
se, m
edic
atio
n ta
king
, illn
ess m
anag
emen
t an
d ho
w to
reco
rd b
lood
glu
cose
leve
ls
Qua
si-
expe
rimen
tal,
2 gr
oups
, pr
e–po
st-t
est
Para
llel
inte
rven
tion,
no
con
trol
gr
oup
[41]
BGSM
: Blo
od g
luco
se m
onito
ring;
CH
W: C
omm
unit
y he
alth
wor
ker;
CM
: Cas
e m
anag
er; D
MSM
: Dia
bet
es m
ellit
us s
elf-
man
agem
ent;
N/A
: Not
app
licab
le; R
CT:
Ran
dom
ized
con
trol
led
tria
l; T1
DM
: Typ
e 1
diab
etes
mel
litus
; T2
DM
: Typ
e 2
diab
etes
mel
litus
; TO
FHLA
: Tes
t of F
unct
iona
l Hea
lth L
itera
cy in
Adu
lts.
-
Interventions to improve medication adherence in Type 2
diabetes review
future science group www.futuremedicine.com 35
evidence available in the literature. The risk of bias across
studies is discussed in this article and the discussion gives more
weight to studies using a RCT design.
Results Study selection
Figure 1 shows the results of the search. After duplicates
were removed, the search resulted in 922 citations for review.
Title review produced 171 abstracts to examine, after which 56
articles were determined eligible for full article review.
Twenty-seven eligible studies were identified based on the
predetermined eligibility criteria [15–41]. Seventeen studies
showed a statistically significant change in medication adherence
for interventions with or without comparison groups, and ten
studies reported significant statistical changes in glycemic
control. Seven of the studies described interventions that
sig-nificantly improved both medication adherence and HbA1c.
Study characteristics & results of individual
studiesTable 1 provides a summary of the 27 studies that were
eligible for inclusion; these studies are heterogeneous in terms of
sample size, sample population, length of duration, setting,
inter-vention description, study design and use of a control group.
Sample sizes ranged from 23 to 29,247, and intervention duration
stretched from 2 weeks to 2 years. Eighteen of the stud-ies were
RCTs [15,18–19,22–28,31–35,37–39], four were pre–post-test
[16–17,21,40], two combined quasiexperimental with pre- and
post-tests [29,41], two were cohorts [20,36], and one used a
parallel group with repeated measure design [30]. Twenty-three of
the studies used a control group for comparisons
[15,17–20,22–28,30–40]. All of the studies focused on adults with
T2DM [15–41], but one study also included individuals diagnosed
with Type 1 diabetes [24]. Thirteen of the 27 articles were
conducted in international locations
[15,22–24,28–31,34–35,37–38,41].
Table 2 presents the medication adherence outcomes of
studies meeting the inclusion crite-ria [15–41]. The mean baseline
medication adher-ence was wide ranging and fluctuated through-out
the studies, particularly given the variety of adherence methods –
direct and indirect – used. Direct measures of adherence indicate
that med-ications have actually been taken by the patients and
indirect measures, those most commonly
used, infer an assumption that medications have been taken by
patients [11]. No direct methods for measuring medication adherence
were used. All forms of indirect methods were used, with 18 studies
measuring medication adherence by self-report
[15–17,21,23–32,35,37,39–41], two by pill count [22,33], three by
electronic devices [18–19,38], and three by pharmacy claims data
[20,34,36]. Of the 27 studies, 13 reported statistically
sig-nificant differences in medication adherence in the
intervention group compared with the control group
[15,17–20,22,24,28,30–31,33,36,40]. All four studies without a
control group reported statistically significant changes in
medication adherence [16,21,29,41].
Table 3 shows glycemic control outcomes of the studies
that met the eligibility criteria [15–23,25–30,32,34–35,39–42] for
which the impact on glycemic control was noted. The mean base-line
HbA1c ranged from 6.8 to 10.6. One of the studies included in this
review [39] reported outcomes for medication adherence and
gly-cemic control in two separate papers; thus, a second article
using the same population and intervention, reporting the
differences in HbA1c between groups, is reported in Table 3
[42]. Eight out of 18 studies demonstrated sta-tistically
significant improvements in HbA1c between the intervention groups
and the control groups [15,17–19,22,28,34–35]. In these studies,
the percentage change in HbA1c in the interven-tion group ranged
from -1.57 to -0.15 compared with -2.1 to +0.2 in the control
group; this also varied at different time points within the
stud-ies. Of the four studies without a control group, two
described statistically significant changes in HbA1c [21,29]. For
one study, there was a -0.6% drop in the HbA1c, while the
percentage change was -1.1% in the other.
Table 4 illustrates intervention characteris-tics of the
27 studies included in this review. Most studies did not employ a
theoretical foundation [15–16,20–22,24–25,27–34,36,38–41], but for
those that did, one study used the Theory of Planned Behavior [23],
one used the Trans-theoretical Model [17], two used a self-efficacy
theory [35,37], two used integrated care [18–19], and one used the
Social–Cognitive Theory [26]. As for the intervention
characteristics, five out of the 27 studies were culturally
tai-lored [16,18,31,38–39], of which four were signifi-cant for
changes in medication adherence and HbA1c. Self-management was the
focus of several interventions, with 18 concentrating on
-
Diabetes Manage. (2014) 4(1) future science group36
review Williams, Walker, Smalls, Campbell & EgedeTa
ble
2. M
edic
atio
n ad
here
nce
outc
omes
of s
tudi
es m
eeti
ng in
clus
ion
crite
ria.
Stud
y (y
ear)
Mea
sure
of
med
icat
ion
adhe
renc
e
Mea
n ±
SD b
asel
ine
med
icat
ion
adhe
renc
ein
terv
enti
on m
ean
± SD
ch
ange
in m
edic
atio
n ad
here
nce
Cont
rol m
ean
± SD
ch
ange
in m
edic
atio
n ad
here
nce
Stat
isti
cal s
igni
fican
ceRe
f.
Al M
azro
ui
et al.
(200
9)Se
lf-re
port
: fo
rget
ting,
mis
sing
or
incr
easi
ng d
oses
Inte
rven
tion:
48.
3% n
onad
here
ntCo
ntro
l: 49
.1%
non
adhe
rent
21.4
% o
f int
erve
ntio
n gr
oup
wer
e no
nadh
eren
t at
12-m
onth
follo
w-u
p
32.5
% o
f con
trol
gro
up
wer
e no
nadh
eren
t at
12-m
onth
follo
w-u
p
Gly
cem
ic c
ontr
ol a
nd h
ealth
-rel
ated
qu
alit
y of
life
wer
e si
gnifi
cant
ly
impr
oved
aft
er re
ceiv
ing
patie
nt
educ
atio
n an
d m
edic
atio
n ad
here
nce
advi
ce (p
= 0
.003
)
[15]
Aro
ra et a
l. (2
012)
Self-
repo
rt: M
MA
SSc
ore
of 3
.5 o
n M
MA
SSc
ore
of 4
.75
on M
MA
S at
3-
wee
k fo
llow
-up
No
cont
rol g
roup
The
pilo
t int
erve
ntio
n de
mon
stra
ted
incr
ease
d he
alth
y be
havi
ors
with
im
prov
ed d
iabe
tes
self-
effica
cy a
nd
med
icat
ion
adhe
renc
e
[16]
Baba
mot
o et al.
(200
9)Se
lf-re
port
(p
erce
ntag
e w
ho
neve
r for
get t
o ta
ke
med
icat
ion)
Inte
rven
tion:
CH
W: 6
9% n
ever
forg
ot to
take
m
edic
atio
nCM
: 77%
nev
er fo
rgot
to ta
ke
med
icat
ion
Cont
rol:
67%
nev
er fo
rgot
to ta
ke m
edic
atio
n
79%
nev
er fo
rgot
to ta
ke
med
icat
ion
in th
e CH
W
inte
rven
tion,
55%
nev
er
forg
ot to
take
med
icat
ion
in th
e CM
inte
rven
tion
50%
nev
er fo
rgot
to ta
ke
med
icat
ion
in th
e co
ntro
l gr
oup
Med
icat
ion-
taki
ng b
ehav
ior
rem
aine
d un
chan
ged
(p >
0.0
5) in
th
e CH
W g
roup
, but
wor
sene
d in
the
CM a
nd c
ontr
ol g
roup
s (p
< 0
.05)
[17]
Bogn
er et a
l. (2
010)
Elec
tron
ic
mon
itorin
g (M
EMS
>80%
adh
eren
t)
34.5
% in
terv
entio
n20
.7%
con
trol
62.1
%24
.1%
Prop
ortio
n of
par
ticip
ants
who
had
80
% a
dher
ence
to h
ypog
lyce
mic
ag
ent w
as g
reat
er in
the
inte
rven
tion
than
the
cont
rol g
roup
(p =
0.0
04)
[18]
Bogn
er et a
l. (2
012)
Elec
tron
ic
mon
itorin
g (M
EMS
>80%
adh
eren
t)
42.0
% in
terv
entio
n35
.9%
con
trol
At 6
wee
ks, t
he
inte
rven
tion
grou
p w
as
61%
adh
eren
t, an
d 65
%
adhe
rent
at 1
2 w
eeks
At 6
wee
ks, t
he c
ontr
ol
grou
p w
as 3
5% a
dher
ent,
and
30%
adh
eren
t at
12 w
eeks
At 6
and
12
wee
ks, t
hose
in th
e in
terv
entio
n gr
oup
had
sign
ifica
nt
impr
ovem
ent i
n ad
here
nce
com
pare
d w
ith u
sual
car
e (p
≤ 0
.001
)
[19]
Bren
nan
et al.
(201
2)To
tal n
umbe
r of
days
of m
edic
atio
n su
pplie
d pe
r mon
th
CVS
Ret
ail:
Inte
rven
tion:
No
rece
nt u
se o
f ACE
inhi
bito
rs:
31.2
%N
o re
cent
use
of s
tatin
s: 3
2.6%
Cont
rol:
No
rece
nt u
se o
f ACE
inhi
bito
rs:
31.6
%N
o re
cent
use
of s
tatin
s: 3
2.4%
Mai
l ord
er:
Inte
rven
tion:
No
rece
nt u
se o
f ACE
inhi
bito
rs:
32.1
%N
o re
cent
use
of s
tatin
s: 3
2.8%
Cont
rol:
No
rece
nt u
se o
f ACE
inhi
bito
rs:
31.3
%N
o re
cent
use
of s
tatin
s: 3
1.9%
3.9%
incr
ease
in s
uppl
y pe
r mon
th in
reta
il in
terv
entio
n gr
oup
com
pare
d w
ith c
ontr
ol
grou
p; 1
.7%
incr
ease
in
supp
ly p
er m
onth
in m
ail
orde
r int
erve
ntio
n gr
oup
com
pare
d w
ith c
ontr
ol
grou
p
N/A
Ther
e w
as a
sta
tistic
ally
sig
nific
ant
diffe
renc
e be
twee
n th
e tw
o in
terv
entio
ns (p
< 0
.01)
[20]
BMQ
: Brie
f med
icat
ion
ques
tionn
aire
; CH
W: C
omm
unit
y he
alth
wor
ker;
CM
: Cas
e m
anag
er; M
ARS
: Med
icat
ion
adhe
renc
e re
por
t sca
le; M
EMS:
Med
icat
ion
Even
t Mon
itorin
g Sy
stem
; MM
AS:
Mor
isky
Med
icat
ion
Adh
eren
ce S
cale
; M
PR: M
edic
atio
n p
osse
ssio
n ra
te; N
/A: N
ot a
pplic
able
; RTM
M: R
eal-t
ime
med
icat
ion
mon
itorin
g; S
D: S
tand
ard
devi
atio
n; S
DSC
A: S
umm
ary
of d
iab
etes
sel
f-ca
re a
ctiv
ities
; T2D
M: T
ype
2 di
abet
es m
ellit
us.
-
Interventions to improve medication adherence in Type 2
diabetes review
future science group www.futuremedicine.com 37
Tabl
e 2.
Med
icat
ion
adhe
renc
e ou
tcom
es o
f stu
dies
mee
ting
incl
usio
n cr
iteri
a (c
ont.)
.
Stud
y (y
ear)
Mea
sure
of
med
icat
ion
adhe
renc
e
Mea
n ±
SD b
asel
ine
med
icat
ion
adhe
renc
ein
terv
enti
on m
ean
± SD
ch
ange
in m
edic
atio
n ad
here
nce
Cont
rol m
ean
± SD
ch
ange
in m
edic
atio
n ad
here
nce
Stat
isti
cal s
igni
fican
ceRe
f.
Cast
illo et al.
(201
0)Se
lf-re
port
: SD
SCA
5.5
± 2.
5 (p
rete
st)
6.6
± 1.
3 (p
ost-
test
)N
/ASi
gnifi
cant
pre
–pos
t im
prov
emen
t in
adh
eren
ce (p
= 0
.009
)[21]
Chan
et a
l. (2
012)
Pill
coun
t (p
erce
ntag
e th
at
are
at le
ast 8
0%
com
plia
nt b
ased
on
num
ber t
aken
as
a p
erce
ntag
e of
co
rrec
t am
ount
)
73.6
% in
terv
entio
n82
.1%
con
trol
The
prop
ortio
n of
in
divi
dual
s w
ho w
ere
at le
ast 8
0% a
dher
ent
incr
ease
d by
22.
5 ±
13.4
%
The
prop
ortio
n of
in
divi
dual
s w
ho w
ere
at le
ast 8
0% a
dher
ent
incr
ease
d 2
± 5.
0%
Inte
rven
tion
grou
p ha
d gr
eate
r im
prov
emen
t in
com
plia
nce
com
pare
d w
ith c
ontr
ol (p
< 0
.001
)
[22]
Farm
er et a
l. (2
012)
Self-
repo
rt: M
ARS
(s
cale
: 5–2
5)In
terv
entio
n: 2
3.6
± 2.
3 sc
ore
on M
ARS
Cont
rol:
23.6
± 2
.8 s
core
on
MA
RS23
.6 ±
2.6
sco
re o
n M
ARS
; -0
.4 (9
5% C
I: -1
.0 to
0.2
)24
.1 ±
1.6
sco
re o
n M
ARS
Ther
e w
as n
o st
atis
tical
ly s
igni
fican
t di
ffere
nce
betw
een
the
cont
rol a
nd
inte
rven
tion
grou
ps (p
= 0
.2)
[23]
Gia
lam
as
et al.
(200
9)Se
lf-re
port
via
the
MA
RS-5
Med
ian
scor
e of
24
(max
imum
sco
re: 2
5)N
/AN
/AIn
terv
entio
n gr
oup
had
high
er
adhe
renc
e th
an c
ontr
ols
with
a
noni
nfer
iorit
y m
argi
n of
-4.1
% (3
9.3
vs 3
7.0%
; p <
0.0
01)
[24]
Gla
sgow
et al.
(201
0)Se
lf-re
port
: Hill
–Bo
ne C
ompl
ianc
e Sc
ale
(sca
le: 0
–1)
Inte
rven
tion
scor
e: 3
.80
± 0.
29Co
ntro
l sco
re: 3
.77
± 0.
303.
84 ±
0.2
93.
79 ±
0.3
9N
o si
gnifi
cant
impr
ovem
ents
in
adhe
renc
e (p
= 0
.262
)[25]
Gla
sgow
et al.
(201
2)Se
lf-re
port
: Hill
–Bo
ne C
ompl
ianc
e Sc
ale
(sca
le: 0
–1)
Inte
rven
tion
scor
e: 0
.35
± 0.
03Co
ntro
l sco
re: 0
.34
± 0.
04
Post
inte
rven
tion
scor
es:
4 m
onth
s: 0
.42
± 0.
03
12 m
onth
s: 0
.43
± 0.
03
Post
stud
y sc
ores
:4
mon
ths:
0.3
8 ±
0.04
12
mon
ths:
0.4
1 ±
0.04
No
stat
istic
al s
igni
fican
ce b
etw
een
inte
rven
tions
and
con
trol
gro
ups
[26]
Gra
nt et a
l. (2
003)
Self-
repo
rt: n
umbe
r of
day
s w
ithou
t m
issi
ng m
edic
atio
n
Inte
rven
tion:
6.7
± 0
.9 d
ays
with
out
mis
sing
med
icat
ion
in th
e pa
st 7
day
s Co
ntro
l: 6.
9 ±
0.4
days
with
out m
issi
ng
med
icat
ion
in th
e pa
st 7
day
s
0.1
± 1
days
with
out
mis
sing
med
icat
ion
in th
e pa
st 7
day
s at
3-m
onth
fo
llow
-up
0.1
± 0.
4 da
ys w
ithou
t m
issi
ng m
edic
atio
n in
the
past
7 d
ays
at 3
-mon
th
follo
w-u
p
Ther
e w
as n
ot a
sta
tistic
ally
si
gnifi
cant
diff
eren
ce w
hen
com
parin
g th
e in
terv
entio
n an
d co
ntro
l gro
ups
(p =
0.8
)
[27]
Jara
b et al.
(201
2)Se
lf-re
port
: MM
AS
Inte
rven
tion:
74.
1% n
onad
here
ntCo
ntro
l: 70
.9%
non
adhe
rent
28.6
% o
f the
inte
rven
tion
grou
p w
ere
nona
dher
ent
post
inte
rven
tion
at
6-m
onth
follo
w-u
p
64.6
% o
f the
con
trol
gr
oup
wer
e no
nadh
eren
t po
stin
terv
entio
n at
6-
mon
th fo
llow
-up
At t
he 6
-mon
th fo
llow
-up
inte
rven
tion
patie
nts
wer
e m
ore
adhe
rent
to m
edic
atio
ns th
an th
e co
ntro
l gro
up (p
= 0
.003
)
[28]
Kim
et a
l. (2
006)
Self-
repo
rt: n
umbe
r of
day
s in
wee
k w
hen
med
icat
ion
was
take
n
4.8
± 2.
6 da
ys+1
.1 d
ays
N/A
Ther
e w
as a
sta
tistic
ally
sig
nific
ant
chan
ge in
the
num
ber o
f day
s of
m
edic
atio
n ad
here
nce
in a
wee
k in
th
e in
terv
entio
n gr
oup
(p =
0.0
32)
[29]
BMQ
: Brie
f med
icat
ion
ques
tionn
aire
; CH
W: C
omm
unit
y he
alth
wor
ker;
CM
: Cas
e m
anag
er; M
ARS
: Med
icat
ion
adhe
renc
e re
por
t sca
le; M
EMS:
Med
icat
ion
Even
t Mon
itorin
g Sy
stem
; MM
AS:
Mor
isky
Med
icat
ion
Adh
eren
ce S
cale
; M
PR: M
edic
atio
n p
osse
ssio
n ra
te; N
/A: N
ot a
pplic
able
; RTM
M: R
eal-t
ime
med
icat
ion
mon
itorin
g; S
D: S
tand
ard
devi
atio
n; S
DSC
A: S
umm
ary
of d
iab
etes
sel
f-ca
re a
ctiv
ities
; T2D
M: T
ype
2 di
abet
es m
ellit
us.
-
Diabetes Manage. (2014) 4(1) future science group38
review Williams, Walker, Smalls, Campbell & EgedeTa
ble
2. M
edic
atio
n ad
here
nce
outc
omes
of s
tudi
es m
eeti
ng in
clus
ion
crite
ria
(con
t.).
Stud
y (y
ear)
Mea
sure
of
med
icat
ion
adhe
renc
e
Mea
n ±
SD b
asel
ine
med
icat
ion
adhe
renc
ein
terv
enti
on m
ean
± SD
ch
ange
in m
edic
atio
n ad
here
nce
Cont
rol m
ean
± SD
ch
ange
in m
edic
atio
n ad
here
nce
Stat
isti
cal s
igni
fican
ceRe
f.
Kras
s et al.
(200
5)Se
lf-re
port
: BM
Q
(sca
le: 0
–7)
Inte
rven
tion:
1.3
8 ±
1.20
BM
Q s
core
Cont
rol:
1.01
± 0
.88
BMQ
sco
reBM
Q s
core
of 0
.94
± 0.
89BM
Q s
core
of 1
.16
± 0.
88
The
BMQ
sco
res
wer
e st
atis
tical
ly
sign
ifica
nt w
hen
com
parin
g th
e in
terv
entio
n an
d co
ntro
l gro
ups
(p =
0.0
09)
[30]
Neg
aran
deh
et al.
(201
3)Se
lf-re
port
: MM
AS
(sca
le: 1
–7)
Inte
rven
tion:
Pict
ure
inte
rven
tion:
4.3
3 ±
1.62
Teac
h ba
ck in
terv
entio
n: 4
.37
± 1.
46Co
ntro
l: 4.
52 ±
1.7
4
Pict
ure
inte
rven
tion:
6.
73 ±
1.5
2 Te
ach
back
inte
rven
tion:
7.
03 ±
0.9
9
Cont
rol:
4.32
± 1
.58
Sign
ifica
nt d
iffer
ence
bet
wee
n tw
o in
terv
entio
n gr
oups
and
the
cont
rol
grou
p (p
< 0
.001
), bu
t no
diffe
renc
e be
twee
n in
terv
entio
n gr
oups
(p
= 0
.56)
[31]
Ode
gard
et al.
(200
5)Se
lf-re
port
: tw
o-qu
estio
n re
call
valid
ated
in a
ch
roni
c di
seas
e m
odel
Inte
rven
tion:
56%
had
diffi
cult
y re
mem
berin
g to
take
med
icat
ions
as
pres
crib
edCo
ntro
l: 35
% h
ad d
ifficu
lty
rem
embe
ring
to ta
ke m
edic
atio
ns a
s pr
escr
ibed
(p =
0.0
7)
Not
repo
rted
N
/ATh
e in
terv
entio
n ha
d no
effe
ct
on a
dher
ence
(p =
0.4
9) a
nd th
e co
ntro
l gro
up h
ad b
ette
r adh
eren
ce
thro
ugho
ut th
e st
udy
(p =
0.0
3)
[32]
Ode
gard
et al.
(201
2)Re
fill r
ate
base
d on
MPR
at 6
and
12
mon
ths
Inte
rven
tion:
74%
had
MPR
abo
ve 8
0%
for p
revi
ous
12 m
onth
sCo
ntro
l: 65
% h
ad M
PR a
bove
80%
for
prev
ious
12
mon
ths
MPR
sco
res
at 6
and
12
mon
ths
impr
oved
si
gnifi
cant
ly w
ithin
the
grou
p (p
= 0
.16
and
p<0.
01,
resp
ectiv
ely)
MPR
rem
aine
d un
chan
ged
at 6
and
12
mon
ths
Inte
rven
tion
grou
p si
gnifi
cant
ly
mor
e lik
ely
to h
ave
an M
PR >
80%
at
12
mon
ths
(odd
s ra
tio: 4
.77;
95
% C
I: 2.
00–1
1.4)
[33]
Ruba
k et al.
(201
1)N
umbe
r of
pres
crip
tions
‘c
ashe
d in
’ by
pat
ient
s at
pha
rmac
y co
mpa
red
with
nu
mbe
r of
pres
crip
tions
pr
escr
ibed
N/A
Ora
l ant
idia
betic
m
edic
atio
n: 3
7% c
ashe
d in
com
pare
d w
ith 3
9%
pres
crib
ed
Ora
l ant
idia
betic
m
edic
atio
n: 3
6% c
ashe
d in
com
pare
d w
ith 3
6%
pres
crib
ed
Ther
e w
ere
no s
tatis
tical
ly
sign
ifica
nt d
iffer
ence
s in
the
num
ber
of p
resc
riptio
ns c
ashe
d in
com
pare
d w
ith th
e nu
mbe
r of p
resc
riptio
ns
pres
crib
ed. N
o eff
ect o
f mot
ivat
iona
l in
terv
iew
ing
on m
edic
atio
n ad
here
nce
was
foun
d
[34]
Tan et al.
(201
1)Se
lf-re
port
(p
erce
ntag
e th
at
are
90%
adh
eren
t ba
sed
on n
umbe
r of
tim
es in
a w
eek
med
icat
ions
are
m
isse
d)
Inte
rven
tion:
84.
48%
Co
ntro
l: 85
%89
.21%
repo
rted
90%
ad
here
nce
base
d on
nu
mbe
r of t
imes
in a
wee
k m
edic
atio
ns a
re m
isse
d(9
1.42
% w
ere
adhe
rent
w
hen
adju
sted
for
chan
ged
adhe
renc
e du
e to
hy
perg
lyce
mia
)
84.4
8% w
ere
90%
ad
here
nt b
ased
on
num
ber o
f tim
es in
a w
eek
med
icat
ions
are
mis
sed
No
diffe
renc
e in
adh
eren
ce b
etw
een
grou
ps u
nles
s ad
just
men
ts in
in
sulin
wer
e co
nsid
ered
adh
eren
t, in
whi
ch c
ase
ther
e w
as a
sig
nific
ant
diffe
renc
e (p
= 0
.008
)
[35]
BMQ
: Brie
f med
icat
ion
ques
tionn
aire
; CH
W: C
omm
unit
y he
alth
wor
ker;
CM
: Cas
e m
anag
er; M
ARS
: Med
icat
ion
adhe
renc
e re
por
t sca
le; M
EMS:
Med
icat
ion
Even
t Mon
itorin
g Sy
stem
; MM
AS:
Mor
isky
Med
icat
ion
Adh
eren
ce S
cale
; M
PR: M
edic
atio
n p
osse
ssio
n ra
te; N
/A: N
ot a
pplic
able
; RTM
M: R
eal-t
ime
med
icat
ion
mon
itorin
g; S
D: S
tand
ard
devi
atio
n; S
DSC
A: S
umm
ary
of d
iab
etes
sel
f-ca
re a
ctiv
ities
; T2D
M: T
ype
2 di
abet
es m
ellit
us.
-
Interventions to improve medication adherence in Type 2
diabetes review
future science group www.futuremedicine.com 39
Tabl
e 2.
Med
icat
ion
adhe
renc
e ou
tcom
es o
f stu
dies
mee
ting
incl
usio
n cr
iteri
a (c
ont.)
.
Stud
y (y
ear)
Mea
sure
of
med
icat
ion
adhe
renc
e
Mea
n ±
SD b
asel
ine
med
icat
ion
adhe
renc
ein
terv
enti
on m
ean
± SD
ch
ange
in m
edic
atio
n ad
here
nce
Cont
rol m
ean
± SD
ch
ange
in m
edic
atio
n ad
here
nce
Stat
isti
cal s
igni
fican
ceRe
f.
Thie
baud
et al.
(200
8)Ph
arm
acy
clai
ms
data
(pro
port
ion
user
s w
ith M
PR
≥80%
)
Inte
rven
tion:
30.
3% h
ad a
n M
PR ≥
80%
Cont
rol:
33%
had
an
MPR
≥80
%Ca
re m
anag
ed v
s no
t car
e m
anag
ed
+8.
7% n
onus
ers
at b
asel
ine
+6.
9% u
sers
at b
asel
ine
N/A
Care
-man
aged
pat
ient
s w
ere
mor
e lik
ely
to h
ave
a hi
gher
MPR
(p
< 0
.001
)
[36]
Thoo
len
et al.
(200
8)Se
lf-re
port
: MA
RS
(sca
le: 1
–5)
Inte
rven
tion:
4.8
MA
RS s
core
Cont
rol:
4.9
MA
RS s
core
MA
RS s
core
of 4
.9 a
t 3 a
nd
12 m
onth
sM
ARS
sco
re o
f 5.0
at 3
and
12
mon
ths
Ther
e w
as n
o st
atis
tical
ly s
igni
fican
t di
ffere
nce
betw
een
the
inte
rven
tion
and
cont
rol g
roup
s
[37]
Verv
loet
et al.
(201
1)El
ectr
onic
m
onito
ring
(RTM
M
mea
surin
g th
e nu
mbe
r of d
ays
with
out d
osin
g,
prop
ortio
n of
m
isse
d do
ses
and
prop
ortio
n of
dos
es
in s
tand
ardi
zed
time)
Not
repo
rted
Day
s w
ithou
t dos
ing:
11
.9 ±
18.
8M
isse
d do
ses:
14.
5 ±
15.7
Dos
es ta
ken
in a
gree
d tim
e:
56.7
± 2
3.8
Day
s w
ithou
t dos
ing:
13
.8 ±
14.
5M
isse
d do
ses:
19.
2 ±
16.0
Dos
es ta
ken
in a
gree
d tim
e: 3
8.7
± 23
.0
Patie
nts
who
rece
ived
rem
inde
rs
took
dos
es w
ithin
agr
eed
upon
w
indo
w (p
= 0
.003
), bu
t sho
wed
no
diff
eren
ce in
day
s w
ithou
t do
sing
(p =
0.2
83) o
r mis
sed
dose
s (p
= 0
.065
)
[38]
Wak
efiel
d et al.
(201
2)Se
lf-re
port
: T2
DM
Reg
imen
A
dher
ence
Sca
le
Low
- and
hig
h-in
tens
ity
inte
rven
tion:
99
.7%
adh
eren
ceCo
ntro
l: 99
.5%
adh
eren
ce
Low
-inte
nsit
y in
terv
entio
n:
99.8
% a
dher
ence
at
6-m
onth
follo
w-u
p an
d 99
.7%
at 1
2 m
onth
sH
igh-
inte
nsity
inte
rven
tion:
99
.6%
at 6
-mon
th
follo
w-u
p an
d 10
0% a
t 12
-mon
th p
ostin
terv
entio
n
99.6
% a
t 6-m
onth
fo
llow
-up;
98.
9%
at 1
2-m
onth
po
stin
terv
entio
n
Repo
rted
med
icat
ion
adhe
renc
e w
as h
igh
acro
ss g
roup
s at
all
thre
e tim
e po
ints
. No
sign
ifica
nt
chan
ges
wer
e fo
und.
At 1
2 m
onth
s po
stin
terv
entio
n p
= 0.
20
[39]
Wol
ever
et al.
(201
0)Se
lf-re
port
: MM
AS
Inte
rven
tion:
6.7
± 0
.96
MM
AS
scor
eCo
ntro
l: 6.
7 ±
1.25
MM
AS
scor
ePo
stin
terv
entio
n: 7
.2 ±
0.9
7 M
MA
S sc
ore
Post
stud
y: 6
.9 ±
1.2
5 M
MA
S sc
ore
Ther
e w
as a
sta
tistic
ally
sig
nific
ant
impr
ovem
ent i
n th
e in
terv
entio
n gr
oup
com
pare
d w
ith c
ontr
ol g
oup
(p =
0.0
04)
[40]
Zolfa
ghar
i et al.
(201
2)Se
lf-ca
re: T
2DM
qu
estio
nnai
reSM
S: 7
5.48
± 1
4.33
Tele
phon
e: 7
3.27
± 1
4.75
SMS:
15.
65 ±
2.7
2 ch
ange
in
adhe
renc
e sc
ore
Tele
phon
e: 2
1.46
± 7
.12
chan
ge in
adh
eren
ce s
core
N/A
Ther
e w
as a
sta
tistic
ally
sig
nific
ant
diffe
renc
e be
twee
n th
e in
terv
entio
n an
d co
ntro
l gro
ups
(p =
0.0
00)
[41]
BMQ
: Brie
f med
icat
ion
ques
tionn
aire
; CH
W: C
omm
unit
y he
alth
wor
ker;
CM
: Cas
e m
anag
er; M
ARS
: Med
icat
ion
adhe
renc
e re
por
t sca
le; M
EMS:
Med
icat
ion
Even
t Mon
itorin
g Sy
stem
; MM
AS:
Mor
isky
Med
icat
ion
Adh
eren
ce S
cale
; M
PR: M
edic
atio
n p
osse
ssio
n ra
te; N
/A: N
ot a
pplic
able
; RTM
M: R
eal-t
ime
med
icat
ion
mon
itorin
g; S
D: S
tand
ard
devi
atio
n; S
DSC
A: S
umm
ary
of d
iab
etes
sel
f-ca
re a
ctiv
ities
; T2D
M: T
ype
2 di
abet
es m
ellit
us.
-
Diabetes Manage. (2014) 4(1) future science group40
review Williams, Walker, Smalls, Campbell & EgedeTa
ble
3. G
lyce
mic
con
trol
out
com
es o
f stu
dies
mee
ting
incl
usio
n cr
iteri
a.
Stud
y (y
ear)
Mea
n ±
SD b
asel
ine
HbA
1c (%
)in
terv
entio
n m
ean
± SD
ch
ange
in o
r mea
n ±
SD
post
inte
rven
tion
HbA
1c (%
)
Cont
rol m
ean
± SD
ch
ange
in m
edic
atio
n ad
here
nce
Stat
isti
cal s
igni
fican
ceRe
f.
Al M
azro
ui et a
l. (2
009)
Inte
rven
tion:
8.5
Cont
rol:
8.4
7.6
at 4
-mon
th fo
llow
-up
7.1 a
t 8-m
onth
follo
w-u
p6.
9 at
12-
mon
th fo
llow
-up
8.0
at 4
-mon
th fo
llow
-up
8.4
at 8
-mon
th fo
llow
-up
8.3
at 1
2-m
onth
follo
w-u
p
The
care
pro
gram
resu
lted
in b
ette
r gly
cem
ic c
ontr
ol fo
r in
terv
entio
n pa
tient
s co
mpa
red
with
con
trol
(p <
0.0
01)
[15]
Baba
mot
o et al.
(200
9)CH
W: 8
.6CM
: 8.5
Stan
dard
car
e co
ntro
l: 9.
5N
onco
ntac
t con
trol
: 7.5
CHW
: 7.2
CM: 7
.4St
anda
rd c
are
cont
rol:
7.4
Non
cont
act c
ontr
ol: 7
.7M
ean
HbA
1c d
ecre
ased
in C
HW
, CM
and
sta
ndar
d ca
re
cont
rol (
p
0.0
5)
[17]
Bogn
er et a
l. (2
010)
Inte
rven
tion:
7.3
Cont
rol:
7.3
6.7
± 2.
37.
9 ±
2.6
Part
icip
ants
who
rece
ived
inte
rven
tion
had
low
er H
bA1c
(p
= 0
.019
)[18]
Bogn
er et a
l. (2
012)
Inte
rven
tion:
7.2
Cont
rol:
7.0
-0.7
0 ±
1.32
0.50
± 1
.11Si
gnifi
cant
ly im
prov
ed m
ean
chan
ge in
HbA
1c c
ompa
red
with
usu
al c
are
(p <
0.0
01)
[19]
Cast
illo et al.
(201
0)8.
39 ±
1.9
67.
79 ±
1.6
7N
/ASi
gnifi
cant
pre
–pos
t-te
st re
duct
ion
in H
bA1c
(p <
0.0
01)
[21]
Chan
et a
l. (2
012)
Inte
rven
tion:
9.7
Cont
rol:
9.5
-1.5
7-0
.4H
bA1c
redu
ced
in in
terv
entio
n gr
oup
com
pare
d w
ith
cont
rol g
roup
(p <
0.0
01)
[22]
Farm
er et a
l. (2
012)
Inte
rven
tion:
8.3
7 ±
1.25
Cont
rol:
8.28
± 1
.22
8.34
± 1
.24
Cont
rol:
8.21
± 1
.32
Ther
e w
as n
o st
atis
tical
ly s
igni
fican
t diff
eren
ce b
etw
een
the
inte
rven
tion
and
cont
rol g
roup
(p =
0.6
4)[23]
Gla
sgow
et a
l. (2
010)
Inte
rven
tion:
8.1
3 ±
1.80
Cont
rol:
8.06
± 1
.76
7.95
± 1
.58
8.00
± 1
.58
No
sign
ifica
nt im
prov
emen
ts in
HbA
1c (p
= 0
.145
)[25]
Gla
sgow
et a
l. (2
012)
Inte
rven
tion:
8.1
4 ±
0.10
Cont
rol:
8.16
± 0
.16
8.00
± 0
.09
at 4
mon
ths
8.16
± 0
.09
at 1
2 m
onth
s8.
02 ±
0.1
4 at
4 m
onth
s8.
04 ±
0.1
4 at
12
mon
ths
No
sign
ifica
nt d
iffer
ence
bet
wee
n co
mbi
ned
inte
rven
tions
an
d co
ntro
l[26]
Gra
nt et a
l. (2
003)
Inte
rven
tion:
7.7
± 1
.7Co
ntro
l: 7.
5 ±
1.1
Not
repo
rted
Not
repo
rted
Not
repo
rted
[27]
Jara
b et al.
(201
2)8.
5-0
.8 a
t 6 m
onth
s po
stin
terv
entio
n+
0.1
at 6
mon
ths
post
inte
rven
tion
Patie
nts
in th
e in
terv
entio
n sh
owed
sig
nific
ant
impr
ovem
ent i
n H
bA1c
leve
ls c
ompa
red
with
the
cont
rol
grou
p (p
= 0
.019
)
[28]
Kim
et a
l. (2
006)
8.1
± 2.
1-1
.1 ±
2.1
No
cont
rol
Sign
ifica
nt c
hang
e in
mea
n H
bA1c
in in
terv
entio
n (p
= 0
.006
)[29]
Ode
gard
et a
l. (2
005)
Inte
rven
tion:
10.
2 ±
0.8
Cont
rol:
10.6
± 1
.4 (p
= 0
.11)
-1.5
at 6
mon
ths
-2 a
t 12
mon
ths
Mea
n H
bA1c
did
not
diff
er b
etw
een
grou
ps a
fter
12
mon
ths
(p =
0.6
1); h
owev
er, t
here
was
a s
igni
fican
t dec
reas
e in
H
bA1c
ove
r tim
e fo
r bot
h gr
oups
(p =
0.0
01)
[32]
Ruba
k et al.
(201
1)In
terv
entio
n: 6
.9Co
ntro
l: 6.
8-0
.7 a
t 12
mon
ths
post
inte
rven
tion
-0.7
at 1
2 m
onth
s po
stin
terv
entio
nSi
gnifi
cant
impr
ovem
ents
wer
e se
en in
bot
h gr
oups
po
stin
terv
entio
n (p
< 0
.01)
. No
stat
istic
ally
sig
nific
ant
diffe
renc
e re
port
ed b
etw
een
grou
ps
[34]
Tan et al.
(201
1)In
terv
entio
n: 9
.9Co
ntro
l: 9.
68.
759.
67Si
gnifi
cant
dec
reas
e in
HbA
1c re
lativ
e to
con
trol
(p <
0.0
01)
[35]
CH
W: C
omm
unit
y he
alth
wor
ker;
CM
: Cas
e m
anag
er; S
D: S
tand
ard
devi
atio
n.
-
Interventions to improve medication adherence in Type 2
diabetes review
future science group www.futuremedicine.com 41
education [16–18,20–23,25–26,28,31–32,34–36,39,41], nine
focusing on skills training [15–18,20–21,35–37], and 13 helping
with problem-solving [16–18,20–21,26–28,31,35–37,41]. Twelve of the
studies emphasizing education – five focusing on skills and seven
assisting with problem-solving – were significant for variations in
medication adherence and/or HbA1c between groups and/or at
differ-ent time points. Eight used monitoring data, such as
providing results of self-monitored blood glucose readings to the
provider [15,25,27,29,31,40–41] and, of these, four were
significant for differ-ences in medication adherence and/or HbA1c.
Fifteen studies provided one-on-one counsel-ing to patients
[17–20,22,24,28–29,31–33,35–36,40–41] and 13 studies were
significant for changes in medication adherence and/or HbA1c. The
study designs for most of the interventions using one-on-one
interactions were RCTs. A total of 14 studies utilized
telehealth/telemedicine tech-nology: mobile phones [22,28,33,40],
telephones [15,17,23,26,30,36,38–40] and the internet [18]. Of
those using health technologies, three of the mobile usage studies
and seven of the studies using telephones were significant for
differ-ences in medication adherence and/or HbA1c. The study using
internet delivery did not show significant differences.
Facilitators were used for intervention delivery in some studies:
eight used nurse educators [17,25,27,31,34,36–37,40], one used
certified diabetes educators (CDEs) [35] and three used CHWs
[16,31,34]. Six involved collaboration with the patients’
physicians [23,26,29–30,38–39]. Of the studies using facilita-tors
that demonstrated statistical significance in medication adherence,
five used nurses, three used CHWs and six used pharmacists. Five of
the six studies collaborating with physi-cians were significant for
medication adherence and/or HbA1c. Using CDEs showed statistical
significance only for HbA1c, as did two of the studies using nurses
and CHWs, and three using pharmacists and physician
collaborations.
In this review, effective medication adher-ence was defined as a
significance improvement at p < 0.05. It is worth mentioning
that out of the 17 articles showing statistical significance in
medication adherence, eight were RCTs, four used a pre–post design,
two were cohort stud-ies, two were quasiexperimental with pre–post
designs, and one used a parallel-group, repeated-measure design.
The remaining studies were all RCTs, one of the strongest research
designs, and did not show a statistically significant difference
T
able
3. G
lyce
mic
con
trol
out
com
es o
f stu
dies
mee
ting
incl
usio
n cr
iteri
a (c
ont.)
.
Stud
y (y
ear)
Mea
n ±
SD b
asel
ine
HbA
1c
(%)
inte
rven
tion
mea
n ±
SD
chan
ge in
or m
ean
± SD
po
stin
terv
entio
n H
bA1c
(%)
Cont
rol m
ean
± SD
ch
ange
in m
edic
atio
n ad
here
nce
Stat
isti
cal s
igni
fican
ceRe
f.
Wak
efiel
d et al.
(201
2)Lo
w-in
tens
ity
inte
rven
tion:
7.2
Hig
h-in
tens
ity
inte
rven
tion:
7.1
Cont
rol:
7.2
Low
inte
nsit
y: -0
.4 a
t 6
mon
ths,
-0.4
4 at
12