Embed Size (px)
Citation preview

AMERICAN JOURNAL OF CRITICAL CARE, January 2003, Volume 12, No. 1 31
• BACKGROUND Tracheal gas insufflation reduces inspired tidal volume and minute ventilation inspontaneously breathing patients and may facilitate weaning from mechanical ventilation.• OBJECTIVE To determine if tracheal gas insufflation can reduce ventilatory demand during weaningtrials in patients who require prolonged mechanical ventilation.• METHODS A reduction in ventilatory demand was defined as a relative decrease in tidal volume,minute ventilation, and mean inspiratory flow during trials with tracheal gas insufflation compared withthe values during trials without this therapy. A total of 14 subjects underwent T-piece trials with andwithout insufflation (flow rate 6 L/min) on 2 consecutive days; the order of insufflation was randomized.Tidal volume, minute ventilation, and mean inspiratory flow were measured at baseline (withoutinsufflation) and 2 hours later.• RESULTS Differences in ventilatory demand were not significant when comparisons were made forcondition (tracheal gas insufflation vs no flow) or time (baseline vs 2 hours) for the total group (P = .48).Subjects were classified post hoc as responders (n = 9) or nonresponders (n = 5). Comparisons betweenresponders and nonresponders indicated a significant (P = .02) 3-way multivariate interaction for group(responder vs nonresponder), condition (tracheal gas insufflation vs no flow), and time (baseline vs 2hours) for ventilatory demand variables.• CONCLUSION Tracheal gas insufflation can reduce ventilatory demand during weaning trials in somepatients who require mechanical ventilation. (American Journal of Critical Care. 2003:12:31-40)
EFFECT OF TRACHEAL GAS INSUFFLATION
DURING WEANING FROM PROLONGED
MECHANICAL VENTILATION: A PRELIMINARY STUDY
To purchase reprints, contact The InnoVision Group, 101 Columbia, AlisoViejo, CA 92656. Phone, (800) 809-2273 or (949) 362-2050 (ext 532); fax,(949) 362-2049; e-mail, [email protected].
By Leslie A. Hoffman, RN, PhD, Frederick J. Tasota, RN, MSN, Edgar Delgado, RRT, Thomas G. Zullo, PhD,and Michael R. Pinsky, MD. From Department of Acute/Tertiary Care, University of Pittsburgh School ofNursing (LAH, FJT, TGZ), and Respiratory Care (ED) and Department of Critical Care Medicine (MRP),University of Pittsburgh Medical Center, Pittsburgh, Pa.
Efficient weaning of patients from prolongedmechanical ventilation continues to be an elu-sive goal. Numerous weaning indices, protocols,
and models of care (eg, weaning teams, case man-agement, specialized weaning units) have been testedin an effort to increase success.1 These strategies canimprove success rates,2-5 but approximately 1% to 5%
of patients receiving mechanical ventilation cannot beweaned from ventilatory support and become long-term ventilator patients.6 The inability to regain thecapacity to breathe without ventilatory support is dueto a variety of causes. However, most commonly, thecause is an imbalance between ventilatory demand andthe patient’s capacity to meet this demand.7-9
Tracheal gas insufflation (TGI) is an adjunctiveventilatory technique that involves inserting a smallcatheter through an endotracheal or tracheostomy tubeto a level just above the carina.10 Alternatively, a catheter
Journal Club Feature
by AACN on January 2, 2019http://ajcc.aacnjournals.org/Downloaded from

32 AMERICAN JOURNAL OF CRITICAL CARE, January 2003, Volume 12, No. 1
can be inserted percutaneously through the anterior wallof the trachea.11 Gas is insufflated through the catheterat various flow rates (eg, 2-10 L/min). TGI can pro-duce an increase in exercise tolerance and a reductionin dyspnea in spontaneously breathing patients withchronic respiratory disease.11-14 Several mechanismsmay contribute to this effect.
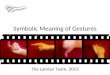
First, the catheter delivers gas lower in the air-ways than during normal breathing, a condition thatreduces anatomic dead space (VDS).15,16 Second, part ofthe inspired tidal volume (VT) enters the lungs pas-sively through the catheter, a situation that decreasesthe oxygen cost of breathing.17 Finally, TGI improvesthe efficiency of carbon dioxide elimination.18,19 Duringexpiration, gas insufflated by the catheter flushes gasladen with carbon dioxide from the anatomic and appa-ratus dead space proximal to the catheter tip (Figure 1).As a result, the amount of carbon dioxide recycled tothe alveoli during the next inspiration is reduced,increasing the ventilatory eff iciency of each tidalbreath.10 Consequently, TGI may reduce ventilatorydemand.11-17,20
Most commonly, TGI has been used as an alterna-tive to traditional oxygen delivery via nasal cannulasin patients with end-stage lung disease.11-14 TGI hasalso been used in conjunction with a lung-protectiveventilatory strategy to improve the efficiency of alveo-lar ventilation and/or minimize ventilator pressurerequirements in patients with acute lung injury.19,20
Use of TGI in patients during weaning from mechan-ical ventilation or after episodes of acute respiratoryfailure that necessitated mechanical ventilation hasalso been investigated.15,16,21-23
Bergofsky and Hurewitz15 tested the potentialadvantages of TGI in 5 patients with chronic respira-tory failure due to obstructive or restrictive disease.VDS, VT, and minute ventilation (Vmin) were signifi-cantly less with TGI than with the no-flow condition.Two patients continued to use TGI for 12 months orlonger, and both had fewer episodes of acute respira-tory failure that required mechanical ventilation whileusing TGI than while receiving oxygen via a tra-cheostomy mask. Hurewitz et al16 extended this workby examining mechanisms that might explain the ben-efits of TGI. With TGI at flow rates of 1, 5, and 8L/min, VDS, VT, and Vmin progressively decreasedwithout an accompanying increase in PaCO2. Thereduction in Vmin was achieved primarily via a reduc-tion in VT, whereas respiratory rate had almost nochange at any flow rate.
Nakos et al21 tested the effects of TGI at flow ratesof 3 and 6 L/min during weaning in 12 spontaneouslybreathing patients with chronic obstructive pulmonary
disease (COPD) who were undergoing weaning trials.In these subjects, TGI progressively decreased the ratioof VDS to VT (VDS/VT), VT, and Vmin; effects weregreatest at the highest flow rates. Schönhofer et al22
found similar changes in 8 patients with COPD treatedwith TGI immediately after weaning from mechanicalventilation. In another study,23 Schönhofer et al found a28% decrease in inspiratory work of breathing relativeto Vmin when TGI was used in 6 patients with COPDwho had undergone long-term mechanical ventilation.In combination, the findings of these studies15,16,21-23 sup-port the notion that TGI can decrease ventilatorydemand in patients with COPD when delivered duringor just after weaning from mechanical ventilation.
The ability of TGI to promote weaning frommechanical ventilation was tested previously only inpatients with COPD.21-23 Because it decreases VT,Vmin, and mean inspiratory flow or the ratio of VT toinspiratory time (VT/TI), TGI may also be useful inweaning patients with other types of pulmonary dys-function from prolonged mechanical ventilation.Accordingly, we tested the ability of TGI to reduceventilatory demand during weaning from mechanicalventilation in patients with and without COPD whorequired prolonged (>14 days) mechanical ventilation.A reduction in ventilatory demand was defined as arelative decrease in VT, Vmin, and VT/TI during trialswith TGI compared with the values during trials with-out this therapy.
Materials and MethodsSample
Subjects were 14 consecutive patients who metthe following criteria: (1) required prolonged (>14days) mechanical ventilation; (2) had a tracheostomybecause they could not be weaned from mechanicalventilation; (3) were undergoing daily weaning trialsordered by the intensive care unit attending physicianat the time of entry into the study; (4) had stablehemodynamic status (ie, no treatment with vasopres-sors, no clinical or radiological evidence of pulmonaryedema, and no unstable arrhythmia); and (5) had hadno evidence of infection for 3 or more days (ie, tem-perature <38°C [<101°F] and white blood cell count<15 x 109/L). The study was approved by the appro-priate institutional review board, and all subjects ortheir legal representative gave informed consent. Allwork was carried out in accordance with standards setforth in the Helsinki Declaration of 1975.
Experimental ProtocolEach subject underwent a 2-hour T-piece wean-
ing trial with and without TGI (flow rate 6 L/min) on
by AACN on January 2, 2019http://ajcc.aacnjournals.org/Downloaded from

AMERICAN JOURNAL OF CRITICAL CARE, January 2003, Volume 12, No. 1 33
2 consecutive days; the order of TGI was randomized.Baseline data were collected to determine respiratoryfrequency, VT, Vmin, and VT/TI 5 minutes after thebeginning of the T-piece trial (baseline) and 2 hourslater. During TGI trials, baseline data were obtained
before TGI was started. Mean arterial blood pressure(cuff pressure), heart rate (standard lead II electrocar-diogram), and arterial oxygen saturation (as deter-mined by pulse oximetry; SpO2) were measured at thesame time points. The protocol required that data col-
Figure 1 Comparison of inspiration and expiration with and without tracheal gas insufflation (TGI) in a patient with atracheotomy. A, Without TGI, during inspiration, all tidal volume (VT) enters the airway through the tracheostomy tube, withactive work by the patient. B, With TGI, during inspiration, part of the VT passively enters lower in the airway at a rate of 100mL/s (flow rate = 6 L/min), improving the patient’s capacity to meet ventilatory demands. C, Without TGI, at the end ofexpiration, gas laden with carbon dioxide (CO2) is present throughout the airway. With the next inspiration, the patientrebreathes this CO2-laden gas as part of the VT. D, With TGI, at the end of expiration, most of the CO2-laden gas is “washedout” with TGI flow and replaced with gas rich in oxygen (O2) before the next inspiration. The efficiency of CO2 elimination isimproved, and the patient’s ventilatory demand is diminished.
No TGIInspiration
TGIInspiration
No TGIExpiration
TGIExpiration
A B
C D
by AACN on January 2, 2019http://ajcc.aacnjournals.org/Downloaded from

34 AMERICAN JOURNAL OF CRITICAL CARE, January 2003, Volume 12, No. 1
lection be terminated if any of the following occurred:SpO2 less than 88%, heart rate greater than 120/min,respirations greater than 35/min or greater than a 15%increase from baseline, new dysrhythmia or change inbaseline dysrhythmia, or request for discontinuationby the subject.
TGI ApparatusA single distal-lumen catheter (internal diameter
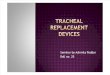
1.67 mm) was inserted through a jet-ventilator adapter(model 600101, Concord/Portex, Keene, NH) for TGI(Figure 2). Before the catheter was inserted, a recentchest radiograph was assessed to determine the posi-tion of the tracheal tube in relationship to the carina.The catheter was then passed ex vivo through a tra-cheal tube of the same size and model as that used inthe patient to a position that would place the cathetertip approximately 1 cm above the carina and waslocked in position by using the jet-ventilator adapter.The catheter and adapter were then inserted into thepatient’s tracheal tube. Gas was delivered through acalibrated flow generator (Bellofram, Newell, WV) at
a flow rate of 6 L/min with the same fraction of inspiredoxygen (0.40-0.50) as that ordered for the weaning trial(Air/O2 Microblender, Bird Products Corp, PalmSprings, Calif). No humidification of the insufflated gaswas used because of the short duration of the study.
During no-flow conditions, the TGI catheter waspositioned in the tracheostomy tube in the same man-ner as during the TGI condition, but no gas was deliv-ered. This practice ensured that patients experiencedequal resistance to air flow during both conditions(TGI vs no TGI).
Respiratory Inductive PlethysmographyRespiratory inductive plethysmography bands
were positioned and secured around the patient’s ribcage and abdomen. The plethysmography device(RespiTrace Plus, Nims, Miami Beach, Fla) was cali-brated by using the semiquantitative single-positioncalibration method, with the patient receiving breathsof consistent volume from the ventilator.24 Subjectswere placed in the same position after the bands werepositioned and were maintained in this positionthroughout calibration and the experimental protocolon both days. Respiratory inductive plethysmographywas used to directly measure all gas entering the pa-tients’ lungs, because total inspired VT included gasfrom spontaneous inspiration and TGI-derived gas. Inaddition, respiratory inductive plethysmography wasused to measure respirations and VT/TI. Signals fromthe RespiTrace were imported for 5 minutes at eachdata collection point and were stored in a computer(Colorbook DX2-50, Gateway 2000, N Sioux City, SD)by using RespiEvents software (Version 4.1, Nims,Miami Beach, Fla). A minimum of 1 minute of contin-uous respiratory inductive plethysmography data wasused for analysis.
Data AnalysisData were analyzed for the total group and for
responders and nonresponders to TGI by using multi-variate and univariate analyses of variance. Subjectswere classified as responders or nonresponders posthoc by using change scores calculated by subtractingthe baseline values for VT, Vmin, and VT/TI from the2-hour values. Responders were defined as subjectswho had a minimum of 20% difference (decrease orless of an increase) with TGI than without TGI in atleast 2 of the 3 parameters measured. Subjects whodid not fulfill these criteria were defined as nonrespon-ders. Demographic data and data on medical conditionswere analyzed by using the Fisher exact test (diagnosis,sex) and the Mann-Whitney test (age, ventilator days,pretrial PaCO2 from an arterial blood gas analysis) with
Figure 2 Apparatus used for tracheal gas insufflation. A,Catheter and jet-ventilator adapter used to deliver the gas.B, The catheter is passed through a tracheostomy tube ofthe same size and model as that used in the patient to betreated to a position that places the tip approximately 1cm above the carina and is locked in place with a jet-ventilator adapter.
A
B
by AACN on January 2, 2019http://ajcc.aacnjournals.org/Downloaded from

AMERICAN JOURNAL OF CRITICAL CARE, January 2003, Volume 12, No. 1 35
a Bonferroni correction for multiple comparisons.Differences were considered significant at P<.05.
ResultsCharacteristics of the Sample
The subjects consisted of 8 men and 6 women 36 to73 years old (Table 1). They had been receiving mech-anical ventilation for a mean of 36.0 days (SD = 15.1days, range = 15-65 days) and were receiving a meanfraction of inspired oxygen of 0.46 (SD = 0.05) at thetime of data collection. Samples for arterial blood gasanalysis were obtained with the patients off mechani-cal ventilation within 3 days of data collection for 12subjects (mean PaCO2 = 51.5 mm Hg, SD = 11.6 mmHg). All subjects completed the 2-hour trial with noadverse effects.
Total Group ResponseNo significant differences in ventilatory demand
(VT, Vmin, VT/TI) were detected when multivariate
comparisons were made for condition (TGI vs noflow), time (baseline vs 2 hours), or the interaction ofcondition and time for the total group. Furthermore,multivariate analysis indicated no significant differ-ences in heart rate, mean arterial pressure, and SpO2 forcondition, time, or the interaction of condition andtime. Univariate analysis revealed a statistically signifi-cant (P = .01), but clinically unimportant, increase inheart rate from a mean of 97.6/min (SD = 15.6/min) atbaseline to a mean of 100.9/min (SD = 14.9/min) at 2hours without TGI.
Responders and NonrespondersOn the basis of change scores, 9 subjects were
classified as responders and 5 subjects as nonrespon-ders. Comparisons between responders and nonrespon-ders indicated a significant (P = .02) 3-way multivariateinteraction for group (responder vs nonresponder),condition (TGI vs no flow), and time (baseline vs 2hours) for ventilatory demand variables (Table 2). In
Table 1 Characteristics of the sample
RespondersAcute respiratory failureNeurodegenerative diseaseLung cancerSepsis
Liver transplantationAcute respiratory failure
PneumoniaHemicolectomyMultivisceral
transplantation/sepsis
NonrespondersLiver transplantationHeart–bilateral lung
transplantationSepsisSepsis
Liver transplantation
Responders plus nonresponders
Primary diagnosis orcondition
Pulmonary diagnosis orcondition
Obstructive lung diseaseAspiration pneumoniaObstructive lung diseaseObstructive lung
disease/acute respiratorydistress syndrome
Obstructive lung diseaseRestrictive lung
disease/scoliosisα1-Antitrypsin deficiencyObstructive lung diseasePneumonia
Mean (SD)
Postoperative complications Diffuse alveolar disease
Acute respiratory failureAcute respiratory distress
syndromePostoperative complications
Mean (SD)
Mean (SD)
Age,years
60605949
4770
547336
56.4 (11.5)
4541
4053
48
42.4 (15.0)
52.5 (11.0)
Sex
MaleMaleMaleMale
MaleMale
MaleFemaleFemale
MaleFemale
FemaleFemale
Female
NA
NA
Days ofmechanicalventilation
49352615
2024
183133
27.9 (10.5)
5139
4355
65
50.6 (10.2)
36.0 (15.1)
Weaningfraction of
inspiredoxygen
0.50.40.50.5
0.50.4
0.40.50.4
0.46 (0.05)
0.40.5
0.50.5
0.4
0.46 (0.05)
0.46 (0.05)
PretrialPaCO2 off
mechanical ventilation,
mm Hg
60406652
5868
5060ND
56.8 (9.1)
3052
4141
ND
41.0 (9.0)
51.5 (11.6)
NA indicates not applicable; ND, not determined.
by AACN on January 2, 2019http://ajcc.aacnjournals.org/Downloaded from

36 AMERICAN JOURNAL OF CRITICAL CARE, January 2003, Volume 12, No. 1
addition, analysis revealed significant 3-way univari-ate interactions (group, condition, time) for VT (P =.006), Vmin (P= .008), and VT/TI (P < .001).
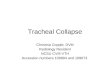
Responders had a 13% decrease in VT, a 10%decrease in Vmin, and a 19% decrease in VT/TI whencomparisons were made between baseline and 2hours during TGI (Figure 3). The respiratory rateremained unchanged. During the no-TGI condition,responders’ respirations increased 19%; VT, 26%;Vmin, 57%; and VT/TI, 39%.
For nonresponders, comparisons between baselineand 2-hour values during TGI indicated a 24% increasein VT, a 42% increase in Vmin, and a 43% increase inVT/TI (Figure 4). Without TGI, changes in these vari-ables were minimal.
Analysis of demographic data and data on medi-cal conditions indicated that responders were morelikely than nonresponders to have a history of obstruc-tive or restrictive lung disease and that nonresponderswere more likely than responders to have an acute pul-monary problem (P = .02). In addition, respondersreceived mechanical ventilation for fewer days than didnonresponders (mean = 27.9 days; SD = 10.5 days vsmean=50.6 days; SD=10.2 days, respectively; P= .002).After Bonferroni correction was used, differences insex, age, and pretrial PaCO2 were not signif icant.However, analysis indicated a trend toward a higherpretrial PaCO2 in the responders than in the nonre-sponders (P = .05).
DiscussionWe found that adding TGI during a T-piece trial in
patients being weaned from prolonged mechanical ven-tilation produced changes consistent with a decreasein ventilatory demand in some but not all patients.Those patients most likely to benefit from TGI had ahistory of obstructive or restrictive lung disease andtended to be hypercapnic, whereas those with anacute pulmonary process tended to have an adverseresponse to TGI during weaning trials. In addition,duration of mechanical ventilation differed in the 2groups; responders received ventilatory support forfewer days than nonresponders did.
For a given level of ventilation, increasing respi-ratory rate, although simultaneously limiting the VT
of each breath, can minimize energy output. Theconsequence (ie, rapid, shallow breathing) can beconsidered an adaptation to reduce fatigue. Unfor-tunately, as VT decreases, VDS increases, and thisincrease reduces ventilatory efficiency. Therefore, Vminmust be increased or hypercapnia will develop.7-9 Inthis situation, TGI might confer unique benef itsbecause it can reduce VDS/VT and inspired VT andenhance the eff iciency of carbon dioxide elimination,thus decreasing the imbalance between ventilatorydemand and capacity. Our findings suggest that useof TGI may reduce ventilatory demand, but only inpatients with underlying obstructive or restrictive pul-monary dysfunction.
Table 2 Ventilatory and cardiopulmonary responses to tracheal gas insufflation (TGI) during weaning from mechanicalventilation at baseline and 2 hours later with and without TGI*
Responders
2 hours
25 (11)
524 (213)13.0 (8.8)
521 (312)
89 (13)
97 (17)
98 (2)
Baseline
26 (3)
411 (279)10.4 (6.6)
382 (177)
94 (12)
103 (14)
99 (3)
2 hours
28 (6)
511 (236)14.8 (6.0)
548 (166)
95 (19)
106 (10)
99 (2)
Baseline
25 (4)
395 (151)9.9 (3.3)
415 (172)
100 (12)
100 (8)
99 (2)
2 hours
29 (6)
388 (162)10.4 (2.5)
415 (96)
96 (19)
108 (6)
99 (3)
Nonresponders
Variables
VentilatoryRespirations, breaths
per minuteTidal volume, mL/kgMinute ventilation,
L/minMean inspiratory flow,
mL/secCardiopulmonary
Mean arterial pressure,mm Hg
Heart rate, beats perminute
Oxygen saturation, %
Baseline
22 (6)
478 (255)9.4 (3.5)
520 (427)
82 (9)
97 (14)
98 (2)
2 hours
22 (8)
418 (181)8.5 (4.3)
423 (285)
81 (8)
93 (16)
99 (1)
Baseline
21 (6)
415 (172)8.3 (3.1)
375 (170)
80 (15)
94 (14)
98 (2)
*Values are mean (SD). Mean inspiratory flow = tidal volume/inspiratory time.
TGI No TGI TGI No TGI
by AACN on January 2, 2019http://ajcc.aacnjournals.org/Downloaded from

AMERICAN JOURNAL OF CRITICAL CARE, January 2003, Volume 12, No. 1 37
Nakos et al21 evaluated the effect of TGI in 12spontaneously breathing patients with COPD whowere undergoing weaning from mechanical ventilation;7 of the 12 had an endotracheal tube in place, and 5had a tracheostomy tube. During TGI, VT, Vmin,PaCO2, and VDS/VT were reduced in a flow-dependentmanner when gas was delivered through the endotra-cheal tube at flow rates of 3 and 6 L/min. The patientswith tracheostomy tubes had a similar response, but sig-nificant changes occurred only during the higher flowrate (ie, 6 L/min), presumably because the tracheostomyreduced VDS. In our study, we used a single flow rate (6L/min), and the responder group, predominately patientswith obstructive lung disease, had similar changes inVT and Vmin.
The group we characterized as nonresponders haddifferent changes. Without TGI, nonresponders increasedrespiratory rate 16% but had minimal increases in VT
(2%) and Vmin (5%), as would be anticipated during aweaning trial. During TGI, respirations changed mini-mally (8%), but marked increases occurred in VT (24%)and Vmin (42%). Consequently, the ventilatory pattern innonresponders did not change despite tracheal gas flow.Thus, the patients realized a 100-mL increase in VT
equivalent to the gas flow delivered by the catheter dur-ing inspiration. The reason neither respiratory rate norVT decreased during TGI is unknown, but it might havebeen an overriding increase in respiratory drive. Allpatients characterized as nonresponders experienced
acute respiratory failure due to an acute pulmonary pro-cess and, except for 1 patient, were normocapnic.Notably, the nonresponder who was hypercapnic was aheart-lung transplant recipient. Presumably, the conse-quences of pulmonary denervation precluded a similarresponse in this patient, as in other patients withhypercapnia. The ventilatory response to TGI inhypercapnic patients with obstructive and restrictivelung disease in our study was similar to that reportedin patients receiving transtracheal oxygen therapy.11-14
Like our patients, those patients consistently had asubstantial reduction in inspired VT and Vmin. Further,airway insufflation via a transtracheal catheter reducesthe oxygen cost of breathing and shifts the diaphragmto a less demanding pattern.17 The changes in respon-ders to TGI might facilitate the ability to tolerate alonger weaning trial; however, we did not evaluate thispotential.
Responses to TGI in patients who experiencedacute respiratory failure and were successfully weanedfrom mechanical ventilation were evaluated in severalother studies. Schönhofer et al22,23 inserted a transtra-cheal catheter into the tracheostomy stoma and closedthe area around the stoma with a latex membrane.Thereafter, measures were taken during two 1-hour tri-als in which patients received TGI at a flow rate of 2L/min or no flow. However, the long-term responsewas not evaluated. Bergofsky et al15 used a similar
Figure 3 Impact of tracheal gas insufflation (TGI) onresponders. Percentage change in respirations, tidal volume(VT), minute ventilation (Vmin), and mean inspiratory flow(VT/TI), from baseline (before weaning trial) to 2 hourslater with TGI (flow; light bars) and without TGI (no flow;dark bars).
VT/TI
Vmin
VT
-20 -10 0 10 20 30 40 50 60
No flow
Flow
Percentage change
39
57
26
19
-19
-10
-13
0Respirations
Figure 4 Impact of tracheal gas insufflation (TGI) onnonresponders. Percentage change in respirations, tidalvolume (VT), minute ventilation (Vmin), and meaninspiratory flow (VT/TI) from baseline (before weaningtrial) to 2 hours later with TGI (flow; light bars) andwithout TGI (no flow; dark bars).
VT/TI
Vmin
VT
-20 -10 0 10 20 30 40 50
No flow
Flow
Percentage change
43
42
24
13
5
2
6
0
Respirations
by AACN on January 2, 2019http://ajcc.aacnjournals.org/Downloaded from

38 AMERICAN JOURNAL OF CRITICAL CARE, January 2003, Volume 12, No. 1
technique in 5 patients with chronic hypercapnia and apermanent tracheostomy. Of these 5 patients, 2 chose tocontinue use of TGI through the tracheostomy stoma,which was allowed to close around the catheter. In these2, the number of episodes of respiratory failure requir-ing intubation was reduced during 4 and 12 months offollow-up, suggesting that TGI may confer benefits overan extended period in patients with chronic hypercapnia.
Our goal in this study was to determine if use ofTGI might confer benefits in weaning from mechanicalventilation in patients who were difficult to wean andwho had various diagnoses. Our findings indicate thatthe changes in ventilatory pattern induced by TGI couldbe beneficial for some patients. Potentially, TGI couldassist patients to tolerate longer weaning trials and, ulti-mately, breathe with TGI alone. The insufflating gascould be delivered through a catheter placed in the tra-cheostomy tube (if needed for removal of secretions) ortracheostomy stoma, and the opening could be allowedto close through granulation. When no longer needed,the TGI device could be withdrawn. Thus, TGI mightserve as a “bridge” to spontaneous ventilation.
Alternatively, the insufflating gas might be deliv-ered by using existing equipment, such as the tubing ofa “talking trach” adapter. With the cuff deflated, gasflow from the adapter would create an effect similar tothe effect we tested. However, because gas would bedelivered higher in the airway (adapter vs carina), lessVDS would be available for washout of carbon dioxide,a factor that might preclude benefit. Nakos et al21 deter-mined the effects of TGI when the catheter tip wasplaced at a proximal (3-4 cm into the tracheostomytube) and at a distal (1 cm above the carina) position inthe airway. Compared with the values during no flow,VT and Vmin decreased significantly with TGI, but onlywhen the catheter was in the distal position. Althoughthese f indings suggest this approach might not beeffective, it merits testing because it eliminates theneed for extra equipment.
An important issue in clinical use of TGI is theeffect of this therapy on airway secretions. Moststudies25-27 of TGI were done in patients with end-stage lung disease. In these studies, “mucous balls,” anaccumulation of inspissated mucus that adheres to thecatheter tip, caused infrequent, but serious, complica-tions. If the mucus is not cleared, the mass can increasein size until it partially or totally obstructs the airway.One fatality caused by a mucous ball has beenreported.28 Patients being weaned from mechanical ven-tilation most likely have more secretions than dopatients with end-stage lung disease and therefore are athigher risk for this complication.29 Patients beingweaned from mechanical ventilation are also likely to
have a weak cough, making it more difficult to gener-ate the glottic blast that dislodges mucous balls.Because of the risk of complications, the cathetershould be removed from the tracheostomy tube every 8to 12 hours to assess for the accumulation of mucus.30
Most studies of TGI in mechanically ventilatedpatients were short-term, and the investigators eitherdid not report if the TGI gas was humidified or reportedthat a nonheated, dry gas was used.30 In 2 of 12 adultstreated with mechanical ventilation who used TGI for72 or fewer hours, catheter obstruction due to a muc-ous plug developed (at 58 and 67 hours) despite use ofhumidified gas.31 Both events were detected on thebasis of whistling sounds emitting from the pressure-release valve on the humidifier, and no adverse sequelaoccurred. In another study32 in which humidified andwarmed gas was used with TGI in 9 premature new-borns for up to 31 days (mean 17 days), no problemsdue to formation of a mucous plug occurred. One dif-ference between the gas-conditioning techniques usedin these studies was that Danan et al32 used a heatedhumidifier, whereas Kuo et al31 humidified but did notheat the inspired gas.
Data on changes in the airway morphology afteruse of TGI are limited. Danan et al32 found no trachealabnormalities at autopsy in 3 premature newborns whohad received TGI for 5, 7, or 30 days. Christopher et al14
reported no abnormalities in 13 adults who had receivedtranstracheal oxygen for a mean of 29 months (SD = 26months) and were subsequently treated with oxygennocturnally at a flow rate of 10 L/min for 3 months aspart of a clinical trial. Nocturnally, gas at high flow rateswas provided via a high-humidity oxygen enricher. Inthis study,14 bronchoscopic examination revealed noevidence of hemorrhage, exudates, ulceration, or necro-sis before or after use of the higher flow rate. On thebasis of the limited data available, TGI appears tocause no untoward damage to the airway.
Our study was subject to several limitations. Thesample size was small, and post hoc analysis was usedto identify responders and nonresponders to TGI. Ourfindings are therefore preliminary and should be testedin a prospective randomized trial. The patients mostlikely to benefit from TGI tended to have hypercapnia,as indicated by arterial blood gas analysis of bloodsamples obtained within 3 days of data collectionwhen the patients were off mechanical ventilation.Our ability to fully evaluate a potential decrease inPaCO2 with TGI was limited by the use of noninvasivemeasures. Patients in our protocol were being weanedfrom prolonged mechanical ventilation and no longerhad arterial catheters in place. We chose not to reinsert
by AACN on January 2, 2019http://ajcc.aacnjournals.org/Downloaded from

AMERICAN JOURNAL OF CRITICAL CARE, January 2003, Volume 12, No. 1 39
A. Physiologic determinants of ventilator dependence in long-term mechan-ically ventilated patients. Am J Respir Crit Care Med. 2000;161:1115-1123.
9. Marini JJ. Weaning from mechanical ventilation [editorial]. N Engl J Med.1991;324:1496-1498.
10. Ravenscraft SA. Tracheal gas insufflation: adjunct to conventional mechani-cal ventilation. Respir Care. 1996;41:105-111.
11. Heimlich HJ, Carr GC. Transtracheal catheter technique for pulmonaryrehabilitation. Ann Otol Rhinol Laryngol. 1985;94:502-504.
12. Hoffman LA, Dauber JH, Ferson PF, Openbrier DR, Zullo TG. Patientresponse to tracheal oxygen delivery. Am Rev Respir Dis. 1987;135:153-156.
13. Wesmiller SW, Hoffman LA, Sciurba FC, Ferson PF, Johnson JJ, DauberJH. Exercise tolerance during nasal cannula and transtracheal oxygendelivery. Am Rev Respir Dis. 1990;141:789-791.
14. Christopher KL, Van Hooser DT, Jorgenson SJ, et al. Preliminary observa-tions of transtracheal augmented ventilation for chronic severe respiratory dis-ease. Resp Care. 2001;46:15-25.
15. Bergofsky EH, Hurewitz AN. Airway insufflation: physiologic effects on acuteand chronic gas exchange in humans. Am Rev Respir Dis. 1989;140:885-890.
16. Hurewitz AN, Bergofsky EH, Vomero E. Airway insufflation: increasingflow rates progressively reduce dead space in respiratory failure. Am RevRespir Dis. 1991;144:1229-1233.
17. Benditt J, Pollock M, Roa J, Celli B. Transtracheal delivery of gas decreasesthe oxygen cost of breathing. Am Rev Respir Dis. 1993;147:1207-1210.
18. Scott GC, Hinson JH, Scott RP, Quigley PR, Christopher KL, Metzler M. Theeffects of transtracheal gas delivery on central inspiratory neuromusculardrive. Chest. 1993;104:1199-1202.
19. Nahum A, Burke WC, Ravenscraft SA, et al. Lung mechanics and gasexchange during pressure-control ventilation in dogs: augmentation of CO2elimination by an intratracheal catheter. Am Rev Respir Dis. 1992;146:965-973.
20. Hoffman LA, Miro AM, Tasota FJ, et al. Tracheal gas insufflation: limits ofefficacy in adults with acute respiratory distress syndrome. Am J Respir CritCare Med. 2000;162:387-392.
21. Nakos G, Lachana A, Prekates A, et al. Respiratory effects of tracheal gasinsufflation in spontaneously breathing COPD patients. Intensive Care Med.1995;21:904-912.
22. Schönhofer B, Wenzel M, Wiemann J, Kohler D. Transtracheal oxygeninsufflation: decrease of inspiratory work in weaning from prolongedmechanical ventilation [in German]. Intensivmed. 1995;32:199-204.
23. Schönhofer B, Wenzel M, Wiemann J, Kohler D. Value of transtrachealoxygen insufflation in the weaning period after mechanical ventilation [inGerman]. Med Klin. 1995;90(1 suppl 1):9-12.
24. Neumann P, Zinserling J, Haase C, Sydow M, Burchardi H. Evaluation ofrespiratory inductive plethysmography in controlled ventilation: measure-ment of tidal volume and PEEP-induced changes of end-expiratory lung vol-ume. Chest. 1998;113:443-451.
25. Hoffman LA, Johnson JT, Wesmiller SW, et al. Transtracheal delivery ofoxygen: efficacy and safety for long-term continuous therapy. Ann OtolRhinol Laryngol. 1991;100:108-115.
26. Adamo JP, Mehta AC, Stelmach K, et al. The Cleveland Clinic’s initial expe-rience with transtracheal oxygen therapy. Respir Care. 1990;35:153-160.
27. Orvidas LJ, Kasperbauer JL, Staats BA, Olsen KD. Long-term clinicalexperience with transtracheal oxygen catheters. Mayo Clin Proc. 1998;73:739-744.
28. Fletcher EC, Nickeson D, Costarangos-Galarza C. Endotracheal mass result-ing from a transtracheal oxygen catheter. Chest. 1988;93:438-439.
29. Adams AB. Tracheal gas insufflation. Respir Care. 1996;41:285-291.30. Delgado E, Hoffman LA, Tasota FJ, Pinsky MR. Monitoring and humidifi-
cation during tracheal gas insufflation. Respir Care. 2001;46:185-192.31. Kuo PH, Wu HD, Yu CJ, Yang SC, Lai YL, Yang PC. Efficacy of tra-
cheal gas insufflation in acute respiratory distress syndrome with permis-sive hypercapnia. Am J Respir Crit Care Med. 1996;154:612-616.
32. Danan C, Dassieu G, Janaud GC, Brochard L. Efficacy of dead-spacewashout in mechanically ventilated premature newborns. Am J Respir CritCare Med. 1996;153:1571-1576.
arterial catheters. To equalize airflow resistance betweenconditions (ie, TGI and no TGI), we positioned acatheter in the tracheostomy tube during both condi-tions. Therefore, we were able to analyze the effects ofTGI independent of the effects due to airflow resistance.Our findings might have differed if the catheter had notbeen present during the no-flow condition. Finally, ourstudy was designed to evaluate only the short-termresponse to TGI and therefore does not provide anyinformation about the ability of this technique to facili-tate weaning from mechanical ventilation.
In summary, use of TGI during a 2-hour T-piecetrial produced changes consistent with a decrease inventilatory demand in some but not all patientsbeing weaned from prolonged mechanical ventila-tion. Responders, that is, patients most likely to bene-fit from TGI, were more likely than nonresponders tohave a history of obstructive or restrictive lung diseaseand received mechanical ventilation for fewer days thannonresponders did. Nonresponders were more likelythan responders to have an acute pulmonary process.
ACKNOWLEDGMENTSThis research was performed at the University of Pittsburgh Medical Center andwas supported by grant RO1 NR01086 from the National Institute for NursingResearch, National Institutes of Health.
REFERENCES1. Criteria for Weaning From Mechanical Ventilation: Evidence Report/
Technology Assessment No. 23. Rockville, Md: US Dept of Health andHuman Services, Agency for Healthcare Research and Quality; 2000. AHRQPublication No. 01-E010.
2. Gracey DR, Hardy DC, Naessens JM, Silverstein MD, Hubmayr RD. TheMayo ventilator-dependent rehabilitation unit: a 5-year experience. Mayo ClinProc. 1997;72:13-19.
3. Burns SM, Marshall M, Burns JE, et al. Design, testing, and results of anoutcomes-managed approach to patients requiring prolonged mechanicalventilation. Am J Crit Care. 1998;7:45-57.
4. Seneff MG, Wagner D, Thompson D, Honeycutt C, Silver MR. Theimpact of long-term acute-care facilities on the outcome and cost of carefor patients undergoing prolonged mechanical ventilation. Crit Care Med.2000;28:342-350.
5. Scheinhorn DJ, Chao DC, Stearn-Hassenpflug M, Wallace WA. Outcomesin post-ICU mechanical ventilation: a therapist-implemented weaning proto-col. Chest. 2001;119:236-242.
6. Celli BR. Home mechanical ventilation. In: Tobin MJ, ed. Principles andPractice of Mechanical Ventilation. New York, NY: McGraw-Hill Inc;1994:619-629.
7. Vitacca M, Vianello A, Colombo D, et al. Comparison of two methods forweaning patients with chronic obstructive pulmonary disease requiringmechanical ventilation for more than 15 days. Am J Respir Crit Care Med.2001;164:225-230.
8. Purro A, Appendini L, De Gaetano A, Gudjonsdottir M, Donner CF, Rossi
by AACN on January 2, 2019http://ajcc.aacnjournals.org/Downloaded from

Leslie A. Hoffman, Frederick J. Tasota, Edgar Delgado, Thomas G. Zullo and Michael R. PinskyVentilation: A Preliminary StudyEffect of Tracheal Gas Insufflation During Weaning From Prolonged Mechanical
http://ajcc.aacnjournals.org/Published online Copyright © 2003 by the American Association of Critical-Care Nurses
31-39 12 2003;Am J Crit Care
http://ajcc.aacnjournals.org/cgi/external_ref?link_type=PERMISSIONDIRECTPersonal use only. For copyright permission information:
http://ajcc.aacnjournals.org/subscriptions/Subscription Information
http://ajcc.aacnjournals.org/misc/ifora.xhtmlInformation for authors
http://www.editorialmanager.com/ajcc Submit a manuscript
http://ajcc.aacnjournals.org/subscriptions/etoc.xhtmlEmail alerts
. 532. Fax: (949) 362-2049. Copyright ©2016 by AACN. All rights reserved(AACN) published bimonthly by AACN, 101 Columbia, Aliso Viejo, CA 92656. Telephone: (800) 899-1712, (949) 362-2050, ext. The American Journal of Critical Care is an official peer-reviewed journal of the American Association of Critical-Care Nurses
by AACN on January 2, 2019http://ajcc.aacnjournals.org/Downloaded from




![Transnasal Humidified Rapid Insufflation Ventilatory ... · International symposium in Critical Care and Emergency Medicine (ISICEM 2015) [4] Kinsella SM, et al. Failed tracheal intubation](https://img.dokumen.tips/doc/110x75/5f600bb324038f14e2462b97/transnasal-humidified-rapid-insufflation-ventilatory-international-symposium.jpg)