Embed Size (px)
Citation preview

Effect of temporomandibular joint bony ankylosisand surgical sequelae of gap arthroplasty on middleear volumeMohammad Dehisa, Wahid H. Tantawyb, Abeer Kamalc, Sayed A. Rashedc
and Mamdouh Sayeda
Aim The aim of this study was to evaluate the effect of
temporomandibular joint bony ankylosis and surgical
sequelae of gap arthroplasty on middle ear volume (MEV).
Patients and methods Sixteen Egyptian individuals were
selected and divided into two equal groups. The first group
(group I) included eight patients with 14 bony ankylosed
joints; the second group (group II) included eight normal
individuals. The operated patients were chosen from those
attending the outpatient clinic of the Department of
Oral and Maxillofacial Surgery, Faculty of Oral and Dental
Medicine, Cairo University. Gap arthroplasty was utilized
for the management of such patients. Radiographic
assessments for MEV for the first group were obtained
for all the participants preoperatively and also 3 months
postoperatively. Comparison of MEV was carried out with
normal individuals both preoperatively and 3 months
postoperatively.
Results It was observed that there was a significant
decrease in MEV of ankylosed patients preoperatively
when compared with normal individuals and a
significant decrease in MEV 3 months postoperatively
when compared with the preoperative volume.
Conclusion Patients with temporomandibular joint
bony ankylosis showed a decrease in MEV
compared with normal individuals; also, gap arthroplasty
has a decreasing effect on MEV. Egypt J Oral Maxillofac
Surg 4:72–77 �c 2013 The Egyptian Association of Oral &
Maxillofacial Surgeons.
Egyptian Journal of Oral & Maxillofacial Surgery 2013, 4:72–77
Keywords: computed tomography, gap arthroplasty, middle ear volume,temporomandibular joint ankylosis
aDepartment of Oral and Maxillofacial Surgery, Faculty of Oral and DentalMedicine, Cairo University, bDepartment of Radiology, Faculty of Medicine,Ain Shams University, Cairo and cDepartment of Oral Surgery, Faculty of Oral andDental Surgery, Misr University for Science and Technology (MUST), Giza, Egypt
Correspondence to Abeer Kamal, BDS, MSc, PhD, Department of Oral Surgery,Faculty of Oral and Dental Surgery, Misr University for Science and Technology(MUST), 7 Ghernat St., Roxy Heliopolis, 413 EgyptTel: + 20 24543572/ + 20 1005168009; fax: + 002 02 24543572;e-mail: [email protected]
Received 20 June 2013 accepted 20 July 2013
Introduction and review of the literatureTrauma was reported to be the first etiologic factor in
temporomandibular joint (TMJ) bony ankylosis. Hemar-
throsis and the anatomical nature of joints in children
are believed to be the major cause, whereas condylar
fractures with iatrogenic factors were found to be the
major etiologic factor in adults. TMJ disruption was
reported to be involved in massive head trauma
complicated with the presence of a temporal bone
fracture. It was hypothesized that displaced fracture of
the posterior wall of the TMJ may affect the middle ear
because of a concomitant perforation, leading to ossicular
chain discontinuity. High-resolution computed tomogra-
phy (CT) is an appropriate investigation for the detection
of middle ear changes with ossicular disruptions showing
separation of the incudostapedial joint, fracture of the
stapes, and dislocation of the incus [1–3].
The treatment of TMJ ankylosis poses a significant
challenge because of its technical difficulties and a high
incidence of recurrence. Gap arthroplasty has been
described as a simple and effective surgical technique
in the management of TMJ ankylosis. It is the technique
of resecting a segment of the bone at some point between
the base of the skull and the site of the mandibular
foramen. The gap created usually ranges from 0.6 to
1.5 cm and up to 2 cm as recommended by Topazian [4].
The induced gap should be established at the most
superior part of the ramus to maintain a maximal ramal
height, to minimize the possibility of occurrence of
anterior open bite, and to increase the chance of
normality of postoperative mandibular function [5–7].
The ear and the TMJ are embryologically, physically, and
anatomically very close to each other and have a strong
influence on proper functioning of each other. Pain of
the TMJ may lead to contraction of the little muscles
(the tensor tympani and tensor veli palatini) inside the
tympanic cavity. These muscles hold the ear bones
(malleus, incus, and stapes) in place. All these three ear
bones are essential to the function of hearing. The
contraction and spasm of these muscles cause hearing
impairment by affecting the proper functioning of the ear
bones [8,9].
Posterior displacement of the condyle has been reported
to exert pressure on the auriculotemporal nerve and the
chorda tympani, as well as the Eustachian tube. Pressure
on these structures might induce erosion of the tympanic
plate. Eustachian tube dysfunction has been attributed
to reflex disturbances of the tensor tympani and the veli
palatini muscles. Bettega et al. [10] and Ioannides and
Hoogland [11] reported that the otomandibular (e.g.
diskomalleolar and tympanomandibular) ligaments are
among the structural causes for aural symptoms. It is
hypothesized that patients with TMJ disorders have
muscle spasms responsible for regulating the activity of
the Eustachian tube [12–17].
72 Research paper
2090-097X �c 2013 The Egyptian Association of Oral & Maxillofacial Surgeons DOI: 10.1097/01.OMX.0000434297.76601.e3

It has been reported that the average middle ear volumes
(MEVs) in the normal ears, as measured using CT, were
5.6–7.9 ml [18–20]. Ahn et al. [21] reported that the
MEVs were 1.1 ± 0.8 ml in 44 ears with chronic otitis
media, which were smaller than the normal values.
Acquired cholesteatoma is the main complication of
chronic otitis, resulting from ingrowth of the keratinizing
squamous epithelium from the external acoustic meatus
to the middle ear through the tympanic membrane. It
was represented on the CT scan in the form of a soft-
tissue mass-like opacity in the middle ear cavity and
mastoid antrum associated with smooth bony erosion of
the ossicles and expansion of adjacent structures [22].
CT examination of patients with osteopetrosis showed
conductive hearing loss, and this was attributed to
exostosis projection into the middle ear cavity, calcified
and sclerotic ossicles, recurrent otitis media, and poor
aeration of the mastoid air cells, with no evidence of
internal auditory canal narrowing [23–25]. A CT scan of
Paget’s disease of the skull showed thickening of the
auditory ossicles and stapes suprastructure was not
visible; these findings explain the hearing impairment
in patients with Paget’s disease [26].
High-resolution CT of the temporal bone is the method
of choice for the evaluation of ossicular chain integrity
and tympanic cavity walls. Axial high-resolution CT scans
can ordinarily show the exact nature and placement of
the ossicular fractures and dislocations. High-resolution
CTof the middle ear is a useful noninvasive technique; it
can detect the extent of the disease, exact location,
structures involved, and possible bone erosion. It can be
addressed in cases of traumatic and nontraumatic
opacified middle ear, acute coalescent otomastoiditis,
and chronic otitis media. Recently, virtual endoscopy and
three-dimensional reconstructions of the middle ear as
well as the tympanic cavity were used to assess middle
ear pathologies and ossicular injuries using the standard
high-resolution CT temporal bone as a template [27,28].
Patients and methodsThis study included 16 Egyptian individuals. They were
divided equally into two groups. The first group (group I)
had 14 bony ankylosed TMJ. They were selected from
those attending the outpatient clinic of the Department
of Oral and Maxillofacial Surgery, Faculty of Oral and
Dental Medicine, Cairo University, Egypt. The second
group (group II) included normal individuals of the same
age (range, mean) and sex distribution. They were
recruited from among patients with other medical
conditions of the temporal bone in whom no abnormal-
ities of the middle ear were detected; consequently, CT
was not performed specifically for the middle ear to avoid
extra radiation hazard. The condition was explained and
their consents were obtained. Every patient of group I
was subjected to laboratory routine investigations for
general anesthesia. Surgically, the preauricular approach
was used in all patients to gain access to the TMJ area.
Gap arthroplasty was applied to release the TMJ
ankylosis. MEVs were measured preoperatively and 3
months postoperatively.
Radiographic assessment for ankylosis and for the middle
ear was performed using multislice CT scan. Volumetric
measurement of middle ear was estimated semidigitally.
MEV was calculated starting from the tympanic mem-
brane to the bony part of the Eustachian tube.
Comparison of the MEV in TMJ ankylosis patients with
normal individuals was carried out. Also, comparison
between MEV preoperatively and postoperatively for
detection of the effect of gap arthroplasty on the MEV
was carried out. The data were tabulated and analyzed
statistically (Fig. 1).
Radiological assessment of the middle ear
All the CT examinations were performed using a slice
multidetector CT scanner (Aquillion 64; Toshiba, Tokyo,
Japan). Scanning was performed on the standard axial
plane using the helical technique (a field of view of
18 cm, a pitch of 0.562, a rotation time of 0.35 s, a section
thickness of 0.5 mm, and a matrix of 512� 512). The
patients were scanned in a supine position to obtain
the image plane parallel to the orbitomeatal line. All the
image data sets were transferred from the CT scanner
to the PC workstation and the data sets were analyzed
using the three-dimensional medical imaging software
(Medicor imaging Charlotte, North Carolina, USA) (on
vitra workstation). MEVs were measured using the digital
Fig. 1
Axial, coronal, and three-dimensional reconstruction images of computed tomography showing an ankylosis bony mass.
TMJ bony ankylosis and middle ear volume Dehis et al. 73

image processing CT program. The area of the air-
containing cavity was measured semiautomatically. A
volume of interest was applied manually on each slice.
The volume of the air-containing cavity at each slice was
computed by clicking on the air cavity within the volume
of interest. The total volume of the air-containing cavity
was calculated as the sum of the volumes of the air-
containing cavities of each slice (Figs 2 and 3).
Radiological measurements of middle ear volume
(1) MEV of the right and left ears of the patient group
(group I).
(2) MEV of the right and left ears of the control group
(group II).
(3) Equality test of the right and left MEV.
(4) Comparison of the preoperative results of MEV of
TMJ ankylosed joints (group I) versus control joints
(group II).
(5) Comparison between preoperative and postoperative
results of MEV of ankylosed joints (group I).
Analysis of patients data
Group I included 14 bony ankylosed joints in eight patients
(two men and six women, age range 18–45 years and mean
age 29.5 years). The etiology of ankylosis was trauma in 75%
of cases and congenital cause in the remaining 25%. The
preoperative interincisal opening ranged from 0 to 6 mm,
mean 3.2 mm. Seventy-five percent of cases had bilateral and
Fig. 2
Outline tracing of preoperative middle ear volume (group I).
Fig. 3
Outline tracing of middle ear volume (group II).
74 Egyptian Journal of Oral & Maxillofacial Surgery 2013, Vol 4 No 3

25% had unilateral involvement with fibrous ankylosis in the
contralateral sides. Previous surgical intervention for the
correction of TMJ ankylosis was reported in six patients:
one of them was operated three times, three patients were
operated two times, and two were operated only once.
Surgical procedure
Gap arthroplasty was performed to release TMJ ankylosis
through a modified preauricular incision under fiberoptic
nasoendotracheal intubation. Patients were admitted for
general anesthesia in the Dental Educational Hospital,
Faculty of Oral and Dental Medicine, Cairo University.
The operation was followed by physiotherapy for 6
months to prevent recurrence (Fig. 4).
ResultsThe postoperative course passed without incidence and
all patients resumed their normal activities early; they
were encouraged for early ambulation and were dis-
charged from the hospital at the second postoperative
day. Follow-up was performed at the outpatient clinic.
The maximum interincisal opening achieved at the end
of 3 months postoperatively ranged from 24 to 50 mm,
mean 35.3 mm.
Results of middle ear volume
Middle ear volume of right and left ears of the
patient group (group I)
On studying the MEV of right ears of the patient group,
it was found that the preoperative values obtained ranged
from 0.036 to 0.528 ml, with a mean of 0.26 ml. The
3-month postoperative volumes obtained ranged from
0.039 to 0.216 ml, with a mean of 0.09 ml (Table 1).
On studying the MEV of left ears of the patient group, it
was found that the recorded preoperative values ranged
from 0.043 to 0.676 ml, with a mean of 0.26 ml. The
recorded 3-month postoperative volumes ranged from
0.021 to 0.184 ml, with a mean of 0.07 ml (Table 1).
Fig. 4
(a) Preauricular incision. (b) Exposure of the ankylotic bony mass. (c) Initiation of cutting the ankylotic bony mass. (d) The gap obtained.(e) Intraoperative interincisal opening.
TMJ bony ankylosis and middle ear volume Dehis et al. 75
Middle ear volume of the right and left ears of the
control group (group II)
The MEV of the right ears of the control group ranged
from 0.742 to 2.193 ml, with a mean of 1.23 ml, whereas
that of the left ears ranged from 0.864 to 1.854 ml, with
a mean of 1.29 ml (Table 1).
Equality test of right and left middle ear volumes
On comparing the results of right and left MEVs of the
operated and the control individuals, it was found that
there was no statistical difference. Hence, the results of
the right and left ears of eight patients with ankylosis and
control individuals were summed up into 14 ankylosed
joints and 16 normal joints.
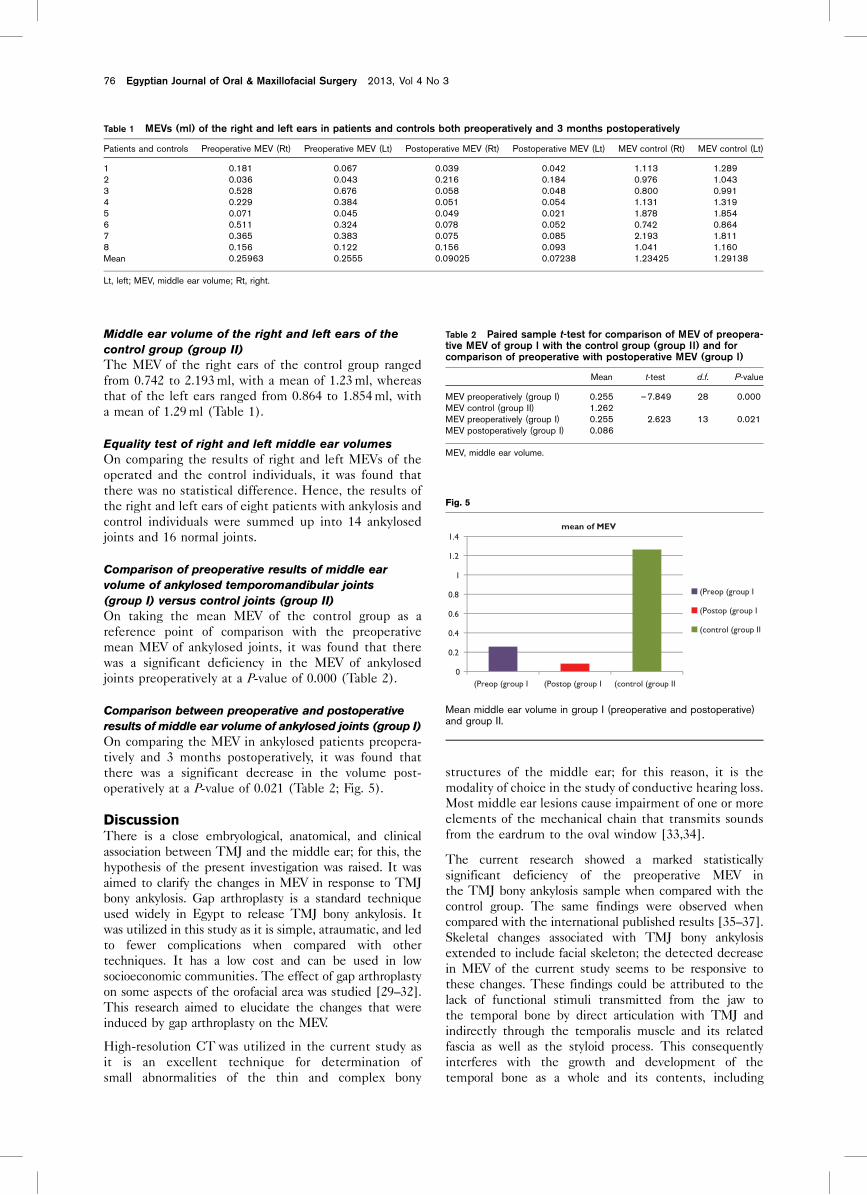
Comparison of preoperative results of middle ear
volume of ankylosed temporomandibular joints
(group I) versus control joints (group II)
On taking the mean MEV of the control group as a
reference point of comparison with the preoperative
mean MEV of ankylosed joints, it was found that there
was a significant deficiency in the MEV of ankylosed
joints preoperatively at a P-value of 0.000 (Table 2).
Comparison between preoperative and postoperative
results of middle ear volume of ankylosed joints (group I)
On comparing the MEV in ankylosed patients preopera-
tively and 3 months postoperatively, it was found that
there was a significant decrease in the volume post-
operatively at a P-value of 0.021 (Table 2; Fig. 5).
DiscussionThere is a close embryological, anatomical, and clinical
association between TMJ and the middle ear; for this, the
hypothesis of the present investigation was raised. It was
aimed to clarify the changes in MEV in response to TMJ
bony ankylosis. Gap arthroplasty is a standard technique
used widely in Egypt to release TMJ bony ankylosis. It
was utilized in this study as it is simple, atraumatic, and led
to fewer complications when compared with other
techniques. It has a low cost and can be used in low
socioeconomic communities. The effect of gap arthroplasty
on some aspects of the orofacial area was studied [29–32].
This research aimed to elucidate the changes that were
induced by gap arthroplasty on the MEV.
High-resolution CT was utilized in the current study as
it is an excellent technique for determination of
small abnormalities of the thin and complex bony
structures of the middle ear; for this reason, it is the
modality of choice in the study of conductive hearing loss.
Most middle ear lesions cause impairment of one or more
elements of the mechanical chain that transmits sounds
from the eardrum to the oval window [33,34].
The current research showed a marked statistically
significant deficiency of the preoperative MEV in
the TMJ bony ankylosis sample when compared with the
control group. The same findings were observed when
compared with the international published results [35–37].
Skeletal changes associated with TMJ bony ankylosis
extended to include facial skeleton; the detected decrease
in MEV of the current study seems to be responsive to
these changes. These findings could be attributed to the
lack of functional stimuli transmitted from the jaw to
the temporal bone by direct articulation with TMJ and
indirectly through the temporalis muscle and its related
fascia as well as the styloid process. This consequently
interferes with the growth and development of the
temporal bone as a whole and its contents, including
Table 1 MEVs (ml) of the right and left ears in patients and controls both preoperatively and 3 months postoperatively
Patients and controls Preoperative MEV (Rt) Preoperative MEV (Lt) Postoperative MEV (Rt) Postoperative MEV (Lt) MEV control (Rt) MEV control (Lt)
1 0.181 0.067 0.039 0.042 1.113 1.2892 0.036 0.043 0.216 0.184 0.976 1.0433 0.528 0.676 0.058 0.048 0.800 0.9914 0.229 0.384 0.051 0.054 1.131 1.3195 0.071 0.045 0.049 0.021 1.878 1.8546 0.511 0.324 0.078 0.052 0.742 0.8647 0.365 0.383 0.075 0.085 2.193 1.8118 0.156 0.122 0.156 0.093 1.041 1.160Mean 0.25963 0.2555 0.09025 0.07238 1.23425 1.29138
Lt, left; MEV, middle ear volume; Rt, right.
Table 2 Paired sample t-test for comparison of MEV of preopera-tive MEV of group I with the control group (group II) and forcomparison of preoperative with postoperative MEV (group I)
Mean t-test d.f. P-value
MEV preoperatively (group I) 0.255 –7.849 28 0.000MEV control (group II) 1.262MEV preoperatively (group I) 0.255 2.623 13 0.021MEV postoperatively (group I) 0.086
MEV, middle ear volume.
Fig. 5
0
0.2
0.4
0.6
0.8
1
1.2
1.4
(Preop (group I (Postop (group I (control (group II
mean of MEV
(Preop (group I
(Postop (group I
(control (group II
Mean middle ear volume in group I (preoperative and postoperative)and group II.
76 Egyptian Journal of Oral & Maxillofacial Surgery 2013, Vol 4 No 3

the middle ear. This explanation needs further investiga-
tion to explore the deficient aspect of the temporal bone
and its relation in patients with TMJ ankylosis. This
finding is supported by hearing impairment in ankylosed
patients detected in a previous study [38].
The postoperative assessment of MEV showed a statis-
tically significant decrease in response to gap arthroplasty.
This might be ascribed to the negative pressure of the
middle ear at that time with an inward movement of
the tympanic membrane. Small MEV in ankylotic
patients makes any change in the volume, however small,
critical or significant. Surgery of TMJ ankylosis, although
it deals with a huge bony mass, usually needs delicate
manipulation to release the jaw from the forest of
multiple abundant vital structures. In contrast, an
atraumatic surgery in close proximity to the external
and middle ears is highly needed. Surgical trauma and its
associated vibration, effusion and collected hematoma are
accused to be responsible for the decrease in MEV.
AcknowledgementsConflicts of interest
There are no conflicts of interest.
References1 Murthy P, Bandasson C, Dhillon RS. Temporomandibular joint
dislocation and deafness from a cricket ball injury. J Laryngol Otol 1994;108:415–416.
2 Cakur B, Sumbullu MA, Durna D, Akgul HM. Prevalence of the types of thepetrotympanic fissure in the temporomandibular joint dysfunction. ActaRadiol 2011; 52:562–565.
3 Axelsson R, Tullberg M, Ernberg M, Hedenberg-Magnusson B. Symptomsand signs of temporomandibular disorders in patients with suddensensorineural hearing loss. Swed Dent J 2009; 33:115–123.
4 Topazian RG. Gap versus interposition arthroplasty for ankylosis of thetemporomandibular joint. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2001; 91:388–389.
5 Belmiro DV, Bessa-Nogueira R, Vago-Cypriano R. Treatment oftemporomandibular joint ankylosis by gap arthroplasty. Med Oral Patol OralCir Bucal 2006; 11:66–69.
6 Devgan A, Siwach RC, Sangwan SS. Functional restoration by excisionarthroplasty in temporomandibular joint ankylosis – a report of 5 cases.Indian J Med Sci 2002; 56:61–64.
7 Matsuura H, Miyamoto H, Ogi N, Kurita K, Goss AN. The effect of gaparthroplasty on temporomandibular joint ankylosis: an experimental study.Int J Oral Maxillofac Surg 2001; 30:431–437.
8 Lam DK, Lawrence HP, Tenenbaum HC. Aural symptoms intemporomandibular disorder patients attending a craniofacial pain unit.J Orofac Pain 2001; 15:146–157.
9 Salvetti G, Manfredini D, Barsotti S, Bosco M. Otologic symptoms intemporomandibular disorders patients: is there evidence of an association-relationship? Minerva Stomatol 2006; 55:627–637.
10 Bettega G, Morand B, Lebeau J, Raphael B. Morphological alterations ofoto-mandibular syndromes. Ann Chir Plast Esthet 2001; 46:495–506.
11 Ioannides AC, Hoogland GA. The disco-malleolar ligament: a possible causeof subjective hearing loss in patients with temporomandibular jointdysfunction. J Maxillofac Surg 1983; 11:227–231.
12 Parker WS, Chole RA. Tinnitus, vertigo and temporomandibular disorders.Am J Orthod Dentofacial Orthop 1995; 107:153–158.
13 Aarnisalo AA, Tervahartiala P, Jero J, Tornwall J. Surgical treatment of chronicotitis media with temporomandibular joint involvement. Auris Nasus Larynx2008; 35:552–555.
14 Cooper BC, Cooper DL. Recognizing otolaryngologic symptoms in patientswith temporomandibular disorders. Cranio 1993; 11:260–267.
15 Morgan DH, Goode RL, Christiansen RL, Tiner LW. The TMJ–earconnection. Cranio 1995; 13:42–43.
16 Kaygusuz I, Karlidag T, Keles E, Yalcin S, Yildiz M, Alpay HC. Ear symptomsaccompanying temporomandibular joint. Kulak Burun Bogaz Ihtis Derg2006; 16:205–208.
17 Sobhy OA, Koutb AR, Abdel-Baki FA, Ali TM, El Raffa I, Khater AH.Evaluation of aural manifestations in temporomandibular joint dysfunction.Clin Otolaryngol Allied Sci 2004; 29:382–385.
18 Vrabec JT, Champion SW, Gomez JD, Johnson RF Jr, Chaljub G. 3D CTimaging method for measuring temporal bone aeration. Acta Otolaryngol2002; 122:831–835.
19 Koc A, Ekinci G, Bilgili AM, Akpinar IN, Yakut H, Han T. Evaluation of themastoid air cell system by high resolution computed tomography threedimensional multiplanar volume rendering technique. J Laryngol Otol 2003;117:595–598.
20 Lee DH, Jun BC, Kim DG, Jung MK, Yeo SW. Volume variation of mastoidpneumatization in different age groups: a study by three-dimensionalreconstruction based on computed tomography images. Surg Radiol Anat2005; 27:37–42.
21 Ahn JY, Park HJ, Park GH, Jeong YS, Kwak HB, Lee YJ, et al. Tympanometryand CT measurement of middle ear volumes in patients with unilateralchronic otitis media. Clin Exp Otorhinolaryngol 2008; 1:139–142.
22 Gaurano JL, Joharjy IA. Middle ear cholesteatoma: characteristic CT findingsin 64 patients. Ann Saudi Med 2004; 24:442–447.
23 Milroy CM, Michaels L. Temporal bone pathology of adult-typeosteopetrosis. Arch Otolaryngol Head Neck Surg 1990; 116:79–84.
24 Hawke M, Jahn AF, Bailey D. Osteopetrosis of the temporal bone. ArchOtolaryngol 1981; 107:278–282.
25 Hamdan AL H, Nabulsi MM, Farhat FT, Haidar RK, Fuleihan N S. When bonebecomes marble: head and neck manifestations of osteopetrosis. PaediatrChild Health 2006; 11:37–40.
26 Papapoulos SE. Paget’s disease of bone: clinical, pathogenetic andtherapeutic aspects. Baillieres Clin Endocrinol Metab 1997; 11:117–143.
27 Ilan O, Bermanb P, Sosnab J, Grossa M. Middle ear virtual endoscopy inmalleus fracture and dislocation. Otorhinolaryngol J 2008; 2:23–25.
28 Trojanowska A, Drop A, Trojanowski P, Rosinska-Bogusiewicz K, Klatka J,Bobek-Billewicz B. External and middle ear diseases: radiological diagnosisbased on clinical signs and symptoms. Insights Imaging 2012; 3:33–48.
29 Kamal A, Dehis M. Effect of gap arthroplasty on tongue position in patientsof temporomandibular joint ankylosis [Master’s thesis]. Cairo, Egypt: Facultyof Oral and Dental Medicine, Cairo University; 1999.
30 Khedr H, Dehis M. Effect of gap arthroplasty on hyoid bone position inpatients of temporomandibular joint ankylosis [Master’s thesis]. Cairo,Egypt: Faculty of Oral and Dental Medicine, Cairo University; 2000.
31 Othman A, Dehis M. Effect of gap arthroplasty on upper airway in patients oftemporomandibular joint ankylosis [Master’s thesis]. Cairo, Egypt: Faculty ofOral and Dental Medicine, Cairo University; 2000.
32 Atta M, Dehis M. Assessment of maxillary sinus volume in patients oftemporomandibular joint bony ankylosis [Master’s thesis]. Cairo, Egypt:Faculty of Oral and Dental Medicine, Cairo University; 2012.
33 Fatterpekar GM, Doshi AH, Dugar M, Delman BN, Naidich TP, Som PM.Role of 3D CT in the evaluation of the temporal bone. Radiographics 2006;26:117–132.
34 Majdani O, Thews K, Bartling S, Leinung M, Dalchow C, Labadie R.Temporal bone imaging: comparison of flat panel volume CT andmultisection CT. Am J Neuroradiol 2009; 30:1419–1424.
35 Jae-Yoon A, Hong-Ju P, Ga-Hyun P, Yong-Soo J, Hi-Boong K, Yeo-Jin S,Won-Jin M. Tympanometry and CT measurement of middle ear volumes inpatients with unilateral chronic otitis media. Surg Radiol Anat 2004;26:145–148.
36 Alexander JO, John SO, Jeffrey TV. Middle ear volume as an adjunctmeasure in congenital aural atresia. Int J Pediatr Otorhinolaryngol 2011;75:910–914.
37 Maroldi R, Farina D, Palvarini L, Marconi A, Gadola E, Menni K, Battaglia G.Computed tomography and magnetic resonance imaging of pathologicconditions of the middle ear. Eur J Radiol 2001; 40:78–93.
38 Rashed SA, Sayed M, Kamal NM, Dehis M, Kamal A. Evaluation of the effectof temporomandibular joint ankylosis and relevant gap arthroplasty onauditory functions. Egypt Dent J 2013; 59:146–151.
TMJ bony ankylosis and middle ear volume Dehis et al. 77





























